
Selective Surface Electrostimulation of the Denervated Zygomaticus Muscle

 ,
,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Study Characteristics
2.2. Study Timeline
2.3. Study Aims
2.4. Population
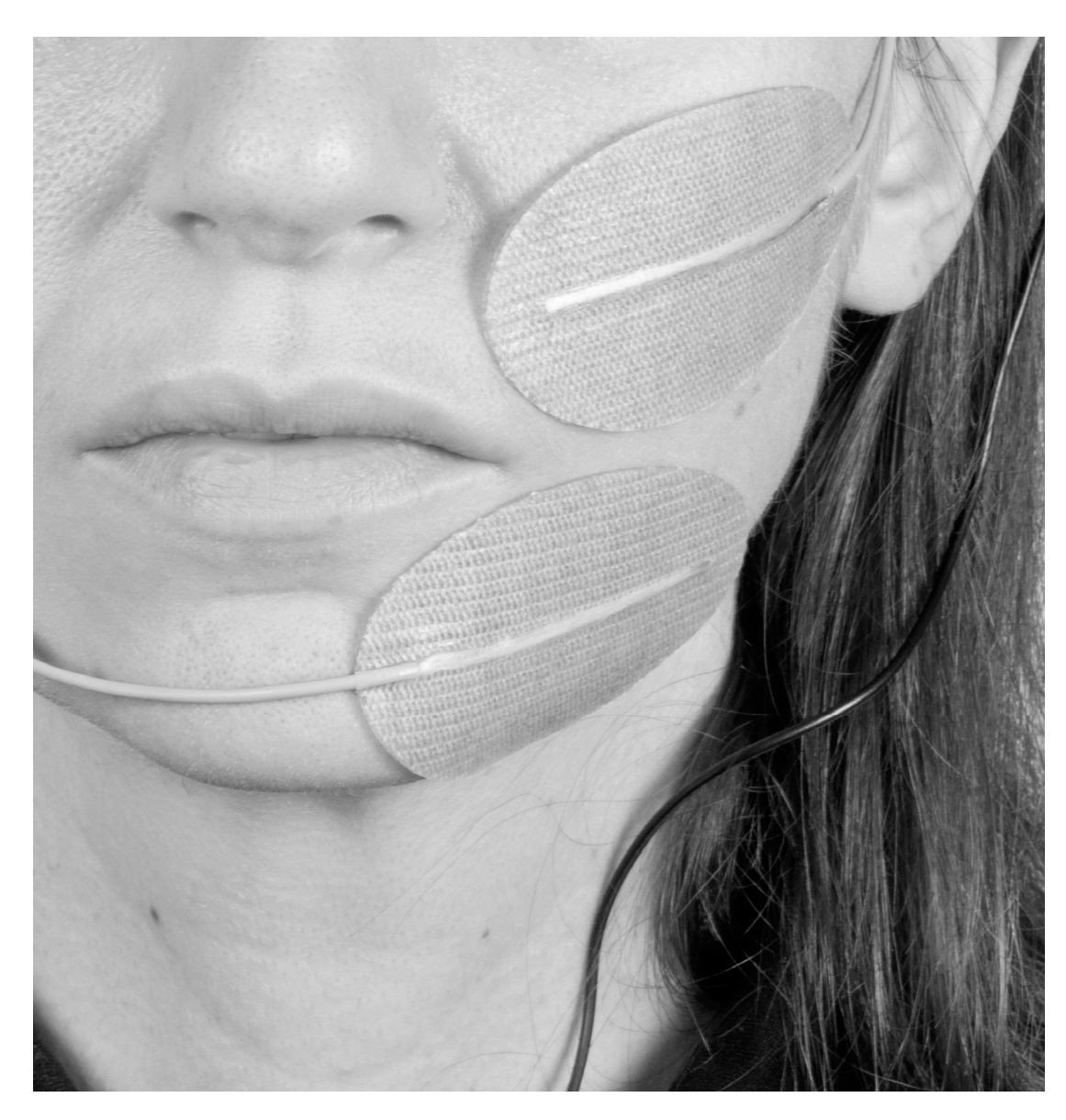
2.5. Electrode Placement
2.6. Stimulation Parameters
2.7. Outcome Measures
2.8. Parameter/Electrode Position Adjustment
2.9. Statistical Analysis
3. Results
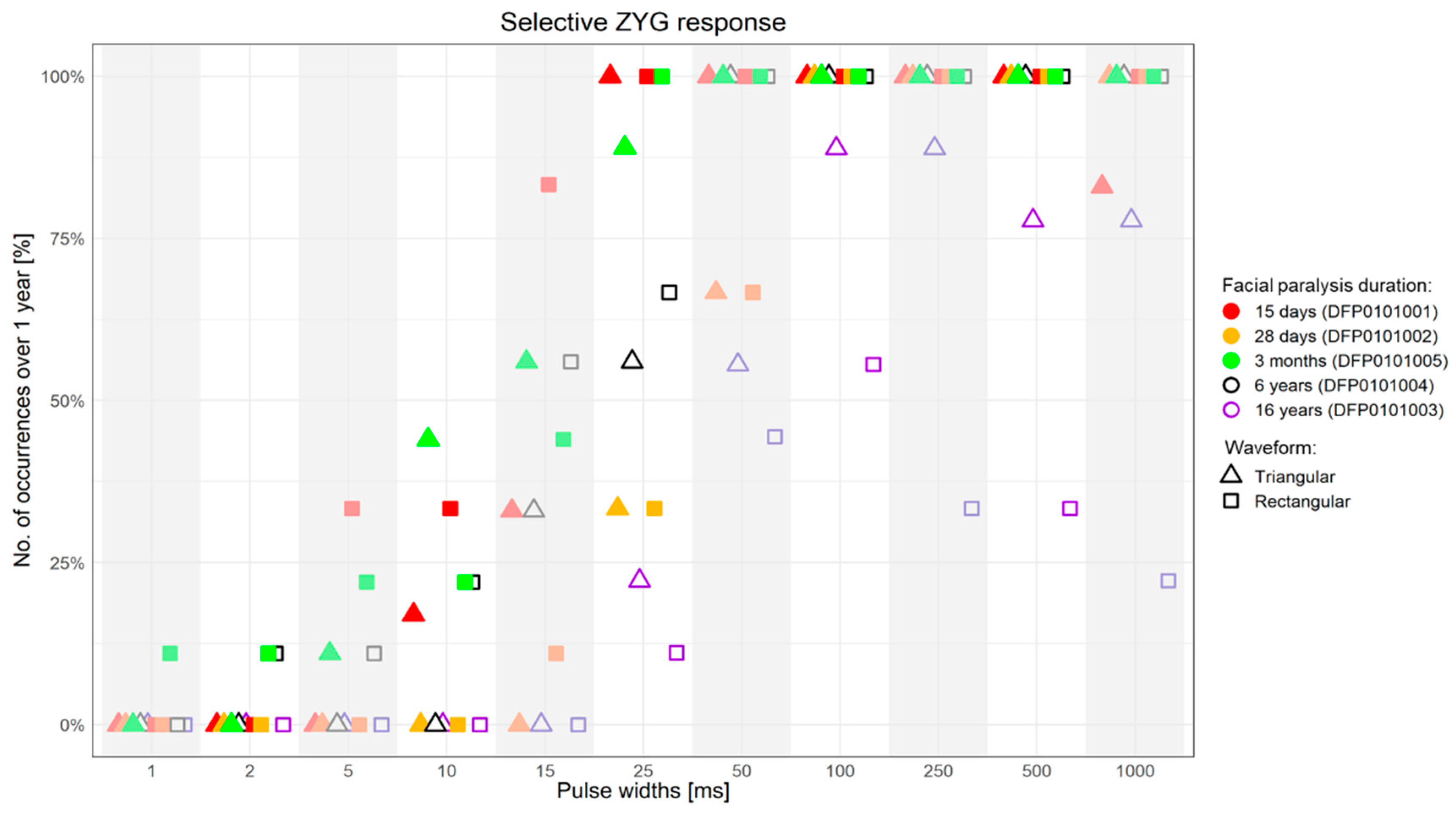
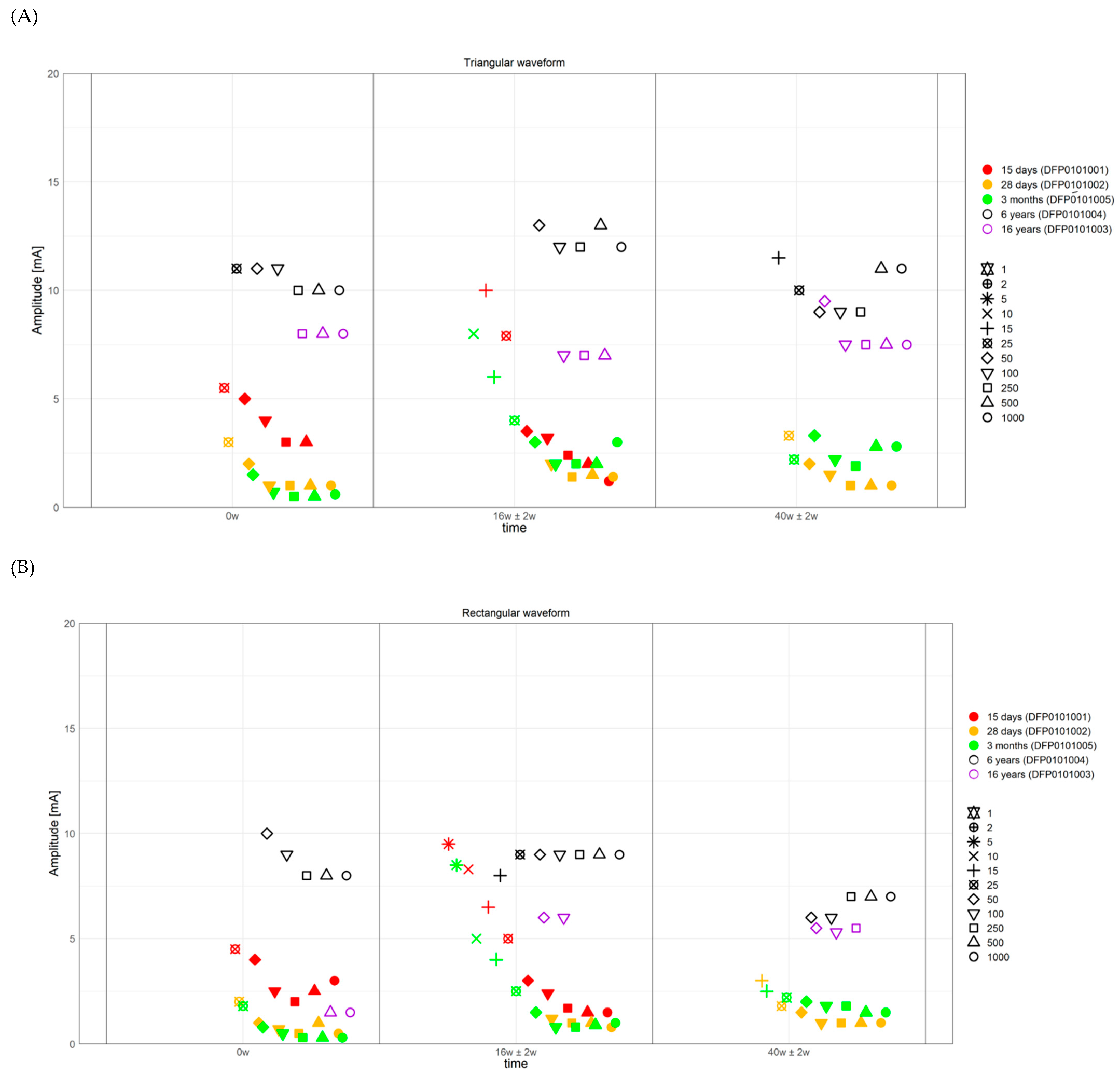
3.1. ZYG Response to Triangular and Rectangular Wave Stimulation
3.2. Use of Trains of Stimulation Bursts
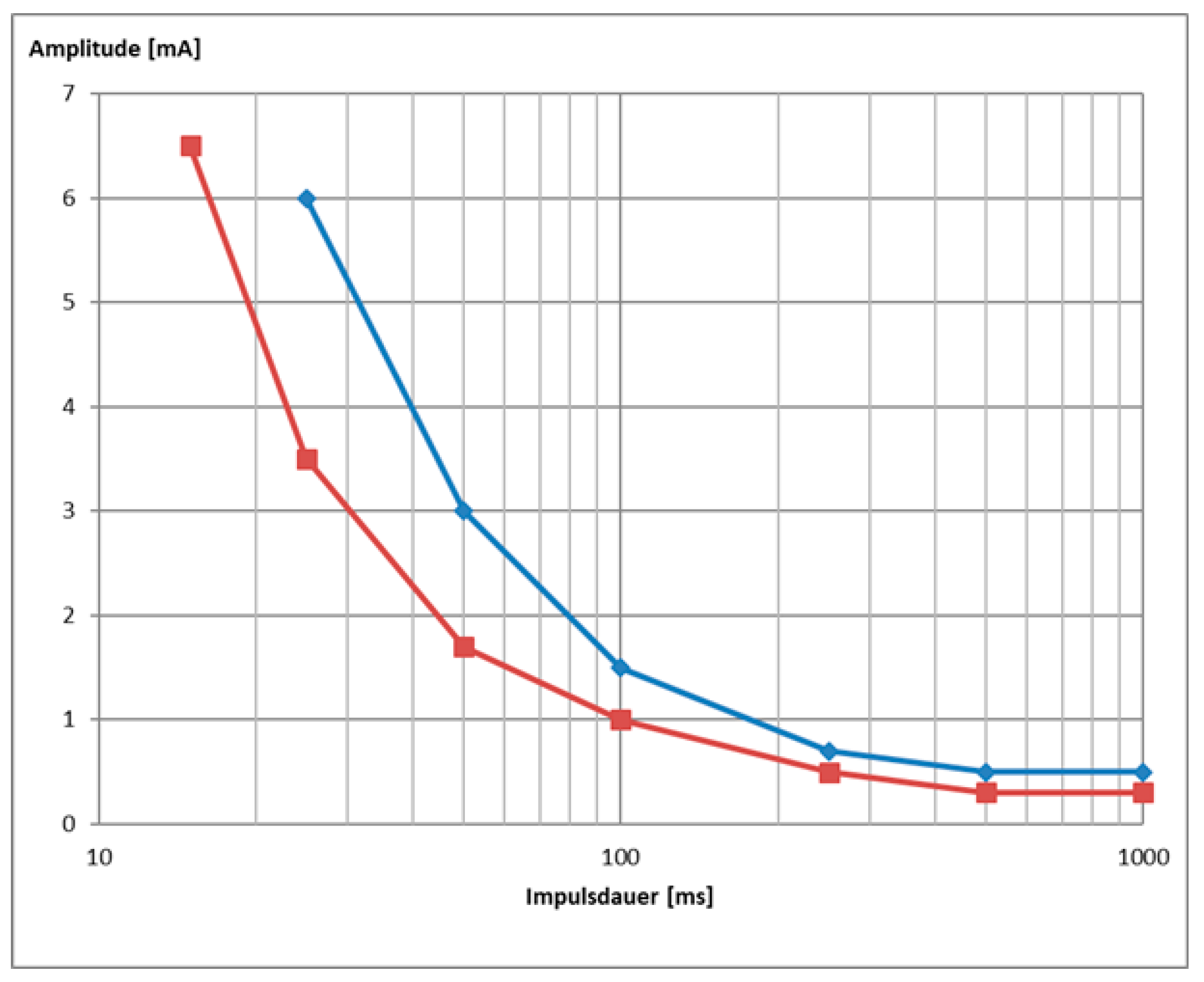
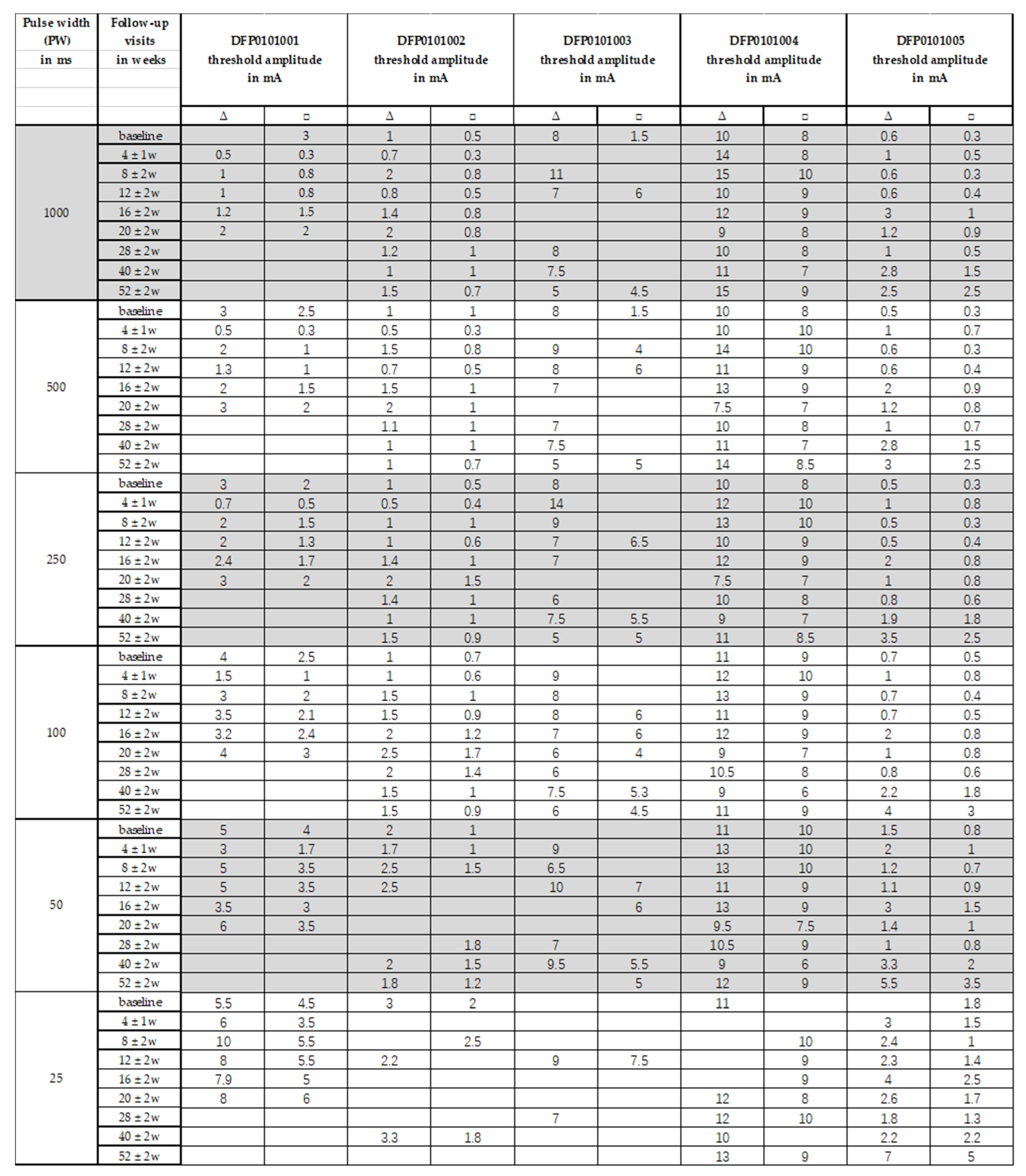
3.3. Strength/Duration Curves
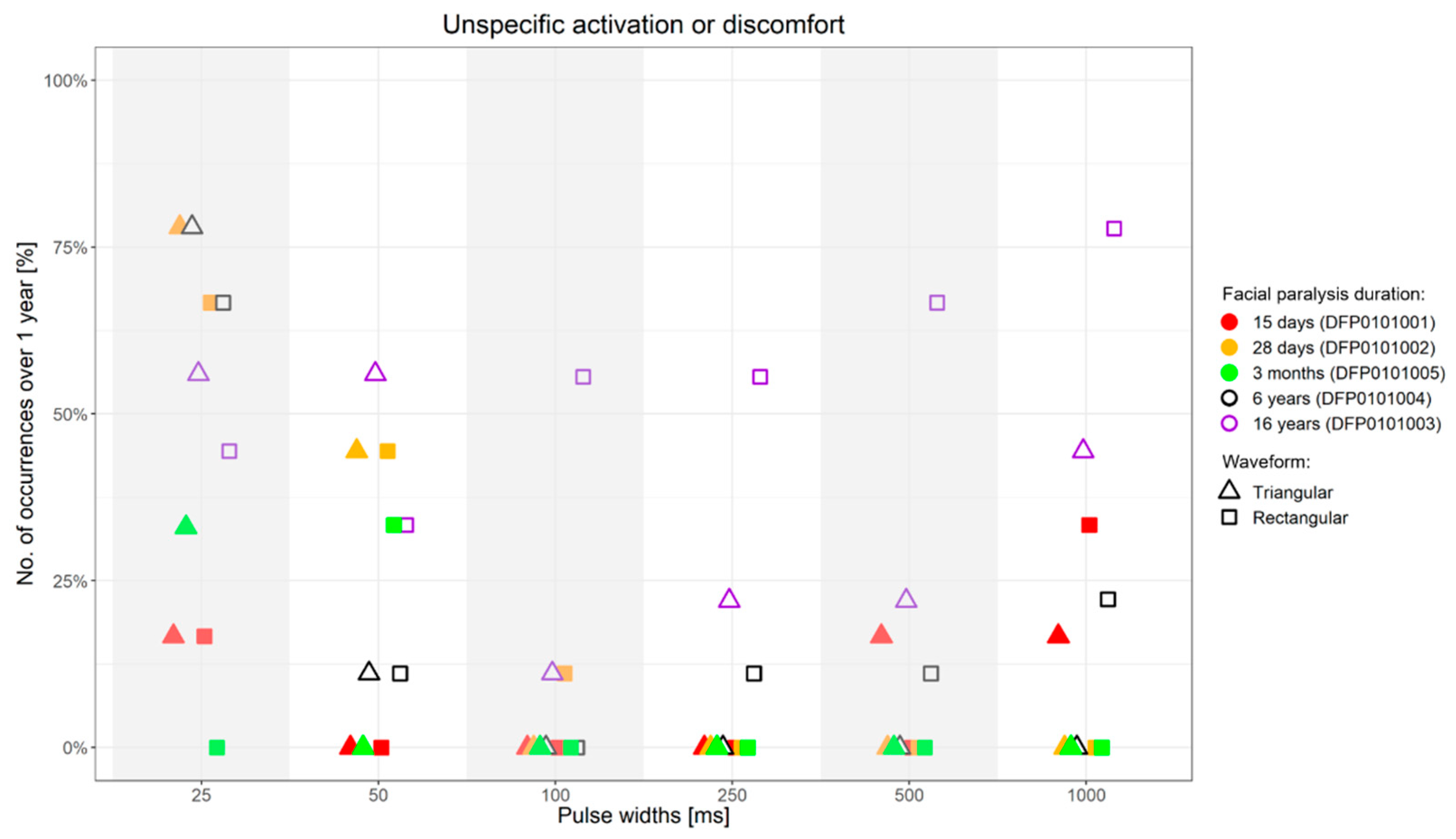
3.4. Side-Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, Y.S.; Choi, J.E.; Kim, S.W.; Baek, S.Y.; Cho, Y.S. Prevalence and associated factors of facial palsy and lifestyle characteristics: Data from the Korean National Health and Nutrition Examination Survey 2010–2012. BMJ Open 2016, 6, e012628. [Google Scholar] [CrossRef] [PubMed]
- Junior, N.; Junior, J.; Gignon, V.; Kitice, A.; Prado, L.; Santos, V. Facial Nerve Palsy: Incidence of Different Ethiologies in a Tertiary Ambulatory. Int. Arch. Otorhinolaryngol. 2009, 13, 167–171. [Google Scholar]
- Odebode, T.; Ologe, F. Facial nerve palsy after head injury: Case incidence, causes, clinical profile and outcome. J. Trauma 2006, 61, 388–391. [Google Scholar] [CrossRef]
- Peitersen, E. Bell’s palsy: The spontaneous course of 2500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol. Suppl. 2002, 122, 4–30. [Google Scholar] [CrossRef]
- Rahman, I.; Sadiq, S.A. Ophthalmic management of facial nerve palsy: A review. Surv. Ophthalmol. 2007, 52, 121–144. [Google Scholar] [CrossRef] [PubMed]
- Saadi, R.; Shokri, T.; Schaefer, E.; Hollenbeak, C.; Lighthall, J.G. Depression Rates After Facial Paralysis. Ann. Plast. Surg. 2019, 83, 190–194. [Google Scholar] [CrossRef]
- Hohman, M.H.; Bhama, P.K.; Hadlock, T.A. Epidemiology of iatrogenic facial nerve injury: A decade of experience. Laryngoscope 2014, 124, 260–265. [Google Scholar] [CrossRef]
- de Almeida, J.R.; Guyatt, G.H.; Sud, S.; Dorion, J.; Hill, M.D.; Kolber, M.R.; Lea, J.; Reg, S.L.; Somogyi, B.K.; Westerberg, B.D.; et al. Management of Bell palsy: Clinical practice guideline. CMAJ 2014, 186, 917–922. [Google Scholar] [CrossRef]
- Iseli, T.A.; Harris, G.; Dean, N.R.; Iseli, C.E.; Rosenthal, E.L. Outcomes of static and dynamic facial nerve repair in head and neck cancer. Laryngoscope 2010, 120, 478–483. [Google Scholar] [CrossRef]
- Kosins, A.M.; Hurvitz, K.A.; Evans, G.R.; Wirth, G.A. Facial paralysis for the plastic surgeon. Can. J. Plast. Surg. 2007, 15, 77–82. [Google Scholar] [CrossRef]
- Mehta, R.P. Surgical treatment of facial paralysis. Clin. Exp. Otorhinolaryngol. 2009, 2, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Pavese, C.; Cecini, M.; Lozza, A.; Biglioli, F.; Lisi, C.; Bejor, M.; Dalla Toffola, E. Rehabilitation and functional recovery after masseteric-facial nerve anastomosis. Eur. J. Phys. Rehabil. Med. 2016, 52, 379–388. [Google Scholar] [PubMed]
- Volk, G.F.; Geitner, M.; Geissler, K.; Thielker, J.; Raslan, A.; Mothes, O.; Dobel, C.; Guntinas-Lichius, O. Functional Outcome and Quality of Life After Hypoglossal-Facial Jump Nerve Suture. Front. Surg. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Volk, G.F.; Pantel, M.; Guntinas-Lichius, O. Modern concepts in facial nerve reconstruction. Head Face Med. 2010, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Volk, G.F.; Thielker, J.; Moller, M.C.; Majcher, D.; Mastryukova, V.; Altmann, C.S.; Dobel, C.; Guntinas-Lichius, O. Tolerability of facial electrostimulation in healthy adults and patients with facial synkinesis. Eur. Arch. Otorhinolaryngol. 2020, 277, 1247–1253. [Google Scholar] [CrossRef]
- Heckmann, J.G.; Urban, P.P.; Pitz, S.; Guntinas-Lichius, O.; Gagyor, I. The Diagnosis and Treatment of Idiopathic Facial Paresis (Bell’s Palsy). Dtsch. Arztebl. Int. 2019, 116, 692–702. [Google Scholar] [CrossRef]
- Jacobson, S.; Guth, L. An Electrophysiological Study of the Early Stages of Peripheral Nerve Regeneration. Exp. Neurol. 1965, 11, 48–60. [Google Scholar] [CrossRef]
- Jenkins, D.W.; Carruthers, R.R.; Litofsky, A.; Collins, W.F. Electrophysiological Study of Regenerating Peripheral Nerve. Relationship of Size of Fibers and Rate of Growth. J. Neurosurg. 1963, 20, 344–347. [Google Scholar] [CrossRef]
- Jowett, N.; Kearney, R.E.; Knox, C.J.; Hadlock, T.A. Toward the Bionic Face: A Novel Neuroprosthetic Device Paradigm for Facial Reanimation Consisting of Neural Blockade and Functional Electrical Stimulation. Plast. Reconstr. Surg. 2019, 143, 62e–76e. [Google Scholar] [CrossRef]
- Puls, W.C.; Jarvis, J.C.; Ruck, A.; Lehmann, T.; Guntinas-Lichius, O.; Volk, G.F. Surface electrical stimulation for facial paralysis is not harmful. Muscle Nerve 2020, 61, 347–353. [Google Scholar] [CrossRef]
- Kern, H.; Hofer, C.; Loefler, S.; Zampieri, S.; Gargiulo, P.; Baba, A.; Marcante, A.; Piccione, F.; Pond, A.; Carraro, U. Atrophy, ultra-structural disorders, severe atrophy and degeneration of denervated human muscle in SCI and Aging. Implications for their recovery by Functional Electrical Stimulation, updated 2017. Neurol. Res. 2017, 39, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Hofer, C.; Mayr, W.; Stöhr, H.; Unger, E.; Kern, H. A stimulator for functional activation of denervated muscles. Artif. Organs 2002, 26, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Kern, H.; Carraro, U. Home-Based Functional Electrical Stimulation of Human Permanent Denervated Muscles: A Narrative Review on Diagnostics, Managements, Results and Byproducts Revisited 2020. Diagnostics 2020, 10, 529. [Google Scholar] [CrossRef] [PubMed]
- Edmunds, K.J.; Gislason, M.K.; Arnadottir, I.D.; Marcante, A.; Piccione, F.; Gargiulo, P. Quantitative Computed Tomography and Image Analysis for Advanced Muscle Assessment. Eur. J. Transl. Myol. 2016, 26, 6015. [Google Scholar] [CrossRef] [PubMed]
- Carraro, U.; Boncompagni, S.; Gobbo, V.; Rossini, K.; Zampieri, S.; Mosole, S.; Ravara, B.; Nori, A.; Stramare, R.; Ambrosio, F.; et al. Persistent Muscle Fiber Regeneration in Long Term Denervation. Past, Present, Future. Eur. J. Transl. Myol. 2015, 25, 4832. [Google Scholar] [CrossRef] [PubMed]
- Kern, H.; Carraro, U.; Adami, N.; Biral, D.; Hofer, C.; Forstner, C.; Modlin, M.; Vogelauer, M.; Pond, A.; Boncompagni, S.; et al. Home-based functional electrical stimulation rescues permanently denervated muscles in paraplegic patients with complete lower motor neuron lesion. Neurorehabil. Neural Repair 2010, 24, 709–721. [Google Scholar] [CrossRef]
- Geddes, L.A.; Bourland, J.D. The strength-duration curve. IEEE Trans. Biomed. Eng. 1985, 32, 458–459. [Google Scholar] [CrossRef]
- Carlson, B.M. The Biology of Long-Term Denervated Skeletal Muscle. Eur. J. Transl. Myol. 2014, 24, 3293. [Google Scholar] [CrossRef]
- Cummings, J.P. Conservative management of peripheral nerve injuries utilizing selective electrical stimulation of denervated muscle with exponentially progressive—current forms. J. Orthop. Sports Phys. Ther. 1985, 7, 11–15. [Google Scholar] [CrossRef]
- Woodcock, A.H.; Taylor, P.N.; Ewins, D.J. Long pulse biphasic electrical stimulation of denervated muscle. Artif. Organs 1999, 23, 457–459. [Google Scholar] [CrossRef]
- Thomas, D.S. Muscle Preservation in Denervation Injury Using Continuous Implantable Electrical Stimulation. Master’s Thesis, McGill University, Montreal, QC, Canada, 1992. [Google Scholar]
- Ravara, B.; Hofer, C.; Kern, H.; Guidolin, D.; Porzionato, A.; De Caro, R.; Albertin, G. Dermal papillae flattening of thigh skin in Conus Cauda Syndrome. Eur. J. Transl. Myol. 2018, 28, 7914. [Google Scholar] [CrossRef] [PubMed]
- Albertin, G.; Kern, H.; Hofer, C.; Guidolin, D.; Porzionato, A.; Rambaldo, A.; De Caro, R.; Piccione, F.; Marcante, A.; Zampieri, S. Two years of Functional Electrical Stimulation by large surface electrodes for denervated muscles improve skin epidermis in SCI. Eur. J. Transl. Myol. 2018, 28, 7373. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject’s Code | Gender | Age | FP Duration | FP Side | FP Origin | FP Surgery | FP Surgery Time | SR-nEMG Time |
|---|---|---|---|---|---|---|---|---|
| DFP0101001 | F | 37 | 15 d | R | FP after resection of a intraparotideal facial nerve schwannoma treated with direct nerve suture | FNSAMG | 2 w before study start | 6m |
| DFP0101002 | F | 29 | 28 d | R | Postoperative FP after resection of a vestibular schwannoma | HFJA | 8 m after study start | 12 m |
| DFP0101003 | F | 37 | 16 y 2 m | R | Postoperative FP after resection of multiple meningiomas of the temporal bone | None | N/A | N/A |
| DFP0101004 | M | 59 | 5 y 11 m | L | Intramastoidal facial nerve schwannoma, schwannoma resection and nerve suture with interposition | HFJA | 2 w before study start | 8 m (single fiber activity) |
| DFP0101005 | F | 53 | 3 m 24 d | L | Postoperative FP after resection of a vestibular schwannoma | None | N/A | 12 m |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arnold, D.; Thielker, J.; Klingner, C.M.; Puls, W.C.; Misikire, W.; Guntinas-Lichius, O.; Volk, G.F. Selective Surface Electrostimulation of the Denervated Zygomaticus Muscle. Diagnostics 2021, 11, 188. https://doi.org/10.3390/diagnostics11020188
Arnold D, Thielker J, Klingner CM, Puls WC, Misikire W, Guntinas-Lichius O, Volk GF. Selective Surface Electrostimulation of the Denervated Zygomaticus Muscle. Diagnostics. 2021; 11(2):188. https://doi.org/10.3390/diagnostics11020188
Chicago/Turabian StyleArnold, Dirk, Jovanna Thielker, Carsten M. Klingner, Wiebke Caren Puls, Wengelawit Misikire, Orlando Guntinas-Lichius, and Gerd Fabian Volk. 2021. "Selective Surface Electrostimulation of the Denervated Zygomaticus Muscle" Diagnostics 11, no. 2: 188. https://doi.org/10.3390/diagnostics11020188
APA StyleArnold, D., Thielker, J., Klingner, C. M., Puls, W. C., Misikire, W., Guntinas-Lichius, O., & Volk, G. F. (2021). Selective Surface Electrostimulation of the Denervated Zygomaticus Muscle. Diagnostics, 11(2), 188. https://doi.org/10.3390/diagnostics11020188