
Whole-Body [18F]FDG PET/CT Can Alter Diagnosis in Patients with Suspected Rheumatic Disease

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PET/CT Acquisition
2.3. PET/CT Analysis
2.4. Statistical Analysis
3. Results
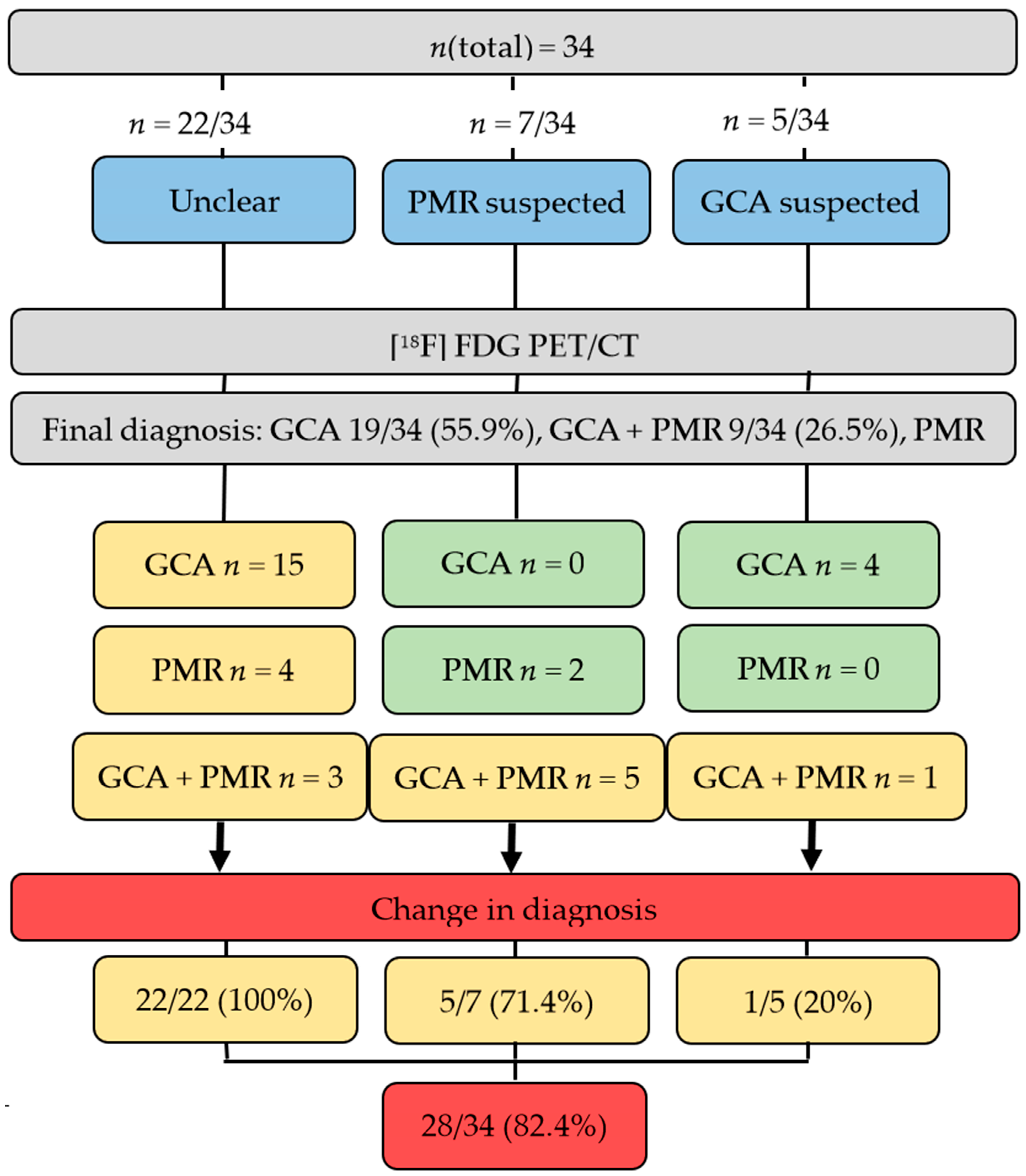
3.1. [18F]FDG PET/CT Can Alter Diagnosis in Individuals with Suspected Diagnosis of Rheumatic Disease
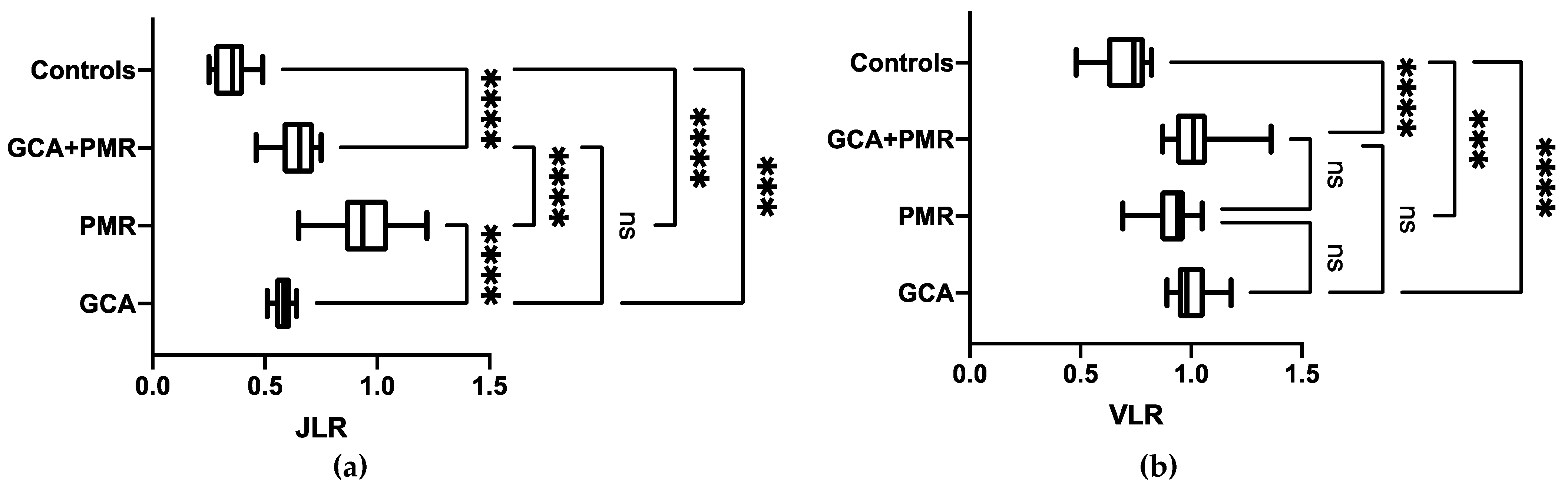
3.2. Semi-Quantitative Assessment Helps in Establishing Final Diagnosis, in Particular for PMR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gonzalez-Gay, M.A.; Vazquez-Rodriguez, T.R.; Lopez-Diaz, M.J.; Miranda-Filloy, J.A.; Gonzalez-Juanatey, C.; Martin, J.; Llorca, J. Epidemiology of giant cell arteritis and polymyalgia rheumatica. Arthritis Care Res. 2009, 61, 1454–1461. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Mohammad, A.J.; Turesson, C. Incidence and prevalence of giant cell arteritis and polymyalgia rheumatica: A systematic literature review. Semin. Arthritis Rheum. 2020, 50, 1040–1048. [Google Scholar] [CrossRef]
- Salvarani, C.; Pipitone, N.; Versari, A.; Hunder, G.G. Clinical features of polymyalgia rheumatica and giant cell arteritis. Nat. Rev. Rheumatol. 2012, 8, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Franzén, P.; Sutinen, S.; von Knorring, J. Giant cell arteritis and polymyalgia rheumatica in a region of Finland: An epidemiologic, clinical and pathologic study, 1984–1988. J. Rheumatol. 1992, 19, 273–276. [Google Scholar] [PubMed]
- Kermani, T.A.; Warrington, K.J. Polymyalgia rheumatica. Lancet 2013, 381, 63–72. [Google Scholar] [CrossRef]
- Nesher, G. Polymyalgia rheumatica—Diagnosis and classification. J. Autoimmun. 2014, 48–49, 76–78. [Google Scholar] [CrossRef]
- Dasgupta, B.; Cimmino, M.A.; Kremers, H.M.; Schmidt, W.A.; Schirmer, M.; Salvarani, C.; Bachta, A.; Dejaco, C.; Duftner, C.; Jensen, H.S.; et al. 2012 Provisional classification criteria for polymyalgia rheumatica: A European League Against Rheumatism/American College of Rheumatology collaborative initiative. Arthritis Rheum. 2012, 64, 943–954. [Google Scholar] [CrossRef] [PubMed]
- Slart, R. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: Joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1250–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribbons, K.B.; Ponte, C.; Carette, S.; Craven, A.; Cuthbertson, D.; Hoffman, G.S.; Khalidi, N.A.; Koening, C.L.; Langford, C.A.; Maksimowicz-McKinnon, K.; et al. Patterns of Arterial Disease in Takayasu Arteritis and Giant Cell Arteritis. Arthritis Care Res. 2020, 72, 1615–1624. [Google Scholar] [CrossRef] [PubMed]
- Schönau, V.; Vogel, K.; Englbrecht, M.; Wacker, J.; Schmidt, D.; Manger, B.; Kuwert, T.; Schett, G. The value of 18F-FDG-PET/CT in identifying the cause of fever of unknown origin (FUO) and inflammation of unknown origin (IUO): Data from a prospective study. Ann. Rheum. Dis. 2018, 77, 70–77. [Google Scholar] [CrossRef]
- Grayson, P.C.; Alehashemi, S.; Bagheri, A.A.; Civelek, A.C.; Cupps, T.R.; Kaplan, M.J.; Malayeri, A.A.; Merkel, P.A.; Novakovich, E.; Bluemke, D.A.; et al. (18) F-Fluorodeoxyglucose-Positron Emission Tomography As an Imaging Biomarker in a Prospective, Longitudinal Cohort of Patients With Large Vessel Vasculitis. Arthritis Rheumatol. 2018, 70, 439–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunder, G.G.; Bloch, D.A.; Michel, B.A.; Stevens, M.B.; Arend, W.P.; Calabrese, L.H.; Edworthy, S.M.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum. 1990, 33, 1122–1128. [Google Scholar] [CrossRef]
- Duell, J.; Krummenast, F.; Schirbel, A.; Klassen, P.; Samnick, S.; Rauert-Wunderlich, H.; Rasche, L.; Buck, A.K.; Wester, H.J.; Rosenwald, A.; et al. Improved primary staging of marginal zone lymphoma by addition of CXCR4-directed PET/CT. J. Nucl. Med. 2021, 62, 1415–1421. [Google Scholar] [CrossRef]
- Sherzay, R.; Witte, T.; Derlin, T.; Hoepfner, M.; Bengel, F.M. Vessel Wall Inflammatory Activity as Determined by F-18 Fluorodeoxyglucose PET in Large Vessel Vasculitis Is Attenuated by Immunomodulatory Drugs. Diagnostics 2021, 11, 1132. [Google Scholar] [CrossRef]
- Medzhitov, R. Origin and physiological roles of inflammation. Nature 2008, 454, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Balink, H.; Bennink, R.J.; Veeger, N.J.; van Eck-Smit, B.L.; Verberne, H.J. Diagnostic utility of (18)F-FDG PET/CT in inflammation of unknown origin. Clin. Nucl. Med. 2014, 39, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Ventura, I.; Reid, P.; Jan, R. Approach to Patients with Suspected Rheumatic Disease. Prim. Care 2018, 45, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Hellmich, B.; Agueda, A.; Monti, S.; Buttgereit, F.; de Boysson, H.; Brouwer, E.; Cassie, R.; Cid, M.C.; Dasgupta, B.; Dejaco, C.; et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann. Rheum. Dis. 2020, 79, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prieto-González, S.; Arguis, P.; García-Martínez, A.; Espígol-Frigolé, G.; Tavera-Bahillo, I.; Butjosa, M.; Sánchez, M.; Hernández-Rodríguez, J.; Grau, J.M.; Cid, M.C. Large vessel involvement in biopsy-proven giant cell arteritis: Prospective study in 40 newly diagnosed patients using CT angiography. Ann. Rheum. Dis. 2012, 71, 1170–1176. [Google Scholar] [CrossRef]
- Blockmans, D.; Ceuninck, L.; Vanderschueren, S.; Knockaert, D.; Mortelmans, L.; Bobbaers, H. Repetitive 18F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: A prospective study of 35 patients. Arthritis Rheum. 2006, 55, 131–137. [Google Scholar] [CrossRef]
- Muratore, F.; Kermani, T.A.; Crowson, C.S.; Green, A.B.; Salvarani, C.; Matteson, E.L.; Warrington, K.J. Large-vessel giant cell arteritis: A cohort study. Rheumatology 2015, 54, 463–470. [Google Scholar] [CrossRef] [Green Version]
- de Boysson, H.; Liozon, E.; Lambert, M.; Parienti, J.-J.; Artigues, N.; Geffray, L.; Boutemy, J.; Ollivier, Y.; Maigné, G.; Ly, K.; et al. 18F-fluorodeoxyglucose positron emission tomography and the risk of subsequent aortic complications in giant-cell arteritis: A multicenter cohort of 130 patients. Medicine 2016, 95, e3851. [Google Scholar] [CrossRef] [PubMed]
- Espitia, O.; Néel, A.; Leux, C.; Connault, J.; Espitia-Thibault, A.; Ponge, T.; Dupas, B.; Barrier, J.H.; Hamidou, M.A.; Agard, C. Giant Cell Arteritis with or without Aortitis at Diagnosis. A Retrospective Study of 22 Patients with Longterm Followup. J. Rheumatol. 2012, 39, 2157–2162. [Google Scholar] [CrossRef] [PubMed]
- Nuenninghoff, D.M.; Hunder, G.G.; Christianson, T.J.H.; McClelland, R.L.; Matteson, E.L. Incidence and predictors of large-artery complication (aortic aneurysm, aortic dissection, and/or large-artery stenosis) in patients with giant cell arteritis: A population-based study over 50 years. Arthritis Rheum. 2003, 48, 3522–3531. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Peña, D.; Martínez-Rodríguez, I.; Loricera, J.; Banzo, I.; Calderón-Goercke, M.; Calvo-Río, V.; González-Vela, C.; Corrales, A.; Castañeda, S.; Blanco, R.; et al. Predictors of positive (18)F-FDG PET/CT-scan for large vessel vasculitis in patients with persistent polymyalgia rheumatica. Semin. Arthritis Rheum. 2019, 48, 720–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Palma, M.J.; Ketchum, J.M.; Saullo, T. What is the source of chronic low back pain and does age play a role? Pain Med. 2011, 12, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henckaerts, L.; Gheysens, O.; Vanderschueren, S.; Goffin, K.; Blockmans, D. Use of 18F-fluorodeoxyglucose positron emission tomography in the diagnosis of polymyalgia rheumatica-A prospective study of 99 patients. Rheumatology 2018, 57, 1908–1916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blockmans, D.; Stroobants, S.; Maes, A.; Mortelmans, L. Positron emission tomography in giant cell arteritis and polymyalgia rheumatica: Evidence for inflammation of the aortic arch. Am. J. Med. 2000, 108, 246–249. [Google Scholar] [CrossRef]
- Besson, F.L.; de Boysson, H.; Parienti, J.J.; Bouvard, G.; Bienvenu, B.; Agostini, D. Towards an optimal semiquantitative approach in giant cell arteritis: An (18)F-FDG PET/CT case-control study. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Hautzel, H.; Sander, O.; Heinzel, A.; Schneider, M.; Müller, H.-W. Assessment of Large-Vessel Involvement in Giant Cell Arteritis with 18F-FDG PET: Introducing an ROC-Analysis–Based Cutoff Ratio. J. Nucl. Med. 2008, 49, 1107. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, P.; Buchtala, S.; Achajew, N.; Haerle, P.; Ehrenstein, B.; Lighvani, H.; Fleck, M.; Marienhagen, J. 18F-FDG PET as a diagnostic procedure in large vessel vasculitis—A controlled, blinded re-examination of routine PET scans. Clin. Rheumatol. 2011, 30, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Prieto-González, S.; Depetris, M.; García-Martínez, A.; Espigol-Frigolé, G.; Tavera-Bahillo, I.; Corbera-Bellata, M.; Planas-Rigol, E.; Alba, M.; Hernández-rodríguez, J.; Grau, J.; et al. Positron emission tomography assessment of large vessel inflammation in patients with newly diagnosed, biopsy-proven giant cell arteritis: A prospective, case control study. Ann. Rheum. Dis. 2014, 73, 1388–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soret, M.; Bacharach, S.L.; Buvat, I. Partial-Volume Effect in PET Tumor Imaging. J. Nucl. Med. 2007, 48, 932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dashora, H.R.; Rosenblum, J.S.; Quinn, K.A.; Alessi, H.; Novakovich, E.; Saboury, B.; Ahlman, M.A.; Grayson, P. Comparing Semi-quantitative and Qualitative Methods of Vascular FDG-PET Activity Measurement in Large-Vessel Vasculitis. J. Nucl. Med. 2021. [Google Scholar] [CrossRef]
- Van der Geest, K.S.M.; Treglia, G.; Glaudemans, A.W.J.M.; Brouwer, E.; Sandovici, M.; Jamar, F.; Gheysens, O.; Slart, R.H.J.A. Diagnostic value of [18F]FDG-PET/CT for treatment monitoring in large vessel vasculitis: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3886–3902. [Google Scholar] [CrossRef]
- Daisaki, H.; Kitajima, K.; Nakajo, M.; Watabe, T.; Ito, K.; Sakamoto, F.; Nakahara, T.; Ishibashi, M.; Toriihara, A. Usefulness of semi-automatic harmonization strategy of standardized uptake values for multicenter PET studies. Sci. Rep. 2021, 11, 8517. [Google Scholar] [CrossRef]
- Werner, R.A.; Hess, A.; Koenig, T.; Diekmann, J.; Derlin, T.; Melk, A.; Thackeray, J.T.; Bauersachs, J.; Bengel, F.M. Molecular imaging of inflammation crosstalk along the cardio-renal axis following acute myocardial infarction. Theranostics 2021, 11, 7984–7994. [Google Scholar] [CrossRef]
- Hess, A.; Derlin, T.; Koenig, T.; Diekmann, J.; Wittneben, A.; Wang, Y.; Wester, H.J.; Ross, T.L.; Wollert, K.C.; Bauersachs, J.; et al. Molecular imaging-guided repair after acute myocardial infarction by targeting the chemokine receptor CXCR4. Eur. Heart J. 2020, 41, 3564–3575. [Google Scholar] [CrossRef]
- Reiter, T.; Kircher, M.; Schirbel, A.; Werner Rudolf, A.; Kropf, S.; Ertl, G.; Buck Andreas, K.; Wester, H.-J.; Bauer Wolfgang, R.; Lapa, C. Imaging of C-X-C Motif Chemokine Receptor CXCR4 Expression After Myocardial Infarction With [68Ga] Pentixafor-PET/CT in Correlation with Cardiac MRI. JACC Cardiovasc. Imaging 2018, 11, 1541–1543. [Google Scholar] [CrossRef]
- Werner, R.A.; Koenig, T.; Diekmann, J.; Haghikia, A.; Derlin, T.; Thackeray, J.T.; Napp, L.C.; Wester, H.J.; Ross, T.L.; Schaefer, A.; et al. CXCR4-Targeted Imaging of Post-Infarct Myocardial Tissue Inflammation: Prognostic Value After Reperfused Myocardial Infarction. JACC Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef]
- Dejaco, C.; Singh, Y.P.; Perel, P.; Hutchings, A.; Camellino, D.; Mackie, S.; Abril, A.; Bachta, A.; Balint, P.; Barraclough, K.; et al. 2015 Recommendations for the management of polymyalgia rheumatica: A European League Against Rheumatism/American College of Rheumatology collaborative initiative. Ann. Rheum. Dis. 2015, 74, 1799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, B.D.; Gormsen, L.C.; Hansen, I.T.; Keller, K.K.; Therkildsen, P.; Hauge, E.M. Three days of high-dose glucocorticoid treatment attenuates large-vessel 18F-FDG uptake in large-vessel giant cell arteritis but with a limited impact on diagnostic accuracy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Dejaco, C.; Brouwer, E.; Mason, J.C.; Buttgereit, F.; Matteson, E.L.; Dasgupta, B. Giant cell arteritis and polymyalgia rheumatica: Current challenges and opportunities. Nat. Rev. Rheumatol. 2017, 13, 578–592. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total |
|---|---|
| Clinical Parameters | |
| Female | 20/34 (58.8) |
| Age (Mean ± SD) | 68 ± 9.7 |
| Symptoms | |
| Vision loss | 1 (2.9) |
| Jaw claudication | 3 (8.8) |
| Headache | 4 (11.8) |
| Abdominal pain | 6 (17.6) |
| Fever | 10 (29.4) |
| Night sweats | 11 (32.3) |
| Weight loss | 12 (35.3) |
| Arthritis/arthralgia | 13 (38.2) |
| -Shoulder/pelvic girdle Pain | 7 (20.6) |
| -Pain in the spine, thigh or other presentations | 6 (17.6) |
| Weakness | 15 (44.1) |
| Laboratory markers of inflammation | |
| CRP, available in | 34/34 (100) |
| Mean ± SD (mg/dl) | 5.2 ± 5.9 |
| abnormal (≥0.5 mg/dl) | 32/34 (94.1) |
| ESR, available in | 28/34 (82.3) |
| Mean ± SD (mm/1st hour) | 56.2 ± 33.4 |
| abnormal (≥50 mm/1st hour) * | 16/28 (57.1) |
| Medication | |
| low dose GC (≤7.5 mg/d) | 4 (11.8) |
| no GC | 30 (88.2) |
| GCA | PMR | GCA + PMR | |||||||
|---|---|---|---|---|---|---|---|---|---|
| SUVmean | VLR | p | SUVmean | VLR | p | SUVmean | VLR | p | |
| Reference Organ | |||||||||
| Liver (Average) | 2.52 ± 0.45 | 2.57 ± 0.74 | 2.31 ± 0.42 | ||||||
| Arterial Segments | |||||||||
| Right carotid artery | 2.46 ± 1.14 | 0.99 ± 0.46 | 2.49 ± 1.34 | 0.97 ± 0.52 | 2.40 ± 0.93 | 1.04 ± 0.40 | |||
| Left carotid artery | 2.43 ± 0.80 | 0.46 ± 0.32 | 2.09 ± 0.86 | 0.81 ± 0.34 | 2.15 ± 0.84 | 0.91 ± 0.35 | |||
| Innominate artery | 2.25 ± 0.85 | 0.90 ± 0.34 | 2.39 ± 1.41 | 0.93 ± 0.55 | 2.35 ± 0.76 | 0.99 ± 0.32 | |||
| Right subclavian artery | 2.67 ± 1.79 | 1.07 ± 0.72 | 2.35 ± 1.72 | 0.92 ± 0.67 | 2.08 ± 1.23 | 0.88 ± 0.52 | |||
| Left subclavian artery | 2.68 ± 1.57 | 1.08 ± 0.63 | 2.21 ± 2.05 | 0.86 ± 0.80 | 2.52 ± 1.11 | 1.06 ± 0.47 | |||
| Ascending aorta | 2.37 ± 0.55 | 0.95 ± 0.22 | 2.42 ± 0.82 | 0.94 ± 0.32 | 3.22 ± 2.21 | 1.36 ± 0.93 | |||
| Aortic arch | 2.36 ± 0.52 | 0.95 ± 0.21 | 2.47 ± 0.89 | 0.96 ± 0.35 | 2.13 ± 0.51 | 0.90 ± 0.21 | |||
| Descending aorta | 2.63 ± 0.74 | 1.06 ± 0.30 | 2.63 ± 0.73 | 1.02 ± 0.28 | 2.39 ± 0.76 | 1.01 ± 0.32 | |||
| Abdominal aorta | 2.98 ± 0.74 | 1.20 ± 0.30 | 2.71 ± 1.06 | 1.05 ± 0.41 | 2.57 ± 0.58 | 1.08 ± 0.24 | |||
| Right iliac artery | 2.45 ± 1.25 | 0.98 ± 0.50 | 1.76 ± 0.77 | 0.69 ± 0.30 | 2.32 ± 1.04 | 0.98 ± 0.44 | |||
| Left iliac artery | 2.53 ± 0.88 | 1.02 ± 0.35 | 2.49 ± 1.75 | 0.97 ± 0.68 | 2.23 ± 0.68 | 0.94 ± 0.29 | |||
| Average | 2.52 ± 0.20 | 1.01 ± 0.08 | 0.07 * | 2.36 ± 0.26 | 0.92 ± 0.1 | 0.09 † | 2.39 ± 0.31 | 1.04 ± 0.14 | 1 ‡ |
| SUVmean | JLR | SUVmean | JLR | SUVmean | JLR | ||||
| Joints | |||||||||
| Right shoulder | 1.61 ± 0.53 | 0.64 ± 0.21 | 2.48 ± 1.44 | 1.07 ± 0.56 | 1.71 ± 1.00 | 0.74 ± 0.43 | |||
| Left shoulder | 1.70 ± 0.95 | 0.64 ± 0.57 | 2.12 ± 0.92 | 0.92 ± 0.36 | 1.64 ± 0.85 | 0.71 ± 0.37 | |||
| SC joint (right and left) | 1.39 ± 0.47 | 0.55 ± 0.19 | 1.51 ± 0.49 | 0.65 ± 0.19 | 1.64 ± 0.69 | 0.71 ± 0.30 | |||
| Right AC joint | 1.47 ± 0.68 | 0.51 ± 0.14 | 2.35 ± 1.61 | 1.02 ± 0.63 | 1.21 ± 0.52 | 0.52 ± 0.22 | |||
| Left AC joint | 1.29 ± 0.35 | 0.58 ± 0.27 | 1.74 ± 0.83 | 0.75 ± 0.32 | 1.06 ± 0.27 | 0.46 ± 0.12 | |||
| Interspinal ligaments | 1.52 ± 0.54 | 0.60 ± 0.21 | 2.06 ± 0.57 | 0.89 ± 0.21 | 1.58 ± 0.78 | 0.68 ± 0.34 | |||
| Right ischial tuberosity | 1.34 ± 0.38 | 0.57 ± 0.24 | 2.17 ± 1.06 | 0.94 ± 0.41 | 1.45 ± 0.63 | 0.63 ± 0.27 | |||
| Left ischial tuberosity | 1.44 ± 0.61 | 0.53 ± 0.15 | 2.40 ± 1.23 | 1.04 ± 0.48 | 1.38 ± 0.80 | 0.60 ± 0.35 | |||
| Right greater trochanter | 1.53 ± 0.45 | 0.59 ± 0.18 | 2.82 ± 1.52 | 1.22 ± 0.59 | 1.74 ± 0.73 | 0.75 ± 0.32 | |||
| Left greater trochanter | 1.48 ± 0.46 | 0.61 ± 0.18 | 2.15 ± 1.26 | 0.93 ± 0.49 | 1.44 ± 0.47 | 0.63 ± 0.20 | |||
| Average | 1.48 ± 0.12 | 0.58 ± 0.04 | <0.0001 * | 2.18 ± 0.37 | 0.94 ± 0.16 | <0.0001 † | 1.48 ± 0.22 | 0.64 ± 0.09 | 0.08 ‡ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fröhlich, M.; Serfling, S.; Higuchi, T.; Pomper, M.G.; Rowe, S.P.; Schmalzing, M.; Tony, H.-P.; Gernert, M.; Strunz, P.-P.; Portegys, J.; et al. Whole-Body [18F]FDG PET/CT Can Alter Diagnosis in Patients with Suspected Rheumatic Disease. Diagnostics 2021, 11, 2073. https://doi.org/10.3390/diagnostics11112073
Fröhlich M, Serfling S, Higuchi T, Pomper MG, Rowe SP, Schmalzing M, Tony H-P, Gernert M, Strunz P-P, Portegys J, et al. Whole-Body [18F]FDG PET/CT Can Alter Diagnosis in Patients with Suspected Rheumatic Disease. Diagnostics. 2021; 11(11):2073. https://doi.org/10.3390/diagnostics11112073
Chicago/Turabian StyleFröhlich, Matthias, Sebastian Serfling, Takahiro Higuchi, Martin G. Pomper, Steven P. Rowe, Marc Schmalzing, Hans-Peter Tony, Michael Gernert, Patrick-Pascal Strunz, Jan Portegys, and et al. 2021. "Whole-Body [18F]FDG PET/CT Can Alter Diagnosis in Patients with Suspected Rheumatic Disease" Diagnostics 11, no. 11: 2073. https://doi.org/10.3390/diagnostics11112073
APA StyleFröhlich, M., Serfling, S., Higuchi, T., Pomper, M. G., Rowe, S. P., Schmalzing, M., Tony, H.-P., Gernert, M., Strunz, P.-P., Portegys, J., Schwaneck, E.-C., Gadeholt, O., Weich, A., Buck, A. K., Bley, T. A., Guggenberger, K. V., & Werner, R. A. (2021). Whole-Body [18F]FDG PET/CT Can Alter Diagnosis in Patients with Suspected Rheumatic Disease. Diagnostics, 11(11), 2073. https://doi.org/10.3390/diagnostics11112073