
Classification of Brain MRI Tumor Images Based on Deep Learning PGGAN Augmentation


Abstract
:1. Introduction
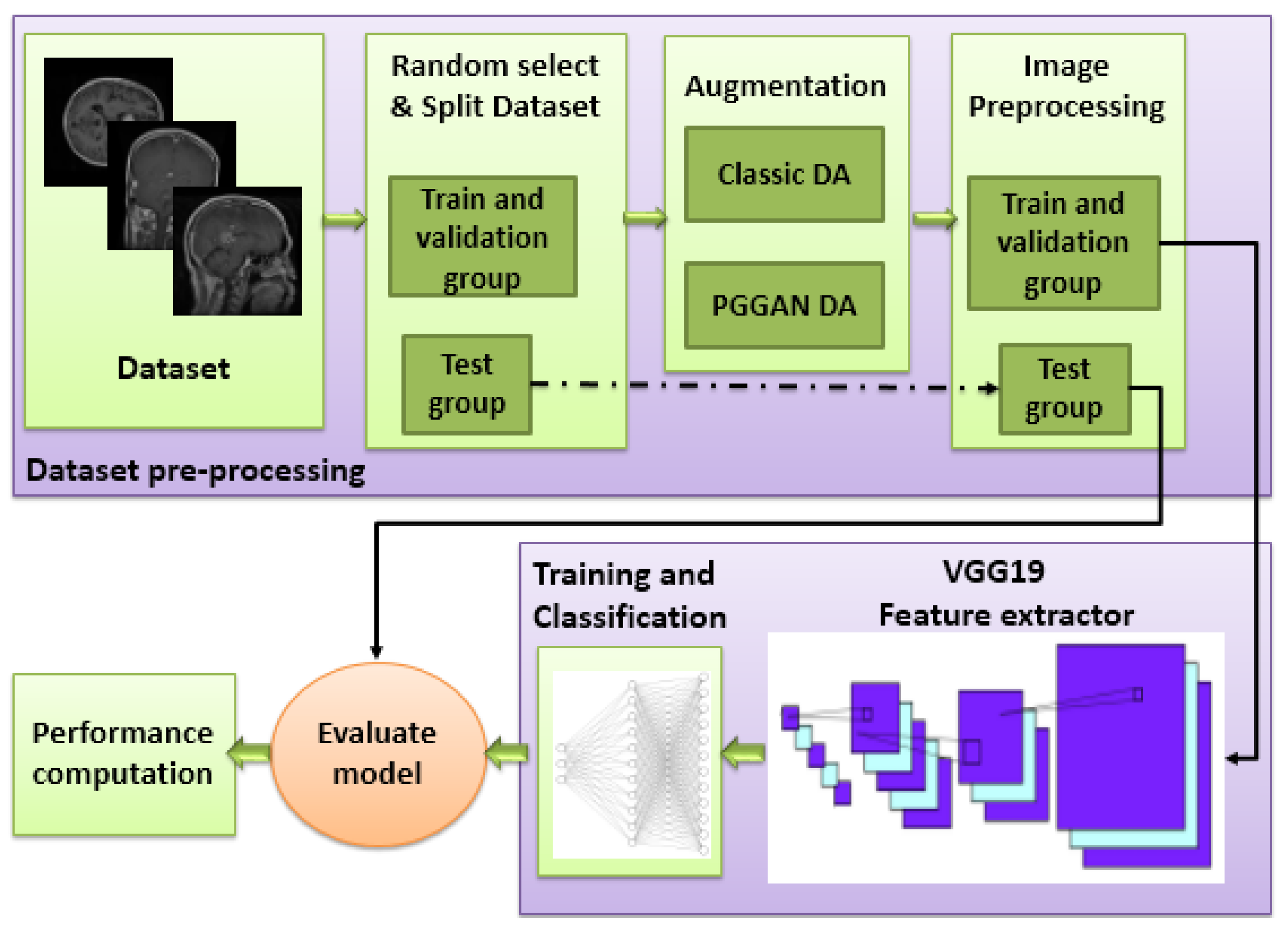
2. Materials and Methods
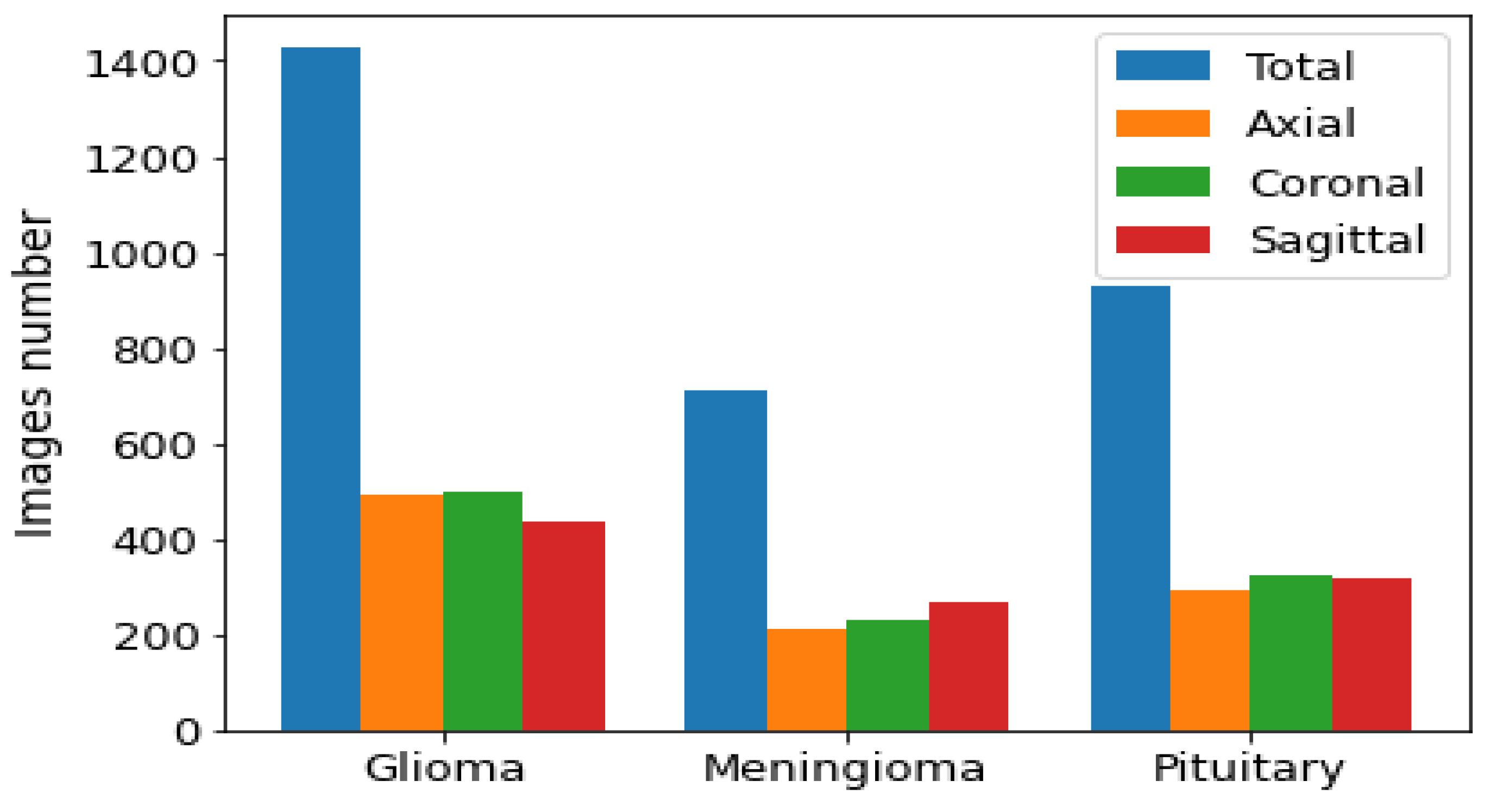
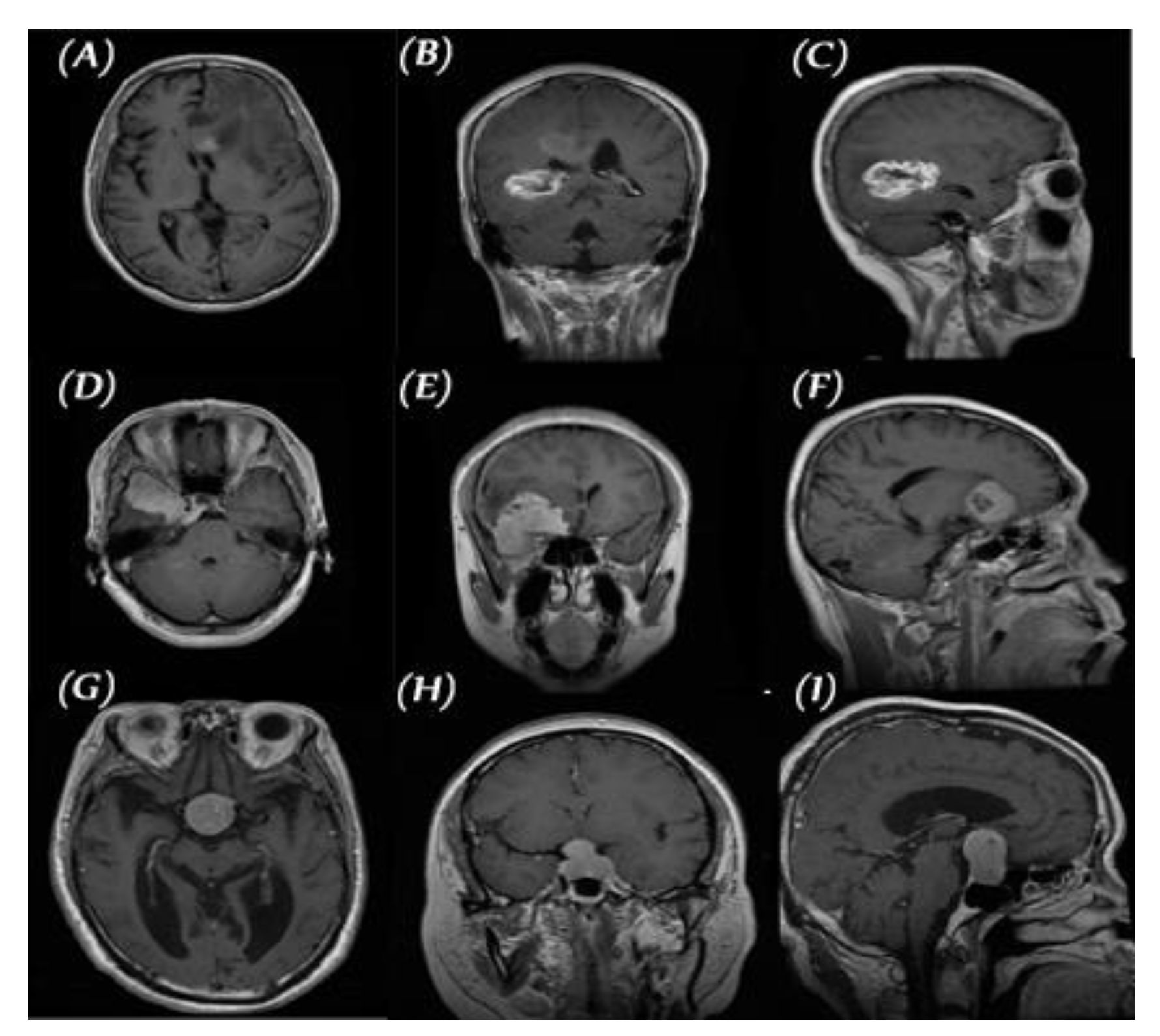
2.1. Data set for the Study
2.2. Pre-Processing and Image Augmentation
2.2.1. Classic Data Augmentation
- Rotation: Rotation of image without cropping because a cropped image may not contain the whole tumor. Images were rotated at 90, 180, and 270 degrees;
- Mirroring: Images are right/left mirrored;
- Flipping: Images are up–down flipped.
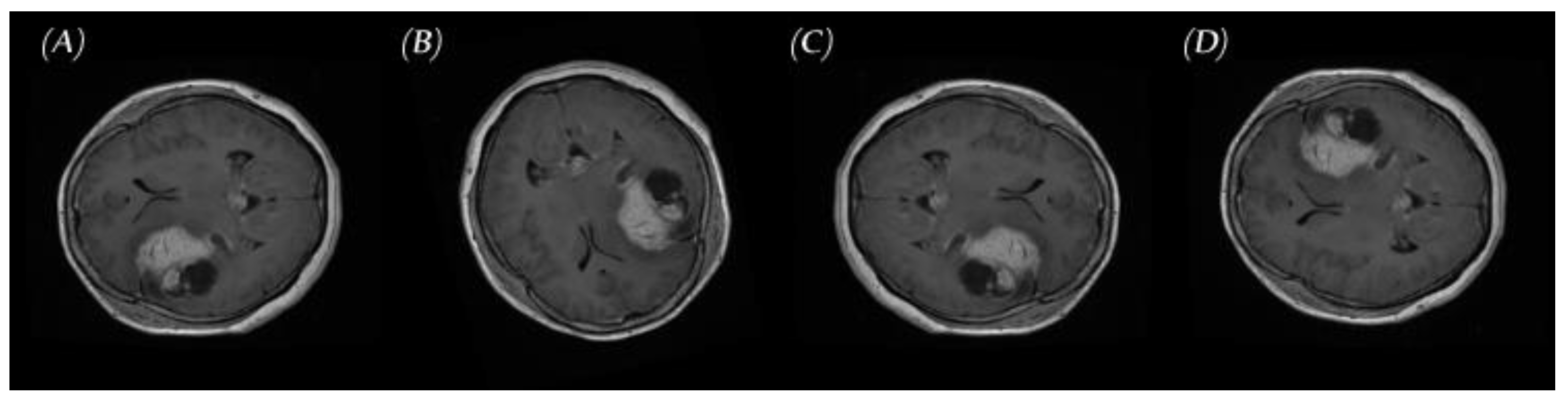
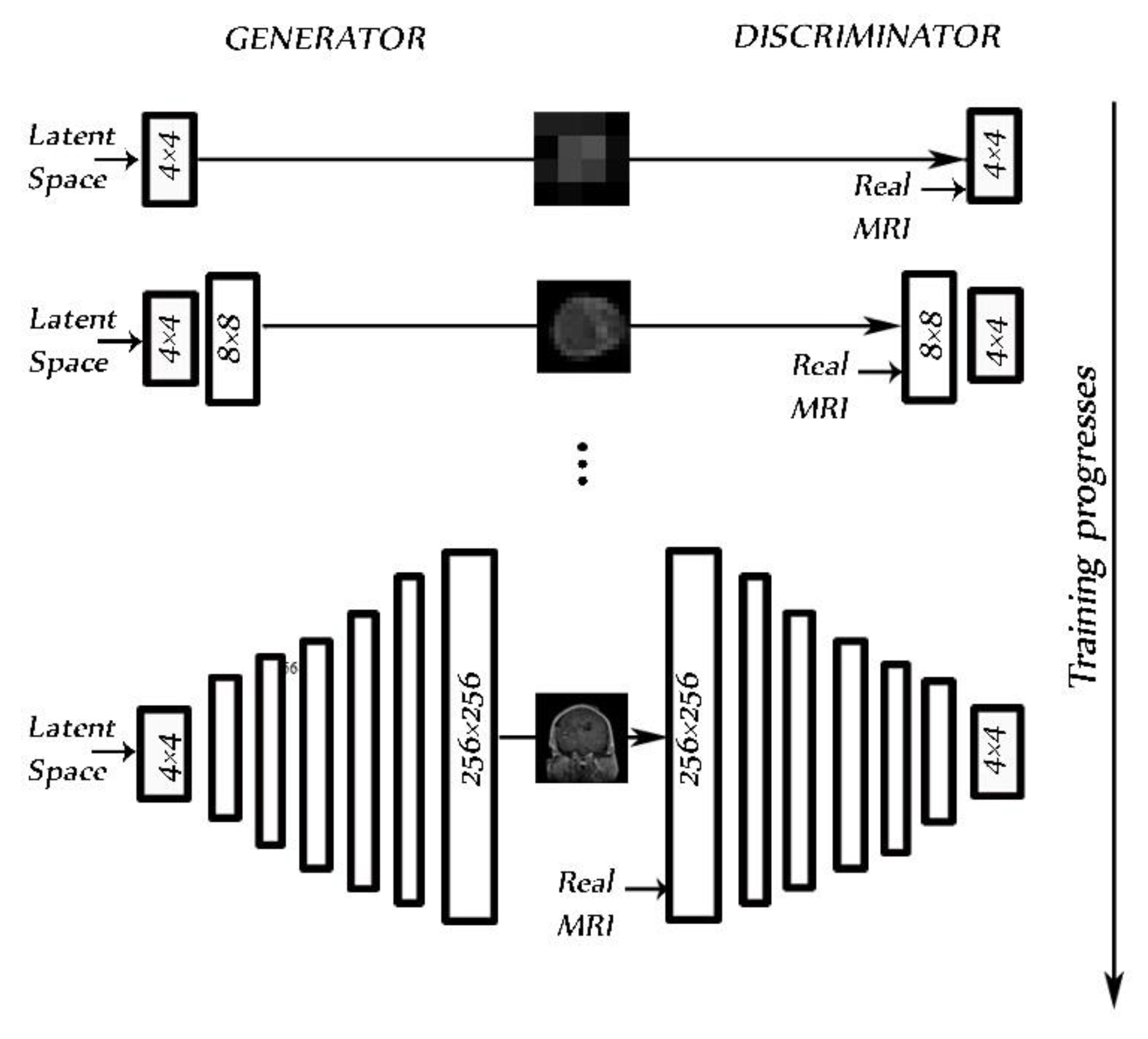
2.2.2. PGGAN-Based Data Augmentation
2.3. Proposed Deep Learning Models
- Classic DA;
- Classic DA + PGGAN-based DA.
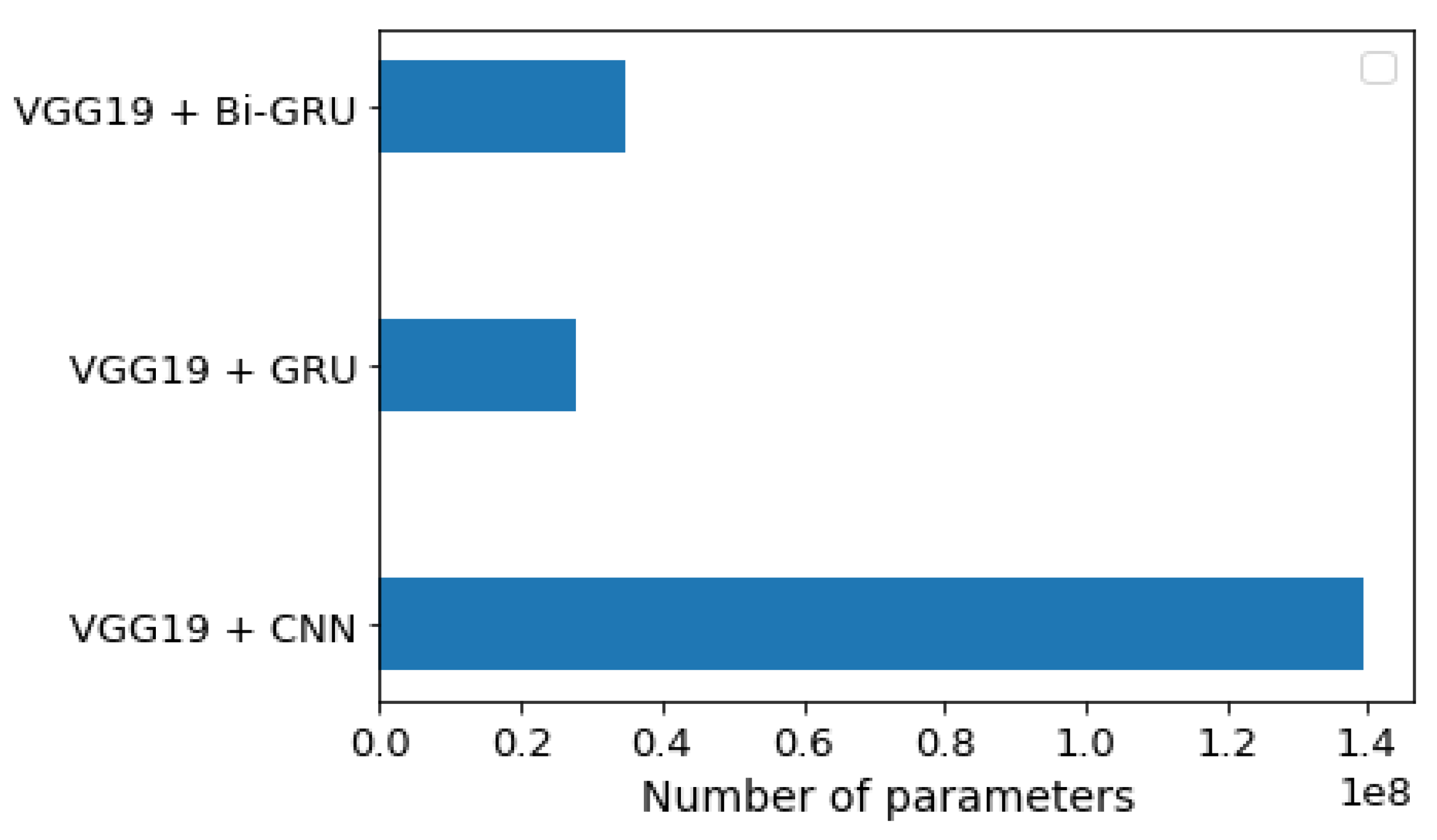
2.3.1. VGG19 and CNN Deep Learning Model
2.3.2. VGG19 and GRU Deep Learning Model
2.3.3. VGG19 and GRU Bidirectional Deep Learning Model
3. Results
3.1. Performance Metrics
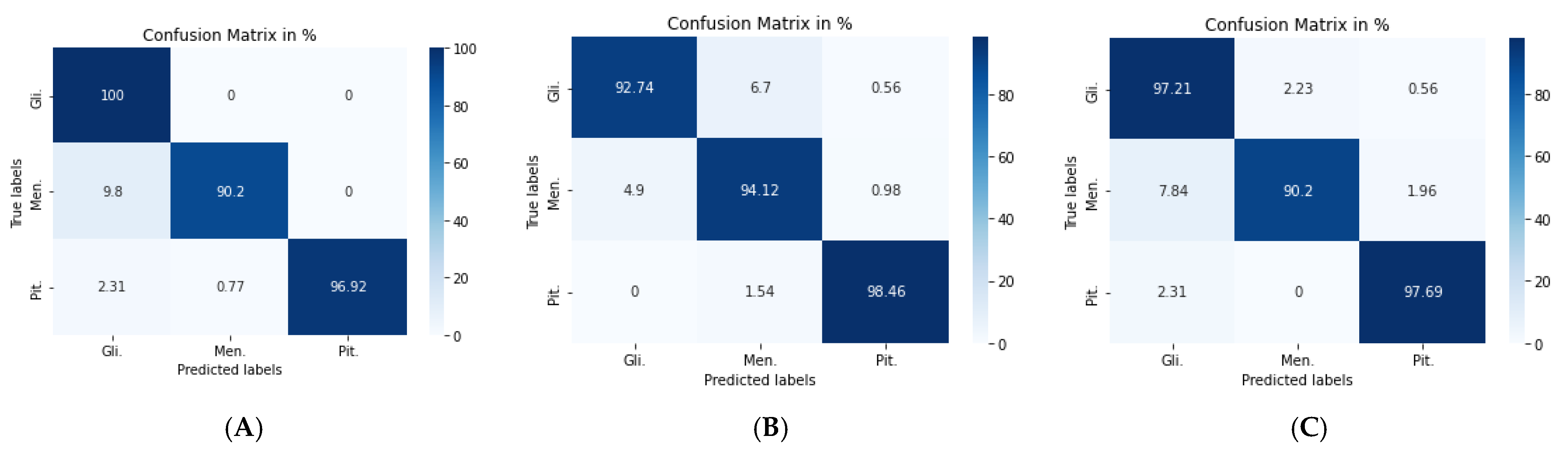
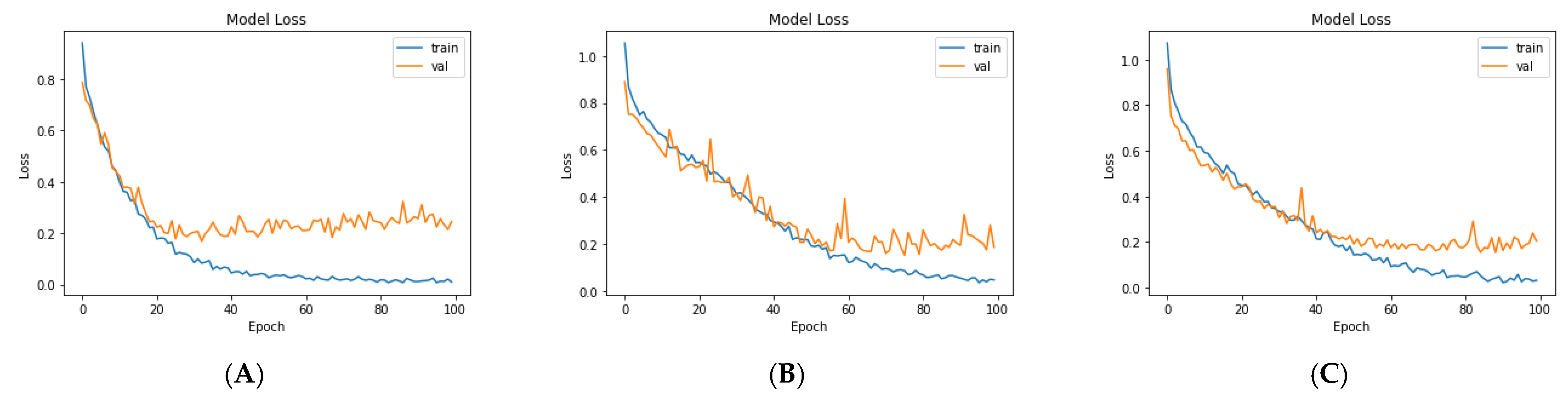
3.2. Scenario I: Deep Learning Models with Classic Augmentation
3.3. Scenario II: Deep Learning Models with PGGAN-Based DA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, D.; Rice, C.M.; Wang, X. Cancer bioinformatics: A new approach to systems clinical medicine. BMC Bioinform. 2012, 13, S7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Dabas, C.; Godara, S. Classification of brain MRI tumor images: A hybrid approach. Procedia Comput. Sci. 2017, 122, 510–517. [Google Scholar] [CrossRef]
- Fathallah-Shaykh, H.M.; DeAtkine, A.; Coffee, E.; Khayat, E.; Bag, A.K.; Han, X.; Warren, P.P.; Bredel, M.; Fiveash, J.; Markert, J. Diagnosing growth in low-grade gliomas with and without longitudinal volume measurements: A retrospective observational study. PLoS Med. 2019, 16, e1002810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghassemi, N.; Shoeibi, A.; Rouhani, M. Deep neural network with generative adversarial networks pre-training for brain tumor classification based on MR images. Biomed. Signal Process. Control 2020, 57, 101678. [Google Scholar] [CrossRef]
- Mohan, G.; Subashini, M.M. MRI based medical image analysis: Survey on brain tumor grade classification. Biomed. Signal Process. Control 2018, 39, 139–161. [Google Scholar] [CrossRef]
- Akkus, Z.; Galimzianova, A.; Hoogi, A.; Rubin, D.L.; Erickson, B.J. Deep learning for brain MRI segmentation: State of the art and future directions. J. Digit. Imaging 2017, 30, 449–459. [Google Scholar] [CrossRef] [Green Version]
- Lundervold, A.S.; Lundervold, A. An overview of deep learning in medical imaging focusing on MRI. Z. Med. Phys. 2019, 29, 102–127. [Google Scholar] [CrossRef]
- Chuquicusma, M.J.M.; Hussein, S.; Burt, J.; Bagci, U. How to fool radiologists with generative adversarial networks? A visual turing test for lung cancer diagnosis. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 240–244. [Google Scholar]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousefi, M.; Krzyżak, A.; Suen, C.Y. Mass detection in digital breast tomosynthesis data using convolutional neural networks and multiple instance learning. Comput. Biol. Med. 2018, 96, 283–293. [Google Scholar] [CrossRef]
- Gu, Y.; Lu, X.; Yang, L.; Zhang, B.; Yu, D.; Zhao, Y.; Gao, L.; Wu, L.; Zhou, T. Automatic lung nodule detection using a 3D deep convolutional neural network combined with a multi-scale prediction strategy in chest CTs. Comput. Biol. Med. 2018, 103, 220–231. [Google Scholar] [CrossRef]
- Elshennawy, N.M.; Ibrahim, D.M. Deep-Pneumonia Framework Using Deep Learning Models Based on Chest X-Ray Images. Diagnostics 2020, 10, 649. [Google Scholar] [CrossRef] [PubMed]
- Pacal, I.; Karaboga, D.; Basturk, A.; Akay, B.; Nalbantoglu, U. A comprehensive review of deep learning in colon cancer. Comput. Biol. Med. 2020, 126, 104003. [Google Scholar] [CrossRef]
- Yao, Z.; Li, J.; Guan, Z.; Ye, Y.; Chen, Y. Liver disease screening based on densely connected deep neural networks. Neural Netw. 2020, 123, 299–304. [Google Scholar] [CrossRef]
- Zuo, H.; Fan, H.; Blasch, E.; Ling, H. Combining convolutional and recurrent neural networks for human skin detection. IEEE Signal Process. Lett. 2017, 24, 289–293. [Google Scholar] [CrossRef]
- Charron, O.; Lallement, A.; Jarnet, D.; Noblet, V.; Clavier, J.-B.; Meyer, P. Automatic detection and segmentation of brain metastases on multimodal MR images with a deep convolutional neural network. Comput. Biol. Med. 2018, 95, 43–54. [Google Scholar] [CrossRef]
- Pereira, R.M.; Bertolini, D.; Teixeira, L.O.; Silla, C.N., Jr.; Costa, Y.M.G. COVID-19 identification in chest X-ray images on flat and hierarchical classification scenarios. Comput. Methods Programs Biomed. 2020, 194, 105532. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Serrano, J.A.; Gordo, A.; Perronnin, F. Label embedding: A frugal baseline for text recognition. Int. J. Comput. Vis. 2015, 113, 193–207. [Google Scholar] [CrossRef]
- Liu, M.; Cheng, D.; Yan, W.; Initiative, A.D.N. Classification of Alzheimer’s disease by combination of convolutional and recurrent neural networks using FDG-PET images. Front. Neuroinform. 2018, 12, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, G.; Hong, H.; Xie, W.; Zheng, L. Combining convolutional neural network with recursive neural network for blood cell image classification. IEEE Access 2018, 6, 36188–36197. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Simard, P.Y.; Steinkraus, D.; Platt, J.C. Best practices for convolutional neural networks applied to visual document analysis. In Proceedings of the International Conference on Document Analysis and Recognition (ICDAR), Edinburgh, UK, 3–6 August 2003; Volume 3. [Google Scholar]
- Sultan, H.H.; Salem, N.M.; Al-Atabany, W. Multi-classification of brain tumor images using deep neural network. IEEE Access 2019, 7, 69215–69225. [Google Scholar] [CrossRef]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. Adv. Neural Inf. Process. Syst. 2014, 27, 2672–2680. [Google Scholar]
- Radford, A.; Metz, L.; Chintala, S. Unsupervised representation learning with deep convolutional generative adversarial networks. arXiv 2015, arXiv:1511.06434. [Google Scholar]
- Salehinejad, H.; Colak, E.; Dowdell, T.; Barfett, J.; Valaee, S. Synthesizing chest X-ray pathology for training deep convolutional neural networks. IEEE Trans. Med. Imaging 2018, 38, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Liu, Z.; Xu, M.; Wang, S.; Zeng, T.; Gao, X.; Li, L. Generative adversarial network-based super-resolution of diffusion-weighted imaging: Application to tumour radiomics in breast cancer. NMR Biomed. 2020, 33, e4345. [Google Scholar] [CrossRef]
- Mukhtar, M.; Bilal, M.; Rahdar, A.; Barani, M.; Arshad, R.; Behl, T.; Brisc, C.; Banica, F.; Bungau, S. Nanomaterials for diagnosis and treatment of brain cancer: Recent updates. Chemosensors 2020, 8, 117. [Google Scholar] [CrossRef]
- Behl, T.; Sharma, A.; Sharma, L.; Sehgal, A.; Singh, S.; Sharma, N.; Zengin, G.; Bungau, S.; Toma, M.M.; Gitea, D. Current Perspective on the Natural Compounds and Drug Delivery Techniques in Glioblastoma Multiforme. Cancers 2021, 13, 2765. [Google Scholar] [CrossRef]
- Cheng, J.; Huang, W.; Cao, S.; Yang, R.; Yang, W.; Yun, Z.; Wang, Z.; Feng, Q. Enhanced performance of brain tumor classification via tumor region augmentation and partition. PLoS ONE 2015, 10, e0140381. [Google Scholar] [CrossRef]
- Paul, J.S.; Plassard, A.J.; Landman, B.A.; Fabbri, D. Deep learning for brain tumor classification. In Proceedings of the Medical Imaging 2017: Biomedical Applications in Molecular, Structural, and Functional Imaging; International Society for Optics and Photonics, Orlando, FL, USA, 12–14 February 2017; Volume 10137, p. 1013710. [Google Scholar]
- Pashaei, A.; Sajedi, H.; Jazayeri, N. Brain tumor classification via convolutional neural network and extreme learning machines. In Proceedings of the 2018 8th International conference on computer and knowledge engineering (ICCKE), Mashhad, Iran, 25–26 October 2018; pp. 314–319. [Google Scholar]
- Zhou, Y.; Li, Z.; Zhu, H.; Chen, C.; Gao, M.; Xu, K.; Xu, J. Holistic brain tumor screening and classification based on densenet and recurrent neural network. In Proceedings of the International MICCAI Brainlesion Workshop, Granada, Spain, 16 September 2018; pp. 208–217. [Google Scholar]
- Ismael, M.R.; Abdel-Qader, I. Brain tumor classification via statistical features and back-propagation neural network. In Proceedings of the 2018 IEEE international conference on electro/information technology (EIT), Rochester, NY, USA, 3–5 May 2018; pp. 252–257. [Google Scholar]
- Afshar, P.; Mohammadi, A.; Plataniotis, K.N. Brain tumor type classification via capsule networks. In Proceedings of the 2018 25th IEEE International Conference on Image Processing (ICIP), Athens, Greece, 7–10 October 2018; pp. 3129–3133. [Google Scholar]
- Afshar, P.; Plataniotis, K.N.; Mohammadi, A. Capsule networks for brain tumor classification based on MRI images and coarse tumor boundaries. In Proceedings of the ICASSP 2019–2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; pp. 1368–1372. [Google Scholar]
- Abiwinanda, N.; Hanif, M.; Hesaputra, S.T.; Handayani, A.; Mengko, T.R. Brain tumor classification using convolutional neural network. In Proceedings of the World congress on medical physics and biomedical engineering, Prague, Czech Republic, 3–8 June 2018; pp. 183–189. [Google Scholar]
- Anaraki, A.K.; Ayati, M.; Kazemi, F. Magnetic resonance imaging-based brain tumor grades classification and grading via convolutional neural networks and genetic algorithms. Biocybern. Biomed. Eng. 2019, 39, 63–74. [Google Scholar] [CrossRef]
- Deepak, S.; Ameer, P.M. Brain tumor classification using deep CNN features via transfer learning. Comput. Biol. Med. 2019, 111, 103345. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Patil, N.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2013–2017. Neuro Oncol. 2020, 22, iv1–iv96. [Google Scholar] [CrossRef]
- Castinetti, F.; Régis, J.; Dufour, H.; Brue, T. Role of stereotactic radiosurgery in the management of pituitary adenomas. Nat. Rev. Endocrinol. 2010, 6, 214–223. [Google Scholar] [CrossRef]
- Balasooriya, N.M.; Nawarathna, R.D. A sophisticated convolutional neural network model for brain tumor classification. In Proceedings of the 2017 IEEE International Conference on Industrial and Information Systems (ICIIS), Peradeniya, Sri Lanka, 15–16 December 2017; pp. 1–5. [Google Scholar]
- Karras, T.; Aila, T.; Laine, S.; Lehtinen, J. Progressive growing of gans for improved quality, stability, and variation. arXiv 2017, arXiv:1710.10196. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Gulrajani, I.; Ahmed, F.; Arjovsky, M.; Dumoulin, V.; Courville, A. Improved training of wasserstein gans. arXiv 2017, arXiv:1704.00028. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Heaton, J. Ian goodfellow, yoshua bengio, and aaron courville: Deep learning. Genet. Program. Evolvable Mach. 2018, 19, 305–307. [Google Scholar] [CrossRef] [Green Version]
- Dozat, T. Incorporating nesterov momentum into adam. In Proceedings of the ICLR 2016 Workshop, San Juan, Puerto Rico, 2–4 May 2016. [Google Scholar]
- Ruuska, S.; Hämäläinen, W.; Kajava, S.; Mughal, M.; Matilainen, P.; Mononen, J. Evaluation of the confusion matrix method in the validation of an automated system for measuring feeding behaviour of cattle. Behav. Process. 2018, 148, 56–62. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Accuracy % | No. of Images |
|---|---|---|
| [30] | 91.28 | 3064 |
| [31] | 91.43 | 989 * |
| [32] | 93.68 | 3064 |
| [33] | 92.13 | 989 * |
| [34] | 91.13 | 3064 |
| [35] | 86.56 | 3064 |
| [36] | 90.89 | 3064 |
| [37] | 84.19 | 2100 |
| [38] | 94.2 | 989 * |
| [23] | 96.13 | 3064 |
| [39] | 98 | 3064 |
| [4] | 95.6 | 3064 |
| VGG19 + CNN Model | Output Shapes |
|---|---|
| [Conv (3 × 3) − 64] × 2 | 224 × 224 × 64 |
| [Conv (3 × 3) − 128] × 2 | 112 × 112 × 128 |
| [Conv (3 × 3) − 256] × 4 | 56 × 56 × 256 |
| [Conv (3 × 3) − 512] × 4 | 28 × 28 × 512 |
| [Conv (3 × 3) − 512] × 4 | 14 × 14 × 512 |
| Max pool | 7 × 7 × 512 |
| Flatten | 25,088 |
| Dense (relu) | 4096 |
| Dropout (0.5) | 4096 |
| Dense (relu) | 4096 |
| Dropout (0.5) | 4096 |
| Dense (SoftMax) | 3 |
| VGG19 + GRU Model | Output Shapes |
|---|---|
| [Conv (3 × 3) − 64] × 2 | 224 × 224 × 64 |
| [Conv (3 × 3) − 128] × 2 | 112 × 112 × 128 |
| [Conv (3 × 3) − 256] × 4 | 56 × 56 × 256 |
| [Conv (3 × 3) − 512] × 4 | 28 × 28 × 512 |
| [Conv (3 × 3) − 512] × 4 | 14 × 14 × 512 |
| Max pool | 7 × 7 × 512 |
| Reshape | 7 × 7 × 512 |
| Time Distributed | 7 × 3584 |
| GRU (512) | 512 |
| Dense (relu) | 1024 |
| Dropout (0.5) | 1024 |
| Dense (relu) | 1024 |
| Dropout (0.5) | 1024 |
| Dense (SoftMax) | 3 |
| VGG19 + Bi-GRU Model | Output Shapes |
|---|---|
| [Conv (3 × 3) − 64] × 2 | 224 × 224 × 64 |
| [Conv (3 × 3) − 128] × 2 | 112 × 112 × 128 |
| [Conv (3 × 3) − 256] × 4 | 56 × 56 × 256 |
| [Conv (3 × 3) − 512] × 4 | 28 × 28 × 512 |
| [Conv (3 × 3) − 512] × 4 | 14 × 14 × 512 |
| Max pool | 7 × 7 × 512 |
| Reshape | 7 × 7 × 512 |
| Time Distributed | 7 × 3584 |
| Bidirectional | 1024 |
| Dense (relu) | 1024 |
| Dropout (0.5) | 1024 |
| Dense (relu) | 1024 |
| Dropout (0.5) | 1024 |
| Dense (SoftMax) | 3 |
| Models | Adam | Adamax | RMSprop | Nadam |
|---|---|---|---|---|
| VGG19 + CNN | 94.16 | 92.94 | 95.59 | 96.59 |
| VGG19 + GRU | 94.89 | 87.10 | 93.19 | 93.67 |
| VGG19 + BI-GRU | 95.38 | 89.05 | 95.62 | 92.94 |
| Model | Class | Accuracy | Precision | Sensitivity | F1-Score | Specificity | NPV | MCC |
|---|---|---|---|---|---|---|---|---|
| VGG19 + CNN | Gli. | 96.97 | 93.81 | 100 | 96.81 | 94.40 | 100 | 94.10 |
| Men. | 97.44 | 98.92 | 90.2 | 94.36 | 99.70 | 97.02 | 92.87 | |
| Pit. | 99.06 | 100 | 96.92 | 98.44 | 100 | 98.68 | 97.80 | |
| VGG19 + GRU | Gli. | 95.01 | 95.87 | 89.92 | 92.8 | 97.84 | 94.58 | 89.01 |
| Men. | 94.46 | 87.27 | 94.12 | 90.1 | 94.59 | 97.61 | 86.78 | |
| Pit. | 98.89 | 98.46 | 98.46 | 98.46 | 99.13 | 99.13 | 97.60 | |
| VGG19 + Bi-GRU | Gli. | 96.11 | 94.05 | 97.21 | 95.6 | 95.26 | 97.79 | 92.15 |
| Men. | 96.59 | 95.83 | 90.20 | 92.93 | 98.71 | 96.83 | 90.76 | |
| Pit. | 98.54 | 97.69 | 97.69 | 97.69 | 98.93 | 98.93 | 96.62 |
| Models | Adam | Adamax | RMSprop | Nadam |
|---|---|---|---|---|
| VGG19 + CNN | 98.54 | 97.57 | 97.57 | 96.59 |
| VGG19 + GRU | 95.62 | 92.21 | 95.13 | 96.59 |
| VGG19 + BI-GRU | 95.62 | 91.97 | 96.84 | 96.35 |
| Model | Class | Accuracy | Precision | Sensitivity | F1-Score | Specificity | NPV | MCC |
|---|---|---|---|---|---|---|---|---|
| VGG19 + CNN | Gli. | 98.54 | 98.87 | 97.77 | 98.31 | 99.14 | 98.29 | 97.03 |
| Men. | 98.54 | 96.15 | 98.04 | 97.09 | 98.71 | 99.35 | 96.12 | |
| Pit. | 100 | 100 | 100 | 100 | 100 | 100 | 100 | |
| VGG19 + GRU | Gli. | 97.08 | 95.63 | 97.77 | 96.69 | 96.55 | 98.25 | 94.1 |
| Men. | 97.23 | 95.05 | 94.12 | 94.58 | 98.38 | 98.06 | 92.81 | |
| Pit. | 98.78 | 99.21 | 96.92 | 98.05 | 99.64 | 98.59 | 97.18 | |
| VGG19 + Bi-GRU | Gli. | 96.84 | 94.62 | 98.32 | 96.44 | 95.69 | 98.67 | 93.65 |
| Men. | 97.08 | 96.88 | 91.18 | 93.94 | 99.03 | 97.14 | 92.09 | |
| Pit. | 99.76 | 100 | 99.23 | 99.61 | 100 | 99.64 | 99.44 |
| Ref. | Augmentation Operation | Data Set Size after Augmentation | Data Set Division | ACC% |
|---|---|---|---|---|
| [31] | Rotation random angle between (0 and 360 angle). Shifted randomly by −4 to 4 pixels left or right and up or down. Mirror across its y-axis. | Not mentioned | Use images for 191 patients and divided them according to patients as follows: training: 149 patients, validation: 21 patients, and testing: 21 patients. | 91.43 |
| [38] | Rotation 10, 20, or 30 clockwise or counterclockwise. Mirroring, and translating 15 pixels to right or left. Scaling to 0.75 of the original. | Augmentation is done after the train and test images are randomly selected. For each tumor class take: 1521 as training images, and 115 as testing images | Divide the data set images into: training group, and testing group. | 94.2 |
| [23] | Rotation image with angle 45. Mirroring right/left. Flipping up–down. Adding salt noise. | Images are shuffled, splitting, and finally, the author applies augmentation. The authors increased the original number to 15,320 images. | Divide the data set images into training group: 68%, validation group: 16%, and testing group: 16%. | 96.13 |
| [4] | Rotation random angle between (0 and 359 angle). Mirror 25% on each axis. | Not mentioned | Not mentioned | 95.6 |
| Our framework (VGG19 + CNN and classic DA) | Rotation 90, 180, 270 angles. Mirroring right/left. Flipping up–down. | Images are randomly selected, then split, and finally, we augment the only training and validation groups. The original images increased to 19,215 images for the training group, and 4536 for the validation group. | Divide the data set images into: training group: 70%, validation group: 15%, and testing group: 15%. | 96.59 |
| Our framework (VGG19 + CNN and PGGAN DA) | Rotation 90, 180, 270 angles. Mirroring right/left. Flipping up–down. Add generated images from PGGAN models (8100 images). | We increased the original images to 27,315 images for training, and 4536 images for validation. | Divide data set into: training: 70% + PGGAN-generated images, validation: 15%, and testing: 15%. | 98.54 |
| Method | PPV | Sensitivity | SPC | ACC% | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Gli. | Men. | Pit. | Gli. | Men. | Pit. | Gli. | Men. | Pit. | ||
| [30] | - | - | - | 96.4 | 86.0 | 87.3 | 96.3 | 95.5 | 95.3 | 91.28 |
| [32] | 91.0 | 94.5 | 98.3 | 97.5 | 76.8 | 100 | - | - | - | 93.68 |
| [34] | - | - | - | 95.1 | 86.97 | 91.24 | 96.29 | 96.0 | 95.66 | 91.13 |
| [38] | 91.9 | 95.3 | 95.7 | 98.3 | 87.8 | 96.5 | 95.7 | 97.8 | 97.8 | 94.2 |
| [23] | 97.2 | 95.8 | 95.2 | 94.4 | 95.5 | 93.4 | 95.1 | 98.7 | 97.0 | 96.13 |
| [39] | 99.2 | 94.7 | 98.0 | 97.9 | 96.0 | 98.9 | 99.4 | 98.4 | 99.1 | 98.0 |
| [4] | 95.89 | 92.43 | 95.29 | 96.83 | 89.98 | 97.93 | 96.38 | 97.79 | 97.54 | 95.6 |
| Our framework | 98.87 | 96.15 | 100 | 97.77 | 98.04 | 100 | 99.14 | 98.71 | 100 | 98.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gab Allah, A.M.; Sarhan, A.M.; Elshennawy, N.M. Classification of Brain MRI Tumor Images Based on Deep Learning PGGAN Augmentation. Diagnostics 2021, 11, 2343. https://doi.org/10.3390/diagnostics11122343
Gab Allah AM, Sarhan AM, Elshennawy NM. Classification of Brain MRI Tumor Images Based on Deep Learning PGGAN Augmentation. Diagnostics. 2021; 11(12):2343. https://doi.org/10.3390/diagnostics11122343
Chicago/Turabian StyleGab Allah, Ahmed M., Amany M. Sarhan, and Nada M. Elshennawy. 2021. "Classification of Brain MRI Tumor Images Based on Deep Learning PGGAN Augmentation" Diagnostics 11, no. 12: 2343. https://doi.org/10.3390/diagnostics11122343
APA StyleGab Allah, A. M., Sarhan, A. M., & Elshennawy, N. M. (2021). Classification of Brain MRI Tumor Images Based on Deep Learning PGGAN Augmentation. Diagnostics, 11(12), 2343. https://doi.org/10.3390/diagnostics11122343