
Technical Evaluation of the COBAS EGFR Semiquantitative Index (SQI) for Plasma cfDNA Testing in NSCLC Patients with EGFR Exon 19 Deletions

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Plasma Samples
2.2. Extraction of cfDNA from Plasma Samples
2.3. Molecular Characterization of EGFR in cfDNA from Plasma
2.4. Statistical Analysis
3. Results
3.1. Study Cohort
3.2. Agreement between Cobas® EGFR Test and the ddPCRTM EGFR Test
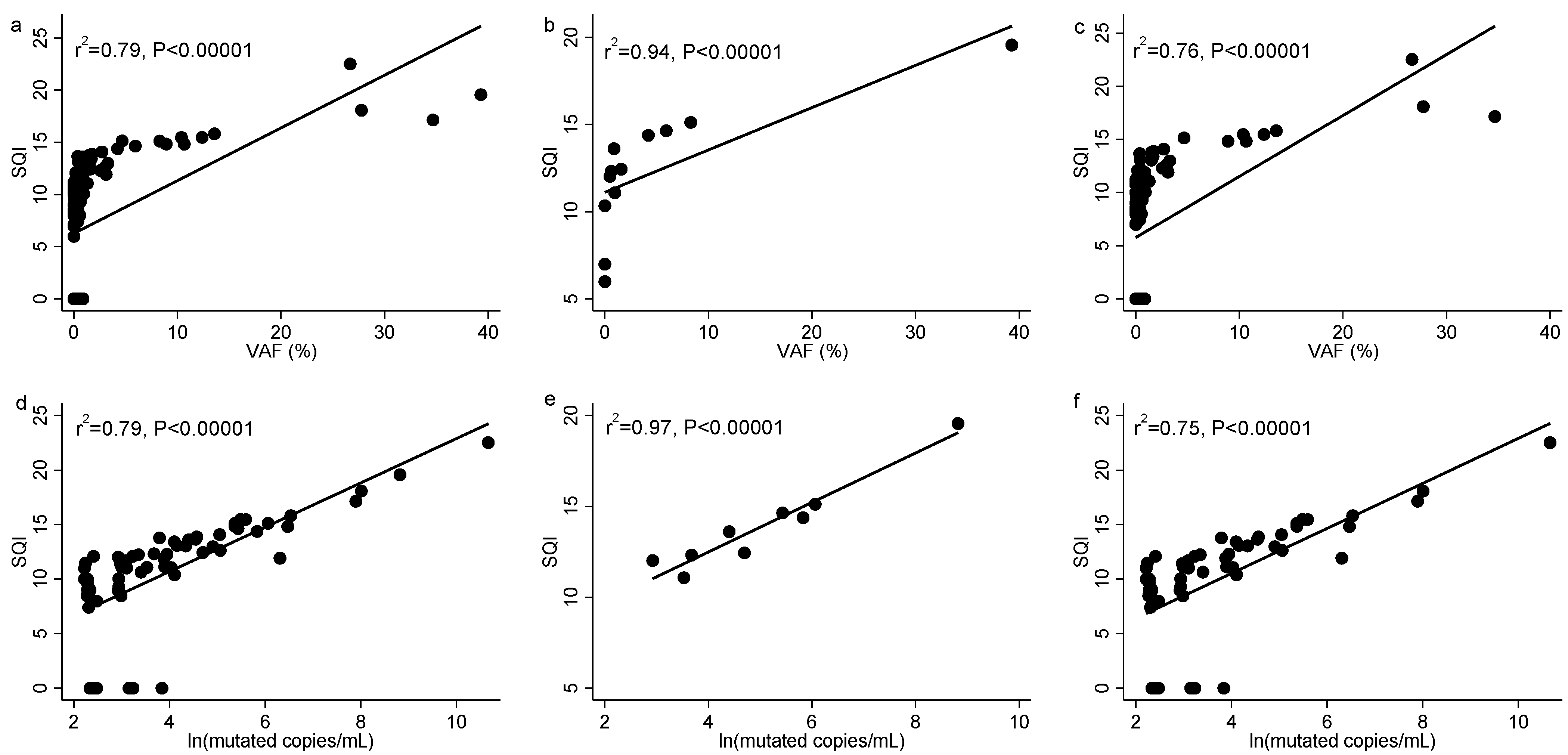
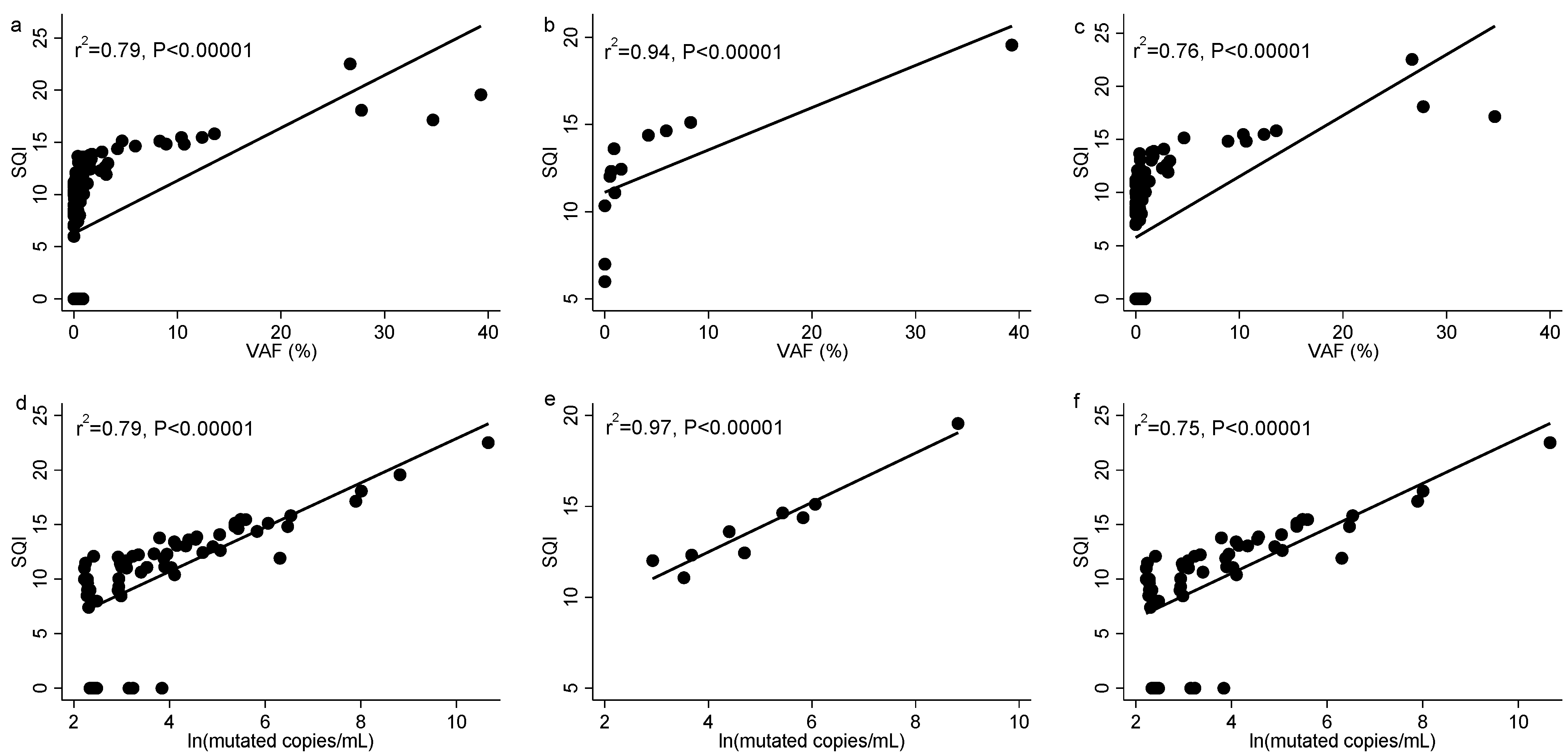
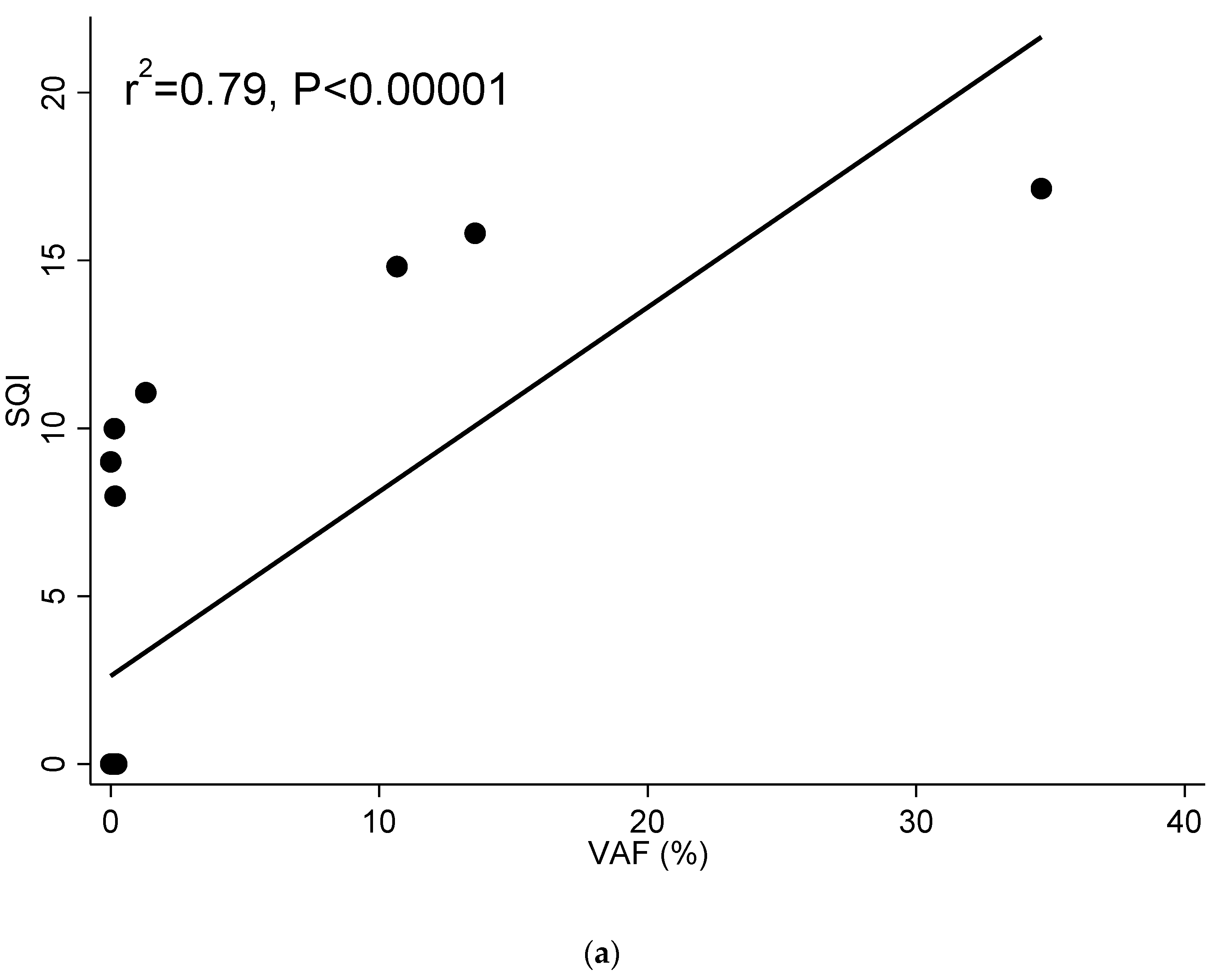
3.3. The SQI from Cobas® EGFR Test Correlates with the VAF and the Number of Mutated Copies/mL from ddPCRTM EGFR Test
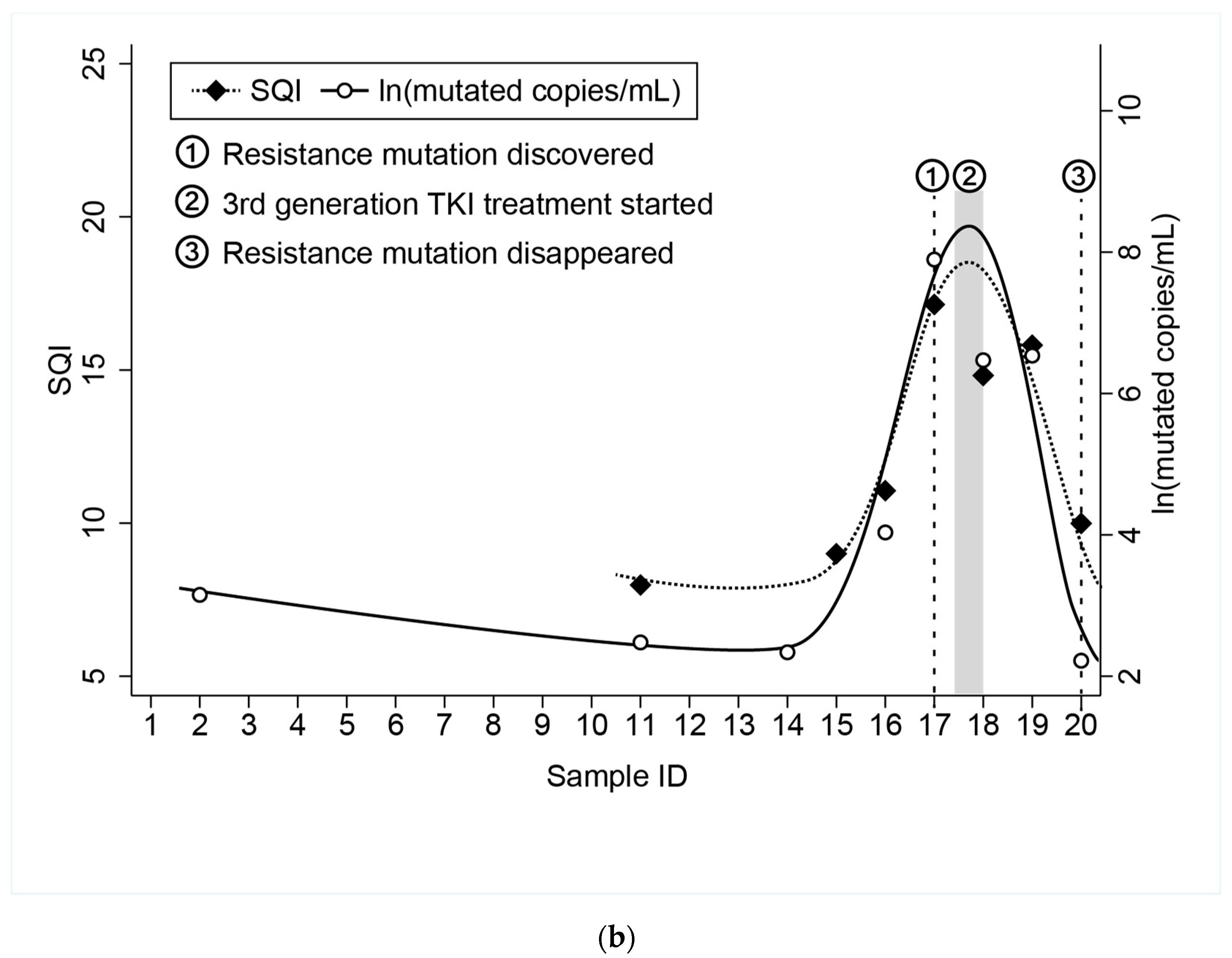
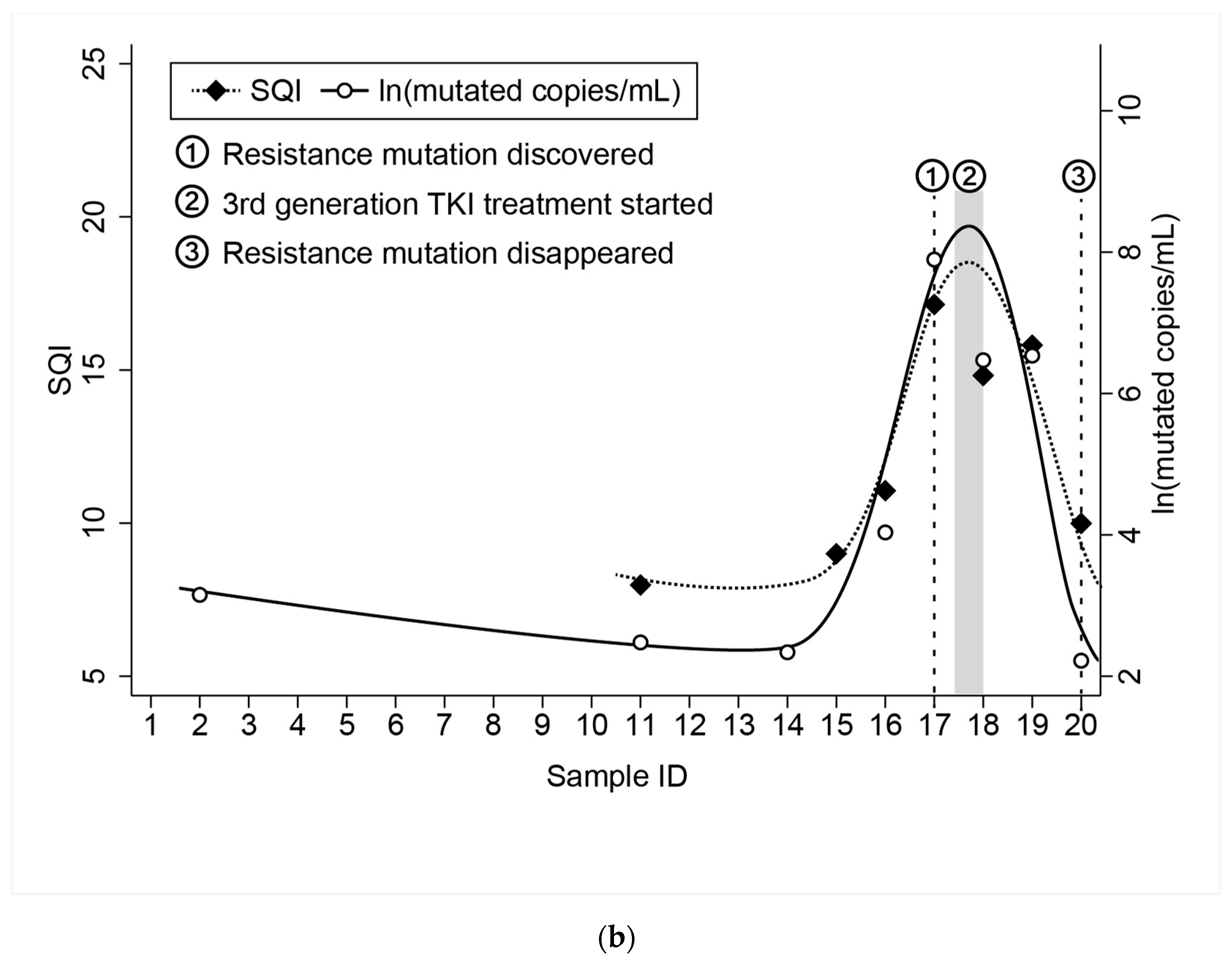
3.4. Example of Correlation between SQI and VAF and SQI and Mutated Copies/mL in a Patient with Longitudinal Follow-Up
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [Green Version]
- Testa, U.; Castelli, G.; Pelosi, E. Lung Cancers: Molecular Characterization, Clonal Heterogeneity and Evolution, and Cancer Stem Cells. Cancers 2018, 10, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, P.T.; Vyse, S.; Huang, P.H. Rare epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer. Semin. Cancer Biol. 2020, 61, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Camidge, D.R.; Pao, W.; Sequist, L.V. Acquired resistance to TKIs in solid tumours: Learning from lung cancer. Nat. Rev. Clin. Oncol. 2014, 11, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated molecular testing guideline for the selection of lung cancer patients for treatment with targeted tyrosine kinase inhibitors guideline from the college of American pathologists, the international association for the study of lung cancer, and the a. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, L.A., Jr.; Bardelli, A.; Diaz, L.A.; Bardelli, A. Liquid biopsies: Genotyping circulating tumor DNA. J. Clin. Oncol. 2014, 32, 579–586. [Google Scholar] [CrossRef] [PubMed]
- González de Aledo-Castillo, J.M.; Arcocha, A.; Victoria, I.; Martinez-Puchol, A.I.; Sánchez, C.; Jares, P.; Rodríguez, G.F.; Viñolas, N.; Reyes, R.; Reguart, N.; et al. Molecular characterization of advanced non-small cell lung cancer patients by cfDNA analysis: Experience from routine laboratory practice. J. Thorac. Dis. 2021, 13, 1658–1670. [Google Scholar] [CrossRef]
- Del Re, M.; Bordi, P.; Rofi, E.; Restante, G.; Valleggi, S.; Minari, R.; Crucitta, S.; Arrigoni, E.; Chella, A.; Morganti, R.; et al. The amount of activating EGFR mutations in circulating cell-free DNA is a marker to monitor osimertinib response. Br. J. Cancer 2018, 119, 1252–1258. [Google Scholar] [CrossRef] [Green Version]
- Guibert, N.; Pradines, A.; Favre, G.; Mazieres, J. Current and future applications of liquid biopsy in nonsmall cell lung cancer from early to advanced stages. Eur. Respir. Rev. 2020, 29. [Google Scholar] [CrossRef] [Green Version]
- Abbosh, C.; Birkbak, N.J.; Swanton, C. Early stage NSCLC—Challenges to implementing ctDNA-based screening and MRD detection. Nat. Rev. Clin. Oncol. 2018, 15, 577–586. [Google Scholar] [CrossRef]
- Abbosh, C.; Birkbak, N.J.; Wilson, G.A.; Jamal-Hanjani, M.; Constantin, T.; Salari, R.; Le Quesne, J.; Moore, D.A.; Veeriah, S.; Rosenthal, R.; et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature 2017, 545, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Pisapia, P.; Malapelle, U.; Troncone, G. Liquid Biopsy and Lung Cancer. Acta Cytol. 2018, 63, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating liquid biopsies into the management of cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar] [CrossRef] [PubMed]
- Roche cobas® EGFR Mutation Test v2 for in vitro diagnostic use. FDA, 2016; 1–71.
- Ntzifa, A.; Kroupis, C.; Haliassos, A.; Lianidou, E. A pilot plasma-ctDNA ring trial for the Cobas® EGFR Mutation Test in clinical diagnostic laboratories. Clin. Chem. Lab. Med. 2019, 57, e97–e101. [Google Scholar] [CrossRef] [PubMed]
- Chae, Y.K.; Oh, M.S. Detection of Minimal Residual Disease Using ctDNA in Lung Cancer: Current Evidence and Future Directions. J. Thorac. Oncol. 2019, 14, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Mok, T.; Wu, Y.-L.; Lee, J.S.; Yu, C.-J.; Sriuranpong, V.; Sandoval-Tan, J.; Ladrera, G.; Thongprasert, S.; Srimuninnimit, V.; Liao, M.; et al. Detection and Dynamic Changes of EGFR Mutations from Circulating Tumor DNA as a Predictor of Survival Outcomes in NSCLC Patients Treated with First-line Intercalated Erlotinib and Chemotherapy. Clin. Cancer Res. 2015, 21, 3196–3203. [Google Scholar] [CrossRef] [Green Version]
- Herbreteau, G.; Vallée, A.; Charpentier, S.; Normanno, N.; Hofman, P.; Denis, M.G. Circulating free tumor DNA in non-small cell lung cancer (NSCLC): Clinical application and future perspectives. J. Thorac. Dis. 2019, 11, S113. [Google Scholar] [CrossRef]
- Marchetti, A.; Palma, J.F.; Felicioni, L.; De Pas, T.M.; Chiari, R.; Del Grammastro, M.; Filice, G.; Ludovini, V.; Brandes, A.A.; Chella, A.; et al. Early prediction of response to tyrosine kinase inhibitors by quantification of EGFR mutations in plasma of NSCLC patients. J. Thorac. Oncol. 2015, 10, 1437–1443. [Google Scholar] [CrossRef] [Green Version]
- Macías, M.; Alegre, E.; Alkorta-Aranburu, G.; Patiño-García, A.; Mateos, B.; Andueza, M.P.; Gúrpide, A.; Lopez-Picazo, J.M.; Gil-Bazo, I.; Perez-Gracia, J.L.; et al. The Dynamic Use of EGFR Mutation Analysis in Cell-Free DNA as a Follow-Up Biomarker during Different Treatment Lines in Non-Small-Cell Lung Cancer Patients. Dis. Markers 2019, 2019, 7954921. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Shin, S.; Lee, K.-A. A Comparative Study for Detection of EGFR Mutations in Plasma Cell-Free DNA in Korean Clinical Diagnostic Laboratories. BioMed Res. Int. 2018, 2018, 7392419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteva-Socias, M.; Enver-Sumaya, M.; Gómez-Bellvert, C.; Guillot, M.; Azkárate, A.; Marsé, R.; Sastre, Ú.; Blasco, A.; Calabuig-Fariñas, S.; Asensio, V.J.; et al. Detection of the EGFR G719S Mutation in Non-small Cell Lung Cancer Using Droplet Digital PCR. Front. Med. 2020, 7, 594900. [Google Scholar] [CrossRef]
- So, M.-K.; Park, J.-H.; Kim, J.-W.; Jang, J.-H. Analytical Validation of a Pan-Cancer Panel for Cell-Free Assay for the Detection of EGFR Mutations. Diagnostics 2021, 11, 1022. [Google Scholar] [CrossRef]
- Keppens, C.; Palma, J.F.; Das, P.M.; Scudder, S.; Wen, W.; Normanno, N.; van Krieken, J.H.; Sacco, A.; Fenizia, F.; Gonzalez de Castro, D.; et al. Detection of EGFR Variants in Plasma: A Multilaboratory Comparison of a Real-Time PCR EGFR Mutation Test in Europe. J. Mol. Diagn. 2018, 20, 483–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buder, A.; Setinek, U.; Hochmair, M.J.; Schwab, S.; Kirchbacher, K.; Keck, A.; Burghuber, O.C.; Pirker, R.; Filipits, M. EGFR Mutations in Cell-free Plasma DNA from Patients with Advanced Lung Adenocarcinoma: Improved Detection by Droplet Digital PCR. Target Oncol. 2019, 14, 197–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef] [PubMed]
- Kalemkerian, G.P.; Narula, N.; Kennedy, E.B.; Biermann, W.A.; Donington, J.; Leighl, N.B.; Lew, M.; Pantelas, J.; Ramalingam, S.S.; Reck, M.; et al. Molecular Testing Guideline for the Selection of Patients With Lung Cancer for Treatment with Targeted Tyrosine Kinase Inhibitors: American Society of Clinical Oncology Endorsement of the College of American Pathologists/International Association for the Study of Lung Cancer/Association for Molecular Pathology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Ayala de la Peña, F.; Ortiz-Muñoz, B.; Quintanar-Verdúguez, T.; Santotoribio, J.D.; de la Cruz, S.; Trapé-Pujol, J.; Galve-Calvo, E.; Augé-Fradera, J.M.; García-Gómez, J.; González-Hernández, Á. Consensus of the Spanish society of laboratory medicine and the Spanish society of medical oncology on the methodology and criteria for evaluation of circulating tumour markers in breast cancer. Clin. Transl. Oncol. 2021, 23, 1272–1280. [Google Scholar] [CrossRef]
- Gaspar Blázquez, M.J.; Trapé Pujol, J.; Augé Fradera, J.M.; Barco Sánchez, A.; Carbonell Muñoz, R.; Filella Pla, X.; Fernández Suarez, A.; González Hernández, Á.; Martínez Peinado, A.; Pérez Barrios, C.; et al. Recomendaciones para la optimización del uso de marcadores tumorales de utilización frecuente. Recomendación (2018). Rev. Lab. Clínico 2019, 12, 38–52. [Google Scholar] [CrossRef]
- de Castro, J.; Cobo, M.; Isla, D.; Puente, J.; Reguart, N.; Cabeza, B.; Gayete, A.; Sánchez, M.; Torres, M.I.; Ferreirós, J. Recommendations for radiological diagnosis and assessment of treatment response in lung cancer: A national consensus statement by the Spanish Society of Medical Radiology and the Spanish Society of Medical Oncology. Clin. Transl. Oncol. 2015, 17, 11–23. [Google Scholar] [CrossRef]
- Majem, M.; Hernández-Hernández, J.; Hernando-Trancho, F.; Rodríguez de Dios, N.; Sotoca, A.; Trujillo-Reyes, J.C.; Vollmer, I.; Delgado-Bolton, R.; Provencio, M. Multidisciplinary consensus statement on the clinical management of patients with stage III non-small cell lung cancer. Clin. Transl. Oncol. 2020, 22, 21–36. [Google Scholar] [CrossRef] [Green Version]
- Soria-Comes, T.; Palomar-Abril, V.; Ureste, M.M.; Guerola, M.T.; Maiques, I.C.M. Real-World Data of the Correlation between EGFR Determination by Liquid Biopsy in Non-squamous Non-small Cell Lung Cancer (NSCLC) and the EGFR Profile in Tumor Biopsy. Pathol. Oncol. Res. 2020, 26, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Sacher, A.G.; Paweletz, C.; Dahlberg, S.E.; Alden, R.S.; O’Connell, A.; Feeney, N.; Mach, S.L.; Jänne, P.A.; Oxnard, G.R. Prospective Validation of Rapid Plasma Genotyping for the Detection of EGFR and KRAS Mutations in Advanced Lung Cancer. JAMA Oncol. 2016, 2, 1014–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oxnard, G.R.; Paweletz, C.P.; Kuang, Y.; Mach, S.L.; O'Connell, A.; Messineo, M.M.; Luke, J.J.; Butaney, M.; Kirschmeier, P.; Jackman, D.M.; et al. Noninvasive Detection of Response and Resistance in EGFR Mutant Lung Cancer Using Quantitative Next-Generation Genotyping of Cell-Free Plasma DNA. Clin. Cancer Res. 2014, 20, 1698–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taus, Á.; Camacho, L.; Rocha, P.; Hardy-Werbin, M.; Pijuan, L.; Piquer, G.; López, E.; Dalmases, A.; Longarón, R.; Clavé, S.; et al. Dynamics of EGFR Mutation Load in Plasma for Prediction of Treatment Response and Disease Progression in Patients with EGFR-Mutant Lung Adenocarcinoma. Clin. Lung Cancer 2018, 19, 387–394.e2. [Google Scholar] [CrossRef] [PubMed]
- Roelofsen-de Beer, R.; Wielders, J.; Boursier, G.; Vodnik, T.; Vanstapel, F.; Huisman, W.; Vukasović, I.; Vaubourdolle, M.; Sönmez, Ç.; Linko, S.; et al. Validation and verification of examination procedures in medical laboratories: Opinion of the EFLM Working Group Accreditation and ISO/CEN standards (WG-A/ISO) on dealing with ISO 15189:2012 demands for method verification and validation. Clin. Chem. Lab. Med. 2020, 58, 361–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, J.D. Translational genomics: The challenge of developing cancer biomarkers. Genome Res. 2012, 22, 183–187. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Guo, Q.; Yu, W.; Qiao, L.; Zhao, M.; Zhang, C.; Hu, X.; Yang, G.; Xiong, L.; Lou, J. Quantification of plasma EGFR mutations in patients with lung cancers: Comparison of the performance of ARMS-Plus and droplet digital PCR. Lung Cancer 2017, 114, 31–37. [Google Scholar] [CrossRef]
- Pender, A.; Garcia-Murillas, I.; Rana, S.; Cutts, R.J.; Kelly, G.; Fenwick, K.; Kozarewa, I.; Gonzalez de Castro, D.; Bhosle, J.; O’Brien, M.; et al. Efficient Genotyping of KRAS Mutant Non-Small Cell Lung Cancer Using a Multiplexed Droplet Digital PCR Approach. PLoS ONE 2015, 10, e0139074. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| ID | Age | Sex | EGFR Status by Tissue Analyses | Number of Samples | Baseline Samples | Follow-Up Samples | Mutation Included in Cobas EGFR Test | Mutation Included in ddPCR Assay |
|---|---|---|---|---|---|---|---|---|
| ID01 | 91 | F | NA | 1 | 1 | 0 | NA | NA |
| ID02 | 73 | M | c.2235_2249del15 | 1 | 1 | 0 | Yes | Yes |
| ID03 | 53 | M | c.2240_2251del12 | 4 | 1 | 3 | Yes | No |
| ID04 | 40 | M | c.2236_2250del15 | 5 | 1 | 4 | Yes | Yes |
| ID05 | 56 | F | NA | 3 | 1 | 2 | NA | NA |
| ID06 | 70 | M | NA | 2 | 1 | 1 | NA | NA |
| ID07 | 77 | M | NA | 3 | 1 | 2 | NA | NA |
| ID08 | 87 | M | c.2236_2250del15 | 2 | 1 | 1 | Yes | Yes |
| ID09 | 72 | F | c.2235_2249del15 | 6 | 1 | 5 | Yes | Yes |
| ID10 | 87 | F | c.2236_2250del15 | 2 | 1 | 1 | Yes | Yes |
| ID11 | 70 | F | NA | 1 | 1 | 0 | NA | NA |
| ID12 | 79 | F | NA | 3 | 1 | 2 | NA | NA |
| ID13 | 61 | F | c.2235_2249del15 | 2 | 0 | 2 | Yes | Yes |
| ID14 | 81 | F | NA | 4 | 0 | 4 | NA | NA |
| ID15 | 69 | F | c.2240_2257del18 | 20 | 0 | 20 | Yes | Yes |
| ID16 | 56 | F | c.2337_2255insT | 2 | 0 | 2 | Yes | No |
| ID17 | 74 | F | c.2235_2249del15 | 1 | 0 | 1 | Yes | Yes |
| ID18 | 83 | F | NA | 8 | 0 | 8 | NA | NA |
| ID19 | 67 | F | NA | 2 | 0 | 2 | NA | NA |
| ID20 | 67 | M | NA | 12 | 0 | 12 | NA | NA |
| ID21 | 80 | F | c.2235_2249del15 | 1 | 0 | 1 | Yes | Yes |
| ID22 | 45 | F | c.2235_2249del15 | 11 | 0 | 11 | Yes | Yes |
| ID23 | 49 | F | c.2236_2250del15 | 5 | 0 | 5 | Yes | Yes |
| ID24 | 58 | F | c.2240_2254del15 | 2 | 0 | 2 | Yes | Yes |
| ID25 | 61 | F | c.2236_2250del15 | 15 | 0 | 15 | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González de Aledo-Castillo, J.M.; Serhir-Sgheiri, S.; Calbet-Llopart, N.; Arcocha, A.; Jares, P.; Reguart, N.; Puig-Butillé, J.A. Technical Evaluation of the COBAS EGFR Semiquantitative Index (SQI) for Plasma cfDNA Testing in NSCLC Patients with EGFR Exon 19 Deletions. Diagnostics 2021, 11, 1319. https://doi.org/10.3390/diagnostics11081319
González de Aledo-Castillo JM, Serhir-Sgheiri S, Calbet-Llopart N, Arcocha A, Jares P, Reguart N, Puig-Butillé JA. Technical Evaluation of the COBAS EGFR Semiquantitative Index (SQI) for Plasma cfDNA Testing in NSCLC Patients with EGFR Exon 19 Deletions. Diagnostics. 2021; 11(8):1319. https://doi.org/10.3390/diagnostics11081319
Chicago/Turabian StyleGonzález de Aledo-Castillo, José Manuel, Samira Serhir-Sgheiri, Neus Calbet-Llopart, Ainara Arcocha, Pedro Jares, Noemí Reguart, and Joan Antón Puig-Butillé. 2021. "Technical Evaluation of the COBAS EGFR Semiquantitative Index (SQI) for Plasma cfDNA Testing in NSCLC Patients with EGFR Exon 19 Deletions" Diagnostics 11, no. 8: 1319. https://doi.org/10.3390/diagnostics11081319
APA StyleGonzález de Aledo-Castillo, J. M., Serhir-Sgheiri, S., Calbet-Llopart, N., Arcocha, A., Jares, P., Reguart, N., & Puig-Butillé, J. A. (2021). Technical Evaluation of the COBAS EGFR Semiquantitative Index (SQI) for Plasma cfDNA Testing in NSCLC Patients with EGFR Exon 19 Deletions. Diagnostics, 11(8), 1319. https://doi.org/10.3390/diagnostics11081319