
Dynapenia Rather Than Sarcopenia Is Associated with Metabolic Syndrome in Patients with Chronic Liver Diseases

Abstract
:1. Introduction
2. Patients and Methods
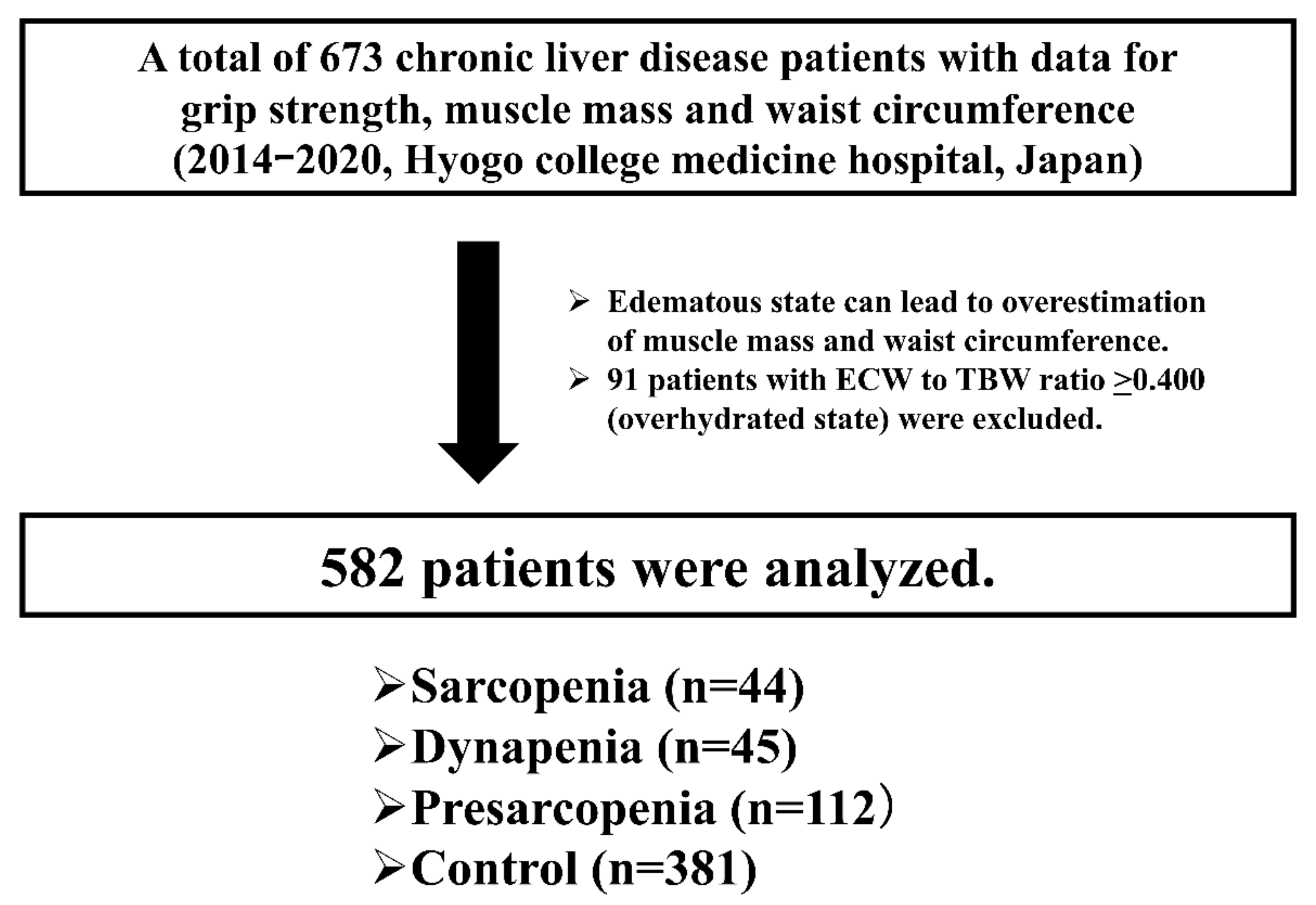
2.1. Patients
2.2. Definition of Met-S
2.3. Measurement of GS and SMI and Our Study
2.4. Statistical Considerations
3. Results
3.1. Patient Baseline Characteristics
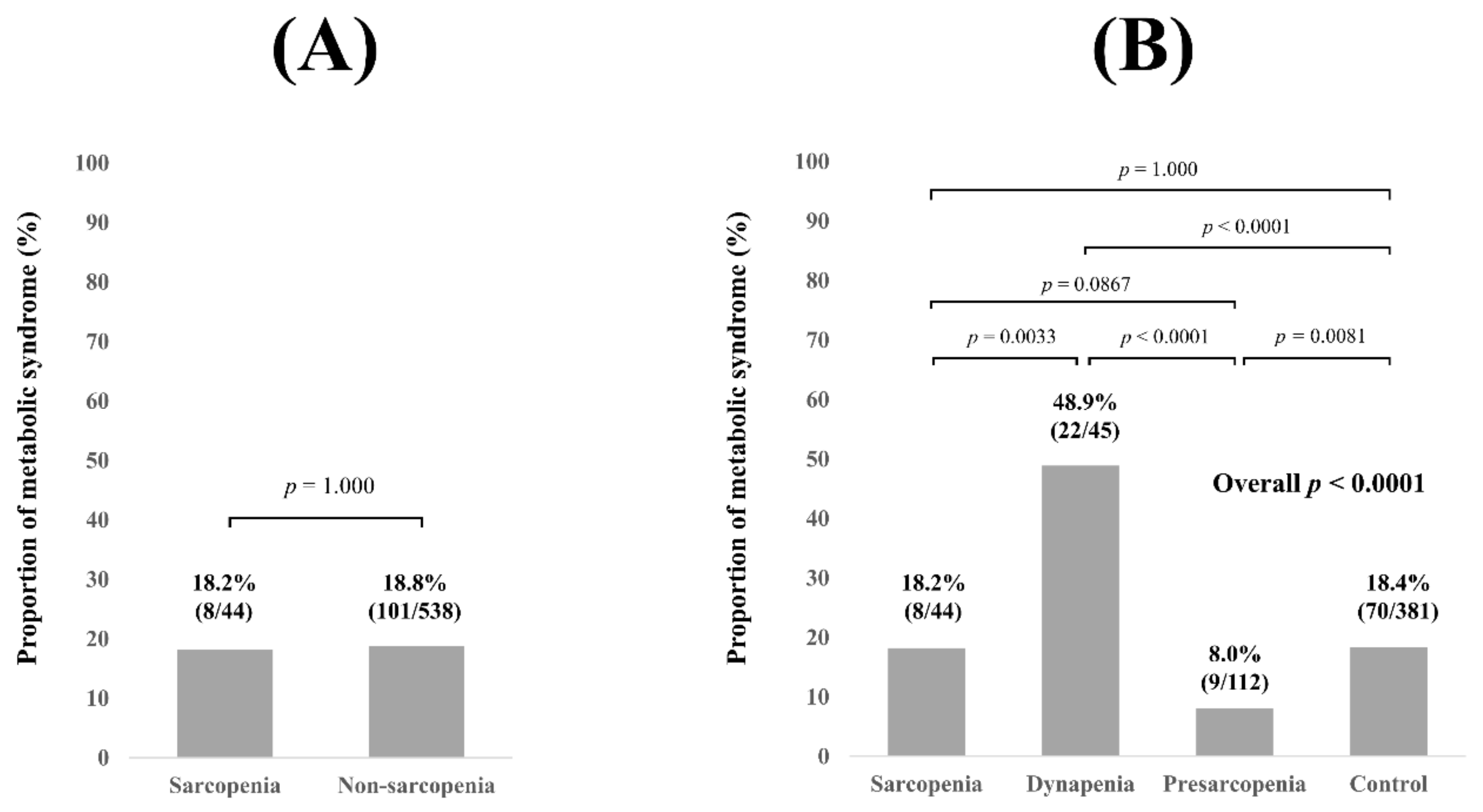
3.2. Proportion of Met-S for All Cases Stratified by GS and SMI
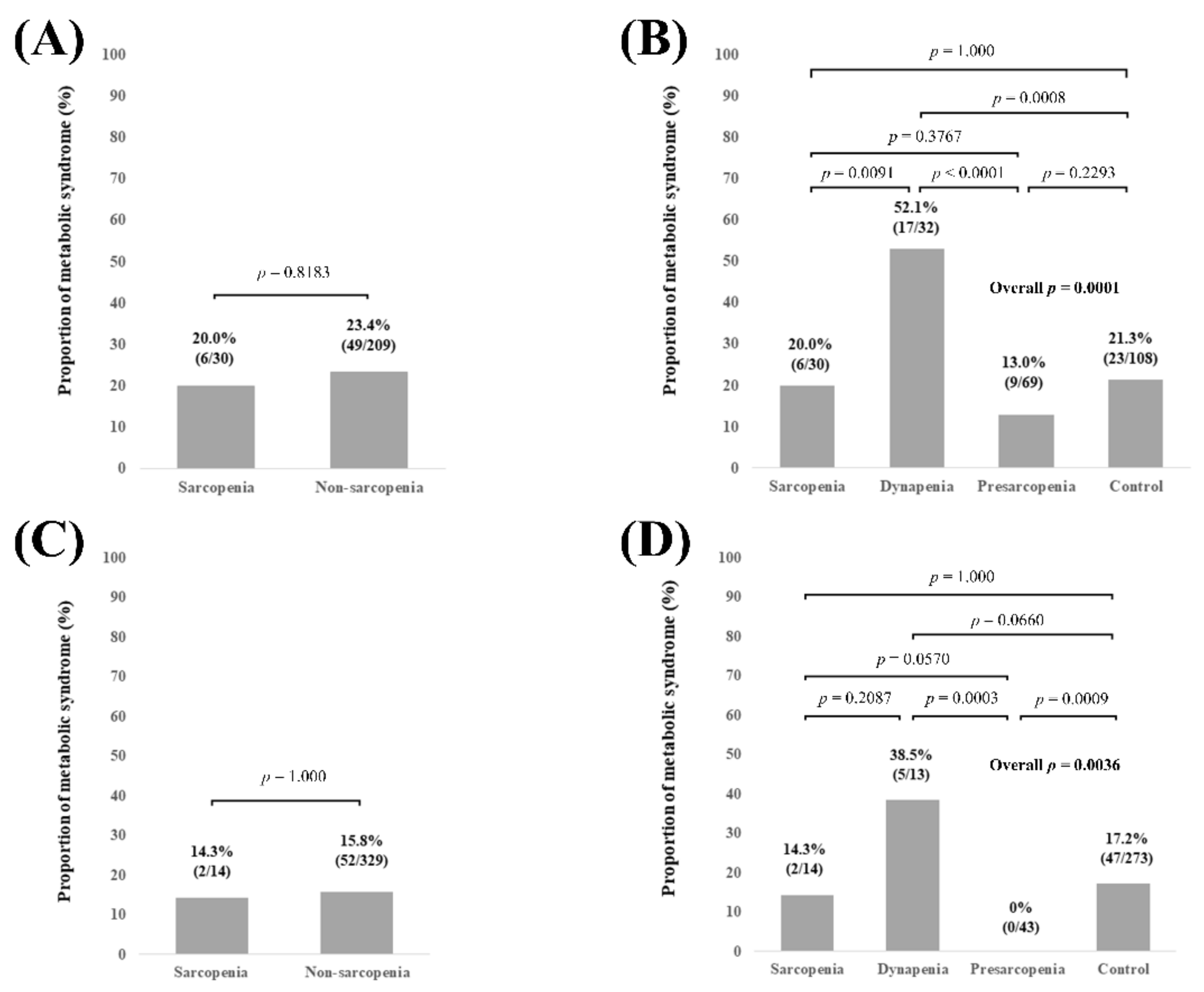
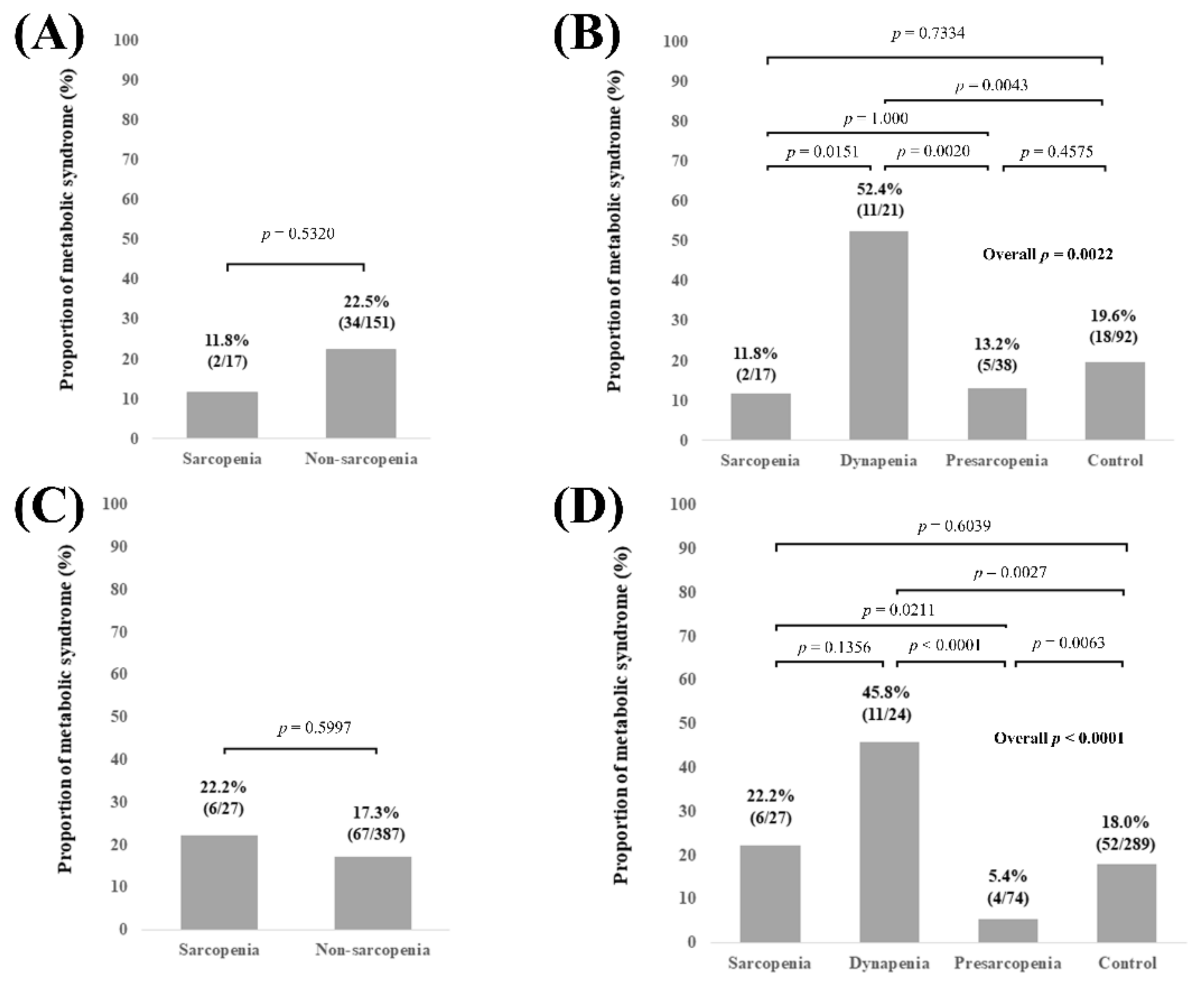
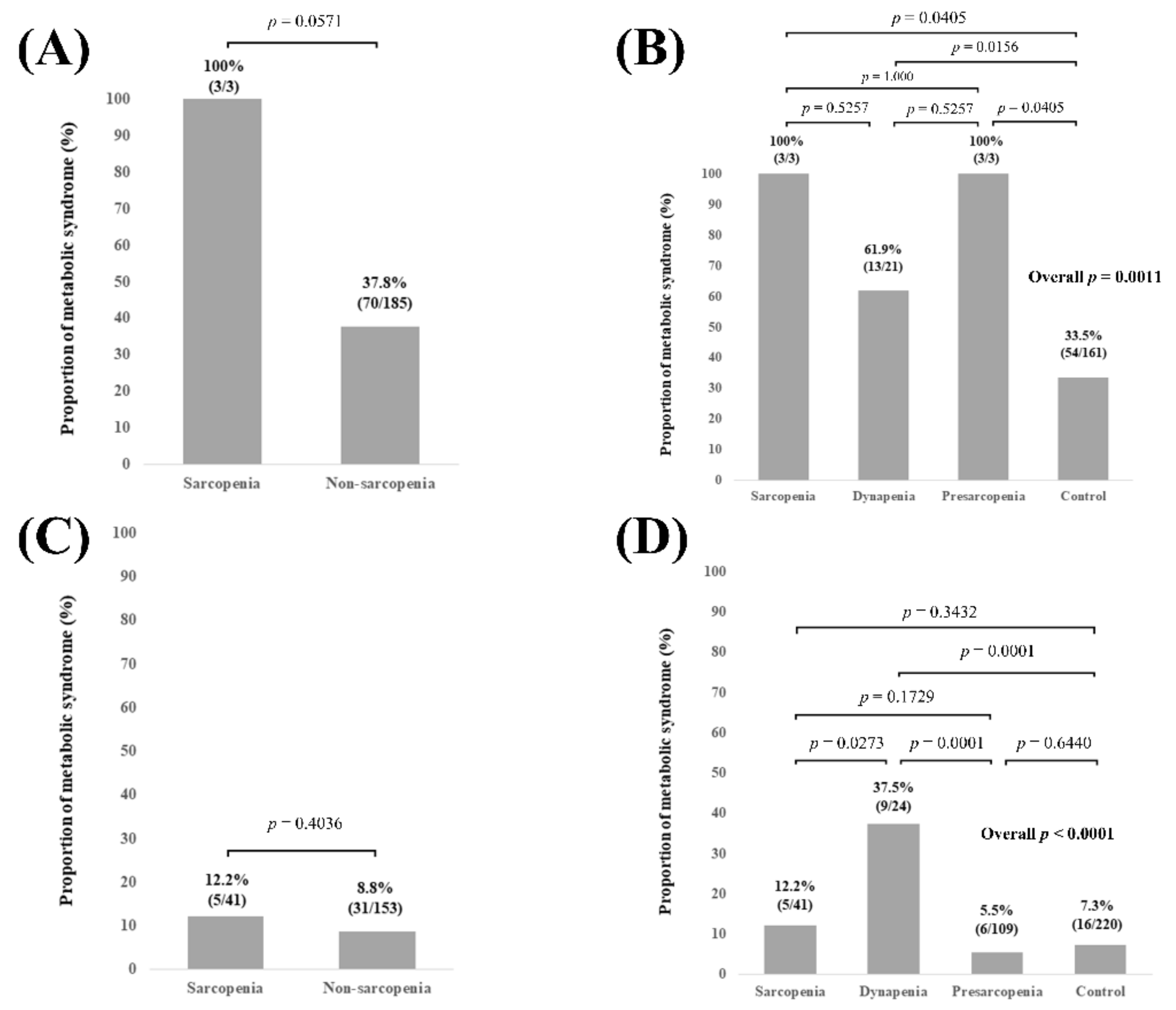
3.3. Subgroup Analysis 1: Proportion of MetS Stratified by GS and SMI According to the LC Status
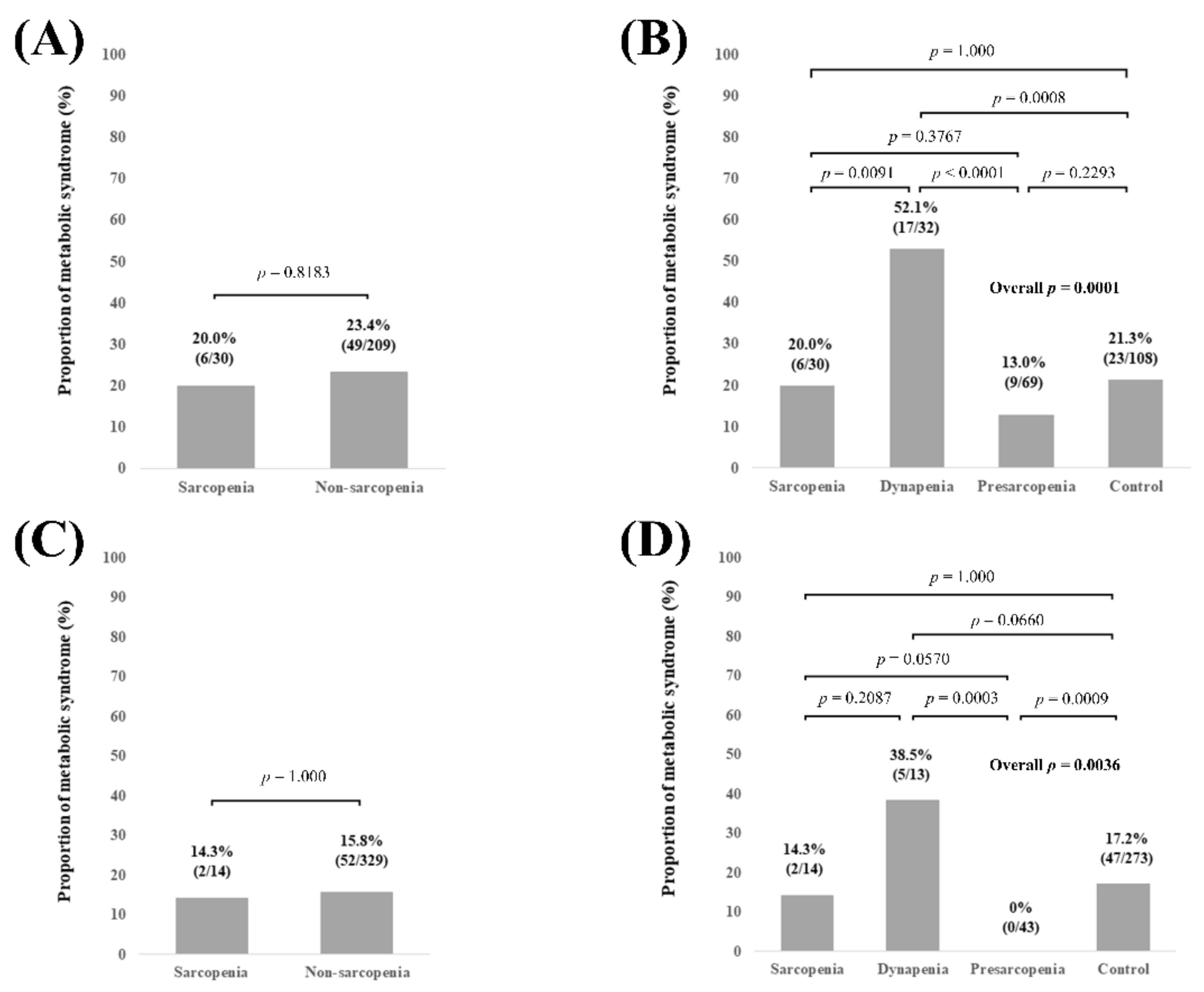
3.4. Subgroup Analysis 2: Proportion of Met-S Stratified by GS and SMI According to Age
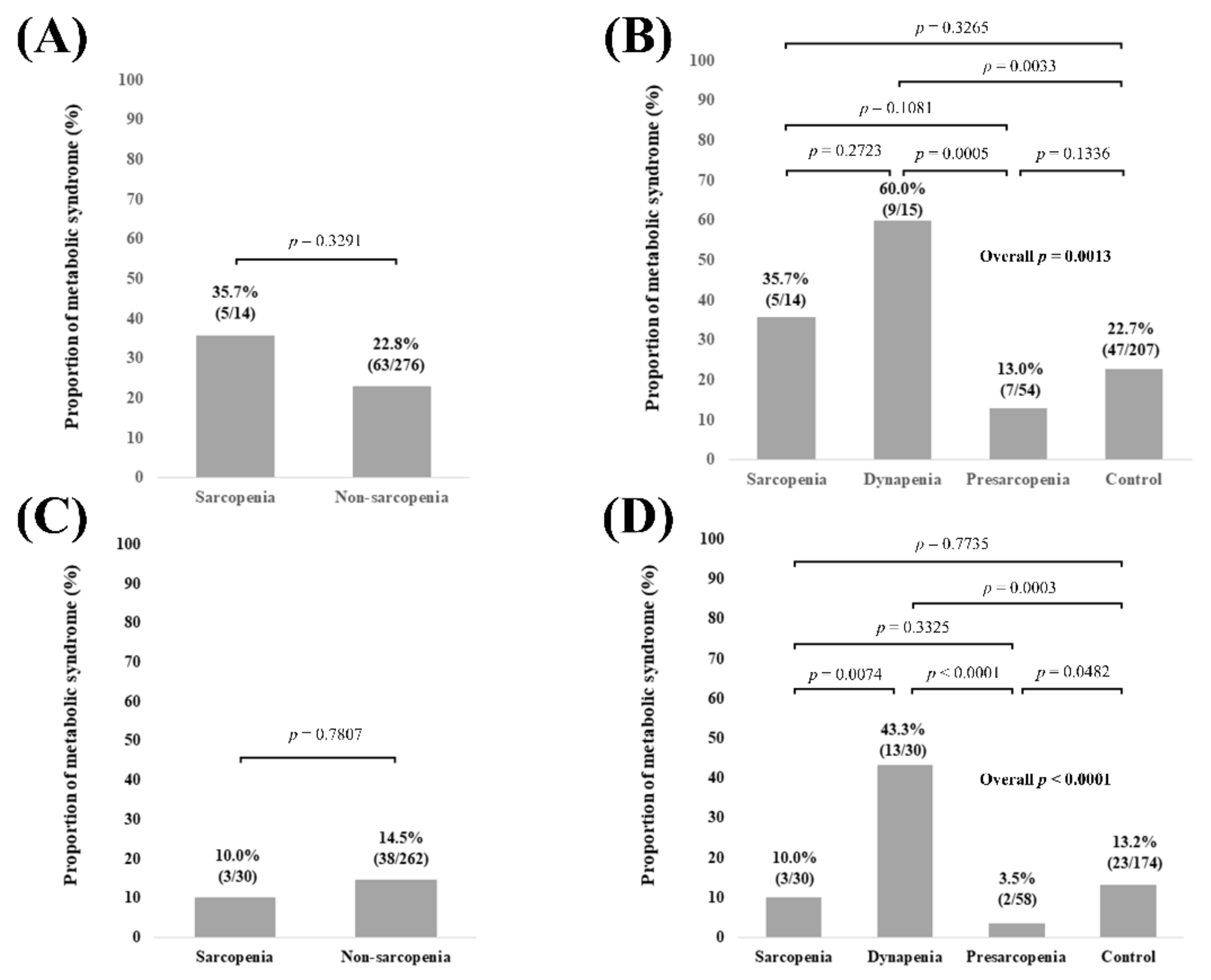
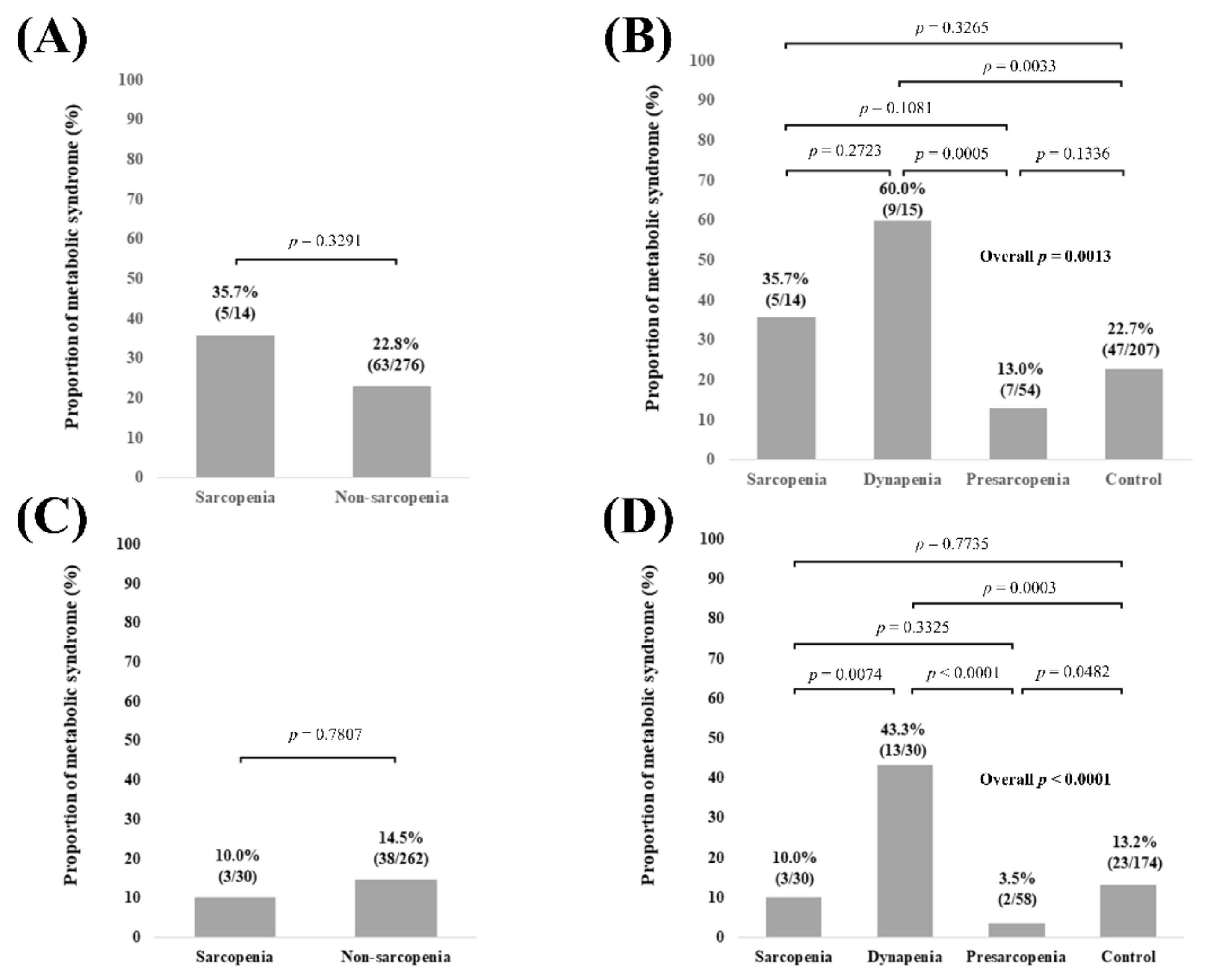
3.5. Subgroup Analysis 3: Proportion of Met-S Stratified by GS and SMI According to Gender
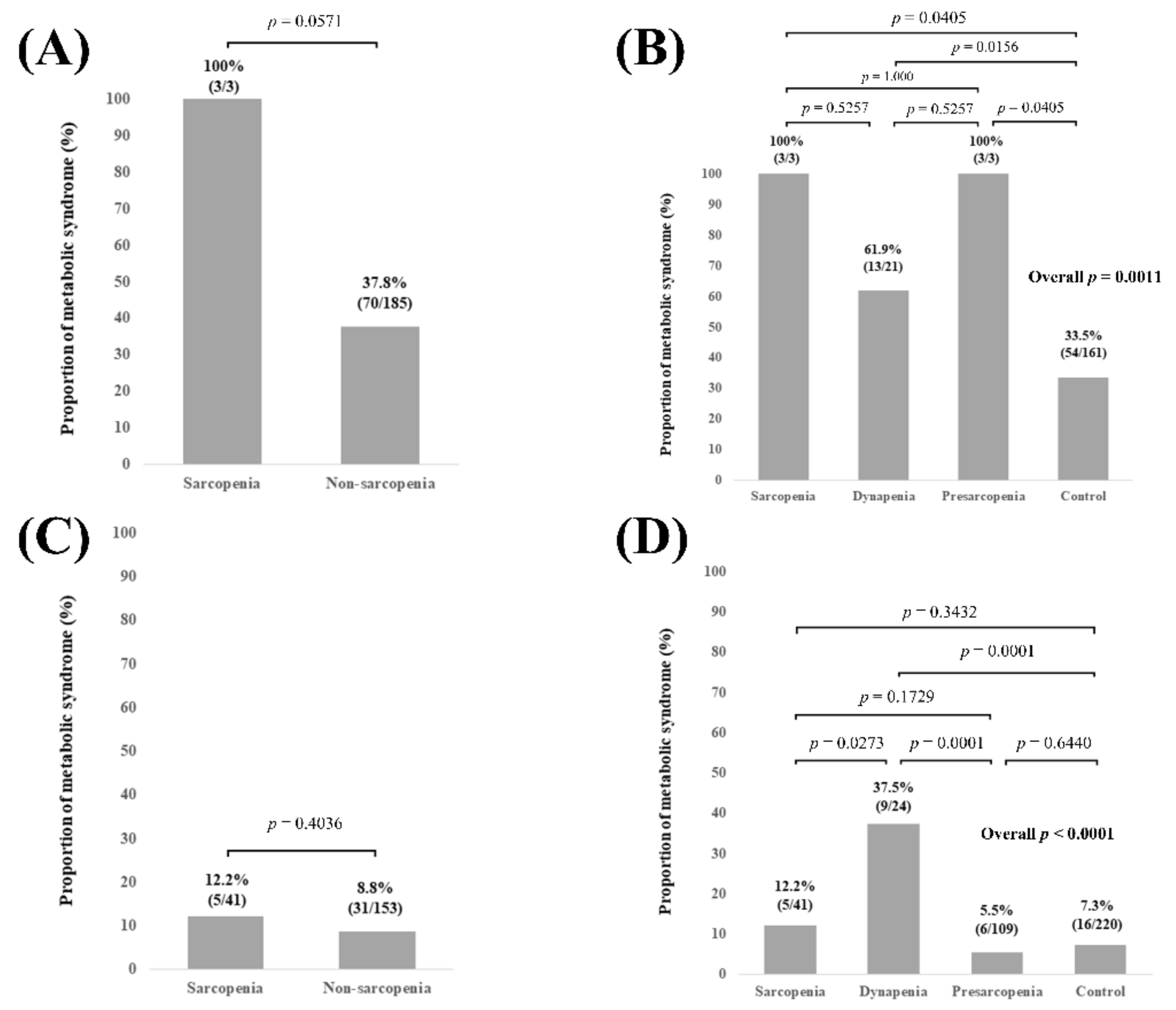
3.6. Subgroup Analysis 4: Proportion of Met-S Stratified by GS and SMI According to BMI
3.7. Univariate and Multivariate Analyses of Factors Associated with the Presence of Mets
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ohashi, K.; Ishikawa, T.; Hoshi, A.; Suzuki, M.; Mitobe, Y.; Yamada, E.; Abeywickrama, H.M.; Seki, N.; Koyama, C.; Aoki, H.; et al. Relationship Between Sarcopenia and Both Physical Activity and Lifestyle in Patients with Chronic Liver Disease. J. Clin. Med. Res. 2018, 10, 920–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, M.; Abe, K.; Fujita, M.; Okai, K.; Takahashi, A.; Ohira, H. Association between sarcopenia and osteoporosis in chronic liver disease. Hepatol. Res. 2018, 48, 893–904. [Google Scholar] [CrossRef]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- Hsu, C.S.; Kao, J.H. Sarcopenia and chronic liver diseases. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 1229–1244. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Nishiguchi, S.; Iijima, H. Liver Cirrhosis and Sarcopenia from the Viewpoint of Dysbiosis. Int. J. Mol. Sci. 2020, 21, 5254. [Google Scholar] [CrossRef]
- Bunchorntavakul, C.; Reddy, K.R. Review article: Malnutrition/sarcopenia and frailty in patients with cirrhosis. Aliment. Pharmacol. Ther. 2020, 51, 64–77. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; Nishimura, T.; et al. Elevated serum myostatin level is associated with worse survival in patients with liver cirrhosis. J. Cachexia Sarcopenia Muscle 2017, 8, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Budui, S.L.; Rossi, A.P.; Zamboni, M. The pathogenetic bases of sarcopenia. Clin. Cases Miner. Bone Metab. 2015, 12, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Otten, L. Financial impact of sarcopenia or low muscle mass-A short review. Clin. Nutr. 2019, 38, 1489–1495. [Google Scholar] [CrossRef]
- Yki-Järvinen, H. Non-alcoholic fatty liver disease as a cause and a consequence of metabolic syndrome. Lancet Diabetes Endocrinol. 2014, 2, 901–910. [Google Scholar] [CrossRef]
- Merli, M.; Lattanzi, B.; Aprile, F. Sarcopenic obesity in fatty liver. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 185–190. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Godoy-Matos, A.F.; Silva Júnior, W.S.; Valerio, C.M. NAFLD as a continuum: From obesity to metabolic syndrome and diabetes. Diabetol. Metab. Syndr. 2020, 12, 60. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, K.A.; Petrick, J.L.; London, W.T. Global epidemiology of hepatocellular carcinoma: An emphasis on demographic and regional variability. Clin. Liver Dis. 2015, 19, 223–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jinjuvadia, R.; Patel, S.; Liangpunsakul, S. The association between metabolic syndrome and hepatocellular carcinoma: Systemic review and meta-analysis. J. Clin. Gastroenterol. 2014, 48, 172–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wedell-Neergaard, A.S.; Lang, L.L.; Christensen, R.H.; Legaard, G.E.; Dorph, E.; Larsen, M.K.; Launbo, N.; Fagerlind, S.R.; Seide, S.K.; Nymand, S.; et al. Exercise-Induced Changes in Visceral Adipose Tissue Mass Are Regulated by IL-6 Signaling: A Randomized Controlled Trial. Cell Metab. 2019, 29, 844–855.e3. [Google Scholar] [CrossRef]
- Jorge, A.S.B.; Andrade, J.M.O.; Paraíso, A.F.; Jorge, G.C.B.; Silveira, C.M.; de Souza, L.R.; Santos, E.P.; Guimaraes, A.L.S.; Santos, S.H.S.; De Paula, A.M.B. Body mass index and the visceral adipose tissue expression of IL-6 and TNF-alpha are associated with the morphological severity of non-alcoholic fatty liver disease in individuals with class III obesity. Obes. Res. Clin. Pract. 2018, 12 (Suppl. 1), 1–8. [Google Scholar] [CrossRef]
- Rinaldi, L.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Morone, M.V.; Silvestri, C.; Giordano, M.; Salvatore, T.; Sasso, F.C. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrative Review. Antioxidants 2021, 10, 270. [Google Scholar]
- Choudhary, N.S.; Saigal, S.; Saraf, N.; Mohanka, R.; Rastogi, A.; Goja, S.; Menon, P.B.; Mishra, S.; Mittal, A.; Soin, A.S. Sarcopenic obesity with metabolic syndrome: A newly recognized entity following living donor liver transplantation. Clin. Transplant. 2015, 29, 211–215. [Google Scholar] [CrossRef]
- Seror, M.; Sartoris, R.; Hobeika, C.; Bouattour, M.; Paradis, V.; Rautou, P.E.; Soubrane, O.; Vilgrain, V.; Cauchy, F.; Ronot, M. Computed Tomography-Derived Liver Surface Nodularity and Sarcopenia as Prognostic Factors in Patients with Resectable Metabolic Syndrome-Related Hepatocellular Carcinoma. Ann. Surg. Oncol. 2020. [Google Scholar] [CrossRef]
- Enomoto, H.; Ueno, Y.; Hiasa, Y.; Nishikawa, H.; Hige, S.; Takikawa, Y.; Taniai, M.; Ishikawa, T.; Yasui, K.; Takaki, A.; et al. Transition in the etiology of liver cirrhosis in Japan: A nationwide survey. J. Gastroenterol. 2020, 55, 353–362. [Google Scholar]
- Drafting Committee for Hepatitis Management Guidelines, the Japan Society of Hepatology. Japan Society of Hepatology guidelines for the management of hepatitis C virus infection: 2019 update. Hepatol. Res. 2020, 50, 791–816. [Google Scholar] [CrossRef] [PubMed]
- Drafting Committee for Hepatitis Management Guidelines, the Japan Society of Hepatology. Japan Society of Hepatology Guidelines for the Management of Hepatitis B Virus Infection: 2019 update. Hepatol. Res. 2020, 50, 892–923. [Google Scholar] [CrossRef]
- Chumlea, W.C.; Schubert, C.M.; Sun, S.S.; Demerath, E.; Towne, B.; Siervogel, R.M. A review of body water status and the effects of age and body fatness in children and adults. J. Nutr. Health Aging 2007, 11, 111–118. [Google Scholar]
- McManus, M.L.; Churchwell, K.B.; Strange, K. Regulation of cell volume in health and disease. N. Engl. J. Med. 1995, 333, 1260–1266. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar]
- Nishikawa, H.; Yoh, K.; Enomoto, H.; Ishii, N.; Iwata, Y.; Nakano, C.; Takata, R.; Nishimura, T.; Aizawa, N.; Sakai, Y.; et al. Extracellular Water to Total Body Water Ratio in Viral Liver Diseases: A Study Using Bioimpedance Analysis. Nutrients 2018, 10, 1072. [Google Scholar] [CrossRef] [Green Version]
- Yamagishi, K.; Iso, H. The criteria for metabolic syndrome and the national health screening and education system in Japan. Epidemiol. Health 2017, 39, e2017003. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.C.; Manini, T.M. What is dynapenia? Nutrition 2012, 28, 495–503. [Google Scholar] [CrossRef] [Green Version]
- Dabke, K.; Hendrick, G.; Devkota, S. The gut microbiome and metabolic syndrome. J. Clin. Investig. 2019, 129, 4050–4057. [Google Scholar] [CrossRef]
- Ren, H.; Wang, J.; Gao, Y.; Yang, F.; Huang, W. Metabolic syndrome and liver-related events: A systematic review and meta-analysis. BMC Endocr. Disord. 2019, 19, 40. [Google Scholar] [CrossRef]
- Sénéchal, M.; Dionne, I.J.; Brochu, M. Dynapenic abdominal obesity and metabolic risk factors in adults 50 years of age and older. J. Aging Health 2012, 24, 812–826. [Google Scholar] [CrossRef]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Hara, N.; Moriya, K.; Hino, K.; Koike, K. Reduced Handgrip Strength Predicts Poorer Survival in Chronic Liver Diseases: A Large Multi-Center Study in Japan. Hepatol. Res. 2021. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar]
- García-Hermoso, A.; Ramírez-Vélez, R.; Peterson, M.D.; Lobelo, F.; Cavero-Redondo, I.; Correa-Bautista, J.E.; Martínez-Vizcaíno, V. Handgrip and knee extension strength as predictors of cancer mortality: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2018, 28, 1852–1858. [Google Scholar] [CrossRef]
- Yoh, K.; Nishikawa, H.; Enomoto, H.; Iwata, Y.; Ikeda, N.; Aizawa, N.; Nishimura, T.; Iijima, H.; Nishiguchi, S. Grip Strength: A Useful Marker for Composite Hepatic Events in Patients with Chronic Liver Diseases. Diagnostics 2020, 10, 238. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Nishio, N.; Abe, Y.; Kakehi, T.; Fujimoto, J.; Tanaka, T.; Ohji, S.; Otobe, Y.; et al. Differential characteristics of skeletal muscle in community-dwelling older adults. J. Am. Med. Dir. Assoc. 2017, 18, 807.e9–807.e16. [Google Scholar] [CrossRef]
- Yang, M.; Ding, X.; Luo, L.; Hao, Q.; Dong, B. Disability associated with obesity, dynapenia and dynapenic-obesity in Chinese older adults. J. Am. Med. Dir. Assoc. 2014, 15, 150.e11–150.e16. [Google Scholar] [CrossRef]
- Rossi, A.P.; Fantin, F.; Caliari, C.; Zoico, E.; Mazzali, G.; Zanardo, M.; Bertassello, P.; Zanandrea, V.; Micciolo, R.; Zamboni, M. Dynapenic abdominal obesity as predictor of mortality and disability worsening in older adults: A 10-year prospective study. Clin. Nutr. 2016, 35, 199–204. [Google Scholar] [CrossRef]
- Wu, H.; Ballantyne, C.M. Skeletal muscle inflammation and insulin resistance in obesity. J. Clin. Investig. 2017, 127, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Kuroda, A.; Ishizu, M.; Ohishi, M.; Takashi, Y.; Otsuka, Y.; Taniguchi, S.; Tamaki, M.; Kurahashi, K.; Yoshida, S.; et al. Association of accumulated advanced glycation end-products with a high prevalence of sarcopenia and dynapenia in patients with type 2 diabetes. J. Diabetes Investig. 2019, 10, 1332–1340. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Cases (n = 582) | Sarcopenia (n = 44) | Dynapenia (n = 45) | Presarcopenia (n = 112) | Control (n = 381) |
|---|---|---|---|---|---|
| Age (years) | 59.5 ± 12.6 | 66.4 ± 11.9 | 67.6 ± 9.1 | 64.8 ± 11.4 | 56.2 ± 12.1 |
| Gender, male/female | 290/292 | 14/30 | 15/30 | 54/58 | 207/174 |
| Liver disease etiologyHBV/HCV/others | 89/255/238 | 5/12/17 | 4/23/18 | 19/56/37 | 61/154/166 |
| Presence of LC, yes/no | 168/414 | 17/27 | 21/24 | 38/74 | 92/289 |
| Body mass index (kg/m2) | 23.7 ± 4.1 | 20.8 ± 1.8 | 25.0 ± 2.6 | 20.1 ± 2.1 | 24.9 ± 4.1 |
| Grip strength (kg), male | 35.8 ± 7.6 | 24.0 ± 1.7 | 21.9 ± 4.9 | 31.8 ± 4.5 | 38.6 ± 6.1 |
| Grip strength (kg), female | 22.1 ± 5.1 | 15.2 ± 2.9 | 15.7 ± 2.9 | 21.8 ± 2.4 | 24.4 ± 4.3 |
| Skeletal muscle index (kg/m2), male | 7.6 ± 0.8 | 6.4 ± 0.4 | 7.7 ± 0.5 | 6.5 ± 0.3 | 8.0 ± 0.7 |
| Skeletal muscle index (kg/m2), female | 6.1 ± 0.8 | 5.2 ± 0.4 | 6.3 ± 0.6 | 5.3 ± 0.3 | 6.5 ± 0.6 |
| Waist circumference (cm), male | 90.1 ± 9.8 | 84.5 ± 5.4 | 93.6 ± 5.4 | 82.7 ± 7.0 | 92.2 ± 9.8 |
| Waist circumference (cm), female | 86.5 ± 11.5 | 81.0 ± 7.2 | 92.4 ± 9.3 | 77.9 ± 7.4 | 89.3 ± 11.7 |
| ECW to TBW ratio | 0.386 ± 0.007 | 0.392 ± 0.005 | 0.390 ± 0.006 | 0.389 ± 0.005 | 0.385 ± 0.007 |
| Total bilirubin (mg/dL) | 0.9 ± 0.6 | 0.8 ± 0.4 | 1.0 ± 0.6 | 0.9 ± 0.4 | 0.9 ± 0.6 |
| Serum albumin (g/dL) | 4.2 ± 0.4 | 4.0 ± 0.6 | 4.0 ± 0.4 | 4.2 ± 0.4 | 4.2 ± 0.4 |
| Prothrombin time (INR) | 1.06 ± 0.13 | 1.08 ± 0.12 | 1.09 ± 0.10 | 1.07 ± 0.18 | 1.05 ± 0.12 |
| Platelet count (×104/mm3) | 18.7 ± 7.6 | 16.5 ± 7.0 | 15.1 ± 6.5 | 17.8 ± 7.4 | 19.6 ± 7.7 |
| Hypertriglyceridemia (≥150 mg/dL) and/or low HDL (<40 mg/dL), yes/no | 198/384 | 23/21 | 24/21 | 32/78 | 119/262 |
| Fasting blood glucose ≥ 110 mg/dL, yes/no | 203/379 | 18/26 | 23/22 | 37/75 | 125/256 |
| Systolic blood pressure ≥ 130 mmHg and/or diastolic blood pressure ≥85 mmHg, yes/no | 183/399 | 19/25 | 25/20 | 35/77 | 104/277 |
| Metabolic syndrome, yes/no | 109/473 | 8/36 | 22/23 | 9/103 | 70/311 |
| AST (IU/L) | 35.9 ± 42.2 | 35.1 ± 21.2 | 40.3 ± 26.6 | 31.8 ± 20.3 | 36.6 ± 49.6 |
| ALT (IU/L) | 37.4 ± 54.7 | 33.6 ± 40.7 | 40.4 ± 40.2 | 27.9 ± 24.1 | 40.2 ± 63.2 |
| eGFR (ml/min/1.73 m2) | 83.3 ± 21.4 | 79.6 ± 26.1 | 77.8 ± 22.2 | 80.8 ± 22.9 | 85.1 ± 20.0 |
| Variables | Metabolic Syndrome, Yes (n = 109) | Metabolic Syndrome, No (n = 473) | p Value |
|---|---|---|---|
| Age (years) | 65 (55, 71) | 61 (49.5, 68) | 0.0040 |
| Gender, male/female | 68/41 | 222/251 | 0.0041 |
| HBV/HCV/others | 19/37/53 | 70/218/185 | 0.0692 |
| Presence of LC, yes/no | 36/73 | 132/341 | 0.2931 |
| Our classification by GS and SMI | 8/22/9/70 | 36/23/103/311 | <0.0001 |
| Total bilirubin (mg/dL) | 0.8 (0.6, 1.0) | 0.8 (0.6, 1.0) | 0.9473 |
| Serum albumin (g/dL) | 4.2 (3.95, 4.5) | 4.2 (4.0, 4.5) | 0.9510 |
| Prothrombin time (INR) | 1.03 (0.97, 1.095) | 1.03 (0.98, 1.09) | 0.7913 |
| Platelet count (×104/mm3) | 17.8 (12.55, 23.1) | 18.8 (13.1, 23.35) | 0.2648 |
| AST (IU/l) | 30 (21.5, 47) | 25 (20, 37) | 0.5935 |
| ALT (IU/l) | 30 (18, 56) | 22 (15, 40) | 0.1778 |
| ECW to TBW ratio | 0.388 (0.383, 0.393) | 0.387 (0.381, 0.392) | 0.1475 |
| eGFR (ml/min/1.73 m2) | 78 (66, 89.5) | 82 (71, 97) | 0.0026 |
| Multivariate Analysis | |||
|---|---|---|---|
| Hazard Ratio | 95% CI | p Value | |
| Age (per one year) | 1.023 | 1.001–1.046 | 0.0438 |
| Gender (male) | 2.361 | 1.482–3.760 | 0.0003 |
| eGFR (per one ml/min/1.73 m2) | 0.989 | 0.977–1.001 | 0.0623 |
| Our classification by GS and SMI | |||
| Sarcopenia | 0.879 | 0.371–2.084 | 0.7703 |
| Dynapenia | 4.020 | 1.989–8.125 | 0.0001 |
| Presarcopenia | 0.350 | 0.110–1.001 | 0.0521 |
| Control | 1.000 | Reference | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, H.; Yoh, K.; Enomoto, H.; Nishiguchi, S.; Iijima, H. Dynapenia Rather Than Sarcopenia Is Associated with Metabolic Syndrome in Patients with Chronic Liver Diseases. Diagnostics 2021, 11, 1262. https://doi.org/10.3390/diagnostics11071262
Nishikawa H, Yoh K, Enomoto H, Nishiguchi S, Iijima H. Dynapenia Rather Than Sarcopenia Is Associated with Metabolic Syndrome in Patients with Chronic Liver Diseases. Diagnostics. 2021; 11(7):1262. https://doi.org/10.3390/diagnostics11071262
Chicago/Turabian StyleNishikawa, Hiroki, Kazunori Yoh, Hirayuki Enomoto, Shuhei Nishiguchi, and Hiroko Iijima. 2021. "Dynapenia Rather Than Sarcopenia Is Associated with Metabolic Syndrome in Patients with Chronic Liver Diseases" Diagnostics 11, no. 7: 1262. https://doi.org/10.3390/diagnostics11071262
APA StyleNishikawa, H., Yoh, K., Enomoto, H., Nishiguchi, S., & Iijima, H. (2021). Dynapenia Rather Than Sarcopenia Is Associated with Metabolic Syndrome in Patients with Chronic Liver Diseases. Diagnostics, 11(7), 1262. https://doi.org/10.3390/diagnostics11071262