The Prognostic Value of Serum Soluble TREM-1 on Outcome in Adult Patients with Sepsis

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Clinical Protocol
2.3. Collection and Processing of Basic Laboratory Tests
2.4. Assay for the sTREM-1 and Biomarkers for Endothelial Dysfunction
2.5. Outcome Analysis
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Patients and Healthy Control
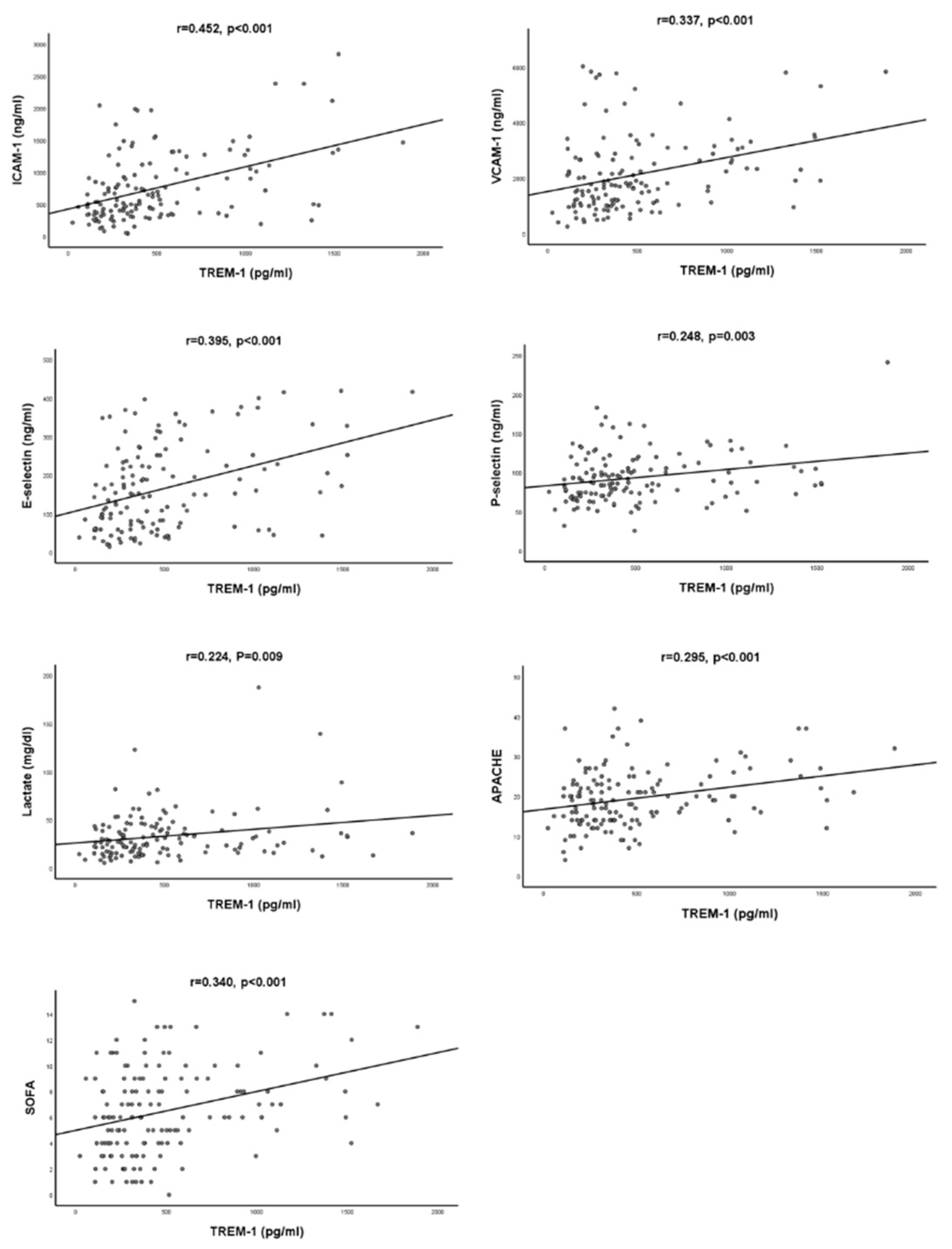
3.2. Correlation Analysis between sTREM-1 and Biomarkers for Endothelial Dysfunction, and Clinical Severity Index
3.3. Comparison of the Characteristics between Survivors and Non-Survivors
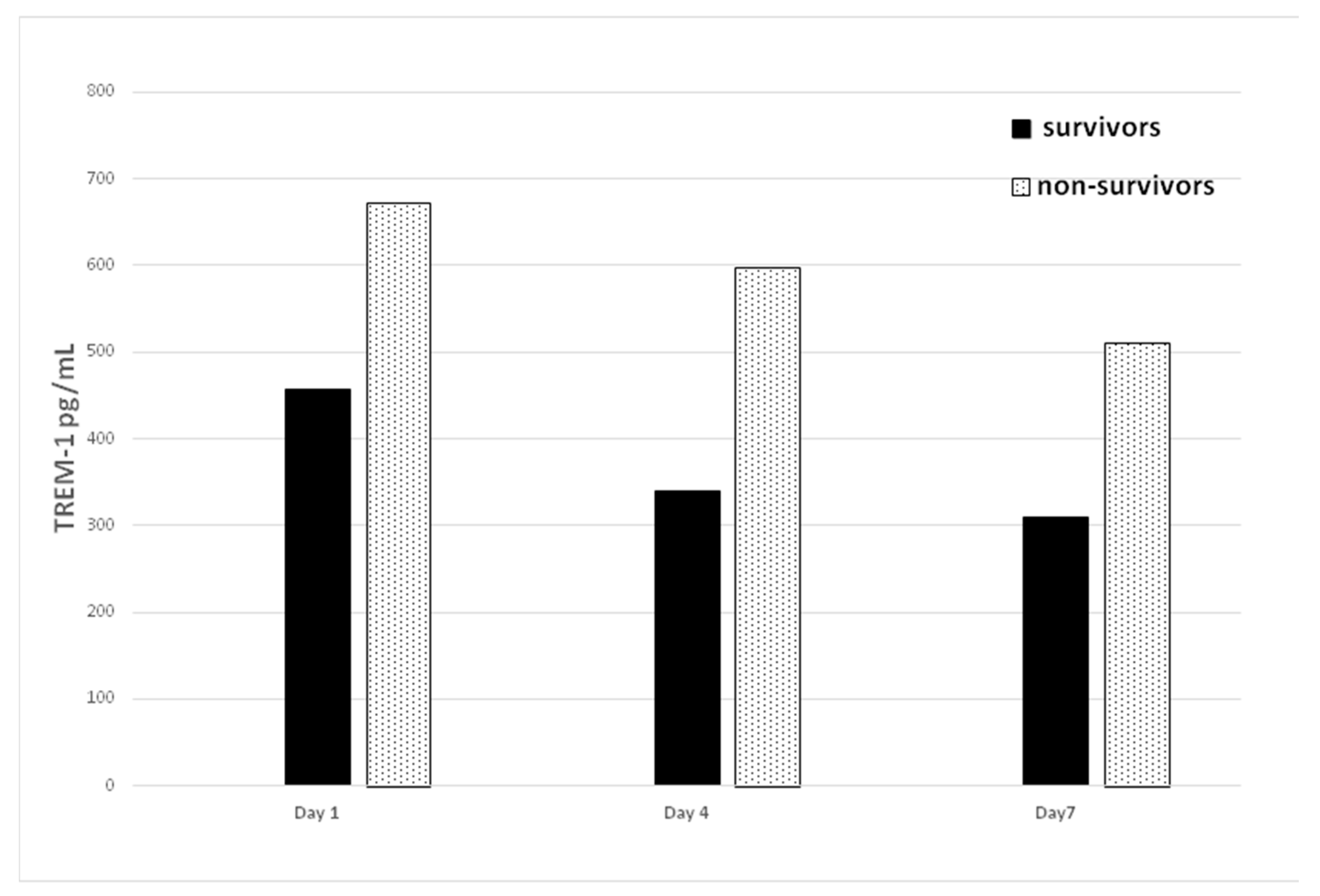
3.4. Serial Changes of Serum sTREM-1 Level between Survivor and Non-Survivors
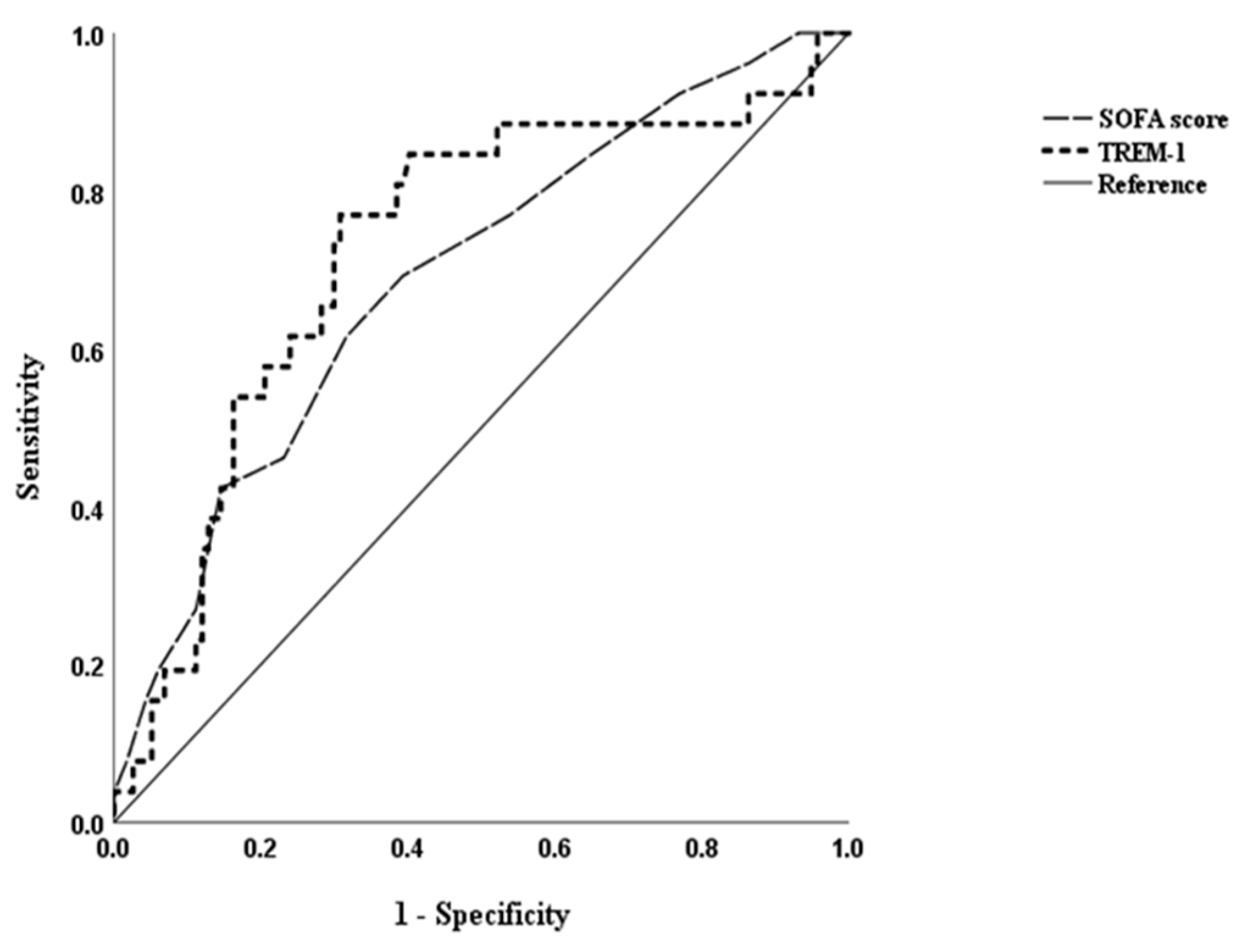
3.5. Prognostic Value of Biomarkers and Clinical Severity Scores on Outcome
3.6. Predictive Ability of sTREM-1 for Septic Shock, Organ Dysfunction, and Bacteremia
4. Discussion
4.1. Major Findings
4.2. The Role of sTREM-1 Levels on Fatality
4.3. Possible Mechanism in This Study
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Stevenson, E.K.; Rubenstein, A.R.; Radin, G.T.; Wiener, R.S.; Walkey, A.J. Two decades of mortality trends among patients with severe sepsis: A comparative meta-analysis. Crit. Care. Med. 2014, 42, 625. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Delano, M.J.; Ward, P.A. The immune system’s role in sepsis progression, resolution, and long-term outcome. Immunol. Rev. 2016, 274, 330–353. [Google Scholar] [CrossRef]
- Bouchon, A.; Facchetti, F.; Weigand, M.A.; Colonna, M. TREM-1 amplifies inflammation and is a crucial mediator of septic shock. Nature 2001, 410, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Bleharski, J.R.; Kiessler, V.; Buonsanti, C.; Sieling, P.A.; Stenger, S.; Colonna, M.; Modlin, R.L. A role for triggering receptor expressed on myeloid cells-1 in host defense during the early-induced and adaptive phases of the immune response. J. Immunol. 2003, 170, 3812–3818. [Google Scholar] [CrossRef] [PubMed]
- Colonna, M.; Facchetti, F. TREM-1 (triggering receptor expressed on myeloid cells): A new player in acute inflammatory responses. J. Infect. Dis. 2003, 187, S397–S401. [Google Scholar] [CrossRef]
- Gibot, S.; Alauzet, C.; Massin, F.; Sennoune, N.; Faure, G.C.; Béné, M.-C.; Lozniewski, A.; Bollaert, P.-E.; Lévy, B. Modulation of the triggering receptor expressed on myeloid cells–1 pathway during pneumonia in rats. J. Infect. Dis. 2006, 194, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Bouchon, A.; Dietrich, J.; Colonna, M. Cutting edge: Inflammatory responses can be triggered by TREM-1, a novel receptor expressed on neutrophils and monocytes. J. Immunol. 2000, 164, 4991–4995. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Liu, S.; Wu, S.; Zhu, Q.; Ou, G.; Liu, C.; Wang, Y.; Liao, Y.; Sun, Z. Blocking TREM-1 signaling prolongs survival of mice with Pseudomonas aeruginosa induced sepsis. Cell. Immunol. 2012, 272, 251–258. [Google Scholar] [CrossRef]
- Brenner, T.; Uhle, F.; Fleming, T.; Wieland, M.; Schmoch, T.; Schmitt, F.; Schmidt, K.; Zivkovic, A.R.; Bruckner, T.; Weigand, M. Soluble TREM-1 as a diagnostic and prognostic biomarker in patients with septic shock: An observational clinical study. Biomarkers 2017, 22, 63–69. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, F.; Fan, X.; Bao, R.; Bo, L.; Li, J.; Deng, X. Accuracy of plasma sTREM-1 for sepsis diagnosis in systemic inflammatory patients: A systematic review and meta-analysis. Crit. Care 2012, 16, R229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kofoed, K.; Andersen, O.; Kronborg, G.; Tvede, M.; Petersen, J.; Eugen-Olsen, J.; Larsen, K. Use of plasma C-reactive protein, procalcitonin, neutrophils, macrophage migration inhibitory factor, soluble urokinase-type plasminogen activator receptor, and soluble triggering receptor expressed on myeloid cells-1 in combination to diagnose infections: A prospective study. Crit. Care 2007, 11, R38. [Google Scholar]
- Gibot, S.; Cravoisy, A.; Kolopp-Sarda, M.-N.; Béné, M.-C.; Faure, G.; Bollaert, P.-E.; Levy, B. Time-course of sTREM (soluble triggering receptor expressed on myeloid cells)-1, procalcitonin, and C-reactive protein plasma concentrations during sepsis. Crit. Care Med. 2005, 33, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Kofoed, K.; Eugen-Olsen, J.; Petersen, J.; Larsen, K.; Andersen, O.; Diseases, I. Predicting mortality in patients with systemic inflammatory response syndrome: An evaluation of two prognostic models, two soluble receptors, and a macrophage migration inhibitory factor. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Jedynak, M.; Siemiatkowski, A.; Mroczko, B.; Groblewska, M.; Milewski, R.; Szmitkowski, M. Soluble TREM-1 serum level can early predict mortality of patients with sepsis, severe sepsis and septic shock. Arch. Immunol. Ther. Exp. (Warsz) 2018, 66, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Wang, H.; Liu, J.; Chen, B.; Li, G. Serum soluble triggering receptor expressed on myeloid cells-1 and procalcitonin can reflect sepsis severity and predict prognosis: A prospective cohort study. Mediators Inflamm. 2014, 2014, 641039. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Feng, L.; Song, Q.; Kang, H.; Zhang, X.; Liang, Z.; Jia, Y.; Feng, D.; Liu, C.; Xie, L. Diagnostic value of dynamics serum sCD163, sTREM-1, PCT, and CRP in differentiating sepsis, severity assessment, and prognostic prediction. Mediators Inflamm. 2013, 2013, 969875. [Google Scholar] [CrossRef] [PubMed]
- Routsi, C.; Giamarellos-Bourboulis, E.; Antonopoulou, A.; Kollias, S.; Siasiakou, S.; Koronaios, A.; Zakynthinos, S.; Armaganidis, A.; Giamarellou, H.; Roussos, C.; et al. Does soluble triggering receptor expressed on myeloid cells-1 play any role in the pathogenesis of septic shock? Clin. Exp. Immunol. 2005, 142, 62–67. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Zakynthinos, S.; Baziaka, F.; Papadomichelakis, E.; Virtzili, S.; Koutoukas, P.; Armaganidis, A.; Giamarellou, H.; Roussos, C. Soluble triggering receptor expressed on myeloid cells 1 as an anti-inflammatory mediator in sepsis. Intensive. Care Med. 2006, 32, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Latour-Pérez, J.; Alcalá-López, A.; García-García, M.; Sánchez-Hernández, J.; Abad-Terrado, C.; Viedma-Contreras, J.; Masiá-Canuto, M.; Broch-Porcar, M.; Arizo-León, D.; Gonzalez-Tejera, M. Prognostic value of the sTREM-1 plasma values in patients with sepsis: A cohort study. Med. Intensiva 2010, 34, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; She, D.; Feng, D.; Jia, Y.; Xie, L. Dynamic changes of serum soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) reflect sepsis severity and can predict prognosis: A prospective study. BMC. Infect. Dis. 2011, 11, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, S.J.; Song, Y.G.; Kim, C.O.; Kim, H.W.; Ku, N.S.; Han, S.H.; Choi, J.Y.; Kim, J.M. Measurement of plasma sTREM-1 in patients with severe sepsis receiving early goal-directed therapy and evaluation of its usefulness. Shock 2012, 37, 574–578. [Google Scholar] [CrossRef]
- Runzheimer, J.; Mewes, C.; Büttner, B.; Hinz, J.; Popov, A.-F.; Ghadimi, M.; Kristof, K.; Beissbarth, T.; Schamroth, J.; Tzvetkov, M. Lack of an Association between the Functional Polymorphism TREM-1 rs2234237 and the Clinical Course of Sepsis among Critically Ill Caucasian Patients—A Monocentric Prospective Genetic Association Study. J. Clin. Med. 2019, 8, 301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.-L.; Ramsay, G. 2001 sccm/esicm/accp/ats/sis international sepsis definitions conference. Intensive. Care Med. 2003, 29, 530–538. [Google Scholar] [CrossRef]
- Kung, C.-T.; Hsiao, S.-Y.; Tsai, T.-C.; Su, C.-M.; Chang, W.-N.; Huang, C.-R.; Wang, H.-C.; Lin, W.-C.; Chang, H.-W.; Lin, Y.-J. Plasma nuclear and mitochondrial DNA levels as predictors of outcome in severe sepsis patients in the emergency room. J. Transl. Med. 2012, 10, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, S.-Y.; Kung, C.-T.; Tsai, N.-W.; Su, C.-M.; Huang, C.-C.; Lai, Y.-R.; Wang, H.-C.; Cheng, B.-C.; Su, Y.-J.; Lin, W.-C. Concentration and value of endocan on outcome in adult patients after severe sepsis. Clin. Chim. Acta. 2018, 483, 275–280. [Google Scholar] [CrossRef]
- Palevsky, P.M.; Liu, K.D.; Brophy, P.D.; Chawla, L.S.; Parikh, C.R.; Thakar, C.V.; Tolwani, A.J.; Waikar, S.S.; Weisbord, S.D. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for acute kidney injury. Am. J. Kidney Dis. 2013, 61, 649–672. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Singh, P.; Singh, P.M.; Trikha, A.J.S. Procalcitonin levels in survivors and nonsurvivors of sepsis: Systematic review and meta-analysis. Shock 2015, 43, 212–221. [Google Scholar] [CrossRef]
- Tomasiuk, R.; Mikaszewska-Sokolewicz, M.; Szlufik, S.; Rzepecki, P.; Lazowski, T. The prognostic value of concomitant assessment of NT-proCNP, C-reactive protein, procalcitonin and inflammatory cytokines in septic patients. Crit. Care 2014, 18, 440. [Google Scholar] [CrossRef] [Green Version]
- Su, L.; Liu, D.; Chai, W.; Liu, D.; Long, Y. Role of sTREM-1 in predicting mortality of infection: A systematic review and meta-analysis. BMJ. Open 2016, 6, e010314. [Google Scholar] [CrossRef] [PubMed]
- Arguinano, A.-A.A.; Dade, S.; Stathopoulou, M.; Derive, M.; Ndiaye, N.C.; Xie, T.; Masson, C.; Gibot, S.; Visvikis-Siest, S. TREM-1 SNP rs2234246 regulates TREM-1 protein and mRNA levels and is associated with plasma levels of L-selectin. PLoS ONE 2017, 12, e0182226. [Google Scholar]
- Wong-Baeza, I.; González-Roldán, N.; Ferat-Osorio, E.; Esquivel-Callejas, N.; Aduna-Vicente, R.; Arriaga-Pizano, L.; Astudillo-de la Vega, H.; Villasis-Keever, M.; Torres-González, R.; Estrada-García, I.; et al. Triggering receptor expressed on myeloid cells (TREM-1) is regulated post-transcriptionally and its ligand is present in the sera of some septic patients. Clin. Exp. Immunol. 2006, 145, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, C.; Wagner, M.; Hermanns, I.; Klein, C.; Köhler, H.; Otto, M.; Van Kooten, T.; Bittinger, F. Physiology and cell biology of the endothelium: A dynamic interface for cell communication. Int. J. Microcirc. Clin. Exp. 1997, 17, 231–240. [Google Scholar] [CrossRef]
- Tao, F.; Peng, L.; Li, J.; Shao, Y.; Deng, L.; Yao, H. Association of serum myeloid cells of soluble triggering receptor-1 level with myocardial dysfunction in patients with severe sepsis. Mediators Inflamm. 2013, 2013, 819246. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control | Study Patients | p-Value | |
|---|---|---|---|
| n = 50 | n = 155 | ||
| Age (mean ± SD) | 56.4 ± 12.0 | 64.5 ± 13.8 | NS |
| Gender (male%) | 52.9 | 66.5 | NS |
| Underlying disease (%) | |||
| Diabetes mellitus | 33.4 | 37.4 | NS |
| Hypertension | 46.5 | 49.7 | NS |
| Coronary artery disease | 8.7 | 9.0 | NS |
| Laboratory data (mean ± SD) | |||
| White blood cell (109/L) | 5.6 ± 1.6 | 16.1 ± 10.6 | <0.001 * |
| Platelet (104/L) | 223.7 ± 61.9 | 182.3 ± 96.6 | <0.001 * |
| Hemoglobin (mg/dL) | 14.3 ± 1.9 | 11.8 ± 2.4 | <0.001 * |
| C-reactive protein (mg/L) | 1.4 ± 1.3 | 191.3 ± 117.6 | <0.001 * |
| sTREM-1 (pg/mL) | 60.4 ± 44.8 | 496.5 ± 382.3 | <0.001 * |
| sTREM-1 | ||
|---|---|---|
| r | p Value | |
| ICAM-1 | 0.452 | <0.001 * |
| VCAM-1 | 0.337 | <0.001 * |
| E-selectin | 0.395 | <0.001 * |
| P-selectin | 0.248 | 0.003 * |
| lactate | 0.224 | 0.009 * |
| APACHE | 0.295 | <0.001 * |
| SOFA | 0.340 | <0.001 * |
| Survivors (n = 126) | Non-Survivors (n = 29) | p-Value | |
|---|---|---|---|
| Age (mean ± SD) | 64.0 ± 13.9 | 67.3 ± 13.6 | NS |
| Female/Male | 44/82 | 8/21 | NS |
| Underlying disease (%) | |||
| Diabetes mellitus | 44(34.9%) | 14(48.3%) | NS |
| Hypertension | 64(50.8%) | 13(44.8%) | NS |
| Liver cirrhosis | 16(12.7%) | 6(20.7%) | NS |
| Chronic lung disease | 17(13.5%) | 4(13.8%) | NS |
| Stroke | 21(16.7%) | 6(20.7%) | NS |
| Coronary artery disease | 12(9.5%) | 2(6.9%) | NS |
| Chronic renal disease | 28(22.2%) | 8(27.6%) | NS |
| Solid tumor | 19(15.1%) | 9(31.0%) | NS |
| Clinical presentation (mean ± SD) a | |||
| Systolic blood pressure | 110.2 ± 41.8 | 108.3 ± 39.8 | NS |
| Pulse rate | 108.4 ± 24.5 | 112.8 ± 30.0 | NS |
| Shock within 24 h | 77(61.1%) | 23(79.3%) | NS |
| Respiratory failure within 24 h | 36(28.9%) | 20(69.0%) | <0.001 * |
| Disease severity index (mean ± SD) | |||
| Maximum 24 h APACHE II score | 18.5 ± 6.9 | 22.8 ± 8.3 | 0.004 * |
| Maximum 24 h SOFA score | 5.9 ± 3.2 | 8.4 ± 3.5 | <0.001 * |
| Bacteremia | 41(32.5%) | 10(34.5%) | NS |
| Steroids use | 36 (28.6%) | 11 (37.9%) | NS |
| Inotropic agents use | 42 (33.3%) | 12 (41.3%) | NS |
| Inappropiate initial antibiotics | 12 (9.5%) | 2 (6.9%) | NS |
| Laboratory data (mean ± SD) a | |||
| White blood cell count (109/L) | 15.2 ± 9.9 | 19.8 ± 12.8 | NS |
| Neutrophil (%) | 80.8 ± 14.9 | 79.2 ± 17.1 | NS |
| Hemoglobin (mg/dL) | 11.9 ± 2.2 | 11.6 ± 3.0 | NS |
| Platelet counts (104/L) | 189.7 ± 99.9 | 150.5 ± 74.5 | 0.050 |
| C-reactive protein (mg/L) | 195.5 ± 119.5 | 172.9 ± 109.1 | NS |
| Lactate (mg/dL) | 30.7 ± 23.2 | 44.6 ± 35.7 | 0.012 * |
| Creatinine (mg/dL) | 2.35 ± 2.18 | 3.03 ± 3.73 | NS |
| T-bilirubin (mg/dL) | 1.86 ± 2.40 | 2.85 ± 3.50 | NS |
| sTREM-1 (pg/mL) | 444.1 ± 348.8 | 732.4 ± 441.7 | <0.001 * |
| ICAM-1 (ng/mL) | 701.0 ± 526.8 | 1010.6 ± 638.2 | 0.020 * |
| VACM-1 (ng/mL) | 1951.7 ± 1263.7 | 2746.7 ± 1517.0 | 0.004 * |
| E-selectin (ng/mL) | 158.7 ± 110.0 | 200.0 ± 124.4 | NS |
| P-selectin (ng/mL) | 92.2 ± 28.8 | 101.0 ± 44.2 | NS |
| AUC | (95% Confidence Interval) | Cut off Point | Sensitivity | Specificity | |
|---|---|---|---|---|---|
| TREM-1 | 0.726 * | 0.613~0.838 | 384.6 pg/mL | 0.808 | 0.615 |
| ICAM-1 | 0.635 * | 0.510~0.759 | 597 ng/mL | 0.615 | 0.550 |
| VCAM-1 | 0.655 * | 0.535~0.774 | 1960 ng/mL | 0.654 | 0.631 |
| Lactate | 0.644 * | 0.535~0.752 | 2 mg/dL | 0.857 | 0.325 |
| SOFA | 0.705 * | 0.602~0.808 | 6.5 | 0.690 | 0.635 |
| APACHE | 0.658 * | 0.548~0.769 | 17.5 | 0.793 | 0.492 |
| Case Numbers (n) | TREM-1 Level | AUC | 95% Confidence Interval | |||
|---|---|---|---|---|---|---|
| Present | Absent | p Value | ||||
| Bacteremia | 51 | 613.9 ± 464.3 | 439.1 ± 332.4 | 0.023 * | 0.593 | 0.491~0.696 |
| AKI | 59 | 557.7 ± 362.7 | 460.5 ± 390.9 | NS | 0.620 * | 0.526~0.714 |
| Septic shock | 100 | 536.8 ± 401.4 | 419.2 ± 333.0 | NS | 0.587 | 0.491~0.682 |
| Respiratory failure | 56 | 552.5 ± 411.7 | 463.5 ± 362.2 | NS | 0.567 | 0.468~0.666 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kung, C.-T.; Su, C.-M.; Hsiao, S.-Y.; Chen, F.-C.; Lai, Y.-R.; Huang, C.-C.; Lu, C.-H. The Prognostic Value of Serum Soluble TREM-1 on Outcome in Adult Patients with Sepsis. Diagnostics 2021, 11, 1979. https://doi.org/10.3390/diagnostics11111979
Kung C-T, Su C-M, Hsiao S-Y, Chen F-C, Lai Y-R, Huang C-C, Lu C-H. The Prognostic Value of Serum Soluble TREM-1 on Outcome in Adult Patients with Sepsis. Diagnostics. 2021; 11(11):1979. https://doi.org/10.3390/diagnostics11111979
Chicago/Turabian StyleKung, Chia-Te, Chih-Min Su, Sheng-Yuan Hsiao, Fu-Cheng Chen, Yun-Ru Lai, Chih-Cheng Huang, and Cheng-Hsien Lu. 2021. "The Prognostic Value of Serum Soluble TREM-1 on Outcome in Adult Patients with Sepsis" Diagnostics 11, no. 11: 1979. https://doi.org/10.3390/diagnostics11111979