1. Introduction
Hepatocellular carcinoma (HCC) is mainly associated with chronic liver disease and it is the fifth most common malignant tumor worldwide and the second leading cause of cancer-related mortality [
1]. Transarterial chemoembolization (TACE) is the first line treatment for HCC at intermediate stage of disease, according to the Barcelona Clinic Liver Cancer (BCLC) staging system, but it was recently demonstrated to be an effective procedure at any HCC stage [
2]. Nowadays, according to the European Association for the Study of the Liver (EASL) guidelines, TACE is also widely accepted as a neoadjuvant therapy before liver transplantation to downstage the tumor burden [
3].
There are two different TACE techniques. Conventional TACE (cTACE) is the most common modality performed worldwide and it employs lipiodol suspension and gelatine sponge particles. It is also possible to perform TACE with drug-eluting beads (DEB-TACE). Currently, there is no scientific evidence to demonstrate the superiority of one technique over the other in terms of tumor response, survival, safety and cost-effectiveness [
2,
4]; nevertheless, TACE outcomes are mainly assessed with imaging such as computed tomography (CT) and magnetic resonance imaging (MRI) and this is the aspect that most studies are focused on [
5].
Radiomics is an advanced analysis method which can be applied on CT, MRI and other imaging techniques, allowing to extrapolate quantitative features from regions or volumes of interest (ROI/VOI) in diagnostic images [
6]. Application of radiomics in oncology for tumor characterization, response assessment, prediction of response to therapies and survival prediction has been widely investigated in the literature with good results, including in HCC [
7].
As far as the prediction of response to treatments in HCC is concerned, radiomics has been applied on CT and MRI pre-treatment images in some studies, identifying specific radiomic features that were significantly correlated with response to surgery [
8], radiofrequency ablation [
9], chemotherapy with Sorafenib [
10] and TACE combined with Sorafenib sistemic therapy [
11]. Some radiomic features were also demonstrated to be valuable predictive factors of response to TACE as a single HCC treatment and most of them were based on MRI [
12,
13,
14,
15]. Furthermore, Kim et al. [
16] identified a combined score model integrating clinical data and texture analysis, with a good predictive value on survival after cTACE.
The purpose of this study was to assess long term outcomes of DEB-TACE in a single center population and to investigate whether pretreatment CT-based radiomics features are associated with response and survival.
2. Materials and Methods
2.1. Patient Population
Patients that underwent treatment with DEB-TACE for radiologically confirmed (LI-RADS 5) [
17] HCC in our center between 2009 and 2014 were reviewed. We included only patients treated with DEB-TACE instead of cTACE because they were much more numerous in our series, allowing a more homogeneous study. Since its introduction, we preferred DEB-TACE over C-TACE due to its lower sistemic effects. Inclusion criteria were: (a) Treatment of HCC with DEB-TACE as a first line of treatment; (b) treatment with DEB-TACE as a second line treatment only when previous treatment was performed at least 12 months earlier and concerned different lesions that were treated only with percutaneous thermal ablation; (c) pre and triphasic contrast (arterial, portal, delayed) CT scan performed at least 60 days before treatment; and (d) pre and triphasic contrast CT scan performed within 3 months after treatment. Exclusion criteria were: (a) non-suitable target lesions for segmentation; (b) presence of portal thrombosis or extra-hepatic disease; (c) lack of availability of clinical information or survival data; and (d) not HCC-related death causes. Applying these criteria, out of the initially 96 recruited patients, 50 were finally selected. Demographic and clinical data of the included population are shown in
Table 1.
2.2. CT Acquisition and Evaluation
CT examinations before and after treatment were performed by using a 256-slice CT (Brilliance iCT 256, Philips Healthcare, Eindhoven, Netherlands), with a tube voltage of 120 kVp.
All CT scans were performed in a cranio-caudal direction, with the patient in a supine position. Dynamic scans were performed using a bolus-tracking software program, with the placement of a 150 HU-threshold region-of-interest (ROI) within the abdominal aorta at the level of the celiac tripod. All CT examinations included a pre-enhanced phase, a parenchimal arterial phase acquired 15 s after reaching the threshold of the ROI, a portal venous phase 70 s after the threshold and a later phase after 180 s.
Response to therapy evaluation was performed by two radiologists in consensus, with 5 and 12 years of experience in the field of interventional radiology, and was based on a post-procedural CT examination performed within 3 months from the treatment and compared to pre-procedural CT, using modified RECIST (mRECIST) criteria for hepatocellular carcinoma [
18], identifying as possible results progressive disease (PD), stable disease (SD), partial response (PR) or complete response (CR).
2.3. Texture Analysis
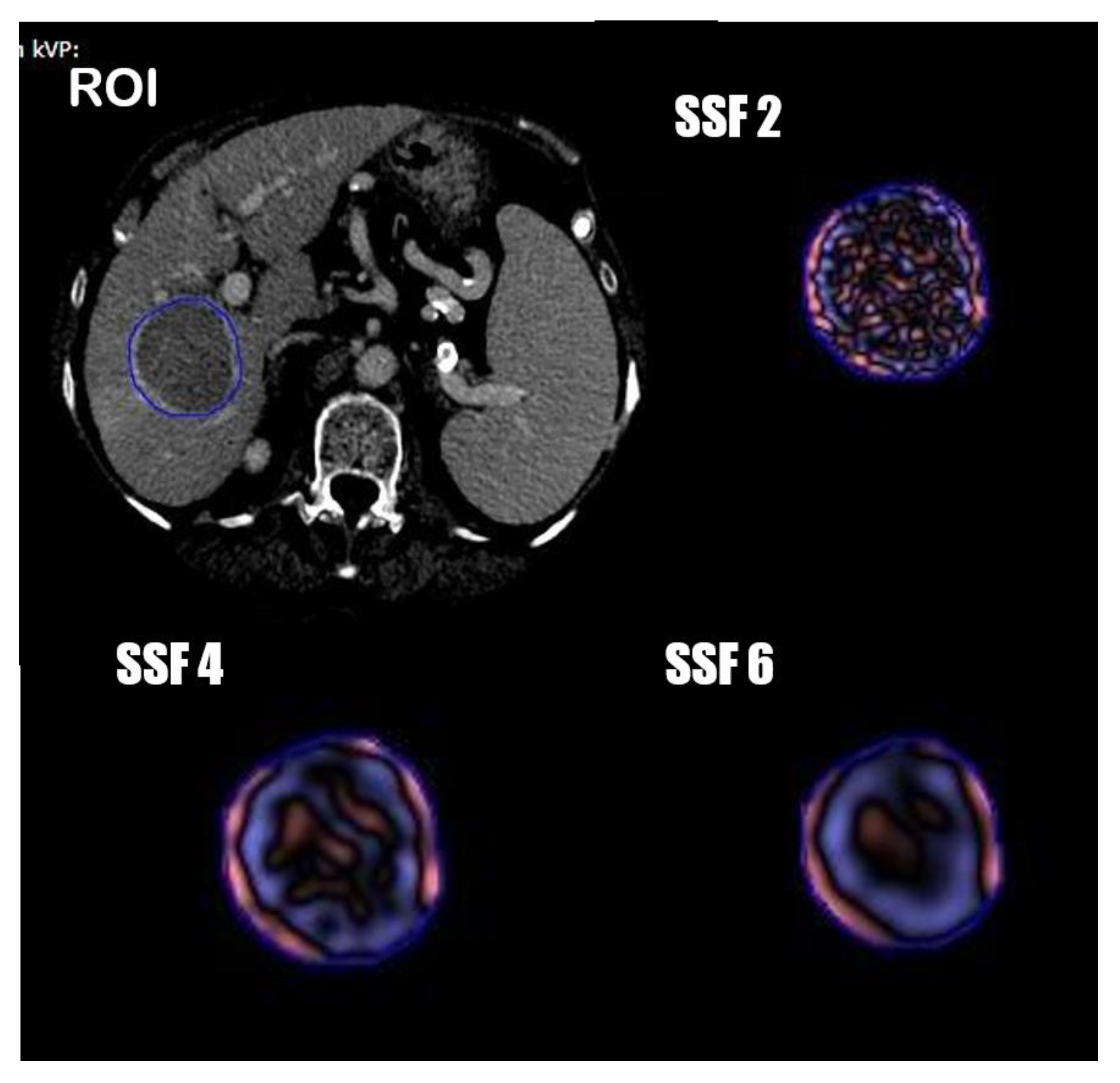
One radiologist and one resident in consensus manually segmented the tumor volumetric region of interest (VOI) on axial portal phases of the pre-treatment CT images, always considering the arterial phase to compare the geometrical shape of the lesion. (
Figure 1) Radiomics features were extracted from the obtained VOIs and analyzed with TexRAD, a proprietary software algorithm (TexRAD Ltd, Somerset, England, United Kingdom).The spatial scale filter (SSF) value was altered between 0 and 6, extrapolating CT intensity features of three different sizes: fine (between 0 and 2 mm), medium (between 3 and 4 mm) and coarse (between 5 and 6 mm). Then, the following histogram parameters were extracted with every filter: mean, standard deviation, mean value of positive pixels (MPP), skewness, entropy, and kurtosis. In the final analysis, 18 features were extracted and analyzed.
2.4. Treatment Modality
The treatment was performed with selective catheterization of the tumoral feeding arteries and injection of DC Bead™ microspheres 100–500 µm (Boston Scientific) associated to 50 to 150 mg of doxorubicin, depending on the tumor size and vascularization, until a complete blockage of the flow of tumor feeding branches was achieved. Procedures were performed by three interventional radiologists with more than 5 years of experience. The angiographic suit was equipped with a flat panel image intensifier, Digital Innova 2000 (GE, New York, NY, USA). According to the operator preference, a 3DCT was performed simultaneously in order to improve the identification of target tumor vessels.
2.5. Statistical Analysis
A normality test was performed on all continuous variables. Continuous variables were expressed as medians and standard deviation, while categorical variables were expressed as counts and percentages.
Univariate analysis was performed for radiomics and clinical features using an independent T-test for variables with a normal distribution, and a Mann–Whitney U test for non-normally distributed variables.
A Pearson chi-squared test was used for categorial variables.
Continuous variables were dichotomized around an optimal cut-off via ROC using the Youden index.
A logistic regression with a forward stepwise selection and a bootstrap internal validation was used to construct the model to predict treatment response, and model performance was evaluated using ROC curves. Survival models were constructed using multivariate Cox regression analysis and Kaplan–Meier survival analysis. A p value of 0.05 was considered statistically significant.
The software BM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA) was used for the statistical analysis.
4. Discussion
This study assessed the feasibility of radiomics in the prediction of response and survival to DEB-TACE for patients with HCC.
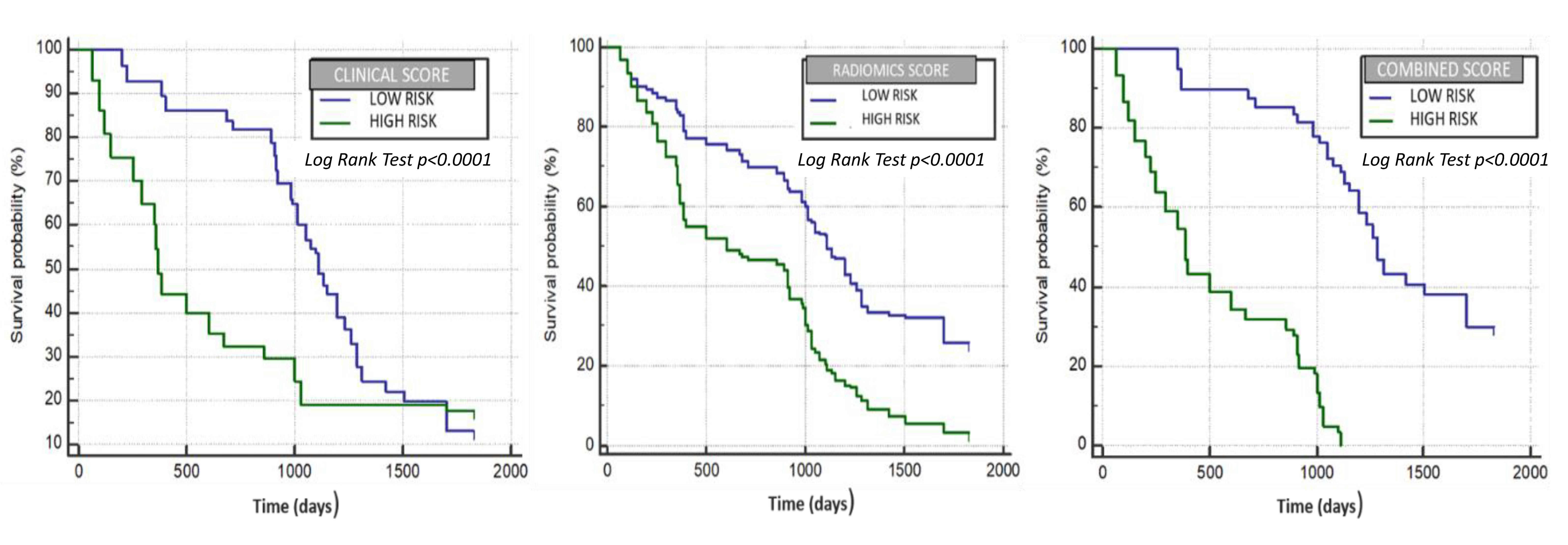
Data of texture analysis extracted from TextRad software (entropy, skewness, MPP and kurtosis) were able to identify two groups of patients with a different probability of response to treatment, evaluated with the mRECIST criteria, respectively with a low and a high probability of obtaining a complete response, corresponding with a better outcome and survival. Moreover, the model built to evaluate the radiomics data association with survival was able to identify two groups of patients with different median survival times (1111 vs. 602 days) as shown in the Kaplan–Meier graphic: an HR of 2.19 (95% CI: 2.03–2.35) (p < 0.0001) while the model built with the only clinical data yield an HR of 1.7 (95% CI: 1.54–1.9) (p < 0.0001) and a median OS of 1111 vs. 370 days. In the end, we combined both the radiomics and clinical models to construct a combined model that provided an even better estimation of survival time (median OS of 1285 vs. 387 days) with an HR of 4.61 (95% CI: 4.24–5.01) (p < 0.0001).
The most significant texture parameters associated with treatment outcome were entropy, skewness and kurtosis. In particular, kurtosis was statistically lower in patients with a better response; elevated values of kurtosis describe the pixel histogram to be more peaked or pointier than a Gaussian distribution, meaning that patients’ nodules with a better prognosis might have more regular nodular architecture reflected in a more homogeneous pixel distribution. On the other hand, ROI asymmetry is expressed by skewness and these values showed the higher heterogeneity in patients with a worse prognosis. A tumor a with high textural heterogeneity often has a poor prognosis and hence can negatively affect survival [
19,
20]. Even the entropy which is another manifestation of higher tumor heterogenicity showed lower values in patients with a better prognosis. This result is in line with the previously published paper by Cozzi et al. [
21] in which the entropy was found to be an independent predictor of OS in patients with advanced HCC undergoing systemic therapy with sorafenib.
Regarding clinical variables, our study revealed that different variables, such as Child–Pugh score, α-fetoprotein level, HCC size and number were significant in the clinical score model, according with existing studies [
22,
23].
As was recently reported, those models with a better performance are those in which radiomic features are computed with clinical data [
16,
24,
25]. Our combined model confirmed the radiomic pretreatment CT features together with clinical variables, and could be a good prognostic biomarker of the overall survival of patients suffering of HCC treated with DEB-TACE.
Texture analysis has been introduced in medical oncologic imaging as a noninvasive imaging biomarker with the aim to extract quantitative parameters from images to provide an objective characterization of the lesions [
26]. Several studies have already tested this approach on different neoplasms and in particular on lung cancer, showing some interesting results in the discrimination of malignancy in pulmonary lesions [
26,
27,
28]. Moreover, texture analysis is being demonstrated to be a potential biomarker for the prediction of response to treatments and therapy [
21]. In particular regarding HCC, Kim et al. first reported the prognostic value of a model based on pre-treatment CT-Texture analysis with better performance when combining clinical and radiomic variables. The authors reported excellent results of the model based on a second-order texture analysis and in evaluating survival after cTACE. In our study, however, pre-treatment CT-texture analysis was evaluated using a first-order statistical analysis with the well-known Texrad software and to evaluate patients treated with DEB-TACE in terms of survival but also in terms of response to treatment. In our view, lipiodol embolization could lead to post treatment CT interpretation pitfalls due to the high attenuation of the lipiodol itself. This pitfall may be overcome with the use of drug-eluting beads that do not influence the postoperative scans in terms of CT density. Moreover, our study demonstrated that texture analysis is significantly associated with response to DEB-TACE evaluated with the mRECIST criteria (model ROC curve (AUC 0.733,
p < 0.001).
This study has some inevitable limitations. Firstly, the population sample is limited; however, it concerns a very specific treatment, and comes from a single center only. Secondly, due to in consensus reading, there is lack of inter-reader agreement analysis. Thirdly, the use of a first-order statistical analysis allowed a simpler prediction model, and the identified cut-off values for the relevant parameters might be different in a different clinical scenario due to the lack of external validation or an internal validation cohort.
Nevertheless, our results are encouraging and confirm the prognostic value of Texture analysis in the pretreatment evaluation of response and survival to DEB-TACE for HCC, especially when combined with clinical data. This information may be useful to gain a more precise personalized oncologic approach that is mainly based on outcome predictions and personalized treatment than “one-fits-all” blanket treatments.
Further studies with a prospective design are required to further investigate the role of texture analysis in this scenario. Moreover, this is also a call for all radiologists and interventional radiologists towards a standardization of pre- and post-treatment imaging and data collection and towards high quality data registries [
29]. Machine learning is already an everyday tool and we need to implement it for the benefit of our patients.


 ,
, 



{kind=link}
{kind=link}