
Are Fatigue and Pain Overlooked in Subjects with Stable Chronic Obstructive Pulmonary Disease?
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Assessment of Fatigue, Pain, Breathlessness and Frailty
2.4. Statistical Methods
3. Results
3.1. Characteristics of the Study Subjects
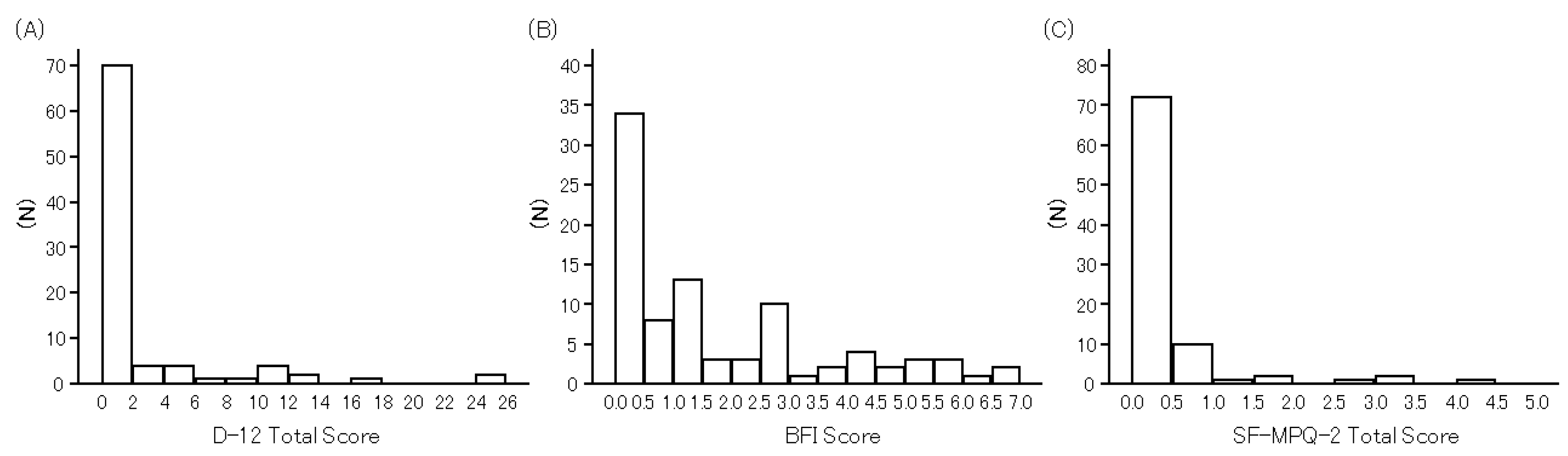
3.2. Internal Consistency and Distribution of Scores
3.3. Relationship between Fatigue and Physiological or Clinical Factors
3.4. Relationship between Pain and Physiological or Clinical Factors
3.5. Relationship between Dyspnoea and Physiological or Clinical Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, G.J.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The GOLD science committee report 2019. Eur. Respir. J. 2019, 53, 1900164. [Google Scholar] [CrossRef] [PubMed]
- Antoniu, S.A.; Apostol, A.; Boiculese, L.V. Extra-respiratory symptoms in patients hospitalized for a COPD exacerbation: Prevalence, clinical burden and their impact on functional status. Clin. Respir. J. 2019, 13, 735–740. [Google Scholar] [CrossRef]
- Walke, L.M.; Byers, A.L.; Tinetti, M.E.; Dubin, J.A.; McCorkle, R.; Fried, T.R. Range and severity of symptoms over time among older adults with chronic obstructive pulmonary disease and heart failure. Arch. Intern. Med. 2007, 167, 2503–2508. [Google Scholar] [CrossRef] [PubMed]
- Blinderman, C.D.; Homel, P.; Billings, J.A.; Tennstedt, S.; Portenoy, R.K. Symptom distress and quality of life in patients with advanced chronic obstructive pulmonary disease. J. Pain Symptom. Manag. 2009, 38, 115–123. [Google Scholar] [CrossRef]
- Peters, J.B.; Heijdra, Y.F.; Daudey, L.; Boer, L.M.; Molema, J.; Dekhuijzen, P.N.; Schermer, T.R.; Vercoulen, J.H. Course of normal and abnormal fatigue in patients with chronic obstructive pulmonary disease, and its relationship with domains of health status. Patient Educ. Couns. 2011, 85, 281–285. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Berman, L.B.; Townsend, M.; Pugsley, S.O.; Chambers, L.W. A measure of quality of life for clinical trials in chronic lung disease. Thorax 1987, 42, 773–778. [Google Scholar] [CrossRef] [Green Version]
- Spruit, M.A.; Vercoulen, J.H.; Sprangers, M.A.G.; Wouters, E.F.M.; Consortium, F.A. Fatigue in COPD: An important yet ignored symptom. Lancet Respir. Med. 2017, 5, 542–544. [Google Scholar] [CrossRef]
- Roberts, M.H.; Mapel, D.W.; Hartry, A.; Von Worley, A.; Thomson, H. Chronic pain and pain medication use in chronic obstructive pulmonary disease. A cross-sectional study. Ann. Am. Thorac. Soc. 2013, 10, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Janssen, D.J.; Wouters, E.F.; Parra, Y.L.; Stakenborg, K.; Franssen, F.M. Prevalence of thoracic pain in patients with chronic obstructive pulmonary disease and relationship with patient characteristics: A cross-sectional observational study. BMC Pulm. Med. 2016, 16, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.W.; Camp, P.G.; Coxson, H.O.; Road, J.D.; Guenette, J.A.; Hunt, M.A.; Reid, W.D. Comorbidities That Cause Pain and the Contributors to Pain in Individuals With Chronic Obstructive Pulmonary Disease. Arch. Phys. Med. Rehabil. 2017, 98, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Andenaes, R.; Momyr, A.; Brekke, I. Reporting of pain by people with chronic obstructive pulmonary disease (COPD): Comparative results from the HUNT3 population-based survey. BMC Public Health 2018, 18, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentsen, S.B.; Miaskowski, C.; Cooper, B.A.; Christensen, V.L.; Henriksen, A.H.; Holm, A.M.; Rustoen, T. Distinct pain profiles in patients with chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 801–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.W.; Camp, P.G.; Coxson, H.O.; Road, J.D.; Guenette, J.A.; Hunt, M.A.; Reid, W.D. A Comparison of Pain, Fatigue, Dyspnea and their Impact on Quality of Life in Pulmonary Rehabilitation Participants with Chronic Obstructive Pulmonary Disease. COPD 2018, 15, 65–72. [Google Scholar] [CrossRef] [PubMed]
- De Miguel-Diez, J.; Lopez-de-Andres, A.; Hernandez-Barrera, V.; Jimenez-Trujillo, I.; Del Barrio, J.L.; Puente-Maestu, L.; Martinez-Huedo, M.A.; Jimenez-Garcia, R. Prevalence of Pain in COPD Patients and Associated Factors: Report From a Population-based Study. Clin. J. Pain 2018, 34, 787–794. [Google Scholar] [CrossRef]
- Maignan, M.; Chauny, J.M.; Daoust, R.; Duc, L.; Mabiala-Makele, P.; Collomb-Muret, R.; Roustit, M.; Maindet, C.; Pepin, J.L.; Viglino, D. Pain during exacerbation of chronic obstructive pulmonary disease: A prospective cohort study. PLoS ONE 2019, 14, e0217370. [Google Scholar] [CrossRef] [Green Version]
- Hansen, J.; Molsted, S.; Ekholm, O.; Hansen, H. Pain Prevalence, Localization, and Intensity in Adults with and without COPD: Results from the Danish Health and Morbidity Survey (a Self-reported Survey). Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 3303–3311. [Google Scholar] [CrossRef]
- Raphaely, R.A.; Mongiardo, M.A.; Goldstein, R.L.; Robinson, S.A.; Wan, E.S.; Moy, M.L. Pain in Veterans with COPD: Relationship with physical activity and exercise capacity. BMC Pulm. Med. 2021, 21, 238. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.L.; Harrison, S.L.; Goldstein, R.S.; Brooks, D. Pain and its clinical associations in individuals with COPD: A systematic review. Chest 2015, 147, 1246–1258. [Google Scholar] [CrossRef]
- Lewthwaite, H.; Williams, G.; Baldock, K.L.; Williams, M.T. Systematic Review of Pain in Clinical Practice Guidelines for Management of COPD: A Case for Including Chronic Pain? Healthcare 2019, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacNee, W. Is Chronic Obstructive Pulmonary Disease an Accelerated Aging Disease? Ann. Am. Thorac. Soc. 2016, 13, S429–S437. [Google Scholar] [CrossRef]
- Liao, S.; Ferrell, B.A. Fatigue in an older population. J. Am. Geriatr. Soc. 2000, 48, 426–430. [Google Scholar] [CrossRef]
- Toye, C.; White, K.; Rooksby, K. Fatigue in frail elderly people. Int. J. Palliat. Nurs. 2006, 12, 202–208. [Google Scholar] [CrossRef]
- Bowden, J.A.; To, T.H.; Abernethy, A.P.; Currow, D.C. Predictors of chronic breathlessness: A large population study. BMC Public Health 2011, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Zengarini, E.; Ruggiero, C.; Perez-Zepeda, M.U.; Hoogendijk, E.O.; Vellas, B.; Mecocci, P.; Cesari, M. Fatigue: Relevance and implications in the aging population. Exp. Gerontol. 2015, 70, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.K.; Currow, D.C.; Abernethy, A.P.; Johnson, M.J.; Miao, Y.; Boscardin, W.J.; Ritchie, C.S. Prevalence and Outcomes of Breathlessness in Older Adults: A National Population Study. J. Am. Geriatr. Soc. 2016, 64, 2035–2041. [Google Scholar] [CrossRef]
- Fukuchi, Y.; Nishimura, M.; Ichinose, M.; Adachi, M.; Nagai, A.; Kuriyama, T.; Takahashi, K.; Nishimura, K.; Ishioka, S.; Aizawa, H.; et al. COPD in Japan: The Nippon COPD Epidemiology study. Respirology 2004, 9, 458–465. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Kusunose, M.; Oga, T.; Nakamura, S.; Hasegawa, Y.; Nishimura, K. Frailty and patient-reported outcomes in subjects with chronic obstructive pulmonary disease: Are they independent entities? BMJ Open Respir. Res. 2017, 4, e000196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, H.; Nakamura, M.; Kida, K.; Kambe, M.; Takahashi, K.; Fujimura, M. Reference values for spirogram and blood gas analysis in Japanese adults. J. Jpn. Respir. Soc. 2001, 39, S1–S17. [Google Scholar]
- Mendoza, T.R.; Wang, X.S.; Cleeland, C.S.; Morrissey, M.; Johnson, B.A.; Wendt, J.K.; Huber, S.L. The rapid assessment of fatigue severity in cancer patients: Use of the Brief Fatigue Inventory. Cancer 1999, 85, 1186–1196. [Google Scholar] [CrossRef]
- Doyle, T.; Palmer, S.; Johnson, J.; Babyak, M.A.; Smith, P.; Mabe, S.; Welty-Wolf, K.; Martinu, T.; Blumenthal, J.A. Association of anxiety and depression with pulmonary-specific symptoms in chronic obstructive pulmonary disease. Int. J. Psychiatry Med. 2013, 45, 189–202. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.W.; Coxson, H.O.; Reid, W.D. Reliability and Validity of the Brief Fatigue Inventory and Dyspnea Inventory in People With Chronic Obstructive Pulmonary Disease. J. Pain Symptom. Manag. 2016, 52, 298–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okuyama, T.; Wang, X.S.; Akechi, T.; Mendoza, T.R.; Hosaka, T.; Cleeland, C.S.; Uchitomi, Y. Validation study of the Japanese version of the brief fatigue inventory. J. Pain Symptom Manag. 2003, 25, 106–117. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Revicki, D.A.; Harding, G.; Coyne, K.S.; Peirce-Sandner, S.; Bhagwat, D.; Everton, D.; Burke, L.B.; Cowan, P.; et al. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain 2009, 144, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Maruo, T.; Nakae, A.; Maeda, L.; Kenrin, S.; Takahashi, K.; Morris, S.; Hosomi, K.; Kanatani, H.; Matsuzaki, T.; Saitoh, Y. Validity, reliability, and assessment sensitivity of the Japanese version of the short-form McGill pain questionnaire 2 in Japanese patients with neuropathic and non-neuropathic pain. Pain Med. 2014, 15, 1930–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yorke, J.; Moosavi, S.H.; Shuldham, C.; Jones, P.W. Quantification of dyspnoea using descriptors: Development and initial testing of the Dyspnoea-12. Thorax 2010, 65, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, K.; Oga, T.; Nakayasu, K.; Taniguchi, H.; Ogawa, T.; Watanabe, F.; Arizono, S.; Kusunose, M.; Sanda, R.; Shibayama, A.; et al. Comparison between tools for measuring breathlessness: Cross-sectional validation of the Japanese version of the Dyspnoea-12. Clin. Respir. J. 2021, 65, 21–26. [Google Scholar] [CrossRef]
- Arai, H.; Satake, S. English translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef] [PubMed]
- Satake, S.; Senda, K.; Hong, Y.J.; Miura, H.; Endo, H.; Sakurai, T.; Kondo, I.; Toba, K. Validity of the Kihon Checklist for assessing frailty status. Geriatr. Gerontol. Int. 2016, 16, 709–715. [Google Scholar] [CrossRef]
- Ebadi, Z.; Goertz, Y.M.J.; Van Herck, M.; Janssen, D.J.A.; Spruit, M.A.; Burtin, C.; Thong, M.S.Y.; Muris, J.; Otker, J.; Looijmans, M.; et al. The prevalence and related factors of fatigue in patients with COPD: A systematic review. Eur. Respir. Rev. 2021, 30, 200298. [Google Scholar] [CrossRef] [PubMed]
- Moy, M.L.; Daniel, R.A.; Cruz Rivera, P.N.; Mongiardo, M.A.; Goldstein, R.L.; Higgins, D.M.; Salat, D.H. Co-occurrence of pain and dyspnea in Veterans with COPD: Relationship to functional status and a pilot study of neural correlates using structural and functional magnetic resonance imaging. PLoS ONE 2021, 16, e0254653. [Google Scholar] [CrossRef]
- Barnes, P.J. Chronic obstructive pulmonary disease: Effects beyond the lungs. PLoS Med. 2010, 7, e1000220. [Google Scholar] [CrossRef] [PubMed]
- Sinden, N.J.; Stockley, R.A. Systemic inflammation and comorbidity in COPD: A result of ‘overspill’ of inflammatory mediators from the lungs? Review of the evidence. Thorax 2010, 65, 930–936. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Moragon, E.; Plaza, V.; Torres, I.; Rosado, A.; Urrutia, I.; Casas, X.; Hinojosa, B.; Blanco-Aparicio, M.; Delgado, J.; Quirce, S. Fibromyalgia as a cause of uncontrolled asthma: A case–control multicenter study. Curr. Med. Res. Opin. 2017, 33, 2181–2186. [Google Scholar] [CrossRef]
- Hyland, M.E.; Lanario, J.W.; Wei, Y.; Jones, R.C.; Masoli, M. Evidence for similarity in symptoms and mechanism: The extra-pulmonary symptoms of severe asthma and the polysymptomatic presentation of fibromyalgia. Immun. Inflamm. Dis. 2019, 7, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Brummel, N.E.; Bell, S.P.; Girard, T.D.; Pandharipande, P.P.; Jackson, J.C.; Morandi, A.; Thompson, J.L.; Chandrasekhar, R.; Bernard, G.R.; Dittus, R.S.; et al. Frailty and Subsequent Disability and Mortality Among Patients With Critical Illness. Am. J. Respir. Crit. Care Med. 2016, 196, 64–72. [Google Scholar] [CrossRef]
- Singer, J.P.; Lederer, D.J.; Baldwin, M.R. Frailty in Pulmonary and Critical Care Medicine. Ann. Am. Thorac. Soc. 2016, 13, 1394–1404. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Median | IQR | Correlation Coefficients (Rs) with | ||||
|---|---|---|---|---|---|---|
| BFI Score | SF-MPQ-2 Total Score | |||||
| Age | years | 78.0 | 74.0–82.0 | 0.165 | 0.162 | |
| BMI | kg/m2 | 22.6 | 20.9–24.4 | 0.036 | 0.121 | |
| Cumulative Smoking | pack-years | 60.0 | 39.0–79.5 | 0.152 | 0.112 | |
| SVC | Liters | 3.22 | 2.54–3.62 | −0.247 * | 0.089 | |
| FEV1 | Liters | 1.69 | 1.31–2.03 | −0.305 ** | 0.062 | |
| FEV1/FVC | % | 58.9 | 48.6–64.2 | −0.242 * | 0.015 | |
| RV/TLC (1) | % | 42.0 | 35.3–50.2 | 0.240 * | −0.039 | |
| DLco (2) | mL/min/mmHg | 10.86 | 6.83–13.55 | −0.260 * | 0.116 | |
| PaO2 (3) | mmHg | 78.1 | 71.9–86.6 | −0.171 | −0.088 | |
| Kihon Checklist Total score | (0–25) | 5 | 2–9 | 0.531 *** | 0.293 ** | |
| BFI score | (0–10) | 1.00 | 0.11–2.78 | N.A. | 0.233 * | |
| SF-MPQ-2 Total score | (0–10) | 0.00 | 0.00–0.27 | 0.233 * | N.A. | |
| Continuous pain | (0–10) | 0.00 | 0.00–0.00 | 0.226 * | 0.753 *** | |
| Intermittent pain | (0–10) | 0.00 | 0.00–0.00 | 0.165 | 0.600 *** | |
| Neuropathic pain | (0–10) | 0.00 | 0.00–0.50 | 0.280 ** | 0.906 *** | |
| Affective descriptors | (0–10) | 0.00 | 0.00–0.00 | 0.401 *** | 0.556 *** | |
| D-12 Total score | (0–36) | 0 | 0–1 | 0.319 ** | 0.045 | |
| D-12 Physical score | (0–21) | 0 | 0–1 | 0.308 ** | 0.049 | |
| D-12 Affect score | (0–15) | 0 | 0–0 | 0.409 *** | −0.005 | |
| Patient-Reported Outcomes | Possible Score Range | Items | Cronbach’s | Score Distribution | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n) | α Coefficient | Mean | SD | Median | Max | Min | IQR | Floor Effect | Ceiling Effect | |||
| BFI score | 0–10 | 9 | 0.975 | 1.70 | 1.92 | 1.00 | 6.78 | 0.00 | 0.11–2.78 | 24.7% | 0.0% | |
| SF-MPQ-2 Total score | 0–10 | 22 | 0.934 | 0.34 | 0.77 | 0.00 | 4.41 | 0.00 | 0.00–0.27 | 50.6% | 0.0% | |
| Continuous pain | 0–10 | 6 | 0.733 | 0.35 | 0.81 | 0.00 | 3.50 | 0.00 | 0.00–0.00 | 76.4% | 0.0% | |
| Intermittent pain | 0–10 | 6 | 0.906 | 0.23 | 0.75 | 0.00 | 5.00 | 0.00 | 0.00–0.00 | 83.1% | 0.0% | |
| Neuropathic pain | 0–10 | 6 | 0.733 | 0.49 | 0.91 | 0.00 | 4.33 | 0.00 | 0.00–0.50 | 56.2% | 0.0% | |
| Affective descriptors | 0–10 | 4 | 0.877 | 0.26 | 0.97 | 0.00 | 6.00 | 0.00 | 0.00–0.00 | 85.4% | 0.0% | |
| D-12 Total score | 0–36 | 12 | 0.960 | 2.2 | 4.8 | 0 | 25 | 0 | 0–1 | 51.7% | 0.0% | |
| D-12 Physical score | 0–21 | 7 | 0.925 | 1.6 | 3.0 | 0 | 15 | 0 | 0–1 | 51.7% | 0.0% | |
| D-12 Affect score | 0–15 | 5 | 0.964 | 0.6 | 1.9 | 0 | 10 | 0 | 0–0 | 86.5% | 0.0% | |
| GOLD 1 (n = 30) | GOLD 2 (n = 46) | GOLD 3+4 (n = 13) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Median | IQR | |||||||||
| Age | years | 77.0 | 71.0 | — | 82.0 | 78.0 | 74.0 | — | 84.0 | 77.0 | 73.0 | — | 80.0 | |
| BMI | kg/m2 | 22.9 | 21.1 | — | 24.2 | 22.9 | 21.0 | — | 25.1 | 21.8 | 18.3 | — | 23.4 | |
| Cumulative Smoking | pack-years | 46.5 ** | 30.0 | — | 61.0 | 66.5 | 50.0 | — | 86.0 | 50.0 | 40.0 | — | 75.0 | |
| SVC | Liters | 3.50 ** | 3.22 | — | 4.05 | 3.08 § | 2.44 | — | 3.57 | 2.39 ¶¶¶ | 2.14 | — | 2.61 | |
| FEV1 | Liters | 2.18 *** | 1.98 | — | 2.45 | 1.59 §§§ | 1.39 | — | 1.83 | 0.85 ¶¶¶ | 0.68 | — | 1.03 | |
| FEV1/FVC | % | 64.3 *** | 59.8 | — | 66.5 | 56.8 §§§ | 48.8 | — | 62.5 | 35.2 ¶¶¶ | 33.1 | — | 40.8 | |
| RV/TLC (1) | % | 35.4 ** | 32.4 | — | 43.5 | 43.4 § | 37.6 | — | 49.3 | 52.4 ¶¶¶ | 50.2 | — | 55.9 | |
| DLco (2) | mL/min/mmHg | 12.34 | 9.52 | — | 14.51 | 10.25 | 6.72 | — | 13.54 | 8.38 ¶ | 5.94 | — | 10.59 | |
| PaO2 (3) | mmHg | 79.0 | 76.0 | — | 87.8 | 80.4 §§ | 72.4 | — | 87.7 | 70.9 ¶¶¶ | 64.8 | — | 72.3 | |
| Kihon Checklist Total score | (0–25) | 3 | 1 | — | 6 | 6 | 2 | — | 10 | 6 | 3 | — | 15 | |
| BFI score | (0–10) | 0.44 | 0.00 | — | 1.89 | 1.00 | 0.00 | — | 2.78 | 2.89 ¶ | 1.00 | — | 5.67 | |
| SF-MPQ-2 Total score | (0–10) | 0.02 | 0.00 | — | 0.45 | 0.05 | 0.00 | — | 0.27 | 0.00 | 0.00 | — | 0.23 | |
| Continuous pain | (0–10) | 0.00 | 0.00 | — | 0.50 | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.00 | |
| Intermittent pain | (0–10) | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.00 | |
| Neuropathic pain | (0–10) | 0.00 | 0.00 | — | 0.50 | 0.00 | 0.00 | — | 0.67 | 0.00 | 0.00 | — | 0.33 | |
| Affective descriptors | (0–10) | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.00 | |
| D-12 Total score | (0–36) | 0 | 0 | — | 1 | 1 §§ | 0 | — | 1 | 8 ¶¶ | 1 | — | 12 | |
| D-12 Physical score | (0–21) | 0 | 0 | — | 1 | 1 §§ | 0 | — | 1 | 7 ¶¶ | 1 | — | 8 | |
| D-12 Affect score | (0–15) | 0 | 0 | — | 0 | 0 §§ | 0 | — | 0 | 0 ¶¶ | 0 | — | 5 | |
| Robust (n = 37) | Pre-Frail (n = 23) | Frail (n = 29) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Median | IQR | |||||||||
| Age | years | 75.0 | 69.0 | — | 80.0 | 77.0 | 75.0 | — | 82.0 | 79.0 ¶ | 76.0 | — | 85.0 | |
| BMI | kg/m2 | 22.7 | 21.1 | — | 24.2 | 21.7 | 19.6 | — | 24.2 | 23.0 | 21.1 | — | 24.8 | |
| Cumulative Smoking | pack-years | 50.0 | 37.0 | — | 61.0 | 56.0 | 38.0 | — | 80.0 | 71.8 ¶ | 50.0 | — | 80.0 | |
| SVC | Liters | 3.39 | 3.00 | — | 3.75 | 3.03 | 2.47 | — | 3.33 | 2.77 ¶ | 2.32 | — | 3.57 | |
| FEV1 | Liters | 2.01 | 1.51 | — | 2.30 | 1.67 | 1.39 | — | 1.99 | 1.49 ¶¶ | 1.03 | — | 1.87 | |
| FEV1/FVC | % | 63.0 | 53.8 | — | 65.0 | 58.5 | 46.7 | — | 64.6 | 57.5 | 42.5 | — | 62.5 | |
| RV/TLC (1) | % | 38.9 * | 33.1 | — | 45.0 | 45.2 | 37.0 | — | 51.0 | 47.0 ¶ | 36.5 | — | 52.4 | |
| DLco (2) | mL/min/mmHg | 12.92 ** | 10.93 | — | 15.01 | 8.85 | 6.34 | — | 11.97 | 9.52 ¶¶ | 5.04 | — | 12.55 | |
| PaO2 (3) | mmHg | 79.0 | 75.2 | — | 88.0 | 81.3 § | 72.8 | — | 92.8 | 73.5 ¶ | 69.4 | — | 79.5 | |
| Kihon Checklist Total score | (0–25) | 2 *** | 1 | — | 2 | 5 §§§ | 5 | — | 6 | 11 ¶¶¶ | 9 | — | 15 | |
| BFI score | (0–10) | 0.22 * | 0.00 | — | 1.00 | 1.89 § | 0.11 | — | 2.78 | 2.89 ¶¶¶ | 1.11 | — | 5.44 | |
| SF-MPQ-2 Total score | (0–10) | 0.00 | 0.00 | — | 0.14 | 0.05 | 0.00 | — | 0.23 | 0.23 ¶ | 0.00 | — | 0.59 | |
| Continuous pain | (0–10) | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.83 | |
| Intermittent pain | (0–10) | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.17 | 0.00 | 0.00 | — | 0.00 | |
| Neuropathic pain | (0–10) | 0.00 | 0.00 | — | 0.17 | 0.00 | 0.00 | — | 0.83 | 0.33 ¶ | 0.00 | — | 1.33 | |
| Affective descriptors | (0–10) | 0.00 | 0.00 | — | 0.00 | 0.00 | 0.00 | — | 0.00 | 0.00 ¶¶ | 0.00 | — | 0.75 | |
| D-12 Total score | (0–36) | 0 | 0 | — | 1 | 1 | 0 | — | 1 | 1 | 0 | — | 5 | |
| D-12 Physical score | (0–21) | 0 | 0 | — | 1 | 1 | 0 | — | 1 | 1 | 0 | — | 5 | |
| D-12 Affect score | (0–15) | 0 | 0 | — | 0 | 0 | 0 | — | 0 | 0 | 0 | — | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimura, K.; Nakayasu, K.; Mori, M.; Sanda, R.; Shibayama, A.; Kusunose, M. Are Fatigue and Pain Overlooked in Subjects with Stable Chronic Obstructive Pulmonary Disease? Diagnostics 2021, 11, 2029. https://doi.org/10.3390/diagnostics11112029
Nishimura K, Nakayasu K, Mori M, Sanda R, Shibayama A, Kusunose M. Are Fatigue and Pain Overlooked in Subjects with Stable Chronic Obstructive Pulmonary Disease? Diagnostics. 2021; 11(11):2029. https://doi.org/10.3390/diagnostics11112029
Chicago/Turabian StyleNishimura, Koichi, Kazuhito Nakayasu, Mio Mori, Ryo Sanda, Ayumi Shibayama, and Masaaki Kusunose. 2021. "Are Fatigue and Pain Overlooked in Subjects with Stable Chronic Obstructive Pulmonary Disease?" Diagnostics 11, no. 11: 2029. https://doi.org/10.3390/diagnostics11112029
APA StyleNishimura, K., Nakayasu, K., Mori, M., Sanda, R., Shibayama, A., & Kusunose, M. (2021). Are Fatigue and Pain Overlooked in Subjects with Stable Chronic Obstructive Pulmonary Disease? Diagnostics, 11(11), 2029. https://doi.org/10.3390/diagnostics11112029