
UA-Zero as a Uranyl Acetate Replacement When Diagnosing Primary Ciliary Dyskinesia by Transmission Electron Microscopy

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Preparation of Nasal Brushing Biopsies for Transmission Electron Microscopy
2.3. Analysis of Diagnostic Results
2.4. Image Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shoemark, A.; Boon, M.; Brochhausen, C.; Bukowy-Bieryllo, Z.; De Santi, M.M.; Goggin, P.; Griffin, P.; Hegele, R.G.; Hirst, R.A.; Leigh, M.; et al. International consensus guideline for reporting transmission electron microscopy results in the diagnosis of Primary Ciliary Dyskinesia. Eur. Respir. J. 2019, 54. [Google Scholar] [CrossRef]
- Shapiro, A.J.; Davis, S.D.; Polineni, D.; Manion, M.; Rosenfeld, M.; Dell, S.D.; Chilvers, M.A.; Ferkol, T.W.; Zariwala, M.A.; Sagel, S.D.; et al. Diagnosis of Primary Ciliary Dyskinesia. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 197, e24–e39. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.S.; Barbato, A.; Collins, S.A.; Goutaki, M.; Behan, L.; Caudri, D.; Dell, S.; Eber, E.; Escudier, E.; Hirst, R.A.; et al. European Respiratory Society guidelines for the diagnosis of primary ciliary dyskinesia. Eur. Respir. J. 2017, 49, 1601090. [Google Scholar] [CrossRef] [PubMed]
- Burgoyne, T.; Dixon, M.; Luther, P.; Hogg, C.; Shoemark, A. Generation of a Three-Dimensional Ultrastructural Model of Human Respiratory Cilia. Am. J. Respir. Cell Mol. Biol. 2012, 47, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Watson, M.L. Staining of Tissue Sections for Electron Microscopy with Heavy Metals. J. Biophys. Biochem. Cytol. 1958, 4, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Inaga, S.; Katsumoto, T.; Tanaka, K.; Kameie, T.; Nakane, H.; Naguro, T. Platinum blue as an alternative to uranyl acetate for staining in transmission electron microscopy. Arch. Histol. Cytol. 2007, 70, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Adachi, A.; Sasaki, Y.; Ghazizadeh, M. Oolong tea extract as a substitute for uranyl acetate in staining of ultrathin sections. J. Microsc. 2007, 229, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.-I.; Inoue, K.; Kanematsu, S.; Horiuchi, Y.; Park, P. Enhanced effects of nonisotopic hafnium chloride in methanol as a substitute for uranyl acetate in TEM contrast of ultrastructure of fungal and plant cells. Microsc. Res. Tech. 2010, 74, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Nakakoshi, M.; Nishioka, H.; Katayama, E. New versatile staining reagents for biological transmission electron microscopy that substitute for uranyl acetate. J. Electron. Microsc. 2011, 60, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Shoemark, A.; Pinto, A.L.; Patel, M.P.; Daudvohra, F.; Hogg, C.; Mitchison, H.M.; Burgoyne, T. PCD Detect: Enhancing ciliary features through image averaging and classification. Am. J. Physiol. Lung Cell. Mol. Physiol. 2020, 319, L1048–L1060. [Google Scholar] [CrossRef] [PubMed]
- Zariwala, M.A.; Gee, H.Y.; Kurkowiak, M.; Al-Mutairi, D.A.; Leigh, M.W.; Hurd, T.W.; Hjeij, R.; Dell, S.; Chaki, M.; Dougherty, G.W.; et al. ZMYND10 Is Mutated in Primary Ciliary Dyskinesia and Interacts with LRRC6. Am. J. Hum. Genet. 2013, 93, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Shinohara, K.; Botilde, Y.; Nabeshima, R.; Takaoka, K.; Ajima, R.; Lamri, L.; Takeda, H.; Saga, Y.; Nakamura, T.; et al. Transport of the outer dynein arm complex to cilia requires a cytoplasmic protein Lrrc6. Genes Cells 2016, 21, 728–739. [Google Scholar] [CrossRef] [PubMed]
- Olbrich, H.; Häffner, K.; Kispert, A.; Völkel, A.; Volz, A.; Sasmaz, G.; Reinhardt, R.; Hennig, S.; Lehrach, H.; Konietzko, N.; et al. Mutations in DNAH5 cause primary ciliary dyskinesia and randomization of left–right asymmetry. Nat. Genet. 2002, 30, 143–144. [Google Scholar] [CrossRef] [PubMed]
- Antony, D.; Becker-Heck, A.; Zariwala, M.A.; Schmidts, M.; Onoufriadis, A.; Forouhan, M.; Wilson, R.; Taylor-Cox, T.; Dewar, A.; Jackson, C.; et al. Mutations inCCDC39andCCDC40are the Major Cause of Primary Ciliary Dyskinesia with Axonemal Disorganization and Absent Inner Dynein Arms. Hum. Mutat. 2013, 34, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Olbrich, H.; Schmidts, M.; Werner, C.; Onoufriadis, A.; Loges, N.T.; Raidt, J.; Banki, N.F.; Shoemark, A.; Burgoyne, T.; Al Turki, S.; et al. Recessive HYDIN Mutations Cause Primary Ciliary Dyskinesia without Randomization of Left-Right Body Asymmetry. Am. J. Hum. Genet. 2012, 91, 672–684. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
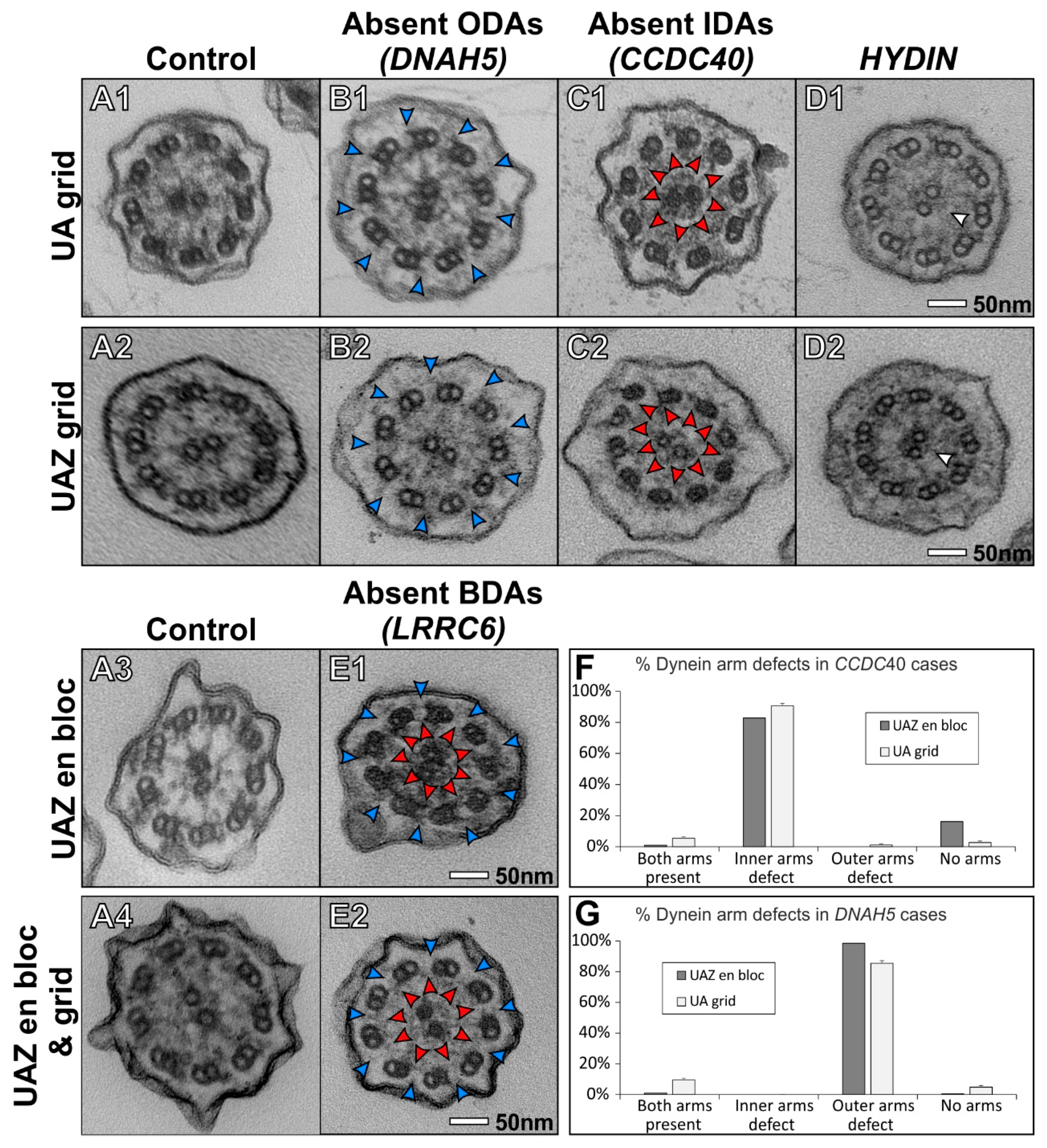
| PCD Gene | Patient Symptoms | Axoneme Structure Affected | Genotype |
|---|---|---|---|
| DNAH5 | Persistent rhinitis and prolonged otorrhea post grommet insertion | Defect of ODAs | Unsolved—Heterozygous DNAH5 NM_001369.2: c.7477G > C (p.Glu2493Arg) |
| CCDC40 | - | IDAs and microtubular disorganisation | CCDC40 NM_017950.3: c.2712–1G > T + c.2712–1G > T |
| HYDIN | Normal situs, chronic wet cough, rhinitis, and otorrhea | CP C2b component | HYDIN NM_001270974.1: c.8487del (p.Pro2830Hisfs*23) + c.8489C > A (p.Pro2830Gln) |
| LRRC6 | Chronic wet cough and affected family members | Defect of both ODAs and IDAs | LRRC6 NM_012472.3: c630del (p.Trp210Cysfs*12) + c630del (p.Trp210Cysfs*12) |
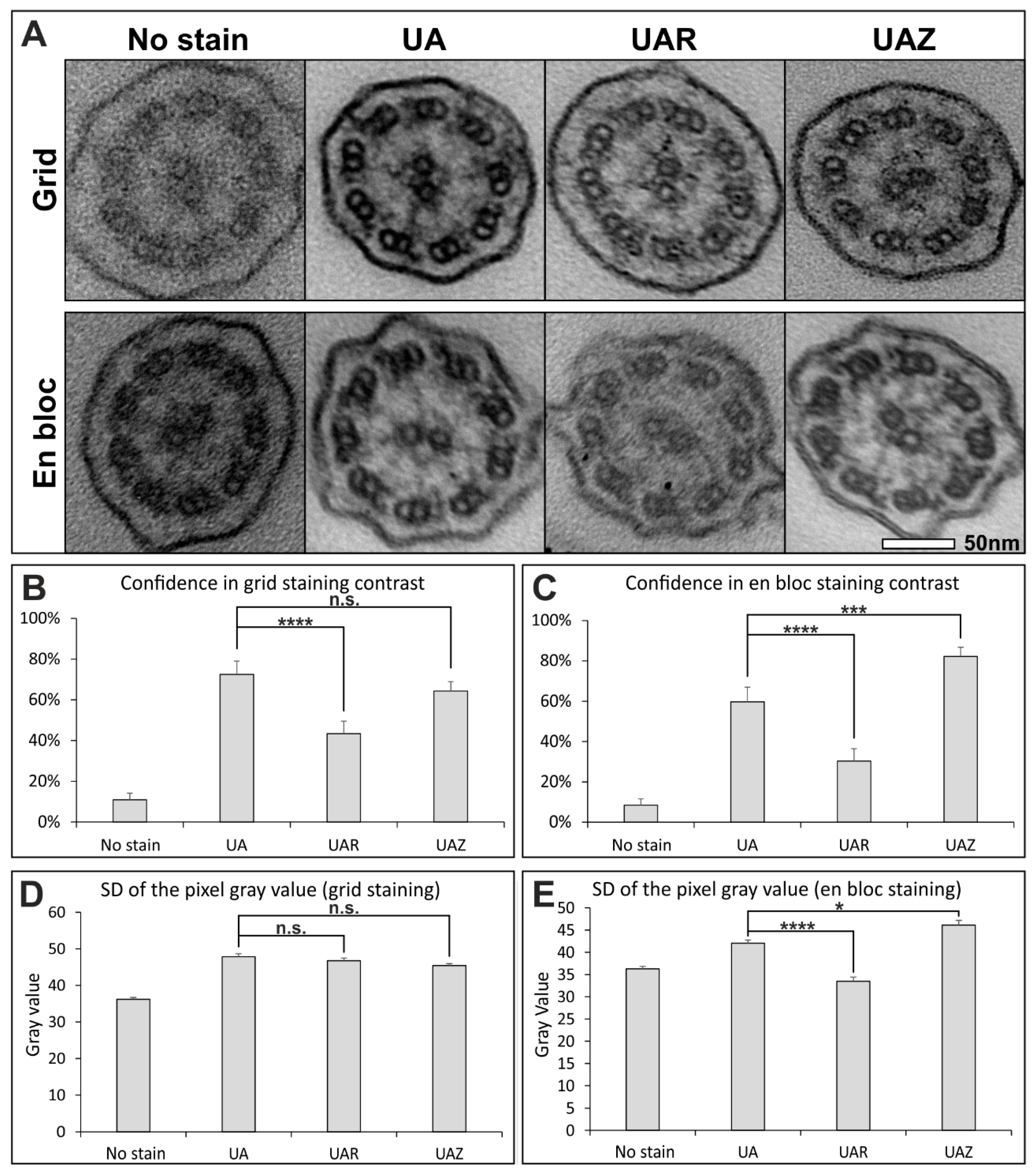
| En Bloc Stain | Method |
|---|---|
| No stain | No stain added during sample preparation |
| UA | 1% aqueous UA (Agar Scientific Ltd.) for 30 min |
| UAR | UAR (Electron Microscopy Sciences) diluted 1:4 in distilled water and applied for 30 min |
| UAZ | undiluted UAZ (Agar Scientific) for 30 min |
| Grid Stain | Method |
|---|---|
| No stain | No stain |
| UA | 2% aqueous UA for 7 min and Reynold’s lead citrate for 10 min |
| UAR | UAR (Electron Microscopy Sciences) diluted 1:4 in distilled water and applied for 30 min and Reynold’s lead citrate Reynold’s lead citrate |
| UAZ | undiluted UAZ for 7 min and Reynold’s lead citrate for 10 min |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, A.L.; Rai, R.K.; Shoemark, A.; Hogg, C.; Burgoyne, T. UA-Zero as a Uranyl Acetate Replacement When Diagnosing Primary Ciliary Dyskinesia by Transmission Electron Microscopy. Diagnostics 2021, 11, 1063. https://doi.org/10.3390/diagnostics11061063
Pinto AL, Rai RK, Shoemark A, Hogg C, Burgoyne T. UA-Zero as a Uranyl Acetate Replacement When Diagnosing Primary Ciliary Dyskinesia by Transmission Electron Microscopy. Diagnostics. 2021; 11(6):1063. https://doi.org/10.3390/diagnostics11061063
Chicago/Turabian StylePinto, Andreia Lucia, Ranjit Kaur Rai, Amelia Shoemark, Claire Hogg, and Thomas Burgoyne. 2021. "UA-Zero as a Uranyl Acetate Replacement When Diagnosing Primary Ciliary Dyskinesia by Transmission Electron Microscopy" Diagnostics 11, no. 6: 1063. https://doi.org/10.3390/diagnostics11061063
APA StylePinto, A. L., Rai, R. K., Shoemark, A., Hogg, C., & Burgoyne, T. (2021). UA-Zero as a Uranyl Acetate Replacement When Diagnosing Primary Ciliary Dyskinesia by Transmission Electron Microscopy. Diagnostics, 11(6), 1063. https://doi.org/10.3390/diagnostics11061063