
Feasibility Study on Using Dynamic Contrast Enhanced MRI to Assess the Effect of Tyrosine Kinase Inhibitor Therapy within the STAR Trial of Metastatic Renal Cell Cancer

 ,
,
Abstract
1. Introduction
2. Materials and Methods
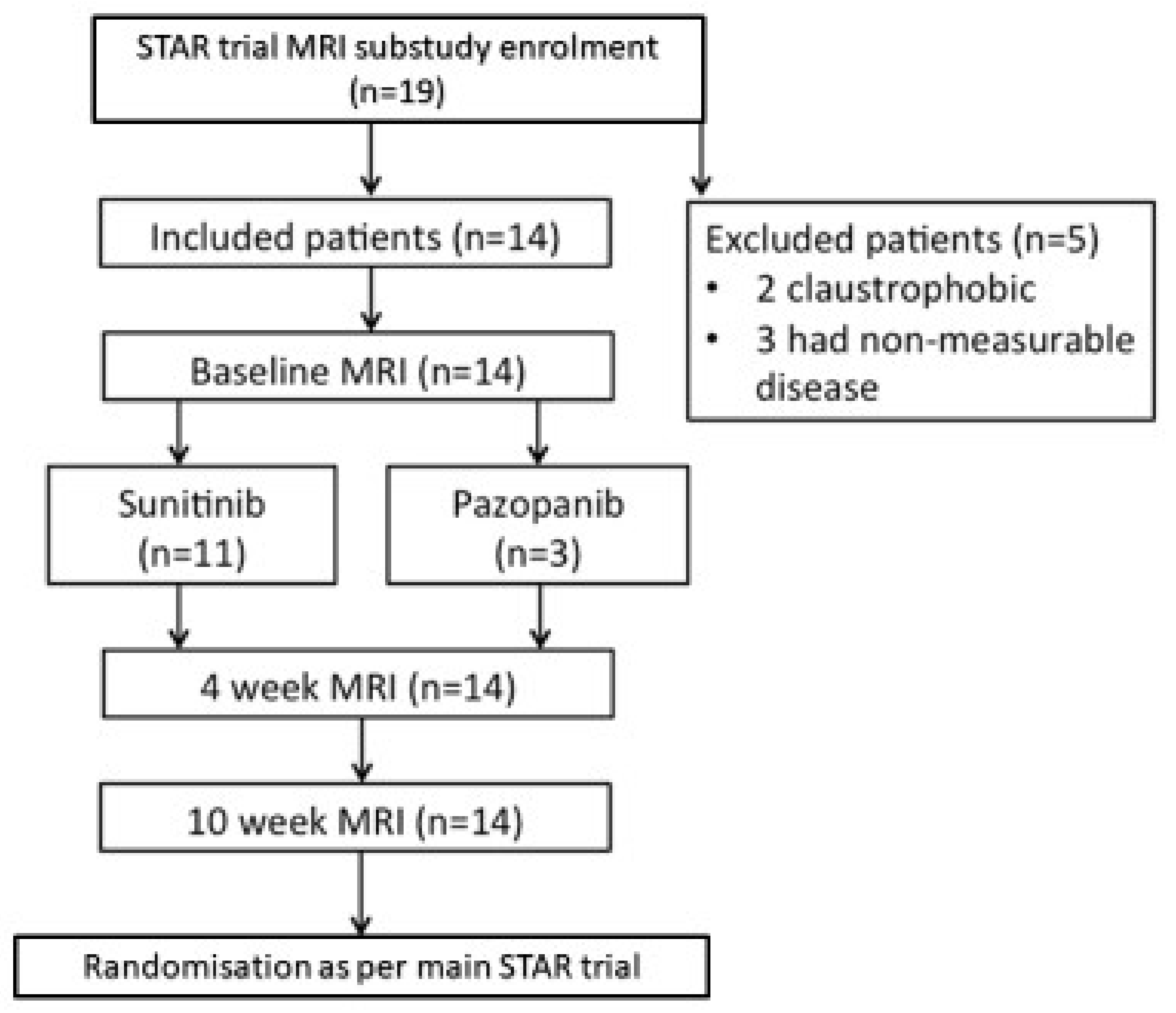
2.1. Patient Recruitment and Intervention
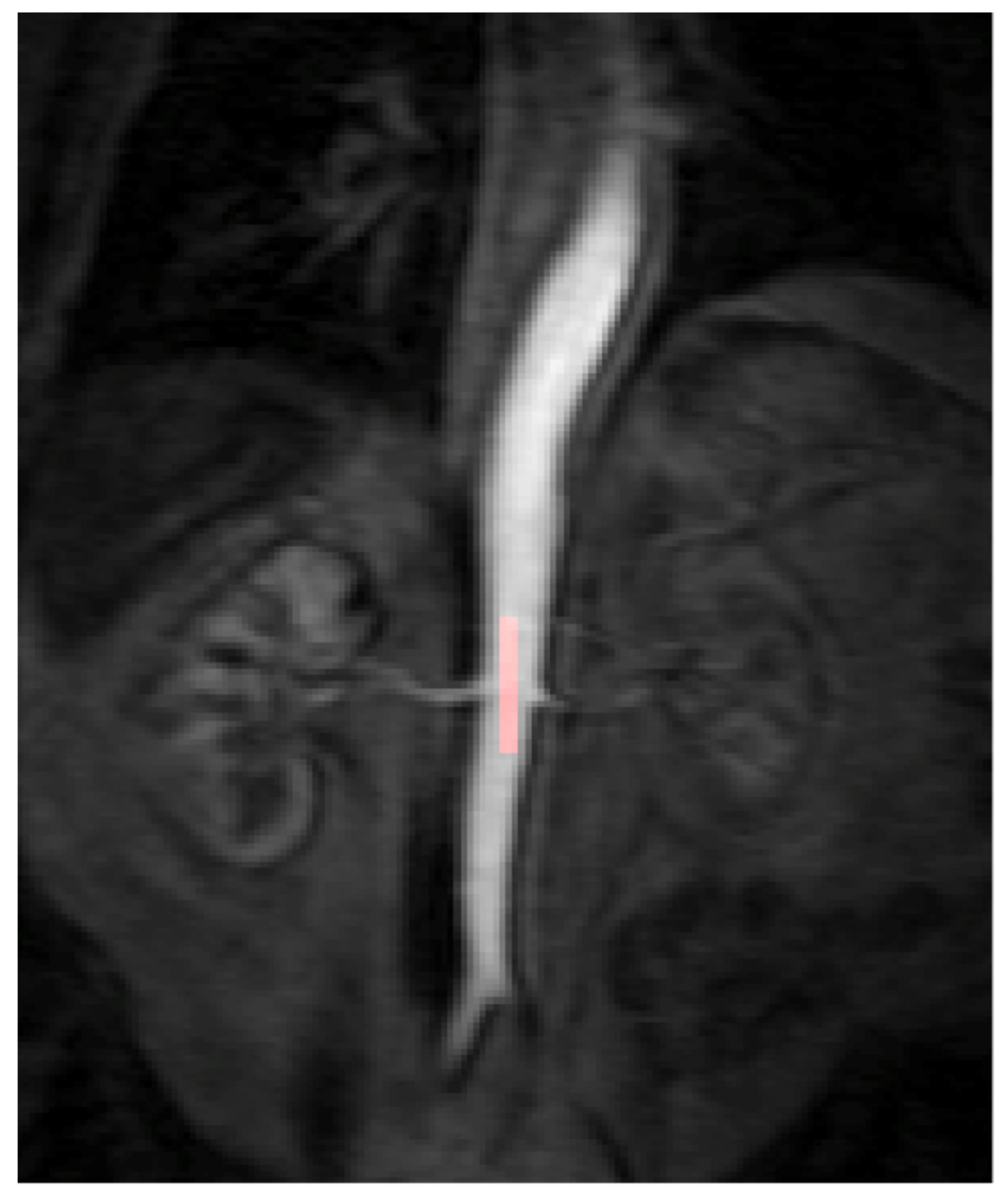
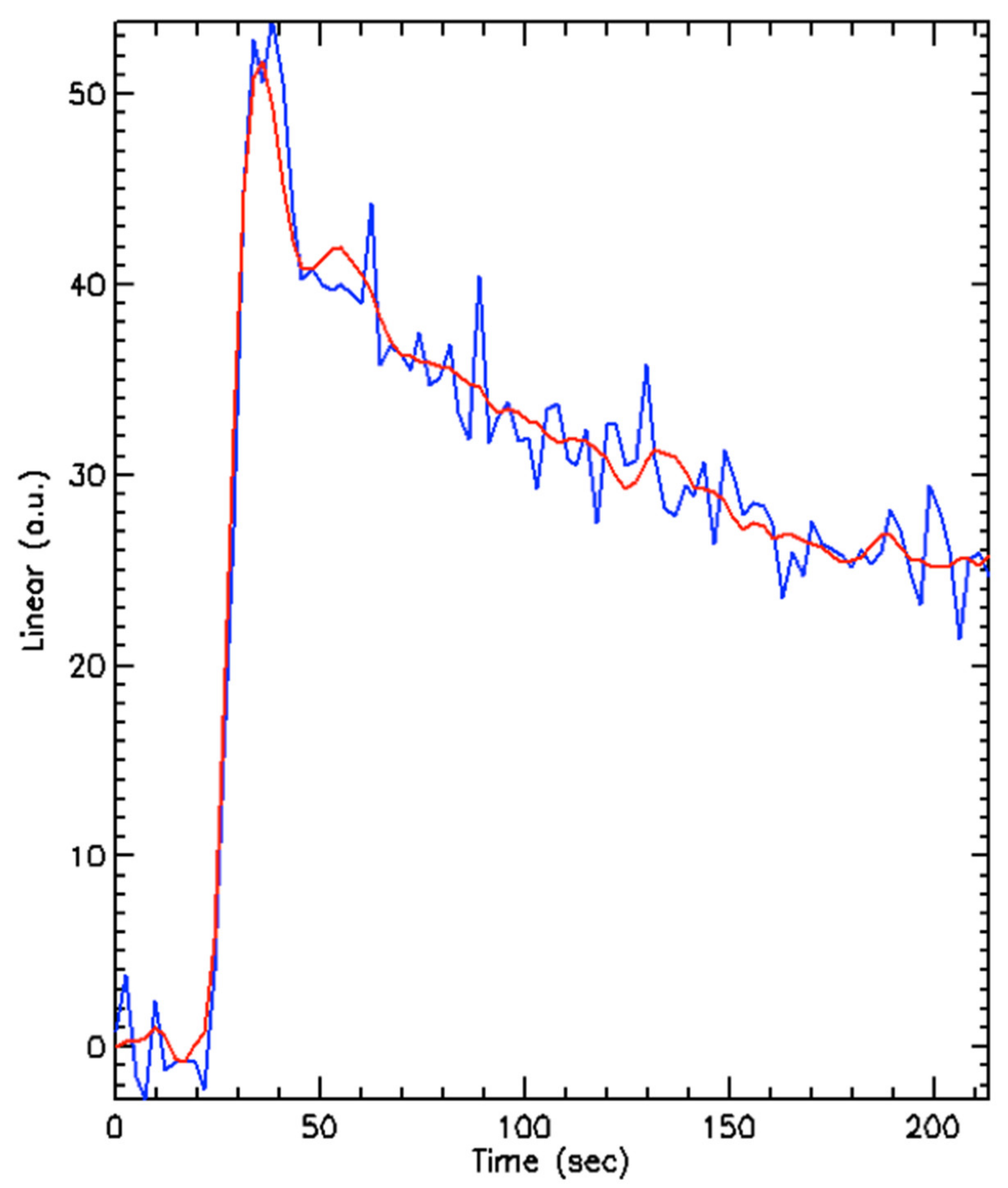
2.2. Dynamic Contrast Enhanced Magnetic Resonance Imaging (DCE-MRI)
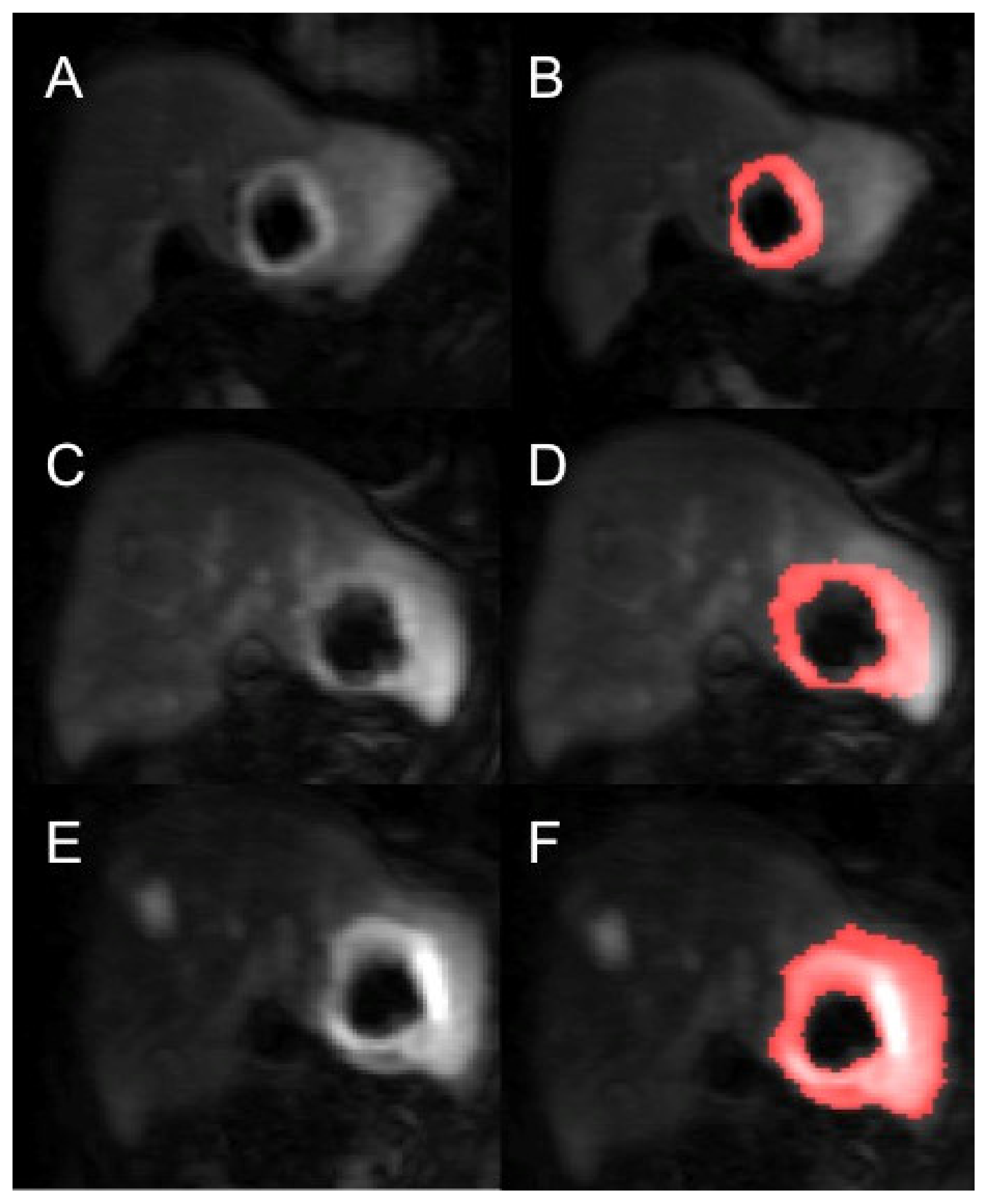
2.3. Post DCE-MRI Acquisition Image Analysis
2.4. Statistical Analysis
3. Results
Interobserver Agreement
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of inci-dence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Saad, A.; Gad, M.M.; Al-Husseini, M.J.; Ruhban, I.A.; Sonbol, M.; Ho, T.H. Trends in renal-cell carcinoma incidence and mortality in the United States in the last 2 decades: A SEER-based study. Clin. Genitourin. Cancer 2019, 17, 46–57. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Surveillance, Epidemiology and End Results (SEER) Program, 2017. Available online: https://seer.cancer.gov/ (accessed on 10 July 2021).
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; De Souza, P.; Merchan, J.R.; et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, J.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Wasser, K.; Klein, S.K.; Fink, C.; Junkermann, H.; Sinn, H.-P.; Zuna, I.; Knopp, M.V.; Delorme, S. Evaluation of neoadjuvant chemotherapeutic response of breast cancer using dynamic MRI with high temporal resolution. Eur. Radiol. 2003, 13, 80–87. [Google Scholar] [CrossRef]
- Mankoff, D.A.; Dunnwald, L.K.; Gralow, J.R.; Ellis, G.K.; Schubert, E.K.; Tseng, J.; Lawton, T.J.; Linden, H.M.; Livingston, R.B. Changes in blood flow and metabolism in locally advanced breast cancer treated with neoadjuvant chemotherapy. J. Nucl. Med. 2003, 44, 1806–1814. [Google Scholar]
- Fournier, L.S.; Oudard, S.; Thiam, R.; Trinquart, L.; Banu, E.; Médioni, J.; Balvay, D.; Chatellier, G.; Frija, G.; Cuenod, C.A. Metastatic renal carcinoma: Evaluation of antiangiogenic therapy with dynamic contrast-enhanced CT. Radiology 2010, 256, 511–518. [Google Scholar] [CrossRef]
- Collinson, F.J.; Gregory, W.M.; McCabe, C.; Howard, H.; Lowe, C.; Potrata, D.B.; Tubeuf, S.; Hanlon, P.; McParland, L.; Wah, T.; et al. The STAR trial protocol: A randomised multi-stage phase II/III study of sunitinib comparing temporary cessation with allowing continuation, at the time of maximal radiological response, in the first-line treatment of locally advanced/metastatic renal cancer. BMC Cancer 2012, 12, 598. [Google Scholar]
- Choueiri, T.; Powles, T.; Burotto, M.; Bourlon, M.; Zurawski, B.; Juárez, V.O.; Hsieh, J.; Basso, U.; Shah, A.; Suarez, C.; et al. 696O_PR Nivolumab + cabozantinib vs. sunitinib in first-line treatment for advanced renal cell carcinoma: First results from the randomized phase III CheckMate 9ER trial. Ann. Oncol. 2020, 31, S1159. [Google Scholar] [CrossRef]
- Chapman, S.; Wah, T.M.; Sourbron, S.; Buckley, D. The effects of cryoablation on renal cell carcinoma perfusion and glomerular filtration rate measured using dynamic contrast-enhanced MRI: A feasibility study. Clin. Radiol. 2013, 68, 887–894. [Google Scholar] [CrossRef]
- Wah, T.; Sourbron, S.; Wilson, D.; Magee, D.; Gregory, W.; Selby, P.; Buckley, D.L. Renal cell carcinoma perfusion before and after radiofrequency ablation measured with dynamic contrast enhanced MRI: A pilot study. Diagnostics 2018, 8, 3. [Google Scholar] [CrossRef]
- Notohamiprodjo, M.; Sourbron, S.; Staehler, M.; Michaely, H.J.; Attenberger, U.I.; Schmidt, G.P.; Boehm, H.; Horng, A.; Glaser, C.; Stief, C.; et al. Measuring perfusion and permeability in renal cell carcinoma with dynamic contrast-enhanced MRI: A pilot study. J. Magn. Reson. Imaging 2010, 31, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Rosen, M.A.; Schnall, M.D. Dynamic contrast-enhanced magnetic resonance imaging for assessing tumor vascularity and vascular effects of targeted therapies in renal cell carcinoma. Clin. Cancer Res. 2007, 13, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, K.T.; Rosen, M.A.; Heitjan, D.F.; Gallagher, M.L.; Schwartz, B.; Schnall, M.D.; O’Dwyer, P.J. Pilot study of DCE-MRI to predict progression-free survival with sorafenib therapy in renal cell carcinoma. Cancer Biol. Ther. 2008, 7, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, L.; Wilson, D.J.; Sharma, N.; Perren, T.J.; Buckley, D.L. A functional form for a representative individual arterial input function measured from a population using high temporal resolution DCE MRI. Magn. Reson. Med. 2018, 81, 1955–1963. [Google Scholar] [CrossRef]
- Sourbron, S.P.; Buckley, D. On the scope and interpretation of the Tofts models for DCE-MRI. Magn. Reson. Med. 2011, 66, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, J.J.; Purdue, M.P.; Signoretti, S.; Swanton, C.; Albiges, L.; Schmidinger, M.; Heng, D.Y.; Larkin, J.; Ficarra, V. Renal cell carcinoma. Nat. Rev. Dis. Prim. 2017, 3, 17009. [Google Scholar] [CrossRef]
- Ng, C.S.; Wang, X.; Faria, S.C.; Lin, E.; Charnsangavej, C.; Tannir, N.M. Perfusion CT in patients with metastatic renal cell carcinoma treated with interferon. Am. J. Roentgenol. 2010, 194, 166–171. [Google Scholar] [CrossRef]
- Bhatt, R.S.; Wang, X.; Zhang, L.; Collins, M.; Signoretti, S.; Alsop, D.; Goldberg, S.N.; Atkins, M.B.; Mier, J.W. Renal cancer resistance to antiangiogenic therapy is delayed by restoration of angiostatic signaling. Mol. Cancer Ther. 2010, 9, 2793–2802. [Google Scholar] [CrossRef]
- Vasudev, N.S.; Goh, V.; Juttla, J.K.; Thompson, V.L.; Larkin, J.M.G.; Gore, M.; Nathan, P.D.; Reynolds, A.R. Changes in tumour vessel density upon treatment with anti-angiogenic agents: Relationship with response and resistance to therapy. Br. J. Cancer 2013, 109, 1230–1242. [Google Scholar] [CrossRef] [PubMed]
- Hahn, O.M.; Yang, C.; Medved, M.; Karczmar, G.; Kistner, E.; Karrison, T.; Manchen, E.; Mitchell, M.; Ratain, M.J.; Stadler, W.M. Dynamic contrast-enhanced magnetic resonance imaging pharmacodynamic biomarker study of sorafenib in metastatic renal carcinoma. J. Clin. Oncol. 2008, 26, 4572–4578. [Google Scholar] [CrossRef] [PubMed]
- Sweis, R.; Medved, M.; Towey, S.; Karczmar, G.S.; Oto, A.; Szmulewitz, R.Z.; O’Donnell, P.H.; Fishkin, P.; Karrison, T.; Stadler, W.M. Dynamic contrast-enhanced magnetic resonance imaging as a pharmacodynamic biomarker for pazopanib in metastatic renal carcinoma. Clin. Genitourin. Cancer 2017, 15, 207–212. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hudson, J.M.; Bailey, C.; Atri, M.; Stanisz, G.; Milot, L.; Williams, R.; Kiss, A.; Burns, P.N.; Bjarnason, G.A. The prognostic and predictive value of vascular response parameters measured by dynamic contrast-enhanced-CT, -MRI and -US in patients with metastatic renal cell carcinoma receiving sunitinib. Eur. Radiol. 2018, 28, 2281–2290. [Google Scholar] [CrossRef] [PubMed]
- Desar, I.; Ter Voert, E.; Hambrock, T.; Van Asten, J.; Van Spronsen, D.; Mulders, M.; Heerschap, A.; Van Der Graaf, W.; Van Laarhoven, H.; Van Herpen, C. Functional MRI techniques demonstrate early vascular changes in renal cell cancer patients treated with sunitinib: A pilot study. Cancer Imaging 2011, 11, 259–265. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.; Jackson, A.; Parker, G.; Roberts, C.; Jayson, G. Dynamic contrast-enhanced MRI in clinical trials of antivascular therapies. Nat. Rev. Clin. Oncol. 2012, 9, 167–177. [Google Scholar] [CrossRef]
- Akisik, M.F.; Sandrasegaran, K.; Bu, G.; Lin, C.; Hutchins, G.D.; Chiorean, E.G. Pancreatic cancer: Utility of dynamic contrast-enhanced MR Imaging in assessment of antiangiogenic therapy. Radiology 2010, 256, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Piludu, F.; Marzi, S.; Pace, A.; Villani, V.; Fabi, A.; Carapella, C.M.; Terrenato, I.; Antenucci, A.; Vidiri, A. Early biomarkers from dynamic contrast-enhanced magnetic resonance imaging to predict the response to antiangiogenic therapy in high-grade gliomas. Neuroradiology 2015, 57, 1269–1280. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Shen, Y.C.; Yu, C.W.; Hsu, C.; Hu, F.C.; Hsu, C.H.; Chen, B.-B.; Wei, S.-Y.; Cheng, A.-L.; Shih, T.T.-F. Dynamic contrast-enhanced magnetic resonance imaging biomarkers predict survival and response in hepatocellular carcinoma patients treated with sorafenib and metronomic tegafur/uracil. J. Hepatol. 2011, 55, 858–865. [Google Scholar] [CrossRef]
- Saito, K.; Ledsam, J.; Sugimoto, K.; Sourbron, S.; Araki, Y.; Tokuuye, K. DCE-MRI for early prediction of response in hepatocellular carcinoma after TACE and sorafenib therapy: A pilot study. J. Belg. Soc. Radiol. 2018, 102, 40. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Ding, Y.; Zhou, M.; Rini, B.I.; Petillo, D.; Qian, C.-N.; Kahnoski, R.; Futreal, P.A.; Furge, K.A.; Teh, B.T. Interleukin-8 mediates resistance to antiangiogenic agent sunitinib in renal cell carcinoma. Cancer Res. 2010, 70, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Fournier, L.; Bellucci, A.; Vano, Y.; Bouaboula, M.; Thibault, C.; Elaidi, R.; Oudard, S.; Cuenod, C. Imaging response of antiangiogenic and immune-oncology drugs in metastatic renal cell carcinoma (mRCC): Current status and future challenges. Kidney Cancer 2017, 1, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Braunagel, M.; Radler, E.; Ingrisch, M.; Staehler, M.; Schmid-Tannwald, C.; Rist, C.; Nikolaou, K.; Reiser, M.; Notohamiprodjo, M. Dynamic contrast-enhanced magnetic resonance imaging measurements in renal cell carcinoma: Effect of region of interest size and positioning on interobserver and intraobserver variability. Invest. Radiol. 2015, 50, 57–66. [Google Scholar] [CrossRef]
- Goh, V.; Halligan, S.; Gharpuray, A.; Wellsted, D.; Sundin, J.; Bartram, C.I. Quantitative assessment of colorectal cancer tumor vascular parameters by using perfusion CT: Influence of tumor region of interest. Radiology 2008, 247, 726–732. [Google Scholar] [CrossRef]
- Beuzit, L.; Eliat, P.-A.; Brun, V.; Ferré, J.; Gandon, Y.; Bannier, E.; Saint-Jalmes, H. Dynamic contrast-enhanced MRI: Study of inter-software accuracy and reproducibility using simulated and clinical data. J. Magn. Reson. Imaging 2015, 43, 1288–1300. [Google Scholar] [CrossRef] [PubMed]
- Heye, T.; Davenport, M.S.; Horvath, J.J.; Feuerlein, S.; Breault, S.R.; Bashir, M.R.; Merkle, E.M.; Boll, D.T. Reproducibility of dynamic contrast-enhanced MR Imaging. Part I. Perfusion characteristics in the female pelvis by using multiple computer-aided diagnosis perfusion analysis solutions. Radiology 2013, 266, 801–811. [Google Scholar] [CrossRef]
- Huang, W.; Li, X.; Chen, Y.; Li, X.; Chang, M.-C.; Oborski, M.J.; Malyarenko, D.I.; Muzi, M.; Jajamovich, G.H.; Fedorov, A.; et al. Variations of dynamic contrast-enhanced magnetic resonance imaging in evaluation of breast cancer therapy response: A multicenter data analysis challenge. Transl. Oncol. 2014, 7, 153–166. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Prior Nephrectomy | Sites of Disease/Index Lesions | Targeted Therapy | Progressive Disease at 6 Months |
|---|---|---|---|---|
| 1 | Yes | Nodal | Sunitinib | No |
| 2 | Yes | Spleen/Stomach | Sunitinib | No |
| 3 | Yes | Nodal | Sunitinib | No |
| 4 | Yes | Liver (2) | Sunitinib | Yes |
| 5 | Yes | Nodal | Sunitinib | Yes |
| 6 | No | Kidney | Sunitinib | No |
| 7 | No | Kidney | Pazopanib | No |
| 8 | No | Kidney | Sunitinib | No |
| 9 | No | Kidney | Pazopanib | No |
| 10 | Yes | Nephrectomy bed/Nodal | Sunitinib | No |
| 11 | Yes | Nodal (2) | Sunitinib | No |
| 12 | Yes | Kidney (2)/Liver/Pancreas (2) | Pazopanib | No |
| 13 | No | Kidney/Pancreas | Sunitinib | Yes |
| 14 | No | Kidney | Sunitinib | No |
| Authors [Reference] | Year | Number of Patients Included in Analysis | Anti-Angiogenic Therapy |
|---|---|---|---|
| Flaherty et al. [17] | 2008 | 15 | Sorafenib |
| Hahn et al. [24] | 2008 | 44 | Sorafenib |
| Sweis et al. [25] | 2017 | 17 | Pazopanib |
| Hudson et al. [26] | 2018 | 34 | Sunitinib |
| Desar et al. [27] | 2011 | 10 | Sunitinib |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhong, J.; Palkhi, E.; Buckley, D.L.; Collinson, F.J.; Ralph, C.; Jagdev, S.; Vasudev, N.S.; Swain, J.; Brown, J.E.; Wah, T.M. Feasibility Study on Using Dynamic Contrast Enhanced MRI to Assess the Effect of Tyrosine Kinase Inhibitor Therapy within the STAR Trial of Metastatic Renal Cell Cancer. Diagnostics 2021, 11, 1302. https://doi.org/10.3390/diagnostics11071302
Zhong J, Palkhi E, Buckley DL, Collinson FJ, Ralph C, Jagdev S, Vasudev NS, Swain J, Brown JE, Wah TM. Feasibility Study on Using Dynamic Contrast Enhanced MRI to Assess the Effect of Tyrosine Kinase Inhibitor Therapy within the STAR Trial of Metastatic Renal Cell Cancer. Diagnostics. 2021; 11(7):1302. https://doi.org/10.3390/diagnostics11071302
Chicago/Turabian StyleZhong, Jim, Ebrahim Palkhi, David L. Buckley, Fiona J. Collinson, Christy Ralph, Satinder Jagdev, Naveen S. Vasudev, Jayne Swain, Janet E. Brown, and Tze Min Wah. 2021. "Feasibility Study on Using Dynamic Contrast Enhanced MRI to Assess the Effect of Tyrosine Kinase Inhibitor Therapy within the STAR Trial of Metastatic Renal Cell Cancer" Diagnostics 11, no. 7: 1302. https://doi.org/10.3390/diagnostics11071302
APA StyleZhong, J., Palkhi, E., Buckley, D. L., Collinson, F. J., Ralph, C., Jagdev, S., Vasudev, N. S., Swain, J., Brown, J. E., & Wah, T. M. (2021). Feasibility Study on Using Dynamic Contrast Enhanced MRI to Assess the Effect of Tyrosine Kinase Inhibitor Therapy within the STAR Trial of Metastatic Renal Cell Cancer. Diagnostics, 11(7), 1302. https://doi.org/10.3390/diagnostics11071302