
Malignancy Rate of Indeterminate Findings on FDG-PET/CT in Cutaneous Melanoma Patients


 ,
, 

Abstract
1. Introduction
2. Methods
2.1. Patient Population
2.2. FDG-PET/CT Acquisition
2.3. FDG-PET/CT Image Analysis
2.4. Lesion Selection
2.5. Statistical Analysis
3. Results
3.1. Patient Population
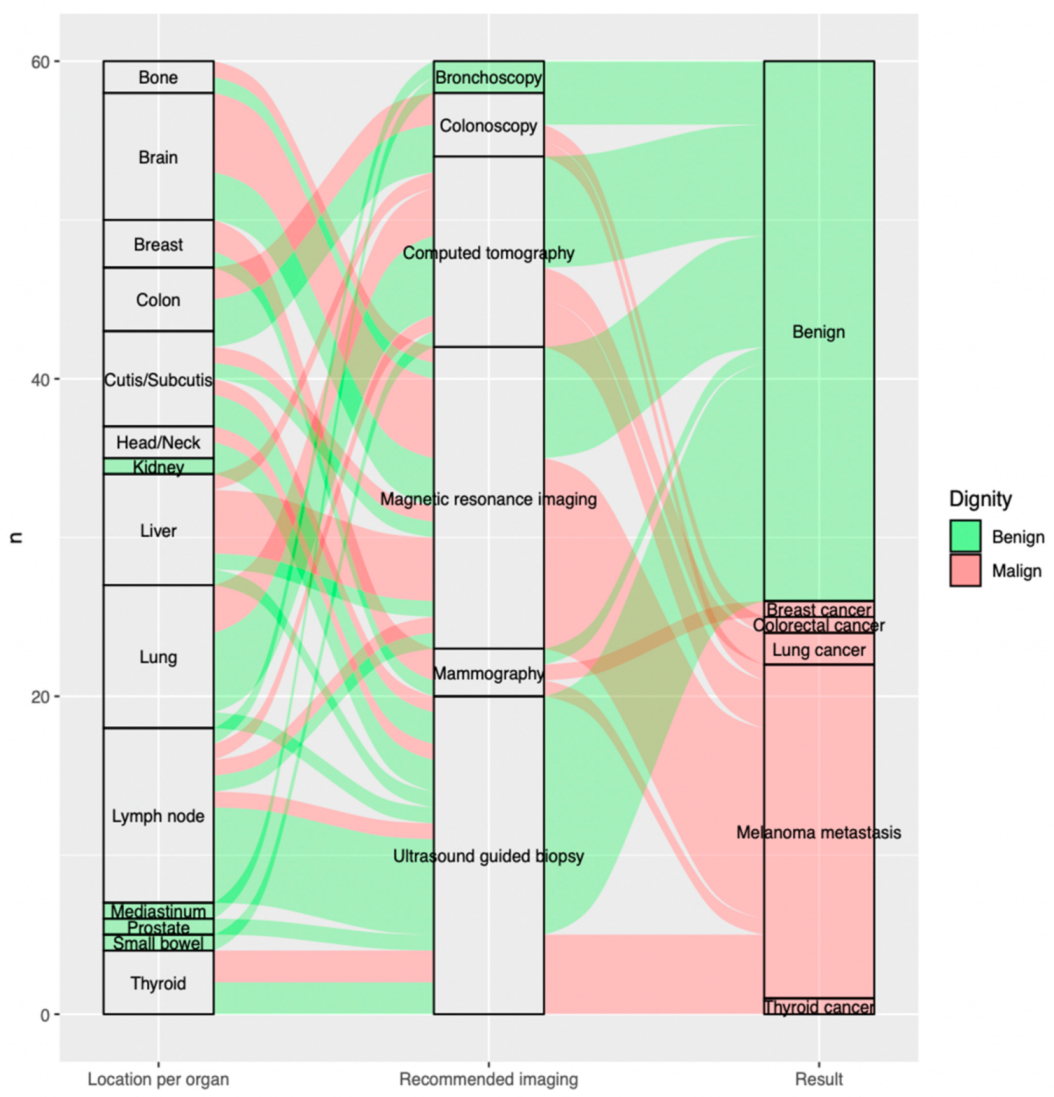
3.2. Indeterminate Findings on FDG-PET/CT Scan
3.3. Additional Imaging Required after FDG-PET/CT Scan
3.4. Standard Assessment of Dignity
3.5. Outcome of Required Additional Imaging after FDG-PET/CT Scan
3.6. Impact of Required Additional Imaging on Clinical Management
3.7. Impact of FDG-PET/CT Indication on Results of Recommended Additional Imaging
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ICI | Immune Checkpoint Inhibitors |
| anti-PD1 | anti-Programmed Death-1 |
| anti-CTLA4 | anti-Cytotoxic T-Lymphocyte-Associated Protein 4 |
| FDG-PET/CT | 18F-2-Fluor-2-desoxy-D-glucose Positron Emission Tomography/Computed Tomography |
| CT | Computed Tomography |
| AJCC | American Joint Committee on Cancer |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| GCP | Good Clinical Practice |
| mg | Milligram |
| dl | Deciliter |
| BMI | Body Mass Index |
| GE | General Electric |
| PET | Positron Emission Tomography |
| OSEM | Ordered Subset Expectation Maximization |
| BSREM | Block Sequential Regularized Expectation Maximation |
| SPSS | Statistical Package for the Social Sciences |
| MRI | Magnetic Resonance Imaging |
| DWI | Diffusion Weighted Imaging |
| MIP | Maximum Intensity Projection |
References
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Bastholt, L.; Bataille, V.; Del Marmol, V.; Dréno, B.; Fargnoli, M.C.; et al. European Consensus-Based Interdisciplinary Guideline for Melanoma. Part 1: Diagnostics-Update 2019. Eur. J. Cancer 2020, 126, 141–158. [Google Scholar] [CrossRef] [PubMed]
- Burns, D.; George, J.; Aucoin, D.; Bower, J.; Burrell, S.; Gilbert, R.; Bower, N. The Pathogenesis and Clinical Management of Cutaneous Melanoma: An Evidence-Based Review. J. Med. Imaging Radiat. Sci. 2019, 50, 460–469.e1. [Google Scholar] [CrossRef] [PubMed]
- Howard, M.D. Melanoma Radiological Surveillance: A Review of Current Evidence and Clinical Challenges. Yale J. Biol. Med. 2020, 93, 207–213. [Google Scholar] [PubMed]
- Leiter, U.; Eigentler, T.; Garbe, C. Epidemiology of Skin Cancer. Adv. Exp. Med. Biol. 2014, 810, 120–140. [Google Scholar] [CrossRef]
- Dimitriou, F.; Krattinger, R.; Ramelyte, E.; Barysch, M.J.; Micaletto, S.; Dummer, R.; Goldinger, S.M. The World of Melanoma: Epidemiologic, Genetic, and Anatomic Differences of Melanoma across the Globe. Curr. Oncol. Rep. 2018, 20, 87. [Google Scholar] [CrossRef]
- Luke, J.J.; Flaherty, K.T.; Ribas, A.; Long, G.V. Targeted Agents and Immunotherapies: Optimizing Outcomes in Melanoma. Nat. Rev. Clin. Oncol. 2017, 14, 463–482. [Google Scholar] [CrossRef]
- Mittal, B.R.; Malik, D.; Sood, A.; Basher, R.K.; Bhattacharya, A.; Singh, G. Role of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Restaging and Prognosis of Recurrent Melanoma after Curative Surgery. World J. Nucl. Med. 2019, 18, 176–182. [Google Scholar] [CrossRef]
- Salvatore, A.; Riccardo, L.; Federico, C.; Daniele, A.P.; Young Aimn Working Group. Clinical Value of PET/CT in Staging Melanoma and Potential New Radiotracers. Curr. Radiopharm. 2020, 13, 6–13. [Google Scholar] [CrossRef]
- Cheng, D.; McNicoll, C.F.; Kirgan, D.; Jones, M.S.; Rivera, M.R.; Doyle, G.M.; De Guzman, M.D.; Baynosa, J.; Hill, C.R.S. The Role of FDG-PET-CT Is Limited in Initial Staging of Nodal Metastasis for Thin Cutaneous Melanoma. Am. J. Surg. 2021, 221, 737–740. [Google Scholar] [CrossRef]
- Castello, A.; Lopci, E. The Role of PET/CT in the Era of Immune Checkpoint Inhibitors: State of Art. Curr. Radiopharm. 2020, 13, 24–31. [Google Scholar] [CrossRef]
- Decazes, P.; Bohn, P. Immunotherapy by Immune Checkpoint Inhibitors and Nuclear Medicine Imaging: Current and Future Applications. Cancers 2020, 12, 371. [Google Scholar] [CrossRef]
- Dittrich, D.; Pyka, T.; Scheidhauer, K.; Lütje, S.; Essler, M.; Bundschuh, R.A. Textural Features in FDG-PET/CT Can Predict Outcome in Melanoma Patients to Treatment with Vemurafenib and Ipililumab. Nukl. Nucl. Med. 2020, 59, 228–234. [Google Scholar] [CrossRef]
- Basler, L.; Gabryś, H.S.; Hogan, S.A.; Pavic, M.; Bogowicz, M.; Vuong, D.; Tanadini-Lang, S.; Foerster, R.; Kudura, K.; Huellner, M.W.; et al. Radiomics, Tumor Volume, and Blood Biomarkers for Early Prediction of Pseudoprogression in Patients with Metastatic Melanoma Treated with Immune Checkpoint Inhibition. Clin. Cancer Res. 2020, 26, 4414–4425. [Google Scholar] [CrossRef]
- Nakamoto, R.; Zaba, L.C.; Rosenberg, J.; Reddy, S.A.; Nobashi, T.W.; Davidzon, G.; Aparici, C.M.; Nguyen, J.; Moradi, F.; Iagaru, A.; et al. Prognostic Value of Volumetric PET Parameters at Early Response Evaluation in Melanoma Patients Treated with Immunotherapy. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2787–2795. [Google Scholar] [CrossRef]
- Hicks, R.J.; Iravani, A.; Sandhu, S. 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography for Assessing Tumor Response to Immunotherapy in Solid Tumors: Melanoma and Beyond. PET Clin. 2020, 15, 11–22. [Google Scholar] [CrossRef]
- Iravani, A.; Hicks, R.J. Imaging the Cancer Immune Environment and Its Response to Pharmacological Intervention-Part 1-The Role of FDG PET/CT. J. Nucl. Med. 2020, 61, 943–950. [Google Scholar] [CrossRef]
- Iravani, A.; Osman, M.M.; Weppler, A.M.; Wallace, R.; Galligan, A.; Lasocki, A.; Hunter, M.O.; Akhurst, T.; Hofman, M.S.; Lau, P.K.H.; et al. FDG PET/CT for Tumoral and Systemic Immune Response Monitoring of Advanced Melanoma during First-Line Combination Ipilimumab and Nivolumab Treatment. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2776–2786. [Google Scholar] [CrossRef]
- Bisschop, C.; De Heer, E.; Brouwers, A.; Hospers, G.; Jalving, M. Rational Use of 18F-FDG PET/CT in Patients with Advanced Cutaneous Melanoma: A Systematic Review. Crit. Rev. Oncol. Hematol. 2020, 153, 103044. [Google Scholar] [CrossRef]
- Nijhuis, A.A.G.; Dieng, M.; Khanna, N.; Lord, S.J.; Dalton, J.; Menzies, A.M.; Turner, R.M.; Allen, J.; Saw, R.P.M.; Nieweg, O.E.; et al. False-Positive Results and Incidental Findings with Annual CT or PET/CT Surveillance in Asymptomatic Patients with Resected Stage III Melanoma. Ann. Surg. Oncol. 2019, 26, 1860–1868. [Google Scholar] [CrossRef]
- Pfannenberg, C.; Gueckel, B.; Wang, L.; Gatidis, S.; Olthof, S.-C.; Vach, W.; Reimold, M.; La Fougere, C.; Nikolaou, K.; Martus, P. Practice-Based Evidence for the Clinical Benefit of PET/CT-Results of the First Oncologic PET/CT Registry in Germany. Eur. J. Nucl. Med. Mol. Imaging 2018, 46, 54–64. [Google Scholar] [CrossRef]
- Forschner, A.; Olthof, S.-C.; Gückel, B.; Martus, P.; Vach, W.; La Fougère, C.; Nikolaou, K.; Keim, U.; Eigentler, T.K.; Garbe, C.; et al. Impact of 18F-FDG-PET/CT on Surgical Management in Patients with Advanced Melanoma: An Outcome Based Analysis. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, F.; Mangana, J.; Curioni-Fontecedro, A.; Rechsteiner, M.; Turko, P.; Braun, R.P.; Dummer, R.; Cheng, P.F. Melanoma Patients with Additional Primary Cancers: A Single-Center Retrospective Analysis. Oncotarget 2019, 10, 3373–3384. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organ | Radiological Follow Up (CT or MRI) | Biopsy Guide by Ultrasound | Biopsy Guide by a Bronchoscopy, b Colonoscopy or Based on c Mammography | Total |
|---|---|---|---|---|
| Lymph node | 3 | 7 | 1a | 11 |
| Liver | 6 | 1 | 0 | 7 |
| Thyroid | 0 | 4 | 0 | 4 |
| Breast | 1 | 1 | 1c | 3 |
| Cutis/Subcutis | 3 | 3 | 0 | 6 |
| Brain | 8 | 0 | 0 | 8 |
| Head/Neck | 0 | 2 | 0 | 2 |
| Lung | 8 | 0 | 1a | 9 |
| Colon | 0 | 0 | 4b | 4 |
| Small bowel | 1 | 0 | 0 | 1 |
| Bone | 2 | 0 | 0 | 2 |
| Kidney | 0 | 1 | 0 | 1 |
| Mediastinum | 0 | 0 | 1a | 1 |
| Prostate | 0 | 1 | 0 | 1 |
| Total | 31 | 20 | 9 | 60 |
| Organ | Number of Benign Finding(s) per Organ | Number of Malignant Finding(s) per Organ | Number of Indeterminate Finding(s) per Organ |
|---|---|---|---|
| Lymph node | 8 | 3 | 11 |
| Liver | 2 | 5 | 7 |
| Thyroid | 2 | 2 | 4 |
| Breast | 1 | 2 | 3 |
| Cutis/Subcutis | 4 | 2 | 6 |
| Brain | 3 | 5 | 8 |
| Head/Neck | 1 | 1 | 2 |
| Lung | 6 | 3 | 9 |
| Colon | 2 | 2 | 4 |
| Small bowel | 1 | 0 | 1 |
| Bone | 1 | 1 | 2 |
| Kidney | 1 | 0 | 1 |
| Mediastinum | 1 | 0 | 1 |
| Prostate | 1 | 0 | 1 |
| Total | 34 | 26 | 60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kudura, K.; Dimitriou, F.; Mihic-Probst, D.; Muehlematter, U.J.; Kutzker, T.; Basler, L.; Förster, R.; Dummer, R.; Mangana, J.; Husmann, L.; et al. Malignancy Rate of Indeterminate Findings on FDG-PET/CT in Cutaneous Melanoma Patients. Diagnostics 2021, 11, 883. https://doi.org/10.3390/diagnostics11050883
Kudura K, Dimitriou F, Mihic-Probst D, Muehlematter UJ, Kutzker T, Basler L, Förster R, Dummer R, Mangana J, Husmann L, et al. Malignancy Rate of Indeterminate Findings on FDG-PET/CT in Cutaneous Melanoma Patients. Diagnostics. 2021; 11(5):883. https://doi.org/10.3390/diagnostics11050883
Chicago/Turabian StyleKudura, Ken, Florentia Dimitriou, Daniela Mihic-Probst, Urs J. Muehlematter, Tim Kutzker, Lucas Basler, Robert Förster, Reinhard Dummer, Joanna Mangana, Lars Husmann, and et al. 2021. "Malignancy Rate of Indeterminate Findings on FDG-PET/CT in Cutaneous Melanoma Patients" Diagnostics 11, no. 5: 883. https://doi.org/10.3390/diagnostics11050883
APA StyleKudura, K., Dimitriou, F., Mihic-Probst, D., Muehlematter, U. J., Kutzker, T., Basler, L., Förster, R., Dummer, R., Mangana, J., Husmann, L., Burger, I. A., & Kreissl, M. C. (2021). Malignancy Rate of Indeterminate Findings on FDG-PET/CT in Cutaneous Melanoma Patients. Diagnostics, 11(5), 883. https://doi.org/10.3390/diagnostics11050883