
Diet in Scleroderma: Is There a Need for Intervention?

 , ,
, , 
Abstract
:1. Introduction
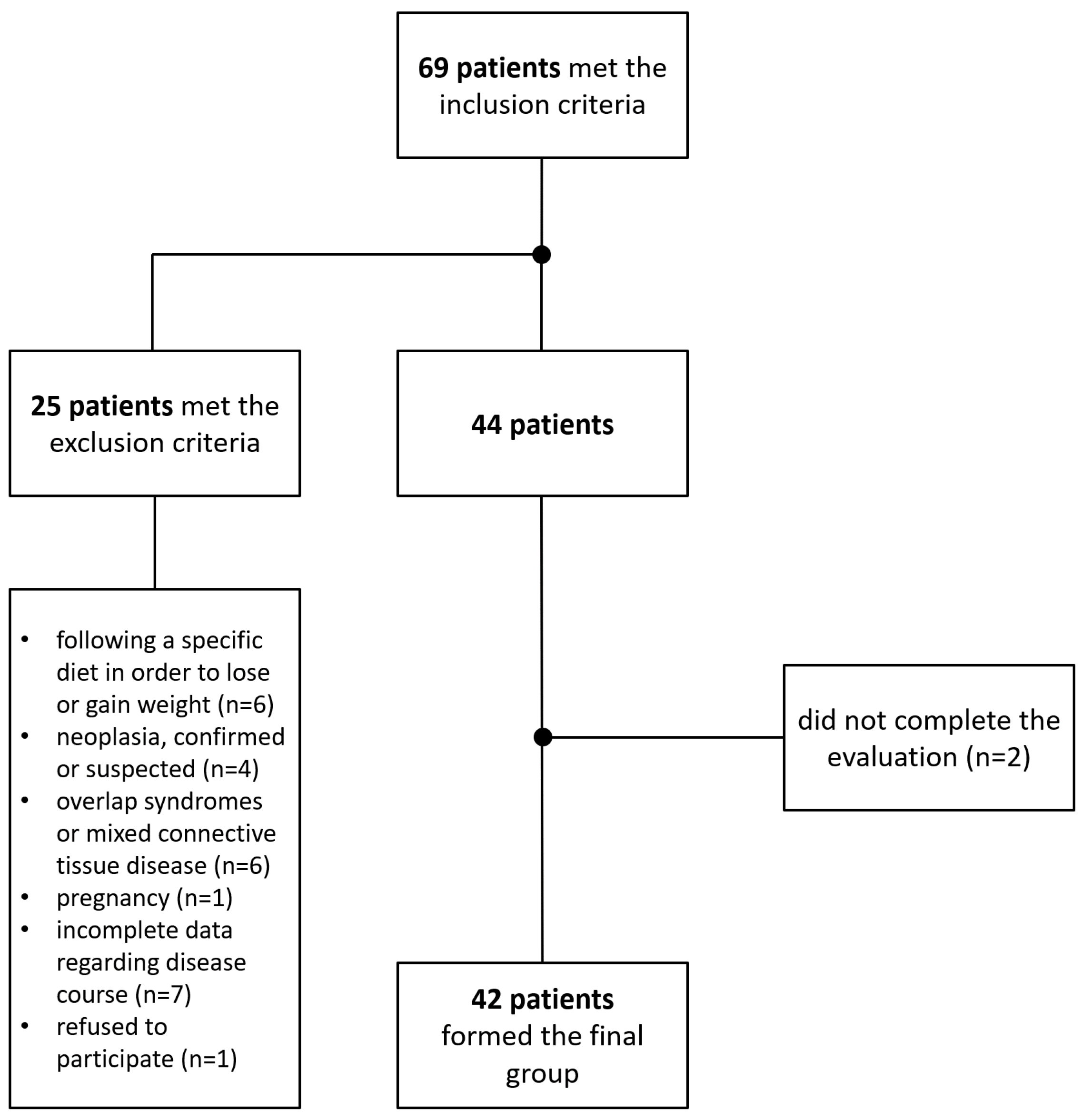
2. Materials and Methods
- Women: EER (kcal/day) = 2403 − 7 × (age − 19);
- Men: EER (kcal/day) = 3067 −10 × (age − 19).
- Women: RFMf = 76 − (20 × H/AC);
- Men: RFMm = 64 − (20 × H/AC);or
- RFM = 64 − (20 × H/AC) + (12 × Gender) (Female = 1, Male = 0).
3. Results
3.1. General Characteristics
3.2. Unintentional Weight Loss and Malnutrition Risk
3.3. Biochemical Parameters
3.4. Eating Habits and EPIC-Norfolk FFQ
3.4.1. Foods and Beverages
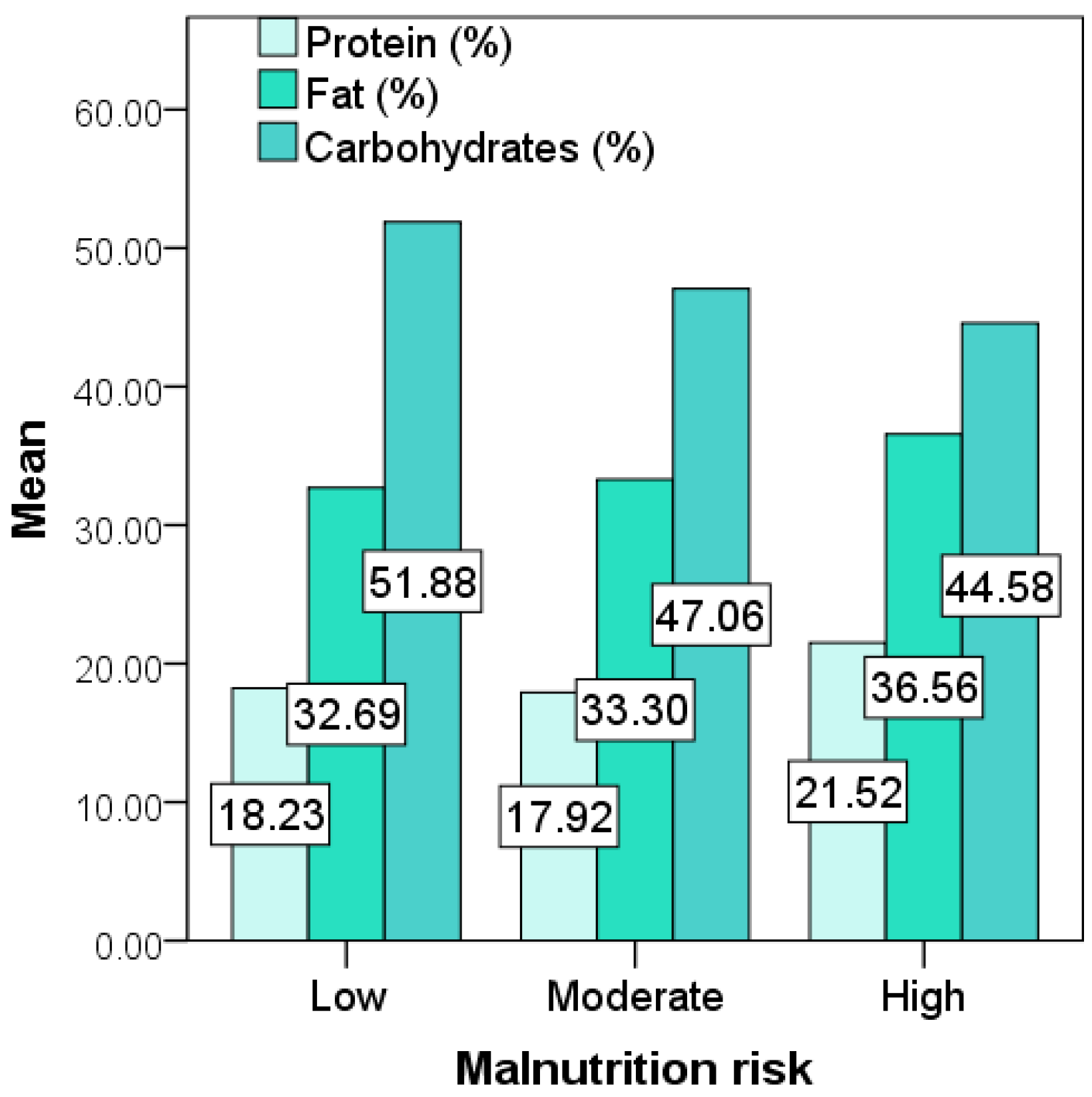
3.4.2. Energy and Macronutrients
3.4.3. Micronutrients and Dietary Fiber
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asano, Y. The Pathogenesis of Systemic Sclerosis: An Understanding Based on a Common Pathologic Cascade across Multiple Organs and Additional Organ-Specific Pathologies. J. Clin. Med. 2020, 9, 2687. [Google Scholar] [CrossRef]
- Hvas, C.L.; Harrison, E.; Eriksen, M.K.; Herrick, A.L.; McLaughlin, J.T.; Lal, S. Nutritional status and predictors of weight loss in patients with systemic sclerosis. Clin. Nutr. ESPEN 2020, 40, 164–170. [Google Scholar] [CrossRef]
- Caimmi, C.; Caramaschi, P.; Venturini, A.; Bertoldo, E.; Vantaggiato, E.; Viapiana, O.; Ferrari, M.; Lippi, G.; Frulloni, L.; Rossini, M. Malnutrition and sarcopenia in a large cohort of patients with systemic sclerosis. Clin. Rheumatol. 2017, 37, 987–997. [Google Scholar] [CrossRef]
- Gullo, A.L.; Mandraffino, G.; Rodríguez-Carrio, J.; Scuruchi, M.; Sinicropi, D.; Postorino, M.; Morace, C.; Giuffrida, C.; Sciortino, D.; Gallizzi, R.; et al. Endocan and Circulating Progenitor Cells in Women with Systemic Sclerosis: Association with Inflammation and Pulmonary Hypertension. Biomedicines 2021, 9, 533. [Google Scholar] [CrossRef] [PubMed]
- Recasens, M.A.; Puig, C.; Ortiz-Santamaría, V. Nutrition in Systemic Sclerosis. Reumatol. Clín. (Engl. Ed.) 2012, 8, 135–140. [Google Scholar] [CrossRef]
- Emmanuel, A. Current management of the gastrointestinal complications of systemic sclerosis. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 461–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medsger, T.A.; Bombardieri, S.; Czirjak, L.; Scorza, R.; Della Rossa, A.; Bencivelli, W. Assessment of disease severity and prognosis. Clin. Exp. Rheumatol. 2003, 21, S42–S46. [Google Scholar]
- Cruz-Dominguez, M.D.P.; García-Collinot, G.; Saavedra, M.A.; Montes-Cortés, D.H.; Morales-Aguilar, R.; Carranza-Muleiro, R.A.; Vera-Lastra, O.L.; Jara, L.J. Malnutrition is an independent risk factor for mortality in Mexican patients with systemic sclerosis: A cohort study. Rheumatol. Int. 2017, 37, 1101–1109. [Google Scholar] [CrossRef]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis. Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [Green Version]
- Valentini, G.; Iudici, M.; Walker, U.A.; Jaeger, V.; Baron, M.; Carreira, P.E.; Czirják, L.; Denton, C.P.; Distler, O.; Hachulla, E.; et al. The European Scleroderma Trials and Research group (EUSTAR) task force for the development of revised activity criteria for systemic sclerosis: Derivation and validation of a preliminarily revised EUSTAR activity index. Ann. Rheum. Dis. 2016, 76, 270–276. [Google Scholar] [CrossRef]
- Ross, L.; Stevens, W.; Wilson, M.; Huq, M.; Strickland, G.; Walker, J.; Sahhar, J.; Ngian, G.-S.; Roddy, J.; Youssef, P.; et al. Performance of the 2017 EUSTAR activity index in an scleroderma cohort. Clin. Rheumatol. 2020, 39, 3701–3705. [Google Scholar] [CrossRef]
- Gherasim, A.; Arhire, L.I.; Nita, O.; Strateanu, R.; Oprescu, A.C.; Graur, M.; Mihalache, L. Can the EPIC food frequency questionnaire be applied to the population in Romania? Rev. Med. Chir. Soc. Med. Nat. 2015, 119, 856–863. [Google Scholar]
- Mulligan, A.A.; Luben, R.; Bhaniani, A.; Parry-Smith, D.J.; O’Connor, L.; Khawaja, A.; Forouhi, N.; Khaw, K.-T. A new tool for converting food frequency questionnaire data into nutrient and food group values: FETA research methods and availability. BMJ Open 2014, 4, e004503. [Google Scholar] [CrossRef] [Green Version]
- Rolfes, S.R.; Pinna, K.; Whitney, E. Understanding Normal and Clinical Nutrition; Cengage Learning: Boston, MA, USA, 2020. [Google Scholar]
- Woolcott, O.O.; Bergman, R.N. Relative fat mass (RFM) as a new estimator of whole-body fat percentage—A cross-sectional study in American adult individuals. Sci. Rep. 2018, 8, 10980. [Google Scholar] [CrossRef] [Green Version]
- WHO/Europe. Nutrition-Body Mass Index-BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 11 June 2021).
- Smith, V.; Scirè, C.A.; Talarico, R.; Airo, P.; Alexander, T.; Allanore, Y.; Bruni, C.; Codullo, V.; Dalm, V.; De Vries-Bouwstra, J.; et al. Systemic sclerosis: State of the art on clinical practice guidelines. RMD Open 2019, 4, e000782. [Google Scholar] [CrossRef] [Green Version]
- Harrison, E.; Herrick, A.; McLaughlin, J.; Lal, S. Malnutrition in systemic sclerosis. Rheumatology 2012, 51, 1747–1756. [Google Scholar] [CrossRef] [PubMed]
- Türk, I.; Cüzdan, N.; Çiftçi, V.; Arslan, D.; Doğan, M.C.; Unal, I. Malnutrition, associated clinical factors, and depression in systemic sclerosis: A cross-sectional study. Clin. Rheumatol. 2019, 39, 57–67. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Romero-Yuste, S.; Carmona, E.C.; Nolla, J.M. Sarcopenia, immune-mediated rheumatic diseases, and nutritional interventions. Aging Clin. Exp. Res. 2021, 1–11. [Google Scholar] [CrossRef]
- Bagnato, G.; Pigatto, E.; Bitto, A.; Pizzino, G.; Irrera, N.; Abignano, G.; Ferrera, A.; Sciortino, D.; Wilson, M.; Squadrito, F.; et al. The PREdictor of MAlnutrition in Systemic Sclerosis (PREMASS) Score: A Combined Index to Predict 12 Months Onset of Malnutrition in Systemic Sclerosis. Front. Med. 2021, 8, 651748. [Google Scholar] [CrossRef] [PubMed]
- Hansi, N.; Thoua, N.; Carulli, M.; Chakravarty, K.; Lal, S.; Smyth, A.; Herrick, A.; Ogunbiyi, O.; Shaffer, J.; McLaughlin, J.; et al. Consensus best practice pathway of the UK scleroderma study group: Gastrointestinal manifestations of systemic sclerosis. Clin. Exp. Rheumatol. 2014, 32, 214–221. [Google Scholar]
- Frech, T.M.; Mar, D. Gastrointestinal and Hepatic Disease in Systemic Sclerosis. Rheum. Dis. Clin. N. Am. 2018, 44, 15–28. [Google Scholar] [CrossRef]
- Li, X.; Kimita, W.; Cho, J.; Ko, J.; Bharmal, S.; Petrov, M. Dietary Fibre Intake in Type 2 and New-Onset Prediabetes/Diabetes after Acute Pancreatitis: A Nested Cross-Sectional Study. Nutrients 2021, 13, 1112. [Google Scholar] [CrossRef]
- Jones, N.R.V.; Forouhi, N.G.; Khaw, K.-T.; Wareham, N.J.; Monsivais, P. Accordance to the Dietary Approaches to Stop Hypertension diet pattern and cardiovascular disease in a British, population-based cohort. Eur. J. Epidemiol. 2018, 33, 235–244. [Google Scholar] [CrossRef] [Green Version]
- Alegria-Lertxundi, I.; Aguirre, C.; Bujanda, L.; Fernández, F.J.; Polo, F.; Ordovás, J.M.; Etxezarraga, M.C.; Zabalza, I.; Larzabal, M.; Portillo, I.; et al. Gene–Diet Interactions in Colorectal Cancer: Survey Design, Instruments, Participants and Descriptive Data of a Case–Control Study in the Basque Country. Nutrients 2020, 12, 2362. [Google Scholar] [CrossRef]
- Verger, E.O.; Armstrong, P.; Nielsen, T.; Chakaroun, R.; Aron-Wisnewsky, J.; Gøbel, R.J.; Schütz, T.; Delaere, F.; Gausseres, N.; Clément, K.; et al. Dietary Assessment in the MetaCardis Study: Development and Relative Validity of an Online Food Frequency Questionnaire. J. Acad. Nutr. Diet. 2017, 117, 878–888. [Google Scholar] [CrossRef]
- Machowicz, A.; Hall, I.; De Pablo, P.; Rauz, S.; Richards, A.; Higham, J.; Poveda-Gallego, A.; Imamura, F.; Bowman, S.J.; Barone, F.; et al. Mediterranean diet and risk of Sjögren’s syndrome. Clin. Exp. Rheumatol. 2020, 38, 216–221. [Google Scholar] [PubMed]
- Parker, R.; Kim, S.-J.; Gao, B. Alcohol, adipose tissue and liver disease: Mechanistic links and clinical considerations. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Trius-Soler, M.; Vilas-Franquesa, A.; Tresserra-Rimbau, A.; Sasot, G.; Storniolo, C.E.; Estruch, R.; Lamuela-Raventós, R.M. Effects of the Non-Alcoholic Fraction of Beer on Abdominal Fat, Osteoporosis, and Body Hydration in Women. Molecules 2020, 25, 3910. [Google Scholar] [CrossRef] [PubMed]
- Akahane, T.; Namisaki, T.; Kaji, K.; Moriya, K.; Kawaratani, H.; Takaya, H.; Sawada, Y.; Shimozato, N.; Fujinaga, Y.; Furukawa, M.; et al. Chronic Alcohol Consumption is Inversely Associated with Insulin Resistance and Fatty Liver in Japanese Males. Nutrients 2020, 12, 1036. [Google Scholar] [CrossRef] [Green Version]
- Lal, A.; Peeters, A.; Brown, V.; Nguyen, P.; Tran, H.N.Q.; Nguyen, T.; Tonmukayakul, U.; Sacks, G.; Calache, H.; Martin, J.; et al. The Modelled Population Obesity-Related Health Benefits of Reducing Consumption of Discretionary Foods in Australia. Nutrients 2020, 12, 649. [Google Scholar] [CrossRef] [Green Version]
- St-Onge, M.-P.; Zuraikat, F.M. Reciprocal Roles of Sleep and Diet in Cardiovascular Health: A Review of Recent Evidence and a Potential Mechanism. Curr. Atheroscler. Rep. 2019, 21, 11. [Google Scholar] [CrossRef]
- Partearroyo, T.; Samaniego-Vaesken, M.D.L.; Ruiz, E.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Sodium Intake from Foods Exceeds Recommended Limits in the Spanish Population: The ANIBES Study. Nutrients 2019, 11, 2451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismail, L.C.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Zampelas, A.; Habib-Mourad, C.; Abu Jamous, D.O.; Ali, H.I.; Al Sabbah, H.; et al. Assessment of eating habits and lifestyle during the coronavirus 2019 pandemic in the Middle East and North Africa region: A cross-sectional study. Br. J. Nutr. 2020, 126, 1–10. [Google Scholar] [CrossRef]
- Neto, H.A.P.; Ausina, P.; Gomez, L.S.; Leandro, J.; Zancan, P.; Sola-Penna, M. Effects of Food Additives on Immune Cells as Contributors to Body Weight Gain and Immune-Mediated Metabolic Dysregulation. Front. Immunol. 2017, 8, 1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laffer, C.L.; Scott, I.R.C.; Titze, J.M.; Luft, F.C.; Elijovich, F. Hemodynamics and Salt-and-Water Balance Link Sodium Storage and Vascular Dysfunction in Salt-Sensitive Subjects. Hypertension 2016, 68, 195–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, M.; Moser, D.; Miller, J.; Lennie, T. Association of age and dietary sodium intake in patients with heart failure: Testing mediating effects of preference for salt and enjoyment of sodium-restricted diet. Eur. J. Cardiovasc. Nurs. 2021, 20, zvab060.098. [Google Scholar] [CrossRef]
- Patel, Y.; Joseph, J. Sodium Intake and Heart Failure. Int. J. Mol. Sci. 2020, 21, 9474. [Google Scholar] [CrossRef]
- Abu-Sawwa, R.; Dunbar, S.B.; Quyyumi, A.A.; Sattler, E.L.P. Nutrition intervention in heart failure: Should consumption of the DASH eating pattern be recommended to improve outcomes? Hear. Fail. Rev. 2019, 24, 565–573. [Google Scholar] [CrossRef]
- He, F.J.; Tan, M.; Ma, Y.; MacGregor, G.A. Salt Reduction to Prevent Hypertension and Cardiovascular Disease. J. Am. Coll. Cardiol. 2020, 75, 632–647. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.; Mente, A.; Alderman, M.H.; Brady, A.J.B.; Diaz, R.; Gupta, R.; López-Jaramillo, P.; Luft, F.C.; Lüscher, T.F.; Mancia, G.; et al. Salt and cardiovascular disease: Insufficient evidence to recommend low sodium intake. Eur. Hear. J. 2020, 41, 3363–3373. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. Role of salt intake in prevention of cardiovascular disease: Controversies and challenges. Nat. Rev. Cardiol. 2018, 15, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Hanipah, Z.N.; Mulcahy, M.J.; Sharma, G.; Punchai, S.; Steckner, K.; Dweik, R.; Aminian, A.; Schauer, P.R.; Brethauer, S.A. Bariatric surgery in patients with pulmonary hypertension. Surg. Obes. Relat. Dis. 2018, 14, 1581–1586. [Google Scholar] [CrossRef]
- Salman, A.A.; Salman, M.A.; Shaaban, H.E.-D.; Abdelsalam, A.; Tourky, M.; Lotfy, S.M.; Omar, H.S.E.; Mostafa, M.S.; Nafea, M.A.; Sultan, A.A.E.A.; et al. Effect of Bariatric Surgery on the Cardiovascular System in Obese Cases with Pulmonary Hypertension. Obes. Surg. 2021, 31, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Corsetti, G.; Pasini, E.; Romano, C.; Chen-Scarabelli, C.; Scarabelli, T.; Flati, V.; Saravolatz, L.; Dioguardi, F. How Can Malnutrition Affect Autophagy in Chronic Heart Failure? Focus and Perspectives. Int. J. Mol. Sci. 2021, 22, 3332. [Google Scholar] [CrossRef]
- Matsumura, K.; Teranaka, W.; Taniichi, M.; Otagaki, M.; Takahashi, H.; Fujii, K.; Yamamoto, Y.; Nakazawa, G.; Shiojima, I. Differential effect of malnutrition between patients hospitalized with new-onset heart failure and worsening of chronic heart failure. ESC Hear. Fail. 2021, 8, 1819–1826. [Google Scholar] [CrossRef] [PubMed]
- Sze, S.; Pellicori, P.; Zhang, J.; Clark, A.L. Malnutrition, congestion and mortality in ambulatory patients with heart failure. Heart 2018, 105, 297–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muangchan, C.; Baron, M.; Pope, J.; Canadian Scleroderma Research Group. The 15% Rule in Scleroderma: The Frequency of Severe Organ Complications in Systemic Sclerosis. A Systematic Review. J. Rheumatol. 2013, 40, 1545–1556. [Google Scholar] [CrossRef]
- Abd-Elraheem, M.; Mashav, N.; Ioffe, M.; Kremer, A.; Justo, D. Which laboratory malnutrition markers best predict 1-year mortality in hospitalized older adults? Eur. Geriatr. Med. 2019, 10, 619–624. [Google Scholar] [CrossRef]
- Lahmann, N.A.; Tannen, A.; Suhr, R. Underweight and malnutrition in home care: A multicenter study. Clin. Nutr. 2016, 35, 1140–1146. [Google Scholar] [CrossRef]
- O’Connell, M.L.; Coppinger, T.; McCarthy, A.L. The role of nutrition and physical activity in frailty: A review. Clin. Nutr. ESPEN 2020, 35, 1–11. [Google Scholar] [CrossRef]
- Pellicciotta, M.; Rigoni, R.; Falcone, E.L.; Holland, S.M.; Villa, A.; Cassani, B. The microbiome and immunodeficiencies: Lessons from rare diseases. J. Autoimmun. 2019, 98, 132–148. [Google Scholar] [CrossRef]
- Quigley, E.M.M. The Spectrum of Small Intestinal Bacterial Overgrowth (SIBO). Curr. Gastroenterol. Rep. 2019, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- Polkowska-Pruszyńska, B.; Gerkowicz, A.; Szczepanik-Kułak, P.; Krasowska, D. Small intestinal bacterial overgrowth in systemic sclerosis: A review of the literature. Arch. Dermatol. Res. 2019, 311, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tandaipan, J.L.; Castellví, I. Systemic sclerosis and gastrointestinal involvement. Rev. Colomb. Reumatol. (Engl. Ed.) 2020, 27, 44–54. [Google Scholar] [CrossRef]
- Hoffmann-Vold, A.-M.; Volkmann, E.R. Gastrointestinal involvement in systemic sclerosis: Effects on morbidity and mortality and new therapeutic approaches. J. Scleroderma Relat. Disord. 2021, 6, 37–43. [Google Scholar] [CrossRef]
- Dupont, R.; Longué, M.; Galinier, A.; Frais, C.C.; Ingueneau, C.; Astudillo, L.; Arlet, P.; Adoue, D.; Alric, L.; Prévot, G.; et al. Impact of micronutrient deficiency & malnutrition in systemic sclerosis: Cohort study and literature review. Autoimmun. Rev. 2018, 17, 1081–1089. [Google Scholar] [CrossRef]
- Bering, J.; Griffing, W.L.; Crowell, M.; Umar, S.B. Progression of gastrointestinal symptoms over time in patients with systemic sclerosis. Rheumatol. Int. 2021, 41, 1281–1287. [Google Scholar] [CrossRef]
- Steelandt, A.; Benmostefa, N.; Avouac, J.; Mouthon, L.; Allanore, Y. Ethnic influence on the phenotype of French patients with systemic sclerosis. Jt. Bone Spine 2021, 88, 105081. [Google Scholar] [CrossRef]
- Østbø, N.; Jimenez, E.Y.; Harb, S.; Msc, A.B.; Carrier, M.; Thombs, B.D.; the Scleroderma Patient-Centered Intervention Network (SPIN) Diet and Nutrition Education Patient Advisory Team. Nutrition Information Resources Used by People With Systemic Sclerosis and Perceived Advantages and Disadvantages: A Nominal Group Technique Study. ACR Open Rheumatol. 2021, 3, 540–549. [Google Scholar] [CrossRef]
- Yadlapati, R.; Khan, A. Gastroesophageal Reflux Disease. In Gastrointestinal and Liver Disorders in Women’s Health; Springer International Publishing: New York, NY, USA, 2019; pp. 35–57. [Google Scholar]
- Kowal-Bielecka, O.; Fransen, J.; Avouac, J.; Becker, M.; Kulak, A.; Allanore, Y.; Distler, O.; Clements, P.J.; Cutolo, M.; Czirjak, L.; et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann. Rheum. Dis. 2017, 76, 1327–1339. [Google Scholar] [CrossRef] [Green Version]
- Newberry, C.; Lynch, K. Can We Use Diet to Effectively Treat Esophageal Disease? A Review of the Current Literature. Curr. Gastroenterol. Rep. 2017, 19, 38. [Google Scholar] [CrossRef] [PubMed]
- Okkels, S.; Saxosen, M.; Bügel, S.; Olsen, A.; Klausen, T.; Beck, A. Acceptance of texture-modified in-between-meals among old adults with dysphagia. Clin. Nutr. ESPEN 2018, 25, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Holm, M.O.; Mikkelsen, S.; Zacher, N.; Østergaard, T.; Rasmussen, H.H.; Holst, M. High risk of disease-related malnutrition in gastroenterology outpatients. Nutrition 2020, 75–76, 110747. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; De Lorenzo, R.; D’Amico, M.; Sofia, V.; Roveri, L.; Mele, R.; Saibene, A.; Rovere-Querini, P.; Conte, C. COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clin. Nutr. 2021, 40, 2420–2426. [Google Scholar] [CrossRef] [PubMed]
- Chatindiara, I.; Sheridan, N.; Kruger, M.; Wham, C. Eating less the logical thing to do? Vulnerability to malnutrition with advancing age: A qualitative study. Appetite 2020, 146, 104502. [Google Scholar] [CrossRef] [PubMed]
- Baron, M.; Hudson, M.; Steele, R. Malnutrition Is Common in Systemic Sclerosis: Results from the Canadian Scleroderma Research Group Database. J. Rheumatol. 2009, 36, 2737–2743. [Google Scholar] [CrossRef] [PubMed]
- Pengpid, S.; Vonglokham, M.; Kounnavong, S.; Sychareun, V.; Peltzer, K. The prevalence of underweight and overweight/obesity and its correlates among adults in Laos: A cross-sectional national population-based survey, 2013. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2018, 25, 265–273. [Google Scholar] [CrossRef]
- Kim, H.Y.; Baik, S.J.; Lee, H.A.; Lee, B.K.; Kim, T.H.; Yoo, K. Relative fat mass at baseline and its early change may be a predictor of incident nonalcoholic fatty liver disease. Sci. Rep. 2020, 10, 17491. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, B.R.; Tan, S.-Y.; Daly, R.M.; Via, J.D.; Georgousopoulou, E.N.; George, E.S. Intake of Nuts and Seeds Is Associated with a Lower Prevalence of Nonalcoholic Fatty Liver Disease in US Adults: Findings from 2005–2018 NHANES. J. Nutr. 2021, 151, 3507–3515. [Google Scholar] [CrossRef]
- Willems, A.E.M.; Jong, M.S.; van Beek, A.P.; Nederhof, E.; van Dijk, G. Effects of macronutrient intake in obesity: A meta-analysis of low-carbohydrate and low-fat diets on markers of the metabolic syndrome. Nutr. Rev. 2021, 79, 429–444. [Google Scholar] [CrossRef]
- Chmurzynska, A.; Muzsik, A.; Krzyżanowska-Jankowska, P.; Walkowiak, J.; Bajerska, J. The Effect of Habitual Fat Intake, IL6 Polymorphism, and Different Diet Strategies on Inflammation in Postmenopausal Women with Central Obesity. Nutrients 2019, 11, 1557. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, H.B.; Pereira, A.M.; Melo, T.; Paiva, A.; Domingues, M.R. Lipidomics in autoimmune diseases with main focus on systemic lupus erythematosus. J. Pharm. Biomed. Anal. 2019, 174, 386–395. [Google Scholar] [CrossRef]
- Pérez, I.S.; Valle, F.M.; Guillén-Del-Castillo, A.; Pérez, A.R.; Calàbria, H.C.; Pizzi, M.; Codina, A.F.; Callejas-Moraga, E.; Gálvez, O.O.; Pla, V.F.; et al. Subclinical cardiovascular disease and Systemic Sclerosis: A comparison between risk charts, quantification of coronary calcium and carotid ultrasonography. Autoimmun. Rev. 2018, 17, 900–905. [Google Scholar] [CrossRef]
- Patti, A.M.; Carruba, G.; Cicero, A.F.G.; Banach, M.; Nikolic, D.; Giglio, R.V.; Terranova, A.; Soresi, M.; Giannitrapani, L.; Montalto, G.; et al. Daily Use of Extra Virgin Olive Oil with High Oleocanthal Concentration Reduced Body Weight, Waist Circumference, Alanine Transaminase, Inflammatory Cytokines and Hepatic Steatosis in Subjects with the Metabolic Syndrome: A 2-Month Intervention Study. Metabolites 2020, 10, 392. [Google Scholar] [CrossRef]
- Klonizakis, M.; Grammatikopoulou, M.G.; Theodoridis, X.; Milner, M.; Liu, Y.; Chourdakis, M. Effects of Long-Versus Short-Term Exposure to the Mediterranean Diet on Skin Microvascular Function and Quality of Life of Healthy Adults in Greece and the UK. Nutrients 2019, 11, 2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogerson, D.; Maçãs, D.; Milner, M.; Liu, Y.; Klonizakis, M. Contrasting Effects of Short-Term Mediterranean and Vegan Diets on Microvascular Function and Cholesterol in Younger Adults: A Comparative Pilot Study. Nutrients 2018, 10, 1897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trombetta, A.C.; Smith, V.; Gotelli, E.; Ghio, M.; Paolino, S.; Pizzorni, C.; Vanhaecke, A.; Ruaro, B.; Sulli, A.; Cutolo, M. Vitamin D deficiency and clinical correlations in systemic sclerosis patients: A retrospective analysis for possible future developments. PLoS ONE 2017, 12, e0179062. [Google Scholar] [CrossRef] [PubMed]
- Berardi, S.; Giardullo, L.; Corrado, A.; Cantatore, F.P. Vitamin D and connective tissue diseases. Inflamm. Res. 2020, 69, 453–462. [Google Scholar] [CrossRef] [PubMed]
- An, L.; Sun, M.-H.; Chen, F.; Li, J.-R. Vitamin D levels in systemic sclerosis patients: A meta-analysis. Drug Des. Dev. Ther. 2017, 11, 3119–3125. [Google Scholar] [CrossRef] [Green Version]
- Bratoiu, I.; Burlui, A.; Richter, P.; Cardoneanu, A.; Rezus, C.; Rezus, E. Digestive Dysbiosis in Systemic Scleroderma: A Review. J. Interdiscip. Med. 2021, 6, 53–59. [Google Scholar] [CrossRef]
- Isola, G.; Palazzo, G.; Polizzi, A.; Murabito, P.; Giuffrida, C.; Gullo, A.L. Association of Systemic Sclerosis and Periodontitis with Vitamin D Levels. Nutrients 2021, 13, 705. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Williams, R.C.; Gullo, A.L.; Ramaglia, L.; Matarese, M.; Iorio-Siciliano, V.; Cosio, C.; Matarese, G. Risk association between scleroderma disease characteristics, periodontitis, and tooth loss. Clin. Rheumatol. 2017, 36, 2733–2741. [Google Scholar] [CrossRef] [PubMed]
- Kamo, T.; Takayama, K.; Ishii, H.; Suzuki, K.; Eguchi, K.; Nishida, Y. Coexisting severe frailty and malnutrition predict mortality among the oldest old in nursing homes: A 1-year prospective study. Arch. Gerontol. Geriatr. 2017, 70, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Burlui, A.; Graur, M.; Constantinescu, D.; Cardoneanu, A.; Macovei, L.; Rezus, E. Nutritional Decline in Scleroderma Patients Data from a single Romanian center. Rev. Chim. 2018, 69, 1279–1282. [Google Scholar] [CrossRef]
- Su, L.; Lin, Q.; Li, R.; Mm, Y.H.; Zhang, H.; Song, X.; Ye, J.; Zhang, W.; Hong, J. Prognostic value of nutritional impairment on treatment-related toxicity and survival in patients with nasopharyngeal carcinoma taking normal nutrition before radiotherapy. Head Neck 2020, 42, 3580–3589. [Google Scholar] [CrossRef]
- Sabatino, A.; Cuppari, L.; Stenvinkel, P.; Lindholm, B.; Avesani, C.M. Sarcopenia in chronic kidney disease: What have we learned so far? J. Nephrol. 2021, 34, 1347–1372. [Google Scholar] [CrossRef]
- Gherasim, A.; Arhire, L.I.; Niță, O.; Popa, A.D.; Graur, M.; Mihalache, L. The relationship between lifestyle components and dietary patterns. Proc. Nutr. Soc. 2020, 79, 311–323. [Google Scholar] [CrossRef] [Green Version]
- Burlui, A.; Graur, M.; Gherasim, A.; Cardoneanu, A.; Rezus, E. The role of adipokines in inflammation and connective tissue diseases: Can we face the challenge. Int. J. Med. Dent. 2018, 8, 26–33. [Google Scholar]
- Li, T.; Zhang, Y.; Gong, C.; Wang, J.; Liu, B.; Shi, L.; Duan, J. Prevalence of malnutrition and analysis of related factors in elderly patients with COVID-19 in Wuhan, China. Eur. J. Clin. Nutr. 2020, 74, 871–875. [Google Scholar] [CrossRef] [Green Version]
- Besora-Moreno, M.; Llauradó, E.; Tarro, L.; Solà, R. Social and Economic Factors and Malnutrition or the Risk of Malnutrition in the Elderly: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2020, 12, 737. [Google Scholar] [CrossRef] [Green Version]
- Guily, J.L.S.; Bouvard, É.; Raynard, B.; Goldwasser, F.; Maget, B.; Prevost, A.; Seguy, D.; Romano, O.; Narciso, B.; Couet, C.; et al. NutriCancer: A French observational multicentre cross-sectional study of malnutrition in elderly patients with cancer. J. Geriatr. Oncol. 2018, 9, 74–80. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter (n = 42) | Mean (±SD)/Number (%) | |||
|---|---|---|---|---|
| General Characteristics | ||||
| Age (years) | 51.67 (±12.42) | |||
| Gender | Female 36 (85.7%) | Male 6 (14.3%) | ||
| Area of residence | Urban 24 (57.1%) | Rural 18 (42.1%) | ||
| Disease phenotype | dcSSc 18 (42.9%) | lcSSc 24 (57.1%) | ||
| mRSS | 12.45 (±9.26) | |||
| Duration | 0–5 years 15 (35.7%) | 6–10 years 11 (36.2%) | >10 years 16 (38.1%) | |
| EUSTAR-AI | 2.22 (±1.73) | |||
| Autoantibodies | ||||
| Anti-topoisomerase I | 17 (40.5%) | |||
| Anti-centromere | 24 (57.1%) | |||
| Anti-RNA polymerase III | 1 (2.4%) | |||
| ANA | 38 (90.5%) | |||
| Organ Involvement | ||||
| PAH | 9 (21.4%) | |||
| ILD | 22 (52.4%) | |||
| CHF | 7 (16.7%) | |||
| CKD | 6 (14.29%) | |||
| Arrythmias and conduction defects | 11 (26.2%) | |||
| Gastrointestinal symptoms | 34 (81%) | |||
| Anthropometric Parameters | ||||
| H (cm) | 164.95 (±7.45) | |||
| W (kg) | 64.44 (±13.09) | |||
| Wdg (kg) | 76.09 (±14.14) | |||
| AC (cm) | 82.31 (±13.21) | |||
| HC (cm) | 101.58 (±8.86) | |||
| WHR | 0.80 (±0.09) | |||
| BMI (kg/m2) | 23.63 (±4.14) | |||
| BMIdg (kg/m2) | 27.94 (±4.72) | |||
| RFM | 33.42 (±6.72) | |||
| MAC (cm) | 31.71 (±5.11) | |||
| Parameter (n = 42) | Min | Max | Mean | SD |
|---|---|---|---|---|
| Albumin (mg/dL) | 32.30 | 54.70 | 39.26 | 4.13 |
| Total protein (g/dL) | 6.01 | 9.41 | 7.25 | 0.62 |
| Vitamin D (ng/mL) | 2.52 | 33.89 | 10.39 | 10.42 |
| CRP (mg/dL) | 0.03 | 5.10 | 1.16 | 1.23 |
| AST (mg/dL) | 10.00 | 36.50 | 20.55 | 5.99 |
| ALT (mg/dL) | 6.43 | 49.00 | 19.33 | 9.57 |
| Creatinine (mg/dL) | 0.49 | 1.31 | 0.78 | 0.21 |
| Total cholesterol (mg/dL) | 98.00 | 280.00 | 180.55 | 47.87 |
| Triglycerides (mg/dL) | 37.80 | 202.60 | 100.42 | 44.12 |
| Foods and Beverages (g/day) (Mean ± SD) | Total | Unintentional Weight Loss | p | |
|---|---|---|---|---|
| Present | Absent | |||
| Cereals and cereal products | 217.39 ± 99.59 | 214.93 ± 96.81 | 219.06 ± 103.39 | 0.896 |
| Fruits | 412.97 ± 360.05 | 296.84 ± 215.30 | 491.94 ± 417.75 | 0.085 |
| Vegetables | 213.66 ± 164.85 | 172.10 ± 96.86 | 241.92 ± 195.24 | 0.134 |
| Meat and meat products | 141.12 ± 151.22 | 197.34 ± 218.80 | 102.89 ± 58.21 | 0.100 |
| Fish and fish products | 27.08 ± 22.84 | 30.32 ± 26.10 | 24.88 ± 20.60 | 0.477 |
| Dairy | 390.04 ± 212.26 | 366.60 ± 194.11 | 405.99 ± 226.27 | 0.550 |
| Eggs and egg dishes | 18.02 ± 13.07 | 16.15 ± 10.51 | 19.30 ± 14.63 | 0.421 |
| Fats and oils | 17.55 ± 13.39 | 19.30 ± 12.89 | 16.36 ± 13.86 | 0.487 |
| Sweets, preserves, snacks | 31.48 ± 22.56 | 25.85 ± 29.60 | 39.77 ± 14.26 | 0.048 |
| Nuts and seeds | 6.74 ± 9.06 | 3.94 ± 6.09 | 8.64 ± 10.31 | 0.099 |
| Potatoes | 67.95 ± 55.25 | 84.65 ± 57.01 | 56.61 ± 52.12 | 0.115 |
| Soups | 256.44 ± 204.29 | 348.48 ± 250.34 | 193.86 ± 139.42 | 0.014 |
| Non-alcoholic beverages other than water | 482.83 ± 331.92 | 464.70 ± 348.53 | 495.16 ± 326.86 | 0.777 |
| Alcoholic beverages | 11.86 ± 33.36 | 17.01 ± 47.18 | 8.35 ± 19.63 | 0.483 |
| Energy and Macronutrients (Mean ± SD) | Total | Unintentional Weight Loss | p | |
|---|---|---|---|---|
| Present | Absent | |||
| Energy (kcal) | 1944.05 ± 844.82 | 2153.52 ± 822.56 | 1801.61 ± 571.81 | 0.246 |
| Protein (g) | 90.64 ± 50.93 | 104.47 ± 73.81 | 81.23 ± 23.89 | 0.226 |
| Protein (kcal) | 355.44 ± 204.97 | 417.88 ± 295.25 | 312.99 ± 94.95 | 0.174 |
| Protein (% of energy intake) | 18.67 ± 3.46 | 19.22 ± 3.74 | 18.29 ± 3.28 | 0.412 |
| Lipids—total (g) | 72.84 ± 37.19 | 83.78 ± 48.89 | 65.40 ± 25.03 | 0.117 |
| Lipids (kcal) | 655.53 ± 334.70 | 754.01 ± 440.02 | 588.56 ± 225.29 | 0.167 |
| Lipids (% of energy intake) | 33.31 ± 6.13 | 34.49 ± 5.56 | 32.51 ± 6.47 | 0.295 |
| MUFA (g) | 25.89 ± 13.73 | 29.92 ± 18.08 | 23.15 ± 9.21 | 0.118 |
| PUFA (g) | 13.45 ± 7.30 | 15.55 ± 9.64 | 12.03 ± 4.90 | 0.127 |
| SFA (g) | 27.20 ± 14.80 | 31.92 ± 18.79 | 23.98 ± 10.60 | 0.088 |
| Cholesterol (g) | 384.73 ± 187.17 | 447.77 ± 256.51 | 341.86 ± 106.08 | 0.071 |
| Carbohydrates—total (g) | 241.94 ± 100.17 | 252.74 ± 116.28 | 234.59 ± 89.38 | 0.591 |
| Carbohydrates (kcal) | 967.75 ± 400.68 | 1010.95 ± 465.12 | 938.38 ± 357.51 | 0.571 |
| Carbohydrates (% of energy intake) | 50.26 ± 8.60 | 47.87 ± 8.29 | 51.89 ± 8.58 | 0.137 |
| Fructose (g) | 31.13 ± 21.41 | 29.18 ± 20.95 | 32.46 ± 22.04 | 0.629 |
| Galactose (g) | 0.96 ± 0.87 | 0.87 ± 0.88 | 1.03 ± 0.87 | 0.575 |
| Glucose (g) | 25.07 ± 16.99 | 27.44 ± 20.38 | 23.46 ± 14.49 | 0.492 |
| Lactose (g) | 17.67 ± 9.48 | 16.37 ± 8.49 | 18.55 ± 10.17 | 0.456 |
| Maltose (g) | 2.13 ± 1.62 | 2.68 ± 2.25 | 1.76 ± 0.88 | 0.073 |
| Starch (g) | 102.56 ± 41.29 | 113.31 ± 46.48 | 95.25 ± 36.53 | 0.189 |
| Sucrose (g) | 58.51 ± 27.90 | 61.18 ± 32.02 | 56.70 ± 25.27 | 0.633 |
| Total sugars (g) | 138.54 ± 68.91 | 141.47 ± 77.52 | 136.55 ± 64.01 | 0.830 |
| Micronutrient (Mean ± SD) | Total | Unintentional Weight Loss | p | |
|---|---|---|---|---|
| Present | Absent | |||
| Calcium (mg) | 899.01 ± 368.57 | 894.01 ± 369.56 | 902.41 ± 375.47 | 0.943 |
| Chloride (mg) | 4726.31 ± 2307.33 | 5602.86 ± 2890.13 | 4130.24 ± 1616.13 | 0.041 |
| Copper (mg) | 1.58 ± 0.94 | 1.82 ± 1.29 | 1.41 ± 0.55 | 0.161 |
| Iodine (mg) | 153.65 ± 60.23 | 161.41 ± 66.95 | 148.35 ± 56.01 | 0.513 |
| Iron (mg) | 10.87 ± 4.91 | 12.01 ± 6.64 | 10.08 ± 3.19 | 0.271 |
| Magnesium (mg) | 291.05 ± 116.60 | 293.79 ± 143.49 | 289.18 ± 97.41 | 0.909 |
| Manganese (mg) | 2.90 ± 1.23 | 2.58 ± 1.22 | 3.11 ± 1.21 | 0.178 |
| Nitrogen (mcg) | 14.57 ± 8.13 | 16.67 ± 11.81 | 13.14 ± 3.82 | 0.248 |
| Phosphorus (mg) | 1410.47 ± 612.38 | 1512.21 ± 824.09 | 1341.27 ± 419.01 | 0.439 |
| Potassium (mg) | 3576.92 ± 1636.08 | 3686.49 ± 1996.31 | 3502.40 ±1379.01 | 0.744 |
| Selenium (mcg) | 74.71 ± 33.55 | 80.95 ± 46.44 | 70.47 ± 20.96 | 0.393 |
| Sodium (mg) | 3143.18 ±1563.81 | 3754.11 ± 1963.09 | 2727.73 ± 1079.08 | 0.035 |
| Zinc (mg) | 9.90 ± 5.96 | 11.74 ± 8.57 | 8.65 ± 2.75 | 0.168 |
| Total folate (mcg) | 262.67 ± 120.92 | 255.14 ± 116.11 | 267.77 ± 126.18 | 0.740 |
| Carotene (total) (mcg) | 3456.39 ± 2294.82 | 2729.51 ± 1495.25 | 3950.67 ± 2622.43 | 0.063 |
| Alpha-carotene (mcg) | 489.52 ± 381.31 | 370.98 ± 368.97 | 570.12 ± 375.37 | 0.097 |
| Beta-carotene (mcg) | 2991.77 ± 2030.92 | 2336.63 ± 1257.51 | 3437.25 ± 2341.21 | 0.056 |
| Vitamin A (retinol) (mcg) | 1413.84 ± 1450.35 | 1801.10 ± 1872.36 | 1150.50 ± 1038.19 | 0.156 |
| Vitamin A—retinol equivalents (mcg) | 1996.54 ± 1472.35 | 2270.95 ± 1925.53 | 1809.94 ± 1068.63 | 0.379 |
| Vitamin B1(thiamin) (mg) | 1.54 ± 0.91 | 1.71 ± 1.31 | 1.42 ± 0.49 | 0.402 |
| Vitamin B2 (riboflavin) (mg) | 1.97 ± 0.87 | 2.06 ± 1.14 | 1.89 ± 0.63 | 0.601 |
| Vitamin B3 (niacin) (mg) | 25.45 ± 14.36 | 30.33 ± 20.65 | 22.13 ± 6.30 | 0.069 |
| Vitamin B6 (pyridoxine) (mg) | 2.08 ± 1.11 | 2.25 ± 1.49 | 1.97 ± 0.75 | 0.488 |
| Vitamin B12 (cobalamin) (mcg) | 8.16 ± 6.30 | 10.08 ± 8.61 | 6.84 ± 3.73 | 0.102 |
| Vitamin C (ascorbic acid) (mg) | 120.69 ± 94.70 | 107.28 ± 80.01 | 129.81 ± 104.12 | 0.433 |
| Vitamin D (ergocalciferol) (mcg) | 2.52 ± 1.56 | 2.91 ± 2.05 | 2.26 ± 1.07 | 0.245 |
| Vitamin E(α-tocopherol equivalents) (mg) | 12.40 ± 6.21 | 13.07 ± 7.17 | 11.94 ± 5.57 | 0.591 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burlui, A.M.; Cardoneanu, A.; Macovei, L.A.; Rezus, C.; Boiculese, L.V.; Graur, M.; Rezus, E. Diet in Scleroderma: Is There a Need for Intervention? Diagnostics 2021, 11, 2118. https://doi.org/10.3390/diagnostics11112118
Burlui AM, Cardoneanu A, Macovei LA, Rezus C, Boiculese LV, Graur M, Rezus E. Diet in Scleroderma: Is There a Need for Intervention? Diagnostics. 2021; 11(11):2118. https://doi.org/10.3390/diagnostics11112118
Chicago/Turabian StyleBurlui, Alexandra Maria, Anca Cardoneanu, Luana Andreea Macovei, Ciprian Rezus, Lucian Vasile Boiculese, Mariana Graur, and Elena Rezus. 2021. "Diet in Scleroderma: Is There a Need for Intervention?" Diagnostics 11, no. 11: 2118. https://doi.org/10.3390/diagnostics11112118
APA StyleBurlui, A. M., Cardoneanu, A., Macovei, L. A., Rezus, C., Boiculese, L. V., Graur, M., & Rezus, E. (2021). Diet in Scleroderma: Is There a Need for Intervention? Diagnostics, 11(11), 2118. https://doi.org/10.3390/diagnostics11112118