
The Influence of Pre-Procedural Imaging and Cystic Duct Cholangiography on Endoscopic Transpapillary Gallbladder Drainage in Acute Cholecystitis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
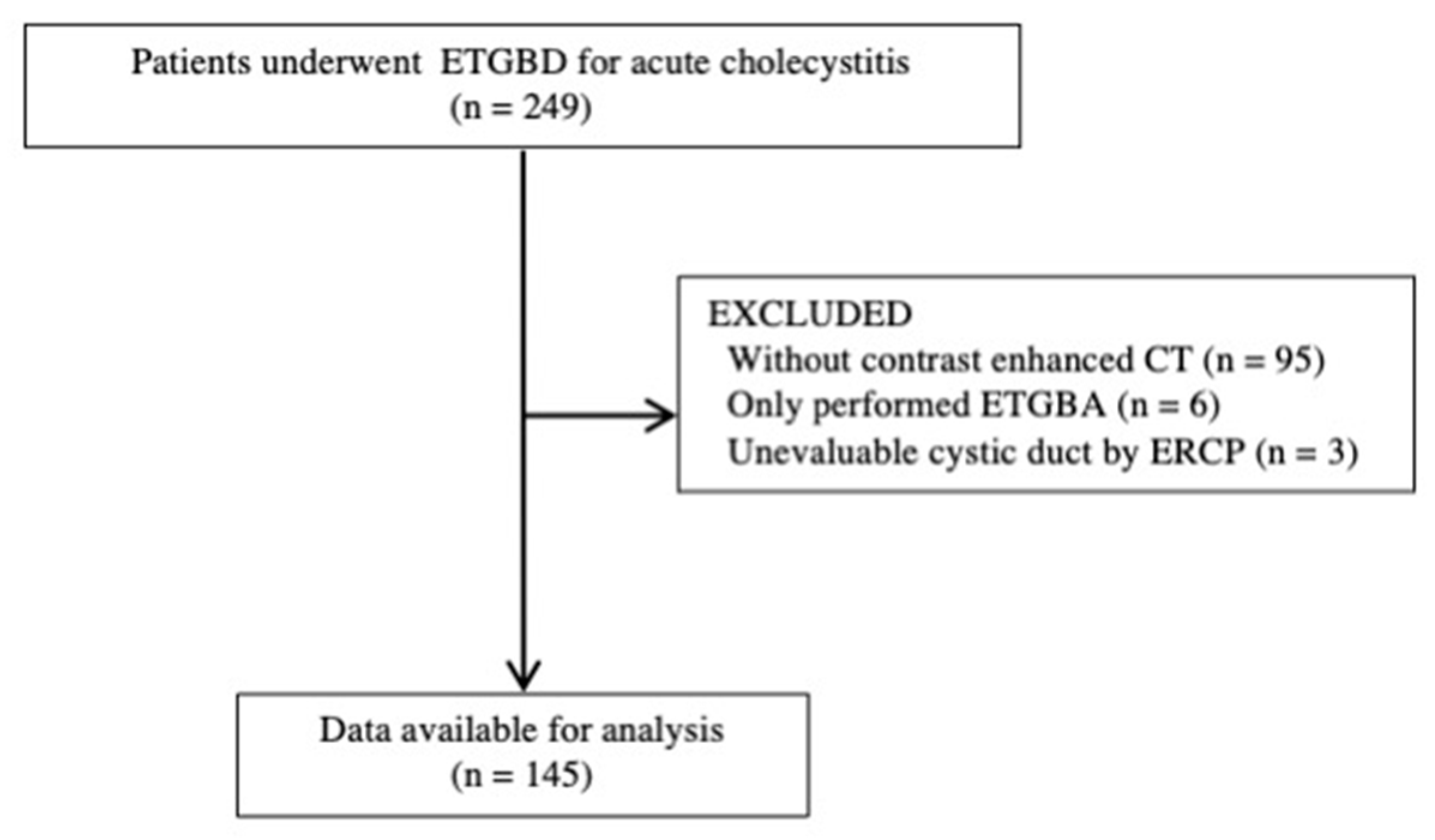
2.1. Patients
2.2. ETGBD Procedure
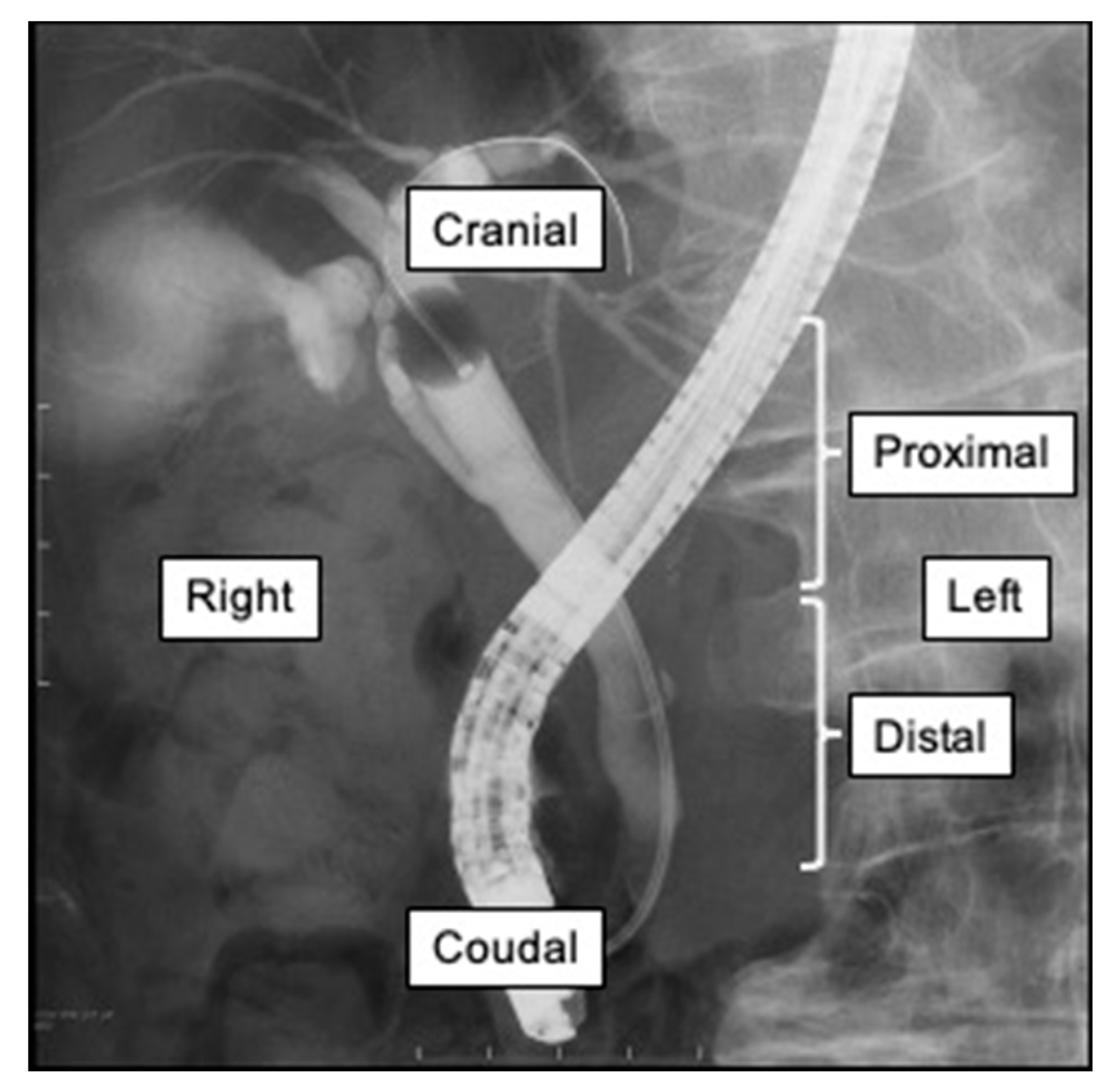
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Cholangiography and ERCP
3.3. Accuracy by CT and MRCP
3.4. Relationship between Pre-Procedural Images and ETGBD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CT | computed tomography |
| PTGBD | percutaneous transhepatic gallbladder drainage |
| ETGBD | endoscopic transpapillary gallbladder drainage |
| MRCP | magnetic resonance cholangiopancreatography |
| ERCP | endoscopic retrograde cholangiopancreatography |
| Fr | French |
| EGBS | endoscopic gallbladder stenting |
| EBS | endoscopic biliary stenting |
| ENBD | endoscopic nasobiliary drainage |
References
- Schmidt, M.; Dumot, J.A.; Søreide, O.; Søndenaa, K. Diagnosis and management of gallbladder calculus disease. Scand. J. Gastroenterol. 2012, 47, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Friedman, G.D.; Kannel, W.B.; Dawber, T.R. The epidemiology of gallbladder disease: Observations in the Framingham study. J. Chronic Dis. 1966, 19, 273–292. [Google Scholar] [CrossRef]
- Poddighe, D.; Tresoldi, M.; Licari, A.; Marseglia, G.L. Acalculous Acute Cholecystitis in Previously Healthy Children: General Overview and Analysis od Pediatric Infectious Cases. Int. J. Hepatol. 2015, 459608. [Google Scholar] [CrossRef] [PubMed]
- Eskelinen, M.; Ikonen, J.; Lipponen, P. Diagnostic Approaches in Acute Cholecystitis; a Prospective Study of 1333 Patients With Acute Abdominal Pain. Theor. Surg. 1993, 8, 15–20. [Google Scholar]
- Brewer, R.J.; Golden, G.T.; Hitch, D.C.; Rudolf, L.E.; Wangensteen, S.L. Abdominal pain: An analysis of 1000 consecutive cases in a university hospital emergency room. Am. J. Surg. 1976, 131, 219–223. [Google Scholar] [CrossRef]
- Telfer, S.; Fenyö, G.; Holt, P.; De Dombal, F.T. Acute abdominal pain in patients over 50 years of age. Scand. J. Gastroenterol. Suppl. 1988, 144, 47–50. [Google Scholar] [PubMed]
- Johansson, M.; Thune, A.; Nelvin, L.; Stiernstam, M.; Westman, B.; Lundell, L. Randomized clinical trial of open versus laparoscopic cholecystectomy in the treatment of acute cholecystitis. BJS 2004, 92, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Suzuki, K.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Endo, I.; Iwashita, Y.; Hibi, T.; Pitt, H.A.; Umezawa, A.; et al. Tokyo Guidelines 2018: Flowchart for the management of acute cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 55–72. [Google Scholar] [CrossRef] [PubMed]
- Itoi, T.; Sofuni, A.; Itokawa, F.; Tsuchiya, T.; Kurihara, T.; Ishii, K.; Tsuji, S.; Ikeuchi, N.; Tsukamoto, S.; Takeuchi, M.; et al. Endoscopic transpapillary gallbladder drainage in patients with acute cholecystitis in whom percutaneous transhepatic approach is contraindicated or anatomically impossible (with video). Gastrointest. Endosc. 2008, 68, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Itoi, T.; Baron, T.H.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Ukai, T.; Shikata, S.; Noguchi, Y.; Teoh, A.Y.B.; et al. Tokyo Guidelines 2018: Management strategies for gallbladder drainage in patients with acute cholecystitis (with videos). J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Itoi, T.; Coelho-Prabhu, N.; Baron, T.H. Endoscopic gallbladder drainage for management of acute cholecystitis. Gastrointest. Endosc. 2010, 71, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, K.; Michikawa, Y.; Morita, R.; Suetani, K.; Morita, N.; Sato, J.; Tsuji, K.; Ikeda, H.; Matsunaga, K.; Watanabe, T.; et al. Endoscopic transpapillary gallbladder stenting using a newly designed plastic stent for acute cholecystitis. Endosc. Int. Open 2019, 7, E1105–E1114. [Google Scholar] [CrossRef] [PubMed]
- Yokoe, M.; Hata, J.; Takada, T.; Strasberg, S.M.; Bun, T.A.Y.; Wakabayashi, G.; Kozaka, K.; Endo, I.; DeZiel, D.J.; Miura, F.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholecystitis (with videos). J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Endo, I.; Takada, T.; Hwang, T.-L.; Akazawa, K.; Mori, R.; Miura, F.; Yokoe, M.; Itoi, T.; Gomi, H.; Chen, M.-F.; et al. Optimal treatment strategy for acute cholecystitis based on predictive factors: Japan-Taiwan multicenter cohort study. J. Hepato-Biliary-Pancreat. Sci. 2017, 24, 346–361. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, J.; Chijiiwa, K.; Yamaguchi, K.; Yokohata, K.; Tanaka, M. Practical Classification of the Branching Types of the Bili-ary Tree: An Analysis of 1,094 Consecutive Direct Cholangiograms. J. Am. Coll. Surg. 1996, 182, 37–40. [Google Scholar] [PubMed]
- Maruta, A.; Iwata, K.; Iwashita, T.; Yoshida, K.; Ando, N.; Toda, K.; Mukai, T.; Shimizu, M. Factors affecting technical success of endoscopic transpapillary gallbladder drainage for acute cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2020, 27, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.; Tannheimer, M.; Danz, B.; Benesch, S.; Geue, R. Clinical Relevance of a Routinely Performed Magnetic Reso-nance Cholangiopancreatography (MRCP) Prior to Cholecystectomy. Zentralbl. Chir. 2012, 137, 541–548. [Google Scholar] [PubMed]
- Cao, J.; Ding, X.; Wu, H.; Shen, Y.; Zheng, R.; Peng, C.; Wang, L.; Zou, X. Classification of the Cystic Duct Patterns and En-doscopic Transpapillary Cannulation of the Gallbladder to Prevent Post-ERCP Cholecystitis. BMC Gastroenterol. 2019, 19, 139. [Google Scholar] [CrossRef] [PubMed]
- Yane, K.; Maguchi, H.; Katanuma, A.; Takahashi, K.; Osanai, M.; Kin, T.; Takaki, R.; Matsumoto, K.; Gon, K.; Matsumori, T.; et al. Feasibility, Efficacy, and Predictive Factors for the Technical Success of Endoscopic Nasogallblad-der Drainage: A Prospective Study. Gut Liver 2015, 9, 239–246. [Google Scholar] [CrossRef] [PubMed][Green Version]



{kind=link}
{kind=link}
| Characteristic | n = 145 |
|---|---|
| Male:Female | 76:69 |
| Median age, years (range) | 77 (12–96) |
| Couse of cholecystitis | |
| Gallstone | 119 (82%) |
| Metal stent | 6 (4%) |
| Malignant obstruction | 8 (6%) |
| Other | 12 (8%) |
| Severity of cholecystitis | |
| Mild | 69 (48%) |
| Moderate | 55 (38%) |
| Severe | 21 (14%) |
| Pre-ERCP images | |
| Contrast-enhanced CT | 145 (100%) |
| MRCP | 29 (20%) |
| Stone impaction | |
| In cystic duct | 17 (12%) |
| In gall neck | 21 (14%) |
| CBD stones | 46 (32%) |
| n = 145 | |
|---|---|
| Contrast on cholangiography | |
| without contrast | 85 (59%) |
| Only cystic duct contrast | 31 (21%) |
| Cystic duct and gallbladder contrast | 29 (20%) |
| Cystic duct direction and location | |
| Proximal/distal | 114/31 |
| Right/left | 101/44 |
| Cranial/caudal | 141/4 |
| Procedure time, min (range) | 50 (13–129) |
| Technical success | 127/145 (88%) |
| Cystic duct injury | 16 (11%) |
| Injury by guidewire | 11 (8%) |
| Injury by cannula | 5 (3%) |
| CT n = 145 | MRCP n = 31 | |
|---|---|---|
| Proximal or distal, n (%) | 114/145 (79) | 21/31 (68) |
| Right or left, n (%) | 87/145 (60) | 17/31 (55) |
| Cranial or caudal, n (%) | 84/145 (58) | 18/31 (58) |
| Presence of the Factor | ||||
|---|---|---|---|---|
| Factor | Yes | No | p-Value | |
| Procedure time, min (range) | with gallbladder contrast | 43 (13–93) | 53 (19–129) | 0.023 |
| proximal cystic duct branch | 53 (13–129) | 43 (21–96) | 0.050 | |
| right cystic duct branch | 50 (13–129) | 50 (20–100) | 0.40 | |
| cranial cystic duct branch | 77 (47–125) | 50 (13–129) | 0.073 | |
| Technical success of ETGBD, n (%) | with gallbladder contrast | 27/29 (93) | 100/116 (86) | 0.53 |
| proximal cystic duct branch | 101/114 (89) | 26/31 (84) | 0.54 | |
| right cystic duct branch | 87/101 (86) | 40/44 (91) | 0.59 | |
| cranial cystic duct branch | 125/141 (89) | 2/4 (50) | 0.075 | |
| Cystic duct injury, n (%) | with gallbladder contrast | 0/29 (0) | 16/116 (14) | 0.042 |
| proximal cystic duct branch | 10/114 (9) | 6/31 (19) | 0.11 | |
| right cystic duct branch | 11/101 (11) | 5/44 (11) | 1.0 | |
| cranial cystic duct branch | 15/141 (11) | 1/4 (25) | 0.38 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, J.; Nakahara, K.; Michikawa, Y.; Morita, R.; Suetani, K.; Sekine, A.; Igarashi, Y.; Kobayashi, S.; Otsubo, T.; Itoh, F. The Influence of Pre-Procedural Imaging and Cystic Duct Cholangiography on Endoscopic Transpapillary Gallbladder Drainage in Acute Cholecystitis. Diagnostics 2021, 11, 1286. https://doi.org/10.3390/diagnostics11071286
Sato J, Nakahara K, Michikawa Y, Morita R, Suetani K, Sekine A, Igarashi Y, Kobayashi S, Otsubo T, Itoh F. The Influence of Pre-Procedural Imaging and Cystic Duct Cholangiography on Endoscopic Transpapillary Gallbladder Drainage in Acute Cholecystitis. Diagnostics. 2021; 11(7):1286. https://doi.org/10.3390/diagnostics11071286
Chicago/Turabian StyleSato, Junya, Kazunari Nakahara, Yosuke Michikawa, Ryo Morita, Keigo Suetani, Akihiro Sekine, Yosuke Igarashi, Shinjiro Kobayashi, Takehito Otsubo, and Fumio Itoh. 2021. "The Influence of Pre-Procedural Imaging and Cystic Duct Cholangiography on Endoscopic Transpapillary Gallbladder Drainage in Acute Cholecystitis" Diagnostics 11, no. 7: 1286. https://doi.org/10.3390/diagnostics11071286
APA StyleSato, J., Nakahara, K., Michikawa, Y., Morita, R., Suetani, K., Sekine, A., Igarashi, Y., Kobayashi, S., Otsubo, T., & Itoh, F. (2021). The Influence of Pre-Procedural Imaging and Cystic Duct Cholangiography on Endoscopic Transpapillary Gallbladder Drainage in Acute Cholecystitis. Diagnostics, 11(7), 1286. https://doi.org/10.3390/diagnostics11071286