
Acceptability and Usability of HCV Self-Testing in High Risk Populations in Vietnam

 , ,
, ,
Abstract
1. Introduction
2. Objective
3. Material and Methods
3.1. Study Design and Sample Size
3.2. Setting and Participant Recruitment
3.3. Study Population—Eligibility Criteria
3.4. Study Procedures
3.5. Data Analysis
3.6. Ethical Approval
4. Results
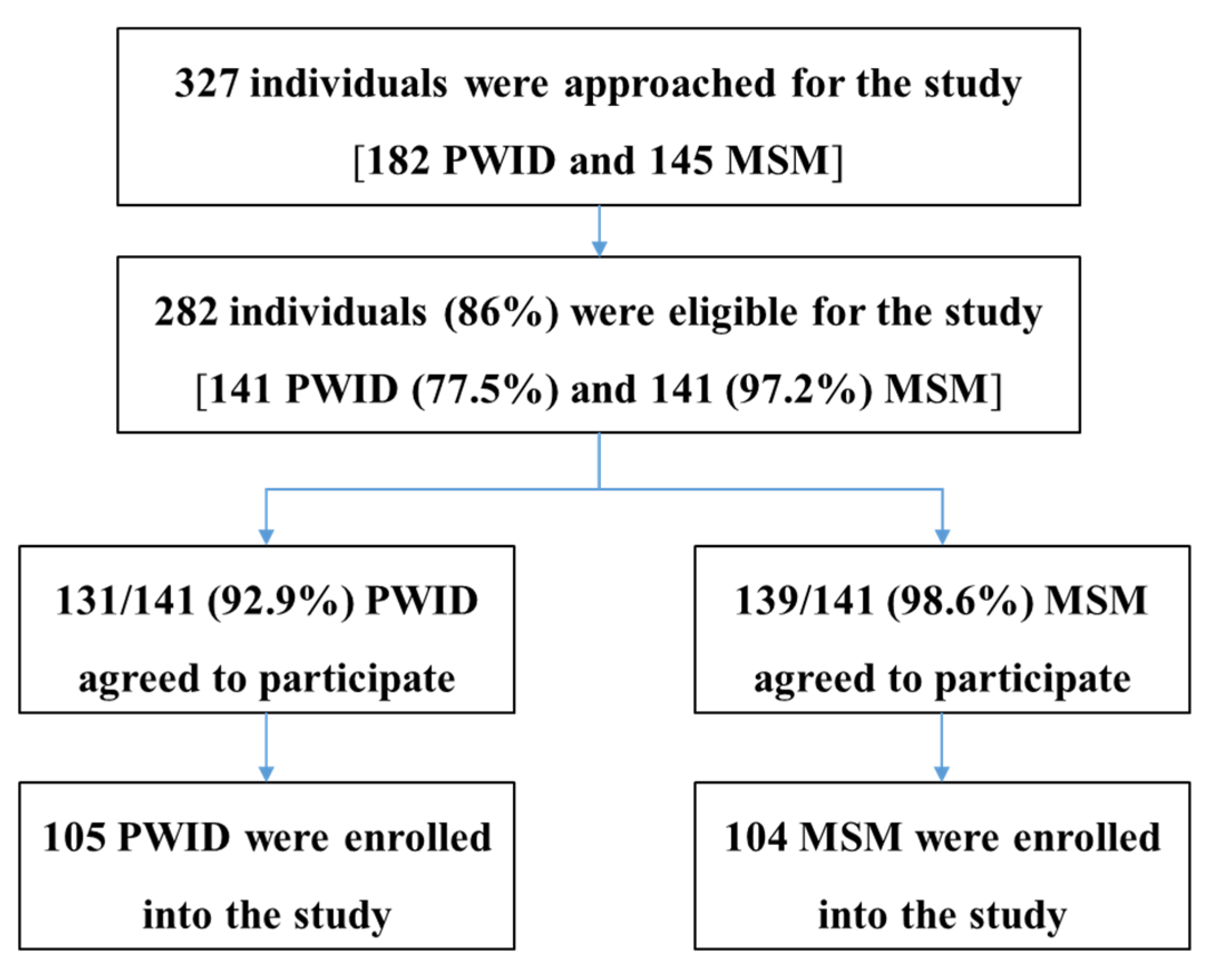
4.1. Patient Recruitment and Characteristics
4.2. Usability of Self-Testing Performed by Participants
4.3. HCV Testing Results
4.4. Acceptability and User Perspectives on HCVST
5. Discussion
5.1. Summary of Findings
5.1.1. Usability
5.1.2. Concordance of Results
5.1.3. Acceptability
5.2. The Performance and Applicability of OraQuick HCV Antibody Self-Test
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Hepatitis Report 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Ho, S.Y.; Su, L.H.; Sun, H.Y.; Huang, Y.S.; Chuang, Y.C.; Huang, M.H.; Liu, W.C.; Su, Y.C.; Lin, P.H.; Chang, S.Y.; et al. Trends of recent hepatitis C virus infection among HIV-positive men who have sex with men in Taiwan, 2011–2018. EClinicalMedicine 2020, 24, 100441. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for the Western Pacific. Viral Hepatitis Situation and Response in Viet Nam; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Zhang, L.; Celentano, D.D.; Le Minh, N.; Latkin, C.A.; Mehta, S.H.; Frangakis, C.; Ha, T.V.; Mo, T.T.; Sripaipan, T.; Davis, W.W.; et al. Prevalence and correlates of HCV monoinfection and HIV and HCV coinfection among persons who inject drugs in Vietnam. Eur. J. Gastroenterol. Hepatol. 2015, 27, 550–556. [Google Scholar] [CrossRef][Green Version]
- Nguyen Truong, T.; Laureillard, D.; Lacombe, K.; Duong Thi, H.; Pham Thi Hanh, P.; Truong Thi Xuan, L.; Chu Thi, N.; Luong Que, A.; Vu Hai, V.; Nagot, N.; et al. High Proportion of HIV-HCV Coinfected Patients with Advanced Liver Fibrosis Requiring Hepatitis C Treatment in Haiphong, Northern Vietnam (ANRS 12262). PLoS ONE 2016, 11, e0153744. [Google Scholar] [CrossRef] [PubMed]
- Nadol, P.; O’Connor, S.; Duong, H.; Mixson-Hayden, T.; Tram, T.H.; Xia, G.L.; Kaldor, J.; Law, M.; Nguyen, T. High hepatitis C virus (HCV) prevalence among men who have sex with men (MSM) in Vietnam and associated risk factors: 2010 Vietnam Integrated Behavioural and Biologic Cross-Sectional Survey. Sex. Transm. Infect. 2016, 92, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Berto, A.; Day, J.; Van Vinh Chau, N.; Thwaites, G.E.; My, N.N.; Baker, S.; Darton, T.C. Current challenges and possible solutions to improve access to care and treatment for hepatitis C infection in Vietnam: A systematic review. BMC Infect. Dis. 2017, 17, 260. [Google Scholar] [CrossRef] [PubMed]
- Dunford, L.; Carr, M.J.; Dean, J.; Waters, A.; Nguyen, L.T.; Ta Thi, T.H.; Thi, L.A.; Do, H.D.; Thi, T.T.; Nguyen, H.T.; et al. Hepatitis C virus in Vietnam: High prevalence of infection in dialysis and multi-transfused patients involving diverse and novel virus variants. PLoS ONE 2012, 7, e41266. [Google Scholar] [CrossRef] [PubMed]
- Pawlotsky, J.M. New hepatitis C therapies: The toolbox, strategies, and challenges. Gastroenterology 2014, 146, 1176–1192. [Google Scholar] [CrossRef] [PubMed]
- Feeney, E.R.; Chung, R.T. Antiviral treatment of hepatitis C. BMJ 2014, 348, g3308. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines on Hepatitis B and C Testing; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Johnson, C.C.; Kennedy, C.; Fonner, V.; Siegfried, N.; Figueroa, C.; Dalal, S.; Sands, A.; Baggaley, R. Examining the effects of HIV self-testing compared to standard HIV testing services: A systematic review and meta-analysis. J. Int. AIDS Soc. 2017, 20, 21594. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Li, X.; Brecht, M.L.; Koniak-Griffin, D. Can self-testing increase HIV testing among men who have sex with men: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0188890. [Google Scholar] [CrossRef] [PubMed]
- Krause, J.; Subklew-Sehume, F.; Kenyon, C.; Colebunders, R. Acceptability of HIV self-testing: A systematic literature review. BMC Public Health 2013, 13, 735. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, C.; Johnson, C.; Ford, N.; Sands, A.; Dalal, S.; Meurant, R.; Prat, I.; Hatzold, K.; Urassa, W.; Baggaley, R. Reliability of HIV rapid diagnostic tests for self-testing compared with testing by health-care workers: A systematic review and meta-analysis. Lancet HIV 2018, 5, e277–e290. [Google Scholar] [CrossRef]
- Pant Pai, N.; Sharma, J.; Shivkumar, S.; Pillay, S.; Vadnais, C.; Joseph, L.; Dheda, K.; Peeling, R.W. Supervised and unsupervised self-testing for HIV in high- and low-risk populations: A systematic review. PLoS Med. 2013, 10, e1001414. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines on HIV Self-testing and Partner Notification: Supplement to Consolidated Guidelines on HIV Testing Services; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. WHO List of Prequalified In Vitro Diagnostic Products. Available online: https://www.who.int/diagnostics_laboratory/evaluations/190121_prequalified_product_list.pdf?ua=1 (accessed on 6 November 2020).
- Nguyen, V.T.T.; Phan, H.T.T.; Kato, M.; Nguyen, Q.; Le Ai, K.A.; Vo, S.H.; Thanh, D.C.; Baggaley, R.C.; Johnson, C.C. Community-led HIV testing services including HIV self-testing and assisted partner notification services in Vietnam: Lessons from a pilot study in a concentrated epidemic setting. J. Int. AIDS Soc. 2019, S3, e25301. [Google Scholar] [CrossRef]
- Kimble, M.M.; Stafylis, C.; Treut, P.; Saab, S.; Klausner, J.D. Clinical evaluation of a hepatitis C antibody rapid immunoassay on self-collected oral fluid specimens. Diagn. Microbiol. Infect. Dis. 2019, 95, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Guise, A.; Witzel, T.C.; Mandal, S.; Sabin, C.; Rhodes, T.; Nardone, A.; Harris, M. A qualitative assessment of the acceptability of hepatitis C remote self-testing and self-sampling amongst people who use drugs in London, UK. BMC Infect. Dis. 2018, 18, 281. [Google Scholar] [CrossRef]
- Tang, W.; Chen, W.; Amini, A.; Boeras, D.; Falconer, J.; Kelly, H.; Peeling, R.; Varsaneux, O.; Tucker, J.D.; Easterbrook, P. Diagnostic accuracy of tests to detect Hepatitis C antibody: A meta-analysis and review of the literature. BMC Infect. Dis. 2017, 17 (Suppl. 1), 695. [Google Scholar] [CrossRef]
- PEPFAR. VIETNAM Country/Regional Operational Plan (COP/ROP) 2016: Strategic Direction Summary. 2016. Available online: https://mz.usembassy.gov/wp-content/uploads/sites/182/2017/04/PEPFAR-cop16-Guidance.pdf (accessed on 20 May 2020).
- Vietnam Ministry of Health. Community-Based Counselling and Testing Guidelines; Ministry of Health: Hanoi, Vietnam, 2018.




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | PWID (n = 105) | MSM (n = 104) | p Value | |
|---|---|---|---|---|
| Age, years, median (range) | 45 (31–62) | 22 (18–26) | <0.0001 | |
| Sex, % (n) | ||||
| Male | 98.1 (103) | 100.0 (104) | 0.497 | |
| Female | 1.9 (2) | 0 | ||
| Education, % (n) | <0.0001 | |||
| Primary school | 6.7 (7) | 0 | ||
| Secondary school | 55.2 (58) | 0 | ||
| High school | 37.1 (39) | 12.5 (13) | ||
| College | 1.0 (1) | 87.5 (91) | ||
| Occupation, % (n) | <0.0001 | |||
| Unemployed | 48.6 (51) | 2.9 (3) | ||
| Employed | 51.4 (54) | 97.1 (101) | ||
| Marital status, % (n) | <0.0001 | |||
| Married or living with a partner | 57.1 (60) | 2.9 (3) | ||
| Divorced, separated or widow | 17.1 (18) | 1.0 (1) | ||
| Unmarried | 25.7 (27) | 96.2 (100) | ||
| Self-reported exposures (ever) to any following risk factors for HCV infection, % (n) | ||||
| Injecting non-prescribed drugs | 100.0 (105) | 0 | <0.0001 | |
| Sharing needles | 46.7 (49) | 0 | <0.0001 | |
| Condomless anal intercourse | 6.7 (7) | 100 (104) | <0.0001 | |
| A surgical procedure | 11.4 (12) | 15.4 (16) | 0.424 | |
| A dental procedure | 27.6 (29) | 45.2 (47) | 0.009 | |
| Sharing shaving tools or toothbrushes | 25.7 (27) | 28.8 (30) | 0.643 | |
| Having a tattoo | 32.4 (34) | 6.7 (7) | <0.0001 | |
| Aware of the existence of self-tests performed at home, % (n) | 32.4 (34) | 87.5 (91) | <0.0001 | |
| Previous use of self-test, % (n) | 1.0 (1) | 0 | 1.000 | |
| Testing Steps | PWID | MSM | p Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Pretesting | |||||
| 1. Opening the pouch and taking all contents out | 0 | 0 | 0 | 0 | |
| 2. Reading/using the instructions for use | 2 | 1.9 | 0 | 0 | 0.498 |
| 3. Removing the test tube from the pack | 0 | 0 | 0 | 0 | |
| 4. Removing the cap from the test tube | 2 | 1.9 | 0 | 0 | 0.498 |
| 5. Sliding the test tube into the stand | 1 | 1 | 1 | 1 | 1.000 |
| 6. Pouring the fluid from the test tube into the stand | 4 | 3.8 | 1 | 1 | 0.369 |
| 7. Removing the test device from the pack | 0 | 0 | 0 | 0 | |
| Conduct of Test | |||||
| 8. Touching the test pad | 7 | 6.7 | 4 | 3.8 | 0.538 |
| 9. Incorrectly collecting oral fluid sample * | 39 | 37.1 | 14 | 13.5 | 0.0001 |
| 10. Wrong placing the test device in the test tube | 3 | 2.9 | 1 | 1 | 0.621 |
| 11. Test device coming out of the tube while testing | 0 | 0 | 0 | 0 | |
| 12. Not reading the result between 20 and 40 min | 4 | 3.8 | 2 | 1.9 | 0.683 |
| Test Interpretation | |||||
| 13. Wrong interpreting the test result ** | 21 | 20 | 1 | 1 | <0.0001 |
| Testing Step, % (n) | Difficulty Observed | Assistance Provided | ||||
|---|---|---|---|---|---|---|
| PWID | MSM | p | PWID * | MSM | p | |
| n = 105 | n = 104 | n = 105 | n = 104 | |||
| Opening the pouch and taking all the contents out | 6.7 (7) | 4.8 (5) | 0.768 | 15.2 (16) | 2.9 (3) | 0.003 |
| Reading/using the instructions for use | NA | NA | 16.2 (17) | 0 (0) | <0.0001 | |
| Removing the cap from the test tube | 21.0 (22) | 19.2 (20) | 0.863 | 21.9 (23) | 1 (1) | <0.0001 |
| Sliding the test tube into the stand | 11.4 (12) | 1.9 (2) | 0.01 | 17.1 (18) | 0 (0) | |
| Collecting the oral fluid sample | NA | NA | 21.9 (23) | 0 (0) | <0.0001 | |
| Placing the test device in the test tube | 1.0 (1) | 1.9 (2) | 0.621 | 15.2 (16) | 1.9 (2) | 0.0008 |
| Interpreting the test result | 13.3 (14) | 1.9 (2) | 0.003 | 26.7 (28) | 2.9 (3) | <0.0001 |
| Demographic Characteristics | Mistake | Difficulty | Assistance | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | p | n | % | p | n | % | p | |
| Age, years, median (range) | |||||||||
| <22 (N = 51) | 21 | 41.2 | 0.0012 | 15 | 29.4 | 0.0030 | 9 | 17.6 | <0.0001 |
| 22–45 (N = 107) | 44 | 41.1 | 40 | 37.4 | 41 | 38.3 | |||
| >45 (N = 51) | 36 | 70.6 | 31 | 60.8 | 38 | 74.5 | |||
| Sex, % (n) | |||||||||
| Male (N = 207) | 48.8 | 101 | 41.1 | 85 | 42.0 | 87 | |||
| Female (N = 2) | 0.0 | 0 | 50.0 | 1 | 50.0 | 1 | |||
| Educational level, % (n) | |||||||||
| Primary school (N = 7) | 4 | 57.1 | 0.0001 | 5 | 71.4 | 0.0010 | 6 | 85.7 | <0.0001 |
| Intermediate school (N = 58) | 41 | 70.7 | 33 | 56.9 | 43 | 74.1 | |||
| Secondary school (N = 62) | 27 | 43.5 | 23 | 37.1 | 22 | 35.5 | |||
| College (N = 92) | 29 | 31.5 | 25 | 27.2 | 17 | 18.5 | |||
| Occupation, % (n) | |||||||||
| Unemployed (N = 54) | 32 | 59.3 | 0.0875 | 25 | 46.3 | 0.4641 | 29 | 53.7 | 0.0651 |
| Employed (N = 155) | 69 | 44.5 | 61 | 39.4 | 59 | 38.1 | |||
| Marital status, % (n) | |||||||||
| Married or living with a partner (N = 63) | 46 | 73.0 | <0.0001 | 38 | 60.3 | 0.0011 | 39 | 61.9 | <0.0001 |
| Divorced, separated or widow (N = 19) | 7 | 36.8 | 6 | 31.6 | 12 | 63.2 | |||
| Unmarried (N = 127) | 48 | 37.8 | 42 | 33.1 | 37 | 29.1 | |||
| PWID (n) | Rereading by Trained Staff (Inter-Reader) | Retesting by Trained Staff (Inter-Operator) | |||||||
| Positive | Negative | Invalid | Unsure | Positive | Negative | Invalid | Unsure | ||
| Self-Testing | Positive | 64 | 0 | 0 | 0 | 64 | 0 | 0 | 0 |
| Negative | 5 | 25 | 0 | 0 | 8 | 22 | 0 | 0 | |
| Invalid | 0 | 0 | 4 | 0 | 2 | 2 | 0 | 0 | |
| Unsure | 4 | 0 | 3 | 0 | 7 | 0 | 0 | 0 | |
| Concordance (%) | Between self-testing and rereading: 88.6% | Between self-testing and retesting: 81.9% | |||||||
| Cohen’s Kappa | 0.77 | 0.61 | |||||||
| MSM (n) | Rereading by Trained Staff (Inter-Reader) | Retesting by Trained Staff (Inter-Operator) | |||||||
| Positive | Negative | Invalid | Unsure | Positive | Negative | Invalid | Unsure | ||
| Self-Testing | Positive | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Negative | 1 | 102 | 0 | 0 | 0 | 103 | 0 | 0 | |
| Invalid | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | |
| Unsure | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Concordance (%) | Between self-testing and rereading: 99% | Between self-testing and retesting: 99% | |||||||
| Cohen’s Kappa | 0.66 | 0.99 * | |||||||
| Study ID | Self-Testing | Rereading | Retesting | Touching the Pad | Collecting Oral Fluid Sample | Assistance to Interpret Result | Observations for Discordant Results |
|---|---|---|---|---|---|---|---|
| Wrong Result Interpretation by Participants (n = 6) | |||||||
| PWID-011 | Negative | Positive | Positive | No | Correct | Yes | Participant did not understand the instruction |
| PWID-022 | Negative | Positive | Positive | No | Correct | No | |
| PWID-048 | Negative | Weak Positive | Positive | No | Correct | Yes | Participant had poor eyesight |
| PWID-082 | Negative | Positive | Positive | No | Incorrect | Yes | Participant placed device on the tongue and swabbed the teeth |
| PWID-097 | Negative | Weak positive | Negative | No | Incorrect | No | Participant placed device on the tongue |
| MSM-062 | Negative | Weak Positive | Negative | No | Correct | Yes | |
| Correct Result Interpretation by Participant but Retesting Result Differing from Self-Testing Result (n = 4) | |||||||
| PWID-073 | Negative | Negative | Positive | No | Correct | No | |
| PWID-075 | Negative | Negative | Positive | No | Incorrect | No | Participant swabbed the teeth |
| PWID-105 | Negative | Negative | Weak positive | No | Correct | No | |
| PWID-106 | Negative | Negative | Positive | No | Incorrect | No | Participant swabbed tongue and teeth |
| Correct Interpretation of Invalid Results in Self-Testing (n = 5) | |||||||
| PWID-010 | Invalid | Invalid | Positive | No | Correct | No | |
| PWID-077 | Invalid | Invalid | Positive | No | Correct | No | |
| PWID-017 | Invalid | Invalid | Negative | No | Incorrect | No | Participant swabbed on one gum only |
| PWID-054 | Invalid | Invalid | Negative | No | Incorrect | No | Participant did not use the whole pad |
| MSM-066 | Invalid | Invalid | Negative | Yes | Incorrect | No | Participant did not swab firmly enough |
| Unsure How to Interpret the Results in Self-Testing (n = 7) | |||||||
| PWID-036 | Unsure | Positive | Positive | No | Correct | Yes | Participant had poor eyesight |
| PWID-052 | Unsure | Positive | Positive | No | Correct | Yes | Participant had poor eyesight |
| PWID-053 | Unsure | Positive | Positive | No | Correct | Yes | |
| PWID-092 | Unsure | Positive | Positive | No | Incorrect | No | Participant did not use the whole pad |
| PWID-043 | Unsure | Invalid | Positive | No | Correct | Yes | |
| PWID-059 | Unsure | Invalid | Positive | No | Correct | No | Participant had poor eyesight |
| PWID-064 | Unsure | Invalid | Positive | No | Correct | No | |
| % (n) | PWID | MSM | p Value | |
|---|---|---|---|---|
| Acceptability, % (n) | n = 105 | n = 104 | ||
| Before self-testing | ||||
| The proportion of participants among eligible subjects who agreed to participate and perform HCV self-testing | 92.9 (131/141) | 98.6 (139/141) | 0.034 | |
| Ready to use HCV self-test if available | 98.1 (103) | 100.0 (104) | 0.498 | |
| After self-testing | ||||
| Willing to use HCV test again | 91.4 (96) | 98.1 (102) | 0.058 | |
| Willing to recommend the test to family and friends | 99 (104) | 97.1 (101) | 0.369 | |
| Taking the tests to family member/friend | 99.0 (104) | 97.1 (101) | 0.503 | |
| Preferences on HCVST, % (n) | n = 105 | n = 104 | ||
| Preferred approach to test for HCV in the future | ||||
| By myself at home | 69.5 (73) | 76.9 (80) | 0.275 | |
| By myself at a health center | 7.6 (8) | 10.6 (11) | 0.481 | |
| In a community center by a healthcare worker | 8.6 (9) | 5.8 (6) | 0.593 | |
| In a screening campaign | 0 (0) | 2.9 (3) | 0.121 | |
| Preferred sample type | ||||
| Prefer oral fluid-based test | 79 (83) | 67.3 (70) | 0.416 | |
| Prefer blood-based test | 10.5 (11) | 26.9 (28) | ||
| No preference | 10.5 (11) | 5.8 (6) | ||
| Steps to take if results of self-test reactive | ||||
| Contact healthcare facility | 95.2 (100) | 83.7 (87) | 0.006 | |
| Contact pharmacy | 1.9 (2) | 1.9 (2) | 1.000 | |
| Do a confirmatory test | 28.6 (30) | 57.7 (60) | <0.0001 | |
| Seek advice from a family member/community | 13.3 (14) | 11.5 (12) | 0.831 | |
| Do not know | 1.0 (1) | 0 (0) | 1.000 | |
| Knowledge about HCV treatment | ||||
| Know that HCV can be cured | 64.8 (68) | 55.8 (58) | 0.205 | |
| Know that there is a treatment but not sure about the cure | 10.5 (11) | 19.2 (20) | 0.083 | |
| Not sure if there is treatment | 4.8 (5) | 8.7 (9) | 0.284 | |
| There is no treatment or cure | 0 (0) | 1.9 (2) | 0.246 | |
| Usability, % (n) | ||||
| Correctly completing self-testing without any mistake | 37.1 (39) | 66.3 (69) | <0.0001 | |
| Correctly collecting oral fluid | 62.9 (66) | 86.5 (90) | 0.0001 | |
| Correctly interpreting the self-test results | 80 (84) | 99 (103) | <0.0001 | |
| Completing self-test procedure without difficulty | 46.7 (49) | 71.2 (74) | 0.0004 | |
| Completing self-test procedure without assistance | 33.3 (35) | 82.7 (86) | <0.0001 | |
| Concordance of Results | ||||
| Inter-reader agreement | ||||
| Concordance, % (n) | 88.6% (93) | 99% (103) | 0.005 | |
| Kappa value | 0.77 | 0.66 | ||
| Inter-operator agreement | ||||
| Concordance, % (n) | 81.9% (86) | 99% (103) | <0.0001 | |
| Kappa value | 0.61 | 0.99 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, L.T.; Nguyen, V.T.T.; Le Ai, K.A.; Truong, M.B.; Tran, T.T.M.; Jamil, M.S.; Johnson, C.; Reipold, E.I.; Easterbrook, P.; Park, K. Acceptability and Usability of HCV Self-Testing in High Risk Populations in Vietnam. Diagnostics 2021, 11, 377. https://doi.org/10.3390/diagnostics11020377
Nguyen LT, Nguyen VTT, Le Ai KA, Truong MB, Tran TTM, Jamil MS, Johnson C, Reipold EI, Easterbrook P, Park K. Acceptability and Usability of HCV Self-Testing in High Risk Populations in Vietnam. Diagnostics. 2021; 11(2):377. https://doi.org/10.3390/diagnostics11020377
Chicago/Turabian StyleNguyen, Linh Thuy, Van Thi Thuy Nguyen, Kim Anh Le Ai, Minh Binh Truong, Tam Thi Minh Tran, Muhammad S. Jamil, Cheryl Johnson, Elena Ivanova Reipold, Philippa Easterbrook, and Kidong Park. 2021. "Acceptability and Usability of HCV Self-Testing in High Risk Populations in Vietnam" Diagnostics 11, no. 2: 377. https://doi.org/10.3390/diagnostics11020377
APA StyleNguyen, L. T., Nguyen, V. T. T., Le Ai, K. A., Truong, M. B., Tran, T. T. M., Jamil, M. S., Johnson, C., Reipold, E. I., Easterbrook, P., & Park, K. (2021). Acceptability and Usability of HCV Self-Testing in High Risk Populations in Vietnam. Diagnostics, 11(2), 377. https://doi.org/10.3390/diagnostics11020377