
The Current Diagnostic Accuracy on Free Peritoneal Fluid in Computed Tomography to Determinate the Necessity of Surgery in Blunt Bowel and Mesenteric Trauma—Systemic Review and Meta-Analysis

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Data Collection and Validity Assessment
2.3. Statistical Analysis
3. Results
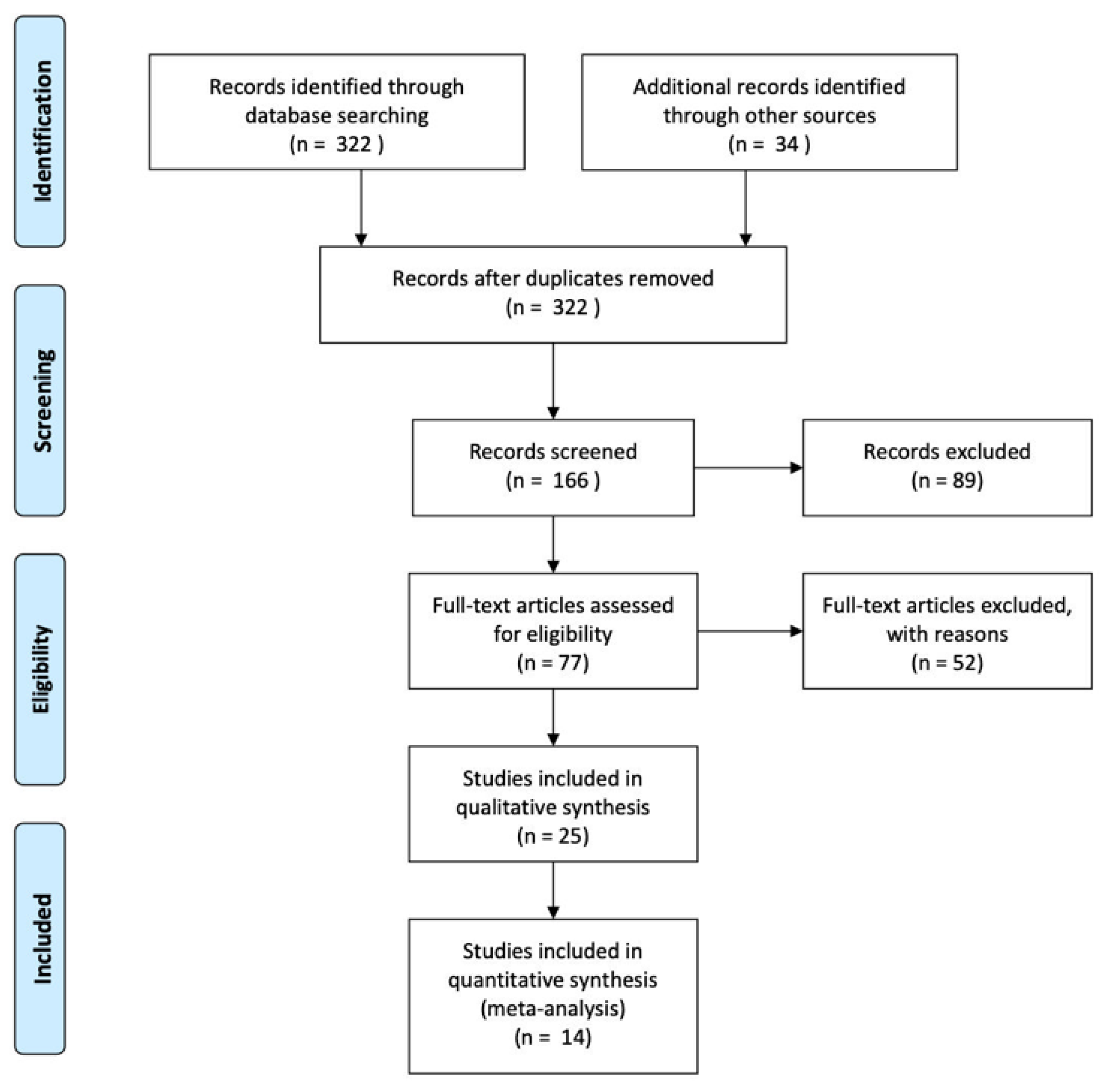
3.1. Search Strategy
3.2. Study Characteristics
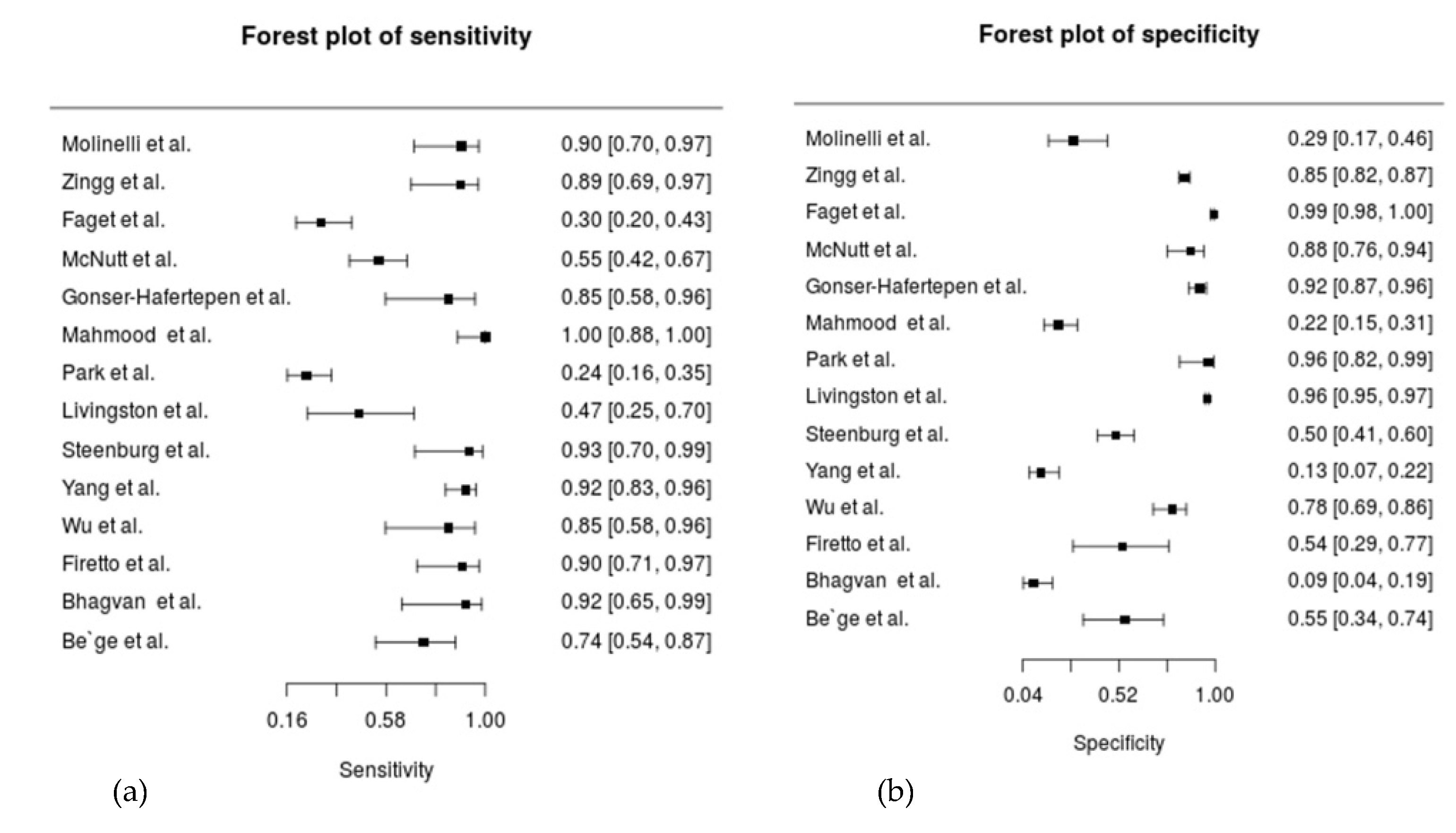
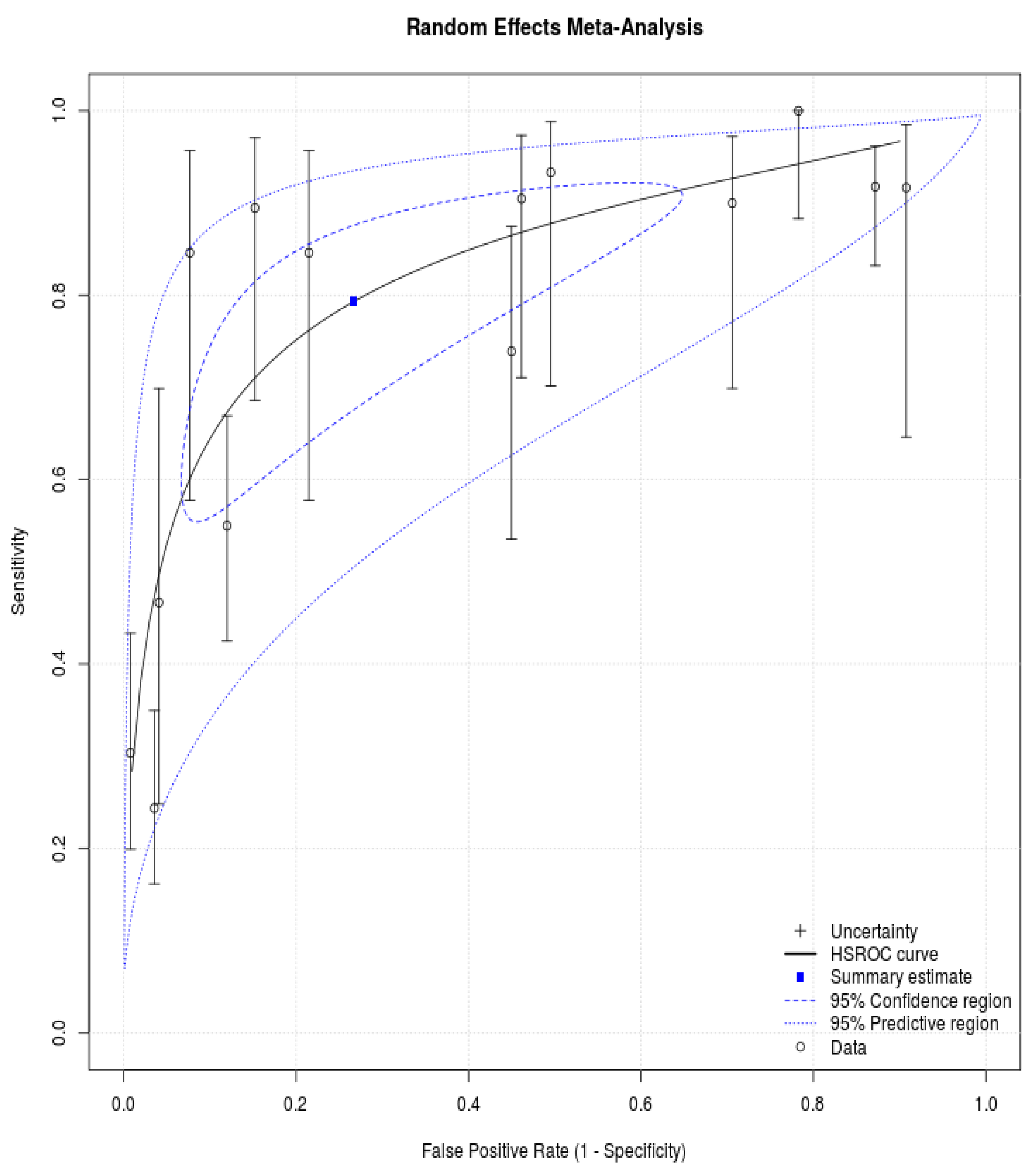
3.3. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liao, C.-H.; Hsieh, F.-J.; Chen, C.-C.; Cheng, C.-T.; Ooyang, C.-H.; Hsieh, C.-H.; Yang, S.-J.; Fu, C.-Y. The Prognosis of Blunt Bowel and Mesenteric Injury—The Pitfall in the Contemporary Image Survey. J. Clin. Med. 2019, 8, 1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, I.; Bew, D.; Elias, D.; Lewis, D.; Meacock, L. Mechanisms of injury and CT findings in bowel and mesenteric trauma. Clin. Radiol. 2014, 69, 639–647. [Google Scholar] [CrossRef]
- Bekker, W.; Kong, V.Y.; Laing, G.L.; Bruce, J.L.; Manchev, V.; Clarke, D. The spectrum and outcome of blunt trauma related enteric hollow visceral injury. Ann. R. Coll. Surg. Engl. 2018, 100, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Malinoski, D.J.; Patel, M.S.; Yakar, D.O.; Green, D.; Qureshi, F.; Inaba, K.; Brown, C.V.R.; Salim, A. A Diagnostic Delay of 5 Hours Increases the Risk of Death After Blunt Hollow Viscus Injury. J. Trauma Inj. Infect. Crit. Care 2010, 69, 84–87. [Google Scholar] [CrossRef]
- Fakhry, S.M.; Brownstein, M.; Watts, D.D.; Baker, C.C.; Oller, D. Relatively Short Diagnostic Delays (<8 Hours) Produce Morbidity and Mortality in Blunt Small Bowel Injury: An Analysis of Time to Operative Intervention in 198 Patients from a Multicenter Experience. J. Trauma Acute Care 2000, 48, 408–415. [Google Scholar] [CrossRef] [PubMed]
- McNutt, M.K.; Chinapuvvula, N.R.; Beckmann, N.M.; Camp, E.A.; Pommerening, M.J.; Laney, R.W.; West, O.C.; Gill, B.S.; Kozar, R.A.; Cotton, B.A.; et al. Early Surgical Intervention for Blunt Bowel Injury: The Bowel Injury Prediction Score (BIPS). J. Trauma Acute Care Surg. 2015, 78, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Chmátal, P.; Lacman, J.; Kupka, P.; Ryska, M. The role of CT for indicating laparotomy in blunt abdominal trauma: Comparing CT results and surgical findings in a group of 101 patients. Prospective study. Perspect. Surg. 2007, 86, 37–40. [Google Scholar]
- Petrosoniak, A.; Engels, P.T.; Hamilton, P.; Tien, H.C. Detection of significant bowel and mesenteric injuries in blunt abdominal trauma with 64-slice computed tomography. J. Trauma Acute Care Surg. 2013, 74, 1081–1086. [Google Scholar] [CrossRef]
- Harmston, C.; Ward, J.B.M.; Patel, A. Clinical outcomes and effect of delayed intervention in patients with hollow viscus injury due to blunt abdominal trauma: A systematic review. Eur. J. Trauma Emerg. Surg. 2018, 44, 369–376. [Google Scholar] [CrossRef]
- Chereau, N.; Wagner, M.; Tresallet, C.; Lucidarme, O.; Raux, M.; Menegaux, F. CT Scan and Diagnostic Peritoneal Lav-age: Towards a Better Diagnosis in the Area of Nonoperative Management of Blunt Abdominal Trauma. Injury 2016, 47, 2006–2011. [Google Scholar] [CrossRef]
- Drasin, T.E.; Anderson, S.; Asandra, A.; Rhea, J.T.; Soto, J.A. MDCT Evaluation of Blunt Abdominal Trauma: Clinical Significance of Free Intraperitoneal Fluid in Males with Absence of Identifiable Injury. Am. J. Roentgenol. 2008, 191, 1821–1826. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Fulcher, A.S.; Turner, M.A.; Cockrell, C.; Halvorsen, R.A. Blunt bowel and mesenteric injury: MDCT diagnosis. Abdom. Imaging 2010, 36, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Scaglione, M.; Tortora, G.; Martino, A.; Di Pietto, F.; Romano, L.; Grassi, R. MDCT in blunt intestinal trauma. Eur. J. Radiol. 2006, 59, 359–366. [Google Scholar] [CrossRef]
- Faget, C.; Taourel, P.; Charbit, J.; Ruyer, A.; Alili, C.; Molinari, N.; Millet, I. Value of CT to Predict Surgically Im-portant Bowel And/or Mesenteric Injury in Blunt Trauma: Performance of a Preliminary Scoring System. Eur. Radiol. 2015, 25, 3620–3628. [Google Scholar] [CrossRef]
- Hines, J.; Rosenblat, J.; Duncan, D.R.; Friedman, B.; Katz, D.S. Perforation of the Mesenteric Small Bowel: Etiologies and CT Findings. Emerg. Radiol. 2013, 20, 155–161. [Google Scholar] [CrossRef]
- Fakhry, S.M.; Allawi, A.; Ferguson, P.L.; Michetti, C.P.; Newcomb, A.B.; Liu, C.; Brownstein, M.R. Blunt small bowel perforation (SBP): An Eastern Association for the Surgery of Trauma Multicenter Update 15 Years Later. J. Trauma Acute Care Surg. 2019, 86, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Firetto, M.C.; Sala, F.; Petrini, M.; Lemos, A.A.; Canini, T.; Magnone, S.; Fornoni, G.; Cortinovis, I.; Sironi, S.; Biondetti, P.R. Blunt bowel and mesenteric trauma: Role of clinical signs along with CT findings in patients’ management. Emerg. Radiol. 2018, 25, 461–467. [Google Scholar] [CrossRef]
- Virmani, V.; George, U.; MacDonald, B.; Sheikh, A. Small-Bowel and Mesenteric Injuries in Blunt Trauma of the Ab-domen. Can. Assoc. Radiol. J. 2013, 64, 140–147. [Google Scholar] [CrossRef] [Green Version]
- LeBedis, C.A.; Anderson, S.W.; Bates, D.D.B.; Khalil, R.; Matherly, D.; Wing, H.; Burke, P.A.; Soto, J.A. CT imaging signs of surgically proven bowel trauma. Emerg. Radiol. 2016, 23, 213–219. [Google Scholar] [CrossRef]
- Molinelli, V.; Iosca, S.; Duka, E.; De Marchi, G.; Lucchina, N.; Bracchi, E.; Carcano, G.; Novario, R.; Fugazzola, C. Ability of Specific and Nonspecific Signs of Multidetector Computed Tomography (MDCT) in the Diagnosis of Blunt Surgi-cally Important Bowel and Mesenteric Injuries. Radiol. Med. 2018, 123, 891–903. [Google Scholar] [CrossRef]
- Landry, B.A.; Patlas, M.N.; Faidi, S.; Coates, A.; Nicolaou, S. Are We Missing Traumatic Bowel and Mesenteric Injuries? Can. Assoc. Radiol. J. 2016, 67, 420–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Altman, D.G.; Liberati, A.; Tetzlaff, J. PRISMA Statement. Epidemiology 2011, 22, 128. [Google Scholar] [CrossRef] [Green Version]
- Freeman, S.C.; Kerby, C.R.; Patel, A.; Cooper, N.J.; Quinn, T.; Sutton, A.J. Development of an Interactive Web-Based Tool to Conduct and Interrogate Meta-Analysis of Diagnostic Test Accuracy Studies: MetaDTA. BMC Med. Res. Methodol. 2019, 19, 81. [Google Scholar] [CrossRef] [PubMed]
- Zingg, T.; Agri, F.; Bourgeat, M.; Yersin, B.; Romain, B.; Schmidt, S.; Keller, N.; Demartines, N. Avoiding Delayed Diagnosis of Significant Blunt Bowel and Mesenteric Injuries: Can a Scoring Tool Make the Difference? A 7-Year Retrospective Cohort Study. Injury 2018, 49, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Gonser-Hafertepen, L.N.; Davis, J.W.; Bilello, J.F.; Ballow, S.L.; Sue, L.P.; Cagle, K.M.; Venugopal, C.; Hafertepen, S.C.; Kaups, K.L. Isolated Free Fluid on Abdominal Computed Tomography in Blunt Trauma: Watch and Wait or Operate? J. Am. Coll. Surg. 2014, 219, 599–605. [Google Scholar] [CrossRef]
- Mahmood, I.; Tawfek, Z.; Abdelrahman, Y.; Siddiuqqi, T.; Abdelrahman, H.; El-Menyar, A.; Al-Hassani, A.; Tuma, M.; Peralta, R.; Zarour, A.; et al. Significance of Computed Tomography Finding of Intra-Abdominal Free Fluid Without Solid Organ Injury after Blunt Abdominal Trauma: Time for Laparotomy on Demand. World J. Surg. 2014, 38, 1411–1415. [Google Scholar] [CrossRef] [PubMed]
- Park, M.-H.; Shin, B.S.; Namgung, H. Diagnostic performance of 64-MDCT for blunt small bowel perforation. Clin. Imaging 2013, 37, 884–888. [Google Scholar] [CrossRef] [PubMed]
- Livingston, D.H.; Lavery, R.F.; Passannante, M.R.; Skurnick, J.H.; Baker, S.; Fabian, T.C.; Fry, D.E.; Malangoni, M.A. Free fluid on abdominal computed tomography without solid organ injury after blunt abdominal injury does not mandate celiotomy. Am. J. Surg. 2001, 182, 6–9. [Google Scholar] [CrossRef]
- Steenburg, S.D.; Petersen, M.J.; Shen, C.; Lin, H. Multi-detector CT of blunt mesenteric injuries: Usefulness of imaging findings for predicting surgically significant bowel injuries. Abdom. Imaging 2014, 40, 1026–1033. [Google Scholar] [CrossRef]
- Yang, X.-Y.; Wei, M.-T.; Jin, C.-W.; Wang, M.; Wang, Z.-Q. Unenhanced Computed Tomography to Visualize Hollow Viscera And/or Mesenteric Injury After Blunt Abdominal Trauma: A Single-Institution Experience. Medicine 2016, 95, e2884. [Google Scholar] [CrossRef]
- Wu, C.-H.; Wang, L.-J.; Wong, Y.-C.; Fang, J.-F.; Lin, B.-C.; Chen, H.-W.; Huang, C.-C.; Hung, S.-C. Contrast-Enhanced Multiphasic Computed Tomography for Identifying Life-Threatening Mesenteric Hemorrhage and Transmural Bowel Injuries. J. Trauma Acute Care Surg. 2011, 71, 543–548. [Google Scholar] [CrossRef]
- Bhagvan, S.; Turai, M.; Holden, A.; Ng, A.; Civil, I. Predicting Hollow Viscus Injury in Blunt Abdominal Trauma with Computed Tomography. World J. Surg. 2013, 37, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Bege, T.; Chaumoître, K.; Leone, M.; Mancini, J.; Berdah, S.V.; Brunet, C. Blunt bowel and mesenteric injuries detected on CT scan: Who is really eligible for surgery? Eur. J. Trauma Emerg. Surg. 2013, 40, 75–81. [Google Scholar] [CrossRef]
- Butela, S.T.; Federle, M.P.; Chang, P.J.; Thaete, F.L.; Peterson, M.S.; Dorvault, C.J.; Hari, A.K.; Soni, S.; Branstetter, B.F.; Paisley, K.J.; et al. Performance of CT in Detection of Bowel Injury. Am. J. Roentgenol. 2001, 176, 129–135. [Google Scholar] [CrossRef]
- Malhotra, A.K.; Fabian, T.C.; Katsis, S.B.; Gavant, M.L.; Croce, M.A. Blunt Bowel and Mesenteric Injuries: The Role of Screening Computed Tomography. J. Trauma Inj. Infect. Crit. Care 2000, 48, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Atri, M.; Hanson, J.M.; Grinblat, L.; Brofman, N.; Chughtai, T.; Tomlinson, G. Surgically Important Bowel and/or Mesenteric Injury in Blunt Trauma: Accuracy of Multidetector CT for Evaluation. Radiology 2008, 249, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.-F.; Wong, Y.-C.; Lin, B.-C.; Hsu, Y.-P.; Chen, M.-F. Usefulness of Multidetector Computed Tomography for the Initial Assessment of Blunt Abdominal Trauma Patients. World J. Surg. 2006, 30, 176–182. [Google Scholar] [CrossRef]
- Rodriguez, C.; Barone, J.E.; Wilbanks, T.O.; Rha, C.-K.; Miller, K. Isolated Free Fluid on Computed Tomographic Scan in Blunt Abdominal Trauma: A Systematic Review of Incidence and Management. J. Trauma Inj. Infect. Crit. Care 2002, 53, 79–85. [Google Scholar] [CrossRef]
- Ng, A.K.T.; Simons, R.K.; Torreggiani, W.C.; Ho, S.G.F.; Kirkpatrick, A.W.; Brown, D.R.G. Intra-abdominal Free Fluid without Solid Organ Injury in Blunt Abdominal Trauma: An Indication for Laparotomy. J. Trauma Inj. Infect. Crit. Care 2002, 52, 1134–1140. [Google Scholar] [CrossRef]
- Cho, H.S.; Woo, J.Y.; Hong, H.-S.; Park, M.H.; Ha, H.I.; Yang, I.; Lee, Y.; Jung, A.Y.; Hwang, J.-Y. Multidetector CT Findings of Bowel Transection in Blunt Abdominal Trauma. Korean J. Radiol. 2013, 14, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.-P.; Liao, C.H. Isolated Free Fluid without Pneumoperitoneum on Computed Tomography in Blunt Abdominal Trauma: Laparotomy Better Based on Imaging Finding and Clinical Presentation. J. Trauma Treat. 2016, 5, 5. [Google Scholar] [CrossRef]
- Lannes, F.; Scemama, U.; Maignan, A.; Boyer, L.; Beyer-Berjot, L.; Berdah, S.V.; Chaumoître, K.; Leone, M.; Bège, T. Value of Early Repeated Abdominal CT in Selective Non-Operative Management for Blunt Bowel and Mesenteric Injury. Eur. Radiol. 2019, 29, 5932–5940. [Google Scholar] [CrossRef]
- Yu, J.; Fulcher, A.S.; Wang, D.-B.; Turner, M.A.; Ha, J.D.; McCulloch, M.; Kennedy, R.M.; Malhotra, A.K.; Halvorsen, R.A. Frequency and Importance of Small Amount of Isolated Pelvic Free Fluid Detected with Multidetector CT in Male Patients with Blunt Trauma. Radiology 2010, 256, 799–805. [Google Scholar] [CrossRef]
- Ormsby, E.L.; Geng, J.; McGahan, J.P.; Richards, J.R. Pelvic free fluid: Clinical importance for reproductive age women with blunt abdominal trauma. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2005, 26, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.C.; Shin, H.C.; Park, S.J.; Park, S.I.; Kim, H.H.; Bae, W.K.; Kim, I.Y.; Jeong, D.S. Traumatic Bowel Perforation: Analysis of CT Findings according to the Perforation Site and the Elapsed Time since Accident. Clin. Imaging 2004, 28, 334–339. [Google Scholar] [CrossRef]
- Raharimanantsoa, M.; Zingg, T.; Thiery, A.; Brigand, C.; Delhorme, J.-B.; Romain, B. Proposal of a new preliminary scoring tool for early identification of significant blunt bowel and mesenteric injuries in patients at risk after road traffic crashes. Eur. J. Trauma Emerg. Surg. 2017, 44, 779–785. [Google Scholar] [CrossRef]
- Lawson, C.M.; Daley, B.J.; Ormsby, C.B.; Enderson, B. Missed Injuries in the Era of the Trauma Scan. J. Trauma Inj. Infect. Crit. Care 2011, 70, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Saku, M.; Yoshimitsu, K.; Murakami, J.; Nakamura, Y.; Oguri, S.; Noguchi, T.; Ayukawa, K.; Honda, H. Small Bowel Perforation Resulting from Blunt Abdominal Trauma: Interval Change of Radiological Characteristics. Radiat. Med. 2006, 24, 358–364. [Google Scholar] [CrossRef]
- Sharma, O.P.; Oswanski, M.F.; Singer, D.; Kenney, B. The Role of Computed Tomography in Diagnosis of Blunt Intestinal and Mesenteric Trauma (BIMT). J. Emerg. Med. 2004, 27, 55–67. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | CT Technique | Equipment Type | TP | FN | FP | TN | n | Sensitivity | Specificity | Weigh Specificity | Weight Sensitivity |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Molinelli et al. [20] | 2018 | 120 kVp, 60–450 mAs, collimation: 1.2 mm × 40, pitch: 1.20. | Somatom Sensation 40 (Siemens) | 18 | 2 | 24 | 10 | 54 | 0.9 | 0.294 | 6.494 | 7.625 |
| Zingg et al. [24] | 2018 | 120 kVp, 300 mA, table speed: 55 mm per rotation (0.8 s), pitch: 1.375 | Light Speed VCT 64 Pro (GE Healthcare) | 17 | 2 | 98 | 545 | 662 | 0.895 | 0.848 | 7.803 | 7.364 |
| Faget et al. [14] | 2015 | 120 kVp, 130 –700 mAs | LightSpeed VCT 16/ 64 detector scanner (GE Healthcare) | 17 | 39 | 4 | 496 | 556 | 0.304 | 0.992 | 7.801 | 5.677 |
| McNutt et al. [6] | 2014 | N/A | Somatom Sensation 40 (Siemens) | 33 | 27 | 6 | 44 | 110 | 0.55 | 0.88 | 7.504 | 7.71 |
| Gonser-Hafertepen et al. [25] | 2014 | N/A | 64-slice he- lical MDCT (GE Healthcare) | 11 | 2 | 11 | 132 | 156 | 0.846 | 0.923 | 7.7 | 6.606 |
| Mahmood et al. [26] | 2014 | N/A | 64-slice scanners (Siemens) | 29 | 0 | 72 | 20 | 121 | 1 | 0.217 | 6.939 | 7.67 |
| Park et al. [27] | 2013 | 120 kVp, 180–380 mAs, nose index: 19, feed/rotation: 39.4 mm, pitch factor: 0.98 | LightSpeed VCT (GE Healthcare) /Somatom Sensation 64 (Siemens) | 19 | 59 | 1 | 27 | 106 | 0.244 | 0.964 | 7.135 | 6.672 |
| Livingston et al. [28] | 2001 | N/A | N/A | 7 | 8 | 83 | 1936 | 2034 | 0.467 | 0.959 | 7.834 | 5.847 |
| Steenburg et al. [29] | 2015 | 120 kVp, 300 mAs | 64-slice helical MDCT scanner (Phillips Healthcare) | 14 | 1 | 55 | 56 | 126 | 0.933 | 0.505 | 7.472 | 7.572 |
| Yang et al. [30] | 2016 | N/A | 64-detector helical CT scanner (Siemens) | 67 | 6 | 68 | 10 | 151 | 0.918 | 0.128 | 6.985 | 7.829 |
| Wu et al. [31] | 2017 | 120 kVp, table speed: 11.25 mm/rotation, 5-mm prospective thickness, 5-mm pro- spective interval | LightSpeed QX/i Scanner (GE Healthcare) | 11 | 2 | 20 | 73 | 106 | 0.846 | 0.785 | 7.573 | 7.297 |
| Firetto et al. [17] | 2018 | N/A | Somatom Definition Flash, (Siemens)/LightSpeed (GE Healthcare) | 19 | 2 | 6 | 7 | 34 | 0.905 | 0.538 | 5.618 | 7.693 |
| Bhagvan et al. [32] | 2013 | N/A | High Speed Advantage (GE Healthcare)/ Volume Zoom (Siemens)/Sensation 16 (Siemens) | 11 | 1 | 59 | 6 | 77 | 0.917 | 0.092 | 6.473 | 6.73 |
| Be`ge et al. [33] | 2014 | 120 kV, 200 mAs | Sensation 64 cardiac scanner (Siemens) | 17 | 6 | 9 | 11 | 43 | 0.739 | 0.55 | 6.67 | 7.708 |
| Parameter | Estimate | 2.5% CI | 97.5% CI |
|---|---|---|---|
| Sensitivity | 0.793 | 0.635 | 0.894 |
| Specificity | 0.733 | 0.468 | 0.896 |
| False Positive Rate | 0.267 | 0.104 | 0.532 |
| Diagnostic Odds Ratio | 10.531 | 5.556 | 19.961 |
| Log Likelihood Ratio + ve | 2.972 | 1.47 | 6.006 |
| Log Likelihood Ratio − ve | 0.282 | 0.188 | 0.424 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.-A.; Wang, C.-Y.; Hsu, C.-P.; Lin, J.-Y.; Cheng, C.-T.; Ouyang, C.-H.; Huang, J.-F.; Liao, C.-H. The Current Diagnostic Accuracy on Free Peritoneal Fluid in Computed Tomography to Determinate the Necessity of Surgery in Blunt Bowel and Mesenteric Trauma—Systemic Review and Meta-Analysis. Diagnostics 2021, 11, 2028. https://doi.org/10.3390/diagnostics11112028
Chen S-A, Wang C-Y, Hsu C-P, Lin J-Y, Cheng C-T, Ouyang C-H, Huang J-F, Liao C-H. The Current Diagnostic Accuracy on Free Peritoneal Fluid in Computed Tomography to Determinate the Necessity of Surgery in Blunt Bowel and Mesenteric Trauma—Systemic Review and Meta-Analysis. Diagnostics. 2021; 11(11):2028. https://doi.org/10.3390/diagnostics11112028
Chicago/Turabian StyleChen, Szu-An, Chen-Yu Wang, Chih-Po Hsu, Jia-Yen Lin, Chi-Tung Cheng, Chun-Hsiang Ouyang, Jen-Fu Huang, and Chien-Hung Liao. 2021. "The Current Diagnostic Accuracy on Free Peritoneal Fluid in Computed Tomography to Determinate the Necessity of Surgery in Blunt Bowel and Mesenteric Trauma—Systemic Review and Meta-Analysis" Diagnostics 11, no. 11: 2028. https://doi.org/10.3390/diagnostics11112028
APA StyleChen, S.-A., Wang, C.-Y., Hsu, C.-P., Lin, J.-Y., Cheng, C.-T., Ouyang, C.-H., Huang, J.-F., & Liao, C.-H. (2021). The Current Diagnostic Accuracy on Free Peritoneal Fluid in Computed Tomography to Determinate the Necessity of Surgery in Blunt Bowel and Mesenteric Trauma—Systemic Review and Meta-Analysis. Diagnostics, 11(11), 2028. https://doi.org/10.3390/diagnostics11112028