
Evaluation of Beta-Catenin Subcellular Localization and Water Channel Protein AQP1 Expression as Predictive Markers of Chemo-Resistance in Ovarian High-Grade Serous Carcinoma: Comparative Study between Preoperative Peritoneal Biopsies and Surgical Samples

 ,
,  ,
,  , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Clinical Data
2.2. Pathology Evaluation
2.3. Immunohistochemistry
2.4. Statistical Analysis
3. Results
3.1. Patient Baseline Characteristics
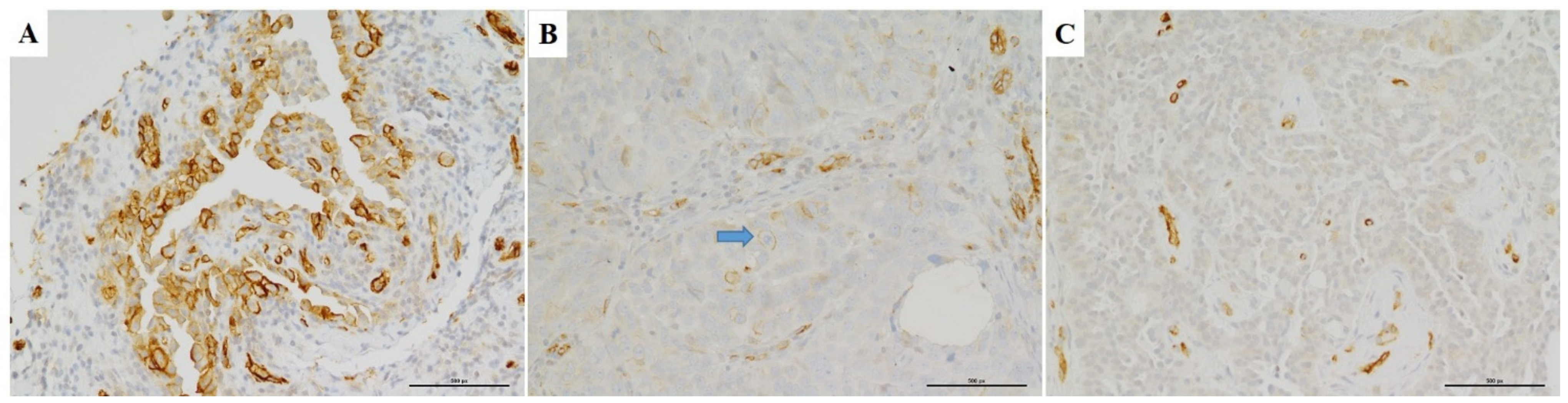
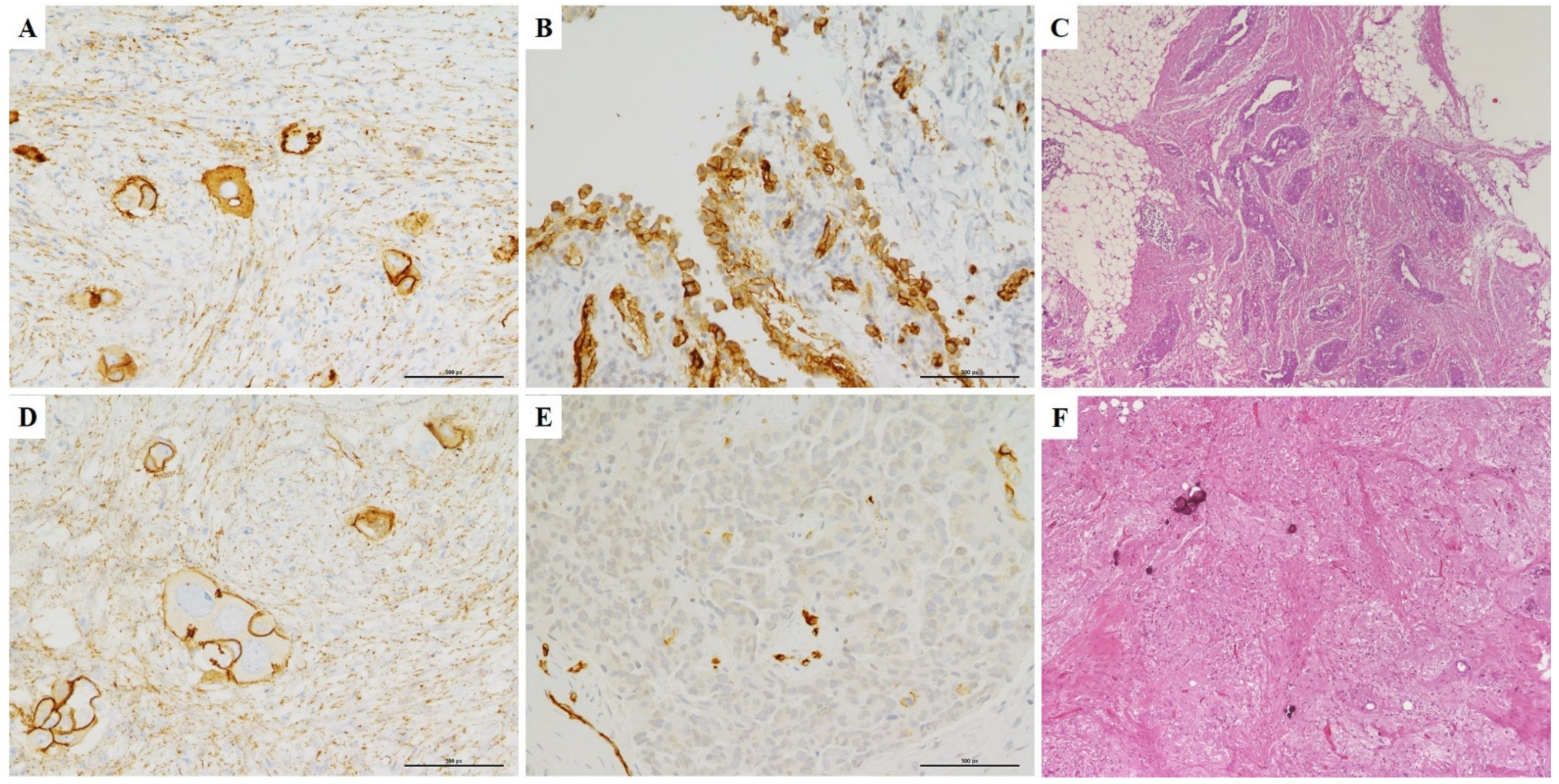
3.2. Immunohistochemistry
3.3. Omental Chemotherapy Response
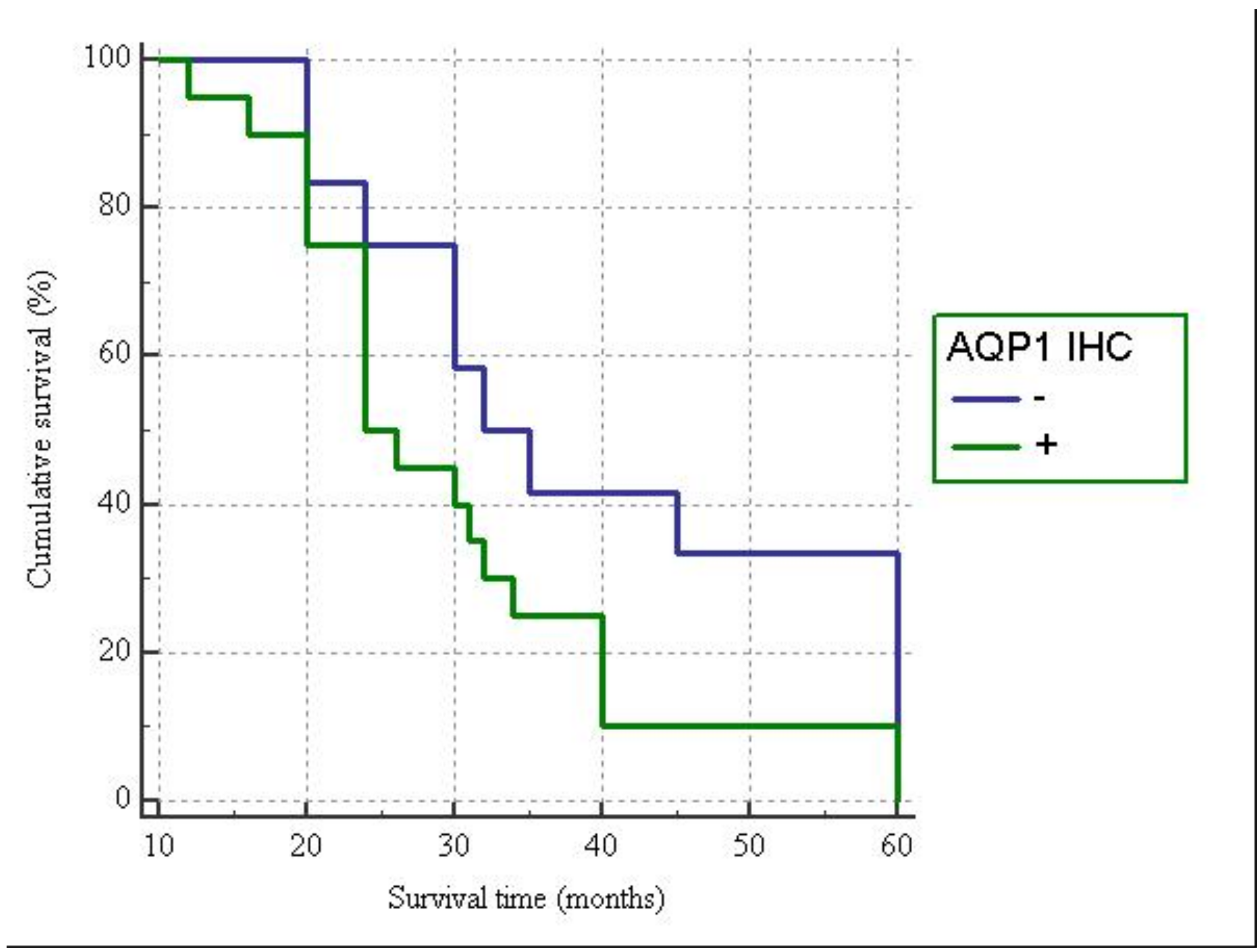
3.4. AQP1 and β-Catenin Immuno-Expression Relationships
3.5. Clinico-Pathological Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-J.; Bristow, R.E. Evolution of surgical treatment paradigms for advanced-stage ovarian cancer: Redefining ‘optimal’ residual disease. Gynecol. Oncol. 2012, 125, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; Tropé, C.G.; Amant, F.; Kristensen, G.B.; Ehlen, T.; Johnson, N.; Verheijen, R.H.M.; Burg, M.E.L.v.d.; Lacave, A.J.; Panici, P.B.; et al. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N. Engl. J. Med. 2010, 363, 943–953. [Google Scholar] [CrossRef]
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.C.; Kitchener, H.; Lopes, T.; Luesley, D.; Perren, T.; Bannoo, S.; Mascarenhas, M.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]
- Petrillo, M.; Zannoni, G.F.; Tortorella, L.; Anchora, L.P.; Salutari, V.; Ercoli, A.; Margariti, P.A.; Scambia, G.; Fagotti, A. Prognostic role and predictors of complete pathologic response to neoadjuvant chemotherapy in primary unresectable ovarian cancer. Am. J. Obstet. Gynecol. 2014, 211, 632.e1-632.e8. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.A.; Powell, A.; Böhm, S.; Gilks, C.B.; Stewart, C.J.R.; Meniawy, T.M.; Bulsara, M.; Avril, S.; Brockbank, E.C.; Bosse, T.; et al. Patho-logical chemotherapy response score is prognostic in tubo-ovarian high-grade serous carcinoma: A systematic review and meta-analysis of individual patient data. Gynecol. Oncol. 2019, 154, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Angelico, G.; Piermattei, A.; Inzani, F.; Valente, M.; Arciuolo, D.; Spadola, S.; Mulè, A.; Zorzato, P.; Fagotti, A.; et al. Patho-logical Chemotherapy Response Score in Patients Affected by High Grade Serous Ovarian Carcinoma: The Prognostic Role of Omental and Ovarian Residual Disease. Front. Oncol. 2019, 9, 778. [Google Scholar] [CrossRef]
- Böhm, S.; Faruqi, A.; Said, I.; Lockley, M.; Brockbank, E.; Jeyarajah, A.; Fitzpatrick, A.; Ennis, D.; Dowe, T.; Santos, J.L.; et al. Chemotherapy Response Score: Development and Validation of a System to Quantify Histopathologic Response to Neoadjuvant Chemotherapy in Tubo-Ovarian High-Grade Serous Carcinoma. J. Clin. Oncol. 2015, 33, 2457–2463. [Google Scholar] [CrossRef]
- McCluggage, W.G.; Judge, M.J.; Clarke, B.A.; Davidson, B.; Gilks, C.B.; Hollema, H.; Ledermann, J.A.; Matias-Guiu, X.; Mikami, Y.; Stewart, C.J.R.; et al. International Collaboration on Cancer Reporting. Data set for reporting of ovary, fallopian tube and primary peri-toneal carcinoma: Recommendations from the International Collaboration on Cancer Reporting (ICCR). Mod. Pathol. 2015, 28, 1101–1122. [Google Scholar] [CrossRef]
- Liang, M.; Prendergast, E.; Staples, J.; Holschneider, C.; Cass, I. Complete pathologic response at interval debulking surgery following neoadjuvant chemotherapy predicts improved survival in women with advanced epithelial ovarian cancer in a mul-ti-institutional cohort. Gynecol. Oncol. 2016, 143, 197. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Chung, Y.S.; Na, K.; Kim, H.M.; Park, C.K.; Nam, E.J.; Kim, S.; Kim, S.W.; Kim, Y.T.; Kim, H.-S. External validation of chemotherapy response score system for histopathological assessment of tumor regression after neoadjuvant chemotherapy in tubo-ovarian high-grade serous carcinoma. J. Gynecol. Oncol. 2017, 28, e73. [Google Scholar] [CrossRef]
- Rajkumar, S.; Polson, A.; Nath, R.; Lane, G.; Sayasneh, A.; Jakes, A.; Begum, S.; Mehra, G. Prognostic implications of histological tumor regression (Böhm’s score) in patients receiving neoadjuvant chemotherapy for high grade serous tubal & ovarian carcinoma. Gynecol. Oncol. 2018, 151, 264–268. [Google Scholar] [CrossRef]
- Zhang, X.-Y.; Zhang, P.-Y. Recent perspectives of epithelial ovarian carcinoma. Oncol. Lett. 2016, 12, 3055–3058. [Google Scholar] [CrossRef] [PubMed]
- Ribatti, D.; Ranieri, G.; Annese, T.; Nico, B. Aquaporins in cancer. Biochim. Biophys. Acta (BBA) Gen. Subj. 2014, 1840, 1550–1553. [Google Scholar] [CrossRef]
- Wang, J.; Feng, L.; Zhu, Z.; Zheng, M.; Wang, D.; Chen, Z.; Sun, H. Aquaporins as diagnostic and therapeutic targets in cancer: How far we are? J. Transl. Med. 2015, 13, 96. [Google Scholar] [CrossRef] [PubMed]
- Tomita, Y.; Dorward, H.; Yool, A.J.; Smith, E.; Townsend, A.R.; Price, T.J.; Hardingham, J.E. Role of Aquaporin 1 Signalling in Cancer Development and Progression. Int. J. Mol. Sci. 2017, 18, 299. [Google Scholar] [CrossRef] [PubMed]
- Angelico, G.; Ieni, A.; Caltabiano, R.; Zeppa, P.; Tuccari, G. Aquaporin-1 expression in fluoro-edenite-induced mesothelioma effusions: An approach by cell-block procedure. Cytopathology 2018, 29, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Angelico, G.; Caltabiano, R.; Loreto, C.; Ieni, A.; Tuccari, G.; Ledda, C.; Rapisarda, V. Immunohistochemical Expression of Aquaporin-1 in Fluoro-Edenite-Induced Malignant Mesothelioma: A Preliminary Report. Int. J. Mol. Sci. 2018, 19, 685. [Google Scholar] [CrossRef]
- Mobasheri, A.; Airley, R.; Hewitt, S.M.; Marples, D. Heterogeneous expression of the aquaporin 1 (AQP1) water channel in tumors of the prostate, breast, ovary, colon and lung: A study using high density multiple human tumor tissue microarrays. Int. J. Oncol. 2005, 26, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.H.; Shi, Y.F.; Chen, X.D.; Qi, W.J. The influence of aquaporin-1 and microvessel density on ovarian carcinogenesis and ascites formation. Int. J. Gynecol. Cancer 2006, 16, 400–405. [Google Scholar] [CrossRef]
- Yang, J.-H.; Yu, Y.-Q.; Yan, C.-X. Localisation and expression of aquaporin subtypes in epithelial ovarian tumours. Histol. Histopathol. 2011, 26, 1197–1205. [Google Scholar]
- Takal, M.K.; Baykal, C.; Baser, E.; Kaya, M.D.; Dursun, P.; Ozen, O.; Haberal, A.N.; Ayhan, A. Does Aquaporin-1 expression have clinical significance in serous epithelial ovarian cancer? J. Turk. Gynecol. Assoc. 2013, 14, 130–135. [Google Scholar] [CrossRef]
- Xuejun, C.; Weimin, C.; Xiaoyan, D.; Wei, Z.; Qiong, Z.; Jianhua, Y. Effects of aquaporins on chemosensitivity to cisplatin in ovarian cancer cells. Arch. Gynecol. Obstet. 2014, 290, 525–532. [Google Scholar] [CrossRef]
- Wang, Y.; Fan, Y.; Zheng, C.; Zhang, X. Knockdown of AQP1 inhibits growth and invasion of human ovarian cancer cells. Mol. Med. Rep. 2017, 16, 5499–5504. [Google Scholar] [CrossRef] [PubMed]
- Chetry, M.; Li, S.; Liu, H.; Hu, X.; Zhu, X. Prognostic values of aquaporins mRNA expression in human ovarian cancer. Biosci. Rep. 2018, 38. [Google Scholar] [CrossRef]
- Sato, K.; Miyamoto, M.; Takano, M.; Furuya, K.; Tsuda, H. Different Prognostic Implications of Aquaporin-1 and Aquaporin-5 Expression among Different Histological Types of Ovarian Carcinoma. Pathol. Oncol. Res. 2018, 26, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Zannoni, G.F.; Angelico, G.; Santoro, A. Aberrant non-canonical WNT pathway as key-driver of high-grade serous ovarian cancer development. Virchows Archiv. 2020, 477, 321–322. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Pannone, G.; Papagerakis, S.; McGuff, H.S.; Cafarelli, B.; Lepore, S.; De Maria, S.; Rubini, C.; Mattoni, M.; Staibano, S.; et al. Beta-Catenin and Epithelial Tumors: A Study Based on 374 Oropharyngeal Cancers. BioMed Res. Int. 2014, 2014, 1–13. [Google Scholar] [CrossRef]
- Gamallo, C.; Palacios, J.; Moreno, G.; Calvo de Mora, J.; Suárez, A.; Armas, A. beta-catenin expression pattern in stage I and II ovarian carcinomas: Relationship with beta-catenin gene mutations, clinicopathological features, and clinical outcome. Am. J. Pathol. 1999, 155, 527–536. [Google Scholar] [CrossRef]
- Bodnar, L.; Stanczak, A.; Cierniak, S.; Smoter, M.; Cichowicz, M.; Kozlowski, W.; Szczylik, C.; Wieczorek, M.; Lamparska-Przybysz, M. Wnt/β-catenin pathway as a potential prognostic and predictive marker in patients with advanced ovarian cancer. J. Ovarian Res. 2014, 7, 16. [Google Scholar] [CrossRef]
- Wong, C.M.; Fan, S.T.; Ng, I.O. beta-Catenin mutation and overexpression in hepatocellular carcinoma: Clinicopathologic and prognostic significance. Cancer 2001, 92, 136–145. [Google Scholar] [CrossRef]
- Mahomed, F.; Altini, M.; Meer, S. Altered E-cadherin/beta-catenin expression in oral squamous carcinoma with and without nodal metastasis. Oral Dis. 2007, 13, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Chong, W.; Zhang, H.; Guo, Z.; Yang, L.; Shao, Y.; Liu, X.; Zhao, Y.; Wang, Z.; Zhang, M.; Guo, C.; et al. Aquaporin 1 promotes sensitivity of anthracycline chemotherapy in breast cancer by inhibiting β-catenin degradation to enhance TopoIIα activity. Cell Death Differ. 2021, 28, 382–400. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Qin, F.; Yang, L.; He, J.; Liu, X.; Shao, Y.; Guo, Z.; Zhang, M.; Li, W.; Fu, L.; et al. Combination of AQP1 and β-catenin expression is an independent prognosis factor in astrocytoma patients. Oncotarget 2017, 8, 99414–99428. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Imaizumi, H.; Ishibashi, K.; Takenoshita, S.; Ishida, H. Aquaporin 1 expression is associated with response to adjuvant chemo-therapy in stage II and III colorectal cancer. Oncol. Lett. 2018, 15, 6450–6456. [Google Scholar]
- Pan, X.-Y.; Guo, H.; Han, J.; Hao, F.; An, Y.; Xu, Y.; Xiaokaiti, Y.; Pan, Y.; Li, X.-J. Ginsenoside Rg3 attenuates cell migration via inhibition of aquaporin 1 expression in PC-3M prostate cancer cells. Eur. J. Pharmacol. 2012, 683, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhu, W. Effects of cetuximab combined with afatinib on the expression of KDR and AQP1 in lung cancer. Genet. Mol. Res. 2015, 14, 16652–16661. [Google Scholar] [CrossRef]
- Monzani, E.; Bazzotti, R.; Perego, C.; La Porta, C.A.M. AQP1 Is Not Only a Water Channel: It Contributes to Cell Migration through Lin7/Beta-Catenin. PLoS ONE 2009, 4, e6167. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Case | Age | Stage | AQP1 IHC | β-Catenin IHC | CRS | Follow-Up (Months) | Outcome |
|---|---|---|---|---|---|---|---|
| 1 | 49 | IIIC | 0 (Negative) | M | 3 | 60 | A |
| 2 | 42 | IV | 0 (Negative) | M | 3 | 60 | A |
| 3 | 73 | IV | 0 (Negative) | M | 3 | 30 | A |
| 4 | 37 | IIIC | 0 (Negative) | MC | 3 | 35 | A |
| 5 | 57 | IIIC | 0 (Negative) | M | 3 | 45 | A |
| 6 | 55 | IIIC | 0 (Negative) | M | 2 | 32 | A |
| 7 | 52 | IIIC | 0 (Negative) | M | 2 | 24 | A |
| 8 | 68 | IIIC | 0 (Negative) | MC | 2 | 20 | D |
| 9 | 45 | IIIC | 0 (Negative) | M | 2 | 60 | A |
| 10 | 48 | IV | 0 (Negative) | M | 2 | 60 | A |
| 11 | 71 | IIIC | 0 (Negative) | M | 1 | 20 | D |
| 12 | 63 | IIIC | 0 (Negative) | M | 1 | 30 | D |
| 13 | 58 | IIIC | 25 (Not uniform) | M | 1 | 40 | A |
| 14 | 73 | IIIC | 25 (Not uniform) | MC | 1 | 40 | A |
| 15 | 75 | IIIC | 25 (Not uniform) | MC | 1 | 12 | D |
| 16 | 68 | IIIC | 25 (Not uniform) | M | 1 | 20 | D |
| 17 | 46 | IIIC | 50 (Diffuse) | MC | 1 | 24 | A |
| 18 | 49 | IIIC | 50 (Diffuse) | MC | 1 | 24 | A |
| 19 | 55 | IIIC | 50 (Diffuse) | MC | 1 | 24 | A |
| 20 | 61 | IV | 50 (Diffuse) | MC | 1 | 32 | A |
| 21 | 75 | IIIC | 80 (Diffuse) | MC | 2 | 24 | A |
| 22 | 72 | IIIC | 80 (Diffuse) | MC | 2 | 20 | D |
| 23 | 48 | IIIC | 5 (Focal) | M | 2 | 20 | D |
| 24 | 53 | IIIC | 5 (Focal) | M | 2 | 16 | D |
| 25 | 57 | IIIC | 5 (Focal) | MC | 2 | 26 | A |
| 26 | 60 | IV | 5 (Focal) | MC | 2 | 40 | A |
| 27 | 63 | IIIC | 1 (Focal) | M | 2 | 60 | A |
| 28 | 52 | IIIC | 1 (Focal) | M | 2 | 60 | A |
| 29 | 59 | IIIC | 1 (Focal) | MC | 2 | 30 | A |
| 30 | 64 | IIIC | 1 (Focal) | MC | 2 | 24 | D |
| 31 | 66 | IIIC | 1 (Focal) | MC | 2 | 34 | A |
| 32 | 50 | IIIC | 1 (Focal) | MC | 2 | 31 | A |
| CRS | AQP1– | AQP1+ |
|---|---|---|
| 1–2 | 7 | 20 |
| 3 | 5 | 0 |
| Total patients | 12 | 20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelico, G.; Ieni, A.; Caltabiano, R.; Santoro, A.; Inzani, F.; Spadola, S.; Tuccari, G.; Macrì, A.; Zannoni, G.F. Evaluation of Beta-Catenin Subcellular Localization and Water Channel Protein AQP1 Expression as Predictive Markers of Chemo-Resistance in Ovarian High-Grade Serous Carcinoma: Comparative Study between Preoperative Peritoneal Biopsies and Surgical Samples. Diagnostics 2021, 11, 452. https://doi.org/10.3390/diagnostics11030452
Angelico G, Ieni A, Caltabiano R, Santoro A, Inzani F, Spadola S, Tuccari G, Macrì A, Zannoni GF. Evaluation of Beta-Catenin Subcellular Localization and Water Channel Protein AQP1 Expression as Predictive Markers of Chemo-Resistance in Ovarian High-Grade Serous Carcinoma: Comparative Study between Preoperative Peritoneal Biopsies and Surgical Samples. Diagnostics. 2021; 11(3):452. https://doi.org/10.3390/diagnostics11030452
Chicago/Turabian StyleAngelico, Giuseppe, Antonio Ieni, Rosario Caltabiano, Angela Santoro, Frediano Inzani, Saveria Spadola, Giovanni Tuccari, Antonio Macrì, and Gian Franco Zannoni. 2021. "Evaluation of Beta-Catenin Subcellular Localization and Water Channel Protein AQP1 Expression as Predictive Markers of Chemo-Resistance in Ovarian High-Grade Serous Carcinoma: Comparative Study between Preoperative Peritoneal Biopsies and Surgical Samples" Diagnostics 11, no. 3: 452. https://doi.org/10.3390/diagnostics11030452
APA StyleAngelico, G., Ieni, A., Caltabiano, R., Santoro, A., Inzani, F., Spadola, S., Tuccari, G., Macrì, A., & Zannoni, G. F. (2021). Evaluation of Beta-Catenin Subcellular Localization and Water Channel Protein AQP1 Expression as Predictive Markers of Chemo-Resistance in Ovarian High-Grade Serous Carcinoma: Comparative Study between Preoperative Peritoneal Biopsies and Surgical Samples. Diagnostics, 11(3), 452. https://doi.org/10.3390/diagnostics11030452