
Validation of a Monte Carlo Modelling Based Dosimetry of Extraoral Photobiomodulation

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Volunteers
2.2. Volunteer MRI and Image Analysis
2.3. LED Light Source
2.4. Transmission Measurement Device
2.5. Transmission Measurements and Analysis
2.6. Monte Carlo Simulations
2.7. Optical Properties
3. Results
3.1. MRI and Image Analysis
3.2. Transmission Measurements and Analysis
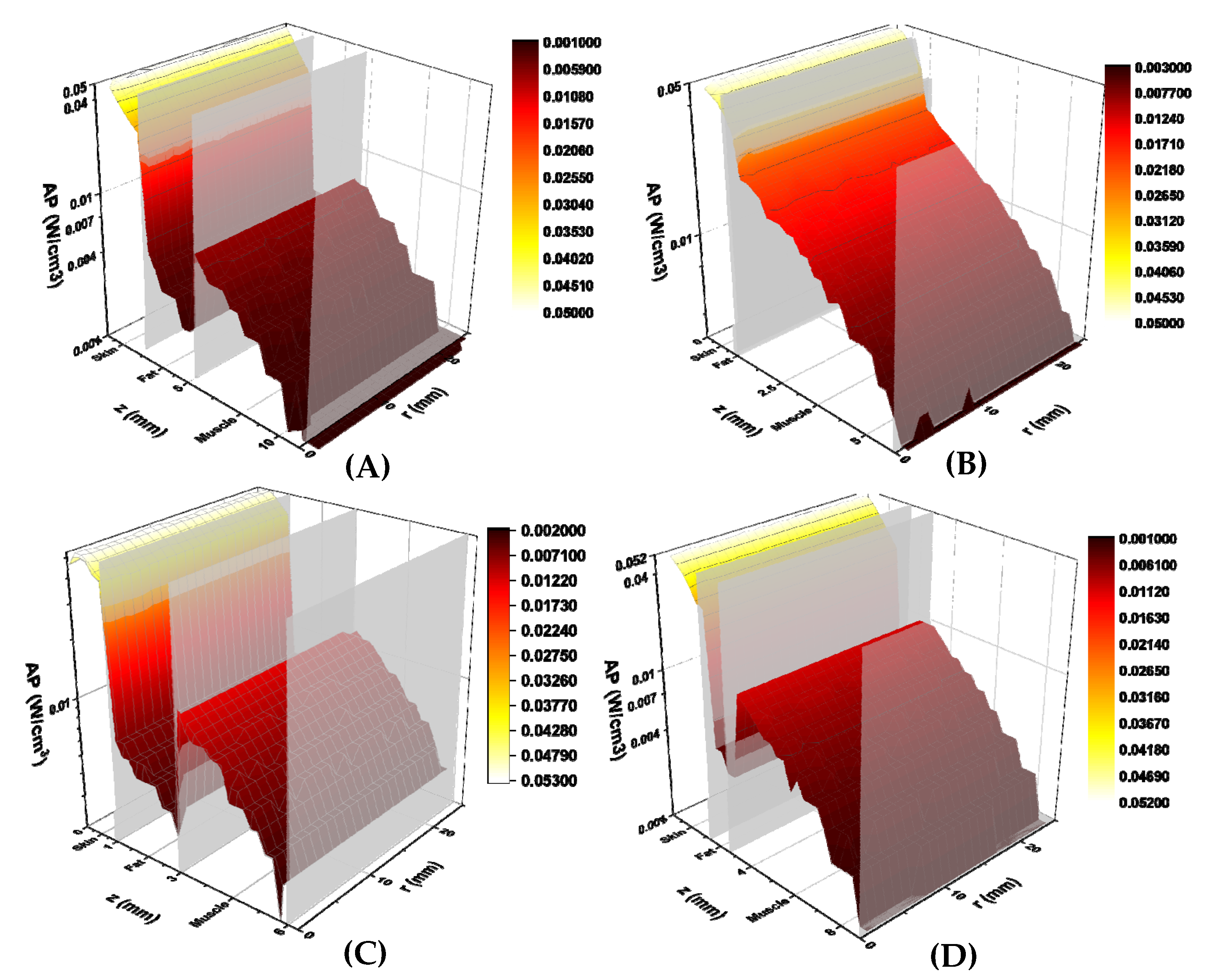
3.3. Monte Carlo Simulations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elting, L.S.; Cooksley, C.; Chambers, M.; Cantor, S.B.; Manzullo, E.; Rubenstein, E.B. The burdens of cancer therapy: Clinical and economic outcomes of chemotherapy-induced mucositis. Cancer 2003, 98, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, E.B.; Peterson, D.E.; Schubert, M.; Keefe, D.; McGuire, D.; Epstein, J.; Elting, L.S.; Fox, P.C.; Cooksley, C.; Sonis, S.T. Clinical practice guidelines for the prevention and treatment of cancer therapy–induced oral and gastrointestinal mucositis. Cancer 2004, 100, 2026–2046. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, H.M.; Bruce, A.J.; Wolf, R.C.; Litzow, M.R.; Hogan, W.J.; Patnaik, M.S.; Kremers, W.K.; Phillips, G.L.; Hashmi, S.K. The Incidence and Severity of Oral Mucositis among Allogeneic Hematopoietic Stem Cell Transplantation Patients: A Systematic Review. Biol. Blood Marrow Transplant. 2016, 22, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Sonis, S.T. The pathobiology of mucositis. Nat. Rev. Cancer 2004, 4, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, S.; Zamperlini-Netto, G.; Beyene, J.; Treister, N.S.; Sung, L. Effect of prophylactic low level laser therapy on oral mucositis: A systematic review and meta-analysis. PLoS ONE 2014, 9, e107418. [Google Scholar]
- Palma, L.F.; Gonnelli, F.A.S.; Marcucci, M.; Dias, R.S.; Giordani, A.J.; Segreto, R.A.; Segreto, H.R.C. Impact of low-level laser therapy on hyposalivation, salivary pH, and quality of life in head and neck cancer patients post radiotherapy. Lasers Med. Sci. 2017, 32, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Paglioni, M.D.P.; Alves, C.G.B.; Fontes, E.K.; Lopes, M.A.; Ribeiro, A.C.P.; Brandão, T.B.; Migliorati, C.A.; Santos-Silva, A.R. Is photobiomodulation therapy effective in reducing pain caused by toxicities related to head and neck cancer treatment? A systematic review. Support. Care Cancer 2019, 27, 4043–4054. [Google Scholar] [CrossRef] [PubMed]
- Zadik, Y.; Arany, P.R.; Fregnani, E.R.; Bossi, P.; Antunes, H.S.; Bensadoun, R.-J.; Gueiros, L.A.; Majorana, A.; Nair, R.G.; Elad, V.R.; et al. Systematic review of photobiomodulation for the management of oral mucositis in cancer patients and clinical practice guidelines. Support. Care Cancer 2019, 27, 3969–3983. [Google Scholar] [CrossRef]
- Treister, N.S.; London, W.B.; Guo, D.; Malsch, M.; Verrill, K.; Brewer, J.; Margossian, S.; Duncan, C. A feasibility study evaluating extraoral photobiomodulation therapy for prevention of mucositis in pediatric hematopoietic cell transplantation. Photomed. Laser Surg. 2016, 34, 178–184. [Google Scholar] [CrossRef]
- Adnan, A.; Yaroslavsky, A.N.; Carroll, J.D.; Selting, W.; Juliano, A.F.; London, W.B.; Sonis, S.T.; Duncan, C.N.; Treister, N.S. The Path to an Evidence-Based Treatment Protocol for Extraoral Photobiomodulation Therapy for the Prevention of Oral Mucositis. Front. Oral Health 2021, 2, 48. [Google Scholar] [CrossRef]
- Yaroslavsky, A. Spectroscopic Investigations of Biological Tissues and Fluids. Ph.D. Thesis, Saratov State University, Saratov Oblast, Russia, 1999. [Google Scholar]
- Keijzer, M.; Jacques, S.L.; Prahl, S.A.; Welch, A.J. Light distributions in artery tissue: Monte Carlo simulations for finite-diameter laser beams. Lasers Surg. Med. 1989, 9, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Tseng, S.H.; Bargo, P.; Durkin, A.; Kollias, N. Chromophore concentrations, absorption and scattering properties of human skin in-vivo. Opt. Exp. 2009, 17, 14599–14617. [Google Scholar] [CrossRef] [PubMed]
- Simpson, C.R.; Kohl, M.; Essenpries, M.; Cope, M. Near-infrared optical properties of ex vivo human skin and subcutaneous tissues measured using the Monte Carlo inversion technique. Phys. Med. Biol. 1998, 43, 2465. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, B.D.; Margolis, D.M.; Salzman, D.E.; Eastwood, D.; Tarima, S.; Williams, L.D.; Sande, J.E.; Vaughan, W.P.; Whelan, H.T. Amelioration of oral mucositis pain by NASA near-infrared light-emitting diodes in bone marrow transplant patients. Support. Care Cancer 2012, 20, 1405–1415. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chung, H.; Dai, T.; Sharma, S.K.; Huang, Y.Y.; Carroll, J.D.; Hamblin, M.R. The nuts and bolts of low-level laser (light) therapy. Ann. Biomed. Eng. 2012, 40, 516–533. [Google Scholar] [CrossRef] [PubMed]
- Chopra, K.; Calva, D.; Sosin, M.; Tadisina, K.K.; Banda, A.; De La Cruz, C.; Chaudhry, M.R.; Legesse, T.; Brachenberg, C.B.; Manson, P.N.; et al. A comprehensive examination of topographic thickness of skin in the human face. Aesthetic Surg. J. 2015, 35, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Hwang, K.; Kim, H.; Kim, D.J. Thickness of skin and subcutaneous tissue of the free flap donor sites: A histologic study. Microsurgery 2016, 36, 54–58. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structure | Absorption Coefficient, /mm | Reduced Scattering Coefficient, /mm |
|---|---|---|
| Skin | 0.056 | 1.65 |
| Fat | 0.009 | 1.1 |
| Muscle | 0.035 | 0.65 |
| Subject | Gender | Age | Skin Type | Anatomy of Right Cheek with Open Mouth Obtained from MRI | Measured Transmission, mW/cm2 | Simulated Transmission, mW/cm2 | % Difference | ||
|---|---|---|---|---|---|---|---|---|---|
| Skin, mm | Fat, mm | Muscle, mm | |||||||
| 1 | M | 25 | IV | 2 | 3 | 7 | 0.47 | 0.41 | 12 |
| 2 | F | 57 | VI | 1 | 0 | 5 | 2.14 | 2.12 | 1 |
| 3 | F | 25 | II | 1 | 2 | 3 | 2.38 | 2.07 | 11 |
| 4 | M | 43 | I | 2 | 1 | 6 | 0.83 | 0.82 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yaroslavsky, A.N.; Juliano, A.F.; Adnan, A.; Selting, W.J.; Iorizzo, T.W.; Carroll, J.D.; Sonis, S.T.; Duncan, C.N.; London, W.B.; Treister, N.S. Validation of a Monte Carlo Modelling Based Dosimetry of Extraoral Photobiomodulation. Diagnostics 2021, 11, 2207. https://doi.org/10.3390/diagnostics11122207
Yaroslavsky AN, Juliano AF, Adnan A, Selting WJ, Iorizzo TW, Carroll JD, Sonis ST, Duncan CN, London WB, Treister NS. Validation of a Monte Carlo Modelling Based Dosimetry of Extraoral Photobiomodulation. Diagnostics. 2021; 11(12):2207. https://doi.org/10.3390/diagnostics11122207
Chicago/Turabian StyleYaroslavsky, Anna N., Amy F. Juliano, Ather Adnan, Wayne J. Selting, Tyler W. Iorizzo, James D. Carroll, Stephen T. Sonis, Christine N. Duncan, Wendy B. London, and Nathaniel S. Treister. 2021. "Validation of a Monte Carlo Modelling Based Dosimetry of Extraoral Photobiomodulation" Diagnostics 11, no. 12: 2207. https://doi.org/10.3390/diagnostics11122207
APA StyleYaroslavsky, A. N., Juliano, A. F., Adnan, A., Selting, W. J., Iorizzo, T. W., Carroll, J. D., Sonis, S. T., Duncan, C. N., London, W. B., & Treister, N. S. (2021). Validation of a Monte Carlo Modelling Based Dosimetry of Extraoral Photobiomodulation. Diagnostics, 11(12), 2207. https://doi.org/10.3390/diagnostics11122207