
Clinical Management and Outcome of Grade III Pneumonitis after Chemoradioimmunotherapy for Inoperable Stage III Non-Small Cell Lung Cancer—A Prospective Longitudinal Assessment


 , ,
, , 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
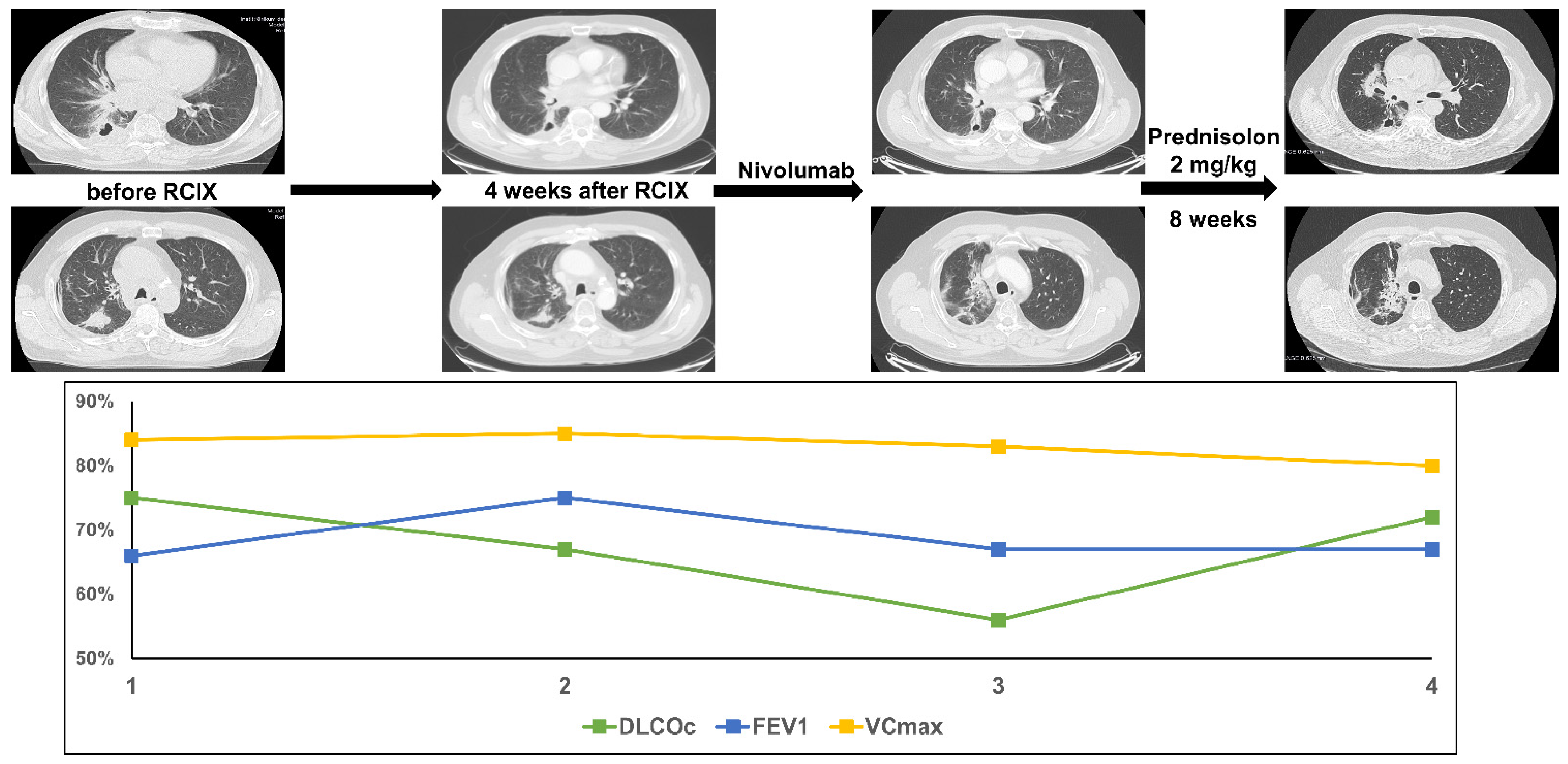
3.1. Patient 1
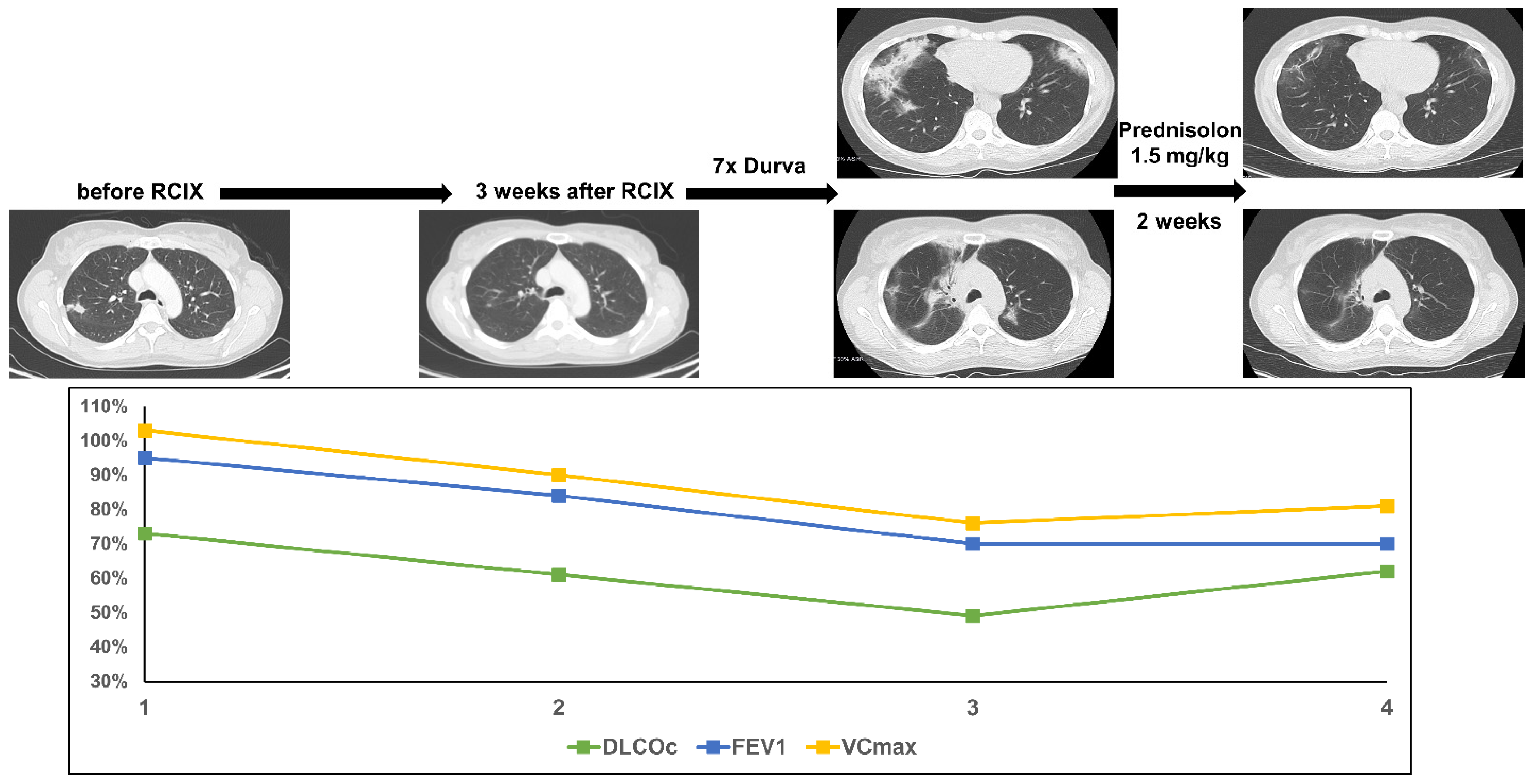
3.2. Patient 2
3.3. Patient 3
3.4. Patient 4
3.5. Patient 5
3.6. Patient 6
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Auperin, A.; Le Pechoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef]
- Naidoo, J.; Nishino, M.; Patel, S.P.; Shankar, B.; Rekhtman, N.; Illei, P.; Camus, P. Immune-Related Pneumonitis After Chemoradiotherapy and Subsequent Immune Checkpoint Blockade in Unresectable Stage III Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2020, 21, e435–e444. [Google Scholar] [CrossRef] [Green Version]
- Paz-Ares, L.; Vicente, D.; Tafreshi, A.; Robinson, A.; Soto Parra, H.; Mazieres, J.; Hermes, B.; Cicin, I.; Medgyasszay, B.; Ro-driguez-Cid, J.; et al. A Randomized, Placebo-Controlled Trial of Pembrolizumab Plus Chemotherapy in Patients With Meta-static Squamous NSCLC: Protocol-Specified Final Analysis of KEYNOTE-407. J. Thorac. Oncol. 2020, 15, 1657–1669. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Wirsdorfer, F.; de Leve, S.; Jendrossek, V. Combining Radiotherapy and Immunotherapy in Lung Cancer: Can We Expect Limitations Due to Altered Normal Tissue Toxicity? Int. J. Mol. Sci. 2018, 20, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.A.; Noh, J.M.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; Ahn, M.J.; Pyo, H.; Ahn, Y.C.; Park, K. Real world data of durvalumab consolidation after chemoradiotherapy in stage III non-small-cell lung cancer. Lung Cancer 2020, 146, 23–29. [Google Scholar] [CrossRef]
- Faehling, M.; Schumann, C.; Christopoulos, P.; Hoffknecht, P.; Alt, J.; Horn, M.; Eisenmann, S.; Schlenska-Lange, A.; Schutt, P.; Steger, F.; et al. Durvalumab after definitive chemoradiotherapy in locally advanced unresectable non-small cell lung cancer (NSCLC): Real-world data on survival and safety from the German expanded-access program (EAP). Lung Cancer 2020, 150, 114–122. [Google Scholar] [CrossRef]
- Taugner, J.; Kasmann, L.; Eze, C.; Ruhle, A.; Tufman, A.; Reinmuth, N.; Duell, T.; Belka, C.; Manapov, F. Real-world pro-spective analysis of treatment patterns in durvalumab maintenance after chemoradiotherapy in unresectable, locally advanced NSCLC patients. Investig. New Drugs 2021, 39, 1189–1196. [Google Scholar] [CrossRef]
- Taugner, J.; Kasmann, L.; Eze, C.; Tufman, A.; Reinmuth, N.; Duell, T.; Belka, C.; Manapov, F. Durvalumab after Chemora-diotherapy for PD-L1 Expressing Inoperable Stage III NSCLC Leads to Significant Improvement of Local-Regional Control and Overall Survival in the Real-World Setting. Cancers 2021, 13, 1613. [Google Scholar] [CrossRef]
- Bozorgmehr, F.; Chung, I.; Christopoulos, P.; Krisam, J.; Schneider, M.A.; Bruckner, L.; Mueller, D.W.; Thomas, M.; Rieken, S. Thoracic radiotherapy plus Durvalumab in elderly and/or frail NSCLC stage III patients unfit for chemotherapy—Employing optimized (hypofractionated) radiotherapy to foster durvalumab efficacy: Study protocol of the TRADE-hypo trial. BMC Cancer 2020, 20, 806. [Google Scholar] [CrossRef]
- Bozorgmehr, F.; Hommertgen, A.; Krisam, J.; Lasitschka, F.; Kuon, J.; Maenz, M.; Huber, P.E.; Konig, L.; Kieser, M.; Debus, J.; et al. Fostering efficacy of anti-PD-1-treatment: Nivolumab plus radiotherapy in advanced non-small cell lung cancer—Study protocol of the FORCE trial. BMC Cancer 2019, 19, 1074. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Felip, E.; Dafni, U.; Belka, C.; Guckenberger, M.; Irigoyen, A.; Nadal, E.; Becker, A.; Vees, H.; Pless, M.; et al. Safety evaluation of nivolumab added concurrently to radiotherapy in a standard first line chemo-radiotherapy regimen in stage III non-small cell lung cancer-The ETOP NICOLAS trial. Lung Cancer 2019, 133, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.H.; Lin, Y.; Yao, L.; Kalhor, N.; Carter, B.W.; Altan, M.; Blumenschein, G.; Byers, L.A.; Fossella, F.; Gibbons, D.L.; et al. Phase II Trial of Concurrent Atezolizumab With Chemoradiation for Unresectable NSCLC. J. Thorac. Oncol. 2020, 15, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Kasmann, L.; Dietrich, A.; Staab-Weijnitz, C.A.; Manapov, F.; Behr, J.; Rimner, A.; Jeremic, B.; Senan, S.; De Ruysscher, D.; Lauber, K.; et al. Radiation-induced lung toxicity—Cellular and molecular mechanisms of pathogenesis, management, and literature review. Radiat. Oncol. 2020, 15, 214. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef]
- Nishino, M.; Ramaiya, N.H.; Awad, M.M.; Sholl, L.M.; Maattala, J.A.; Taibi, M.; Hatabu, H.; Ott, P.A.; Armand, P.F.; Hodi, F.S. PD-1 Inhibitor-Related Pneumonitis in Advanced Cancer Patients: Radiographic Patterns and Clinical Course. Clin. Cancer Res. 2016, 22, 6051–6060. [Google Scholar] [CrossRef] [Green Version]
- Khunger, M.; Rakshit, S.; Pasupuleti, V.; Hernandez, A.V.; Mazzone, P.; Stevenson, J.; Pennell, N.A.; Velcheti, V. Incidence of Pneumonitis with Use of Programmed Death 1 and Programmed Death-Ligand 1 Inhibitors in Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Trials. Chest 2017, 152, 271–281. [Google Scholar] [CrossRef] [Green Version]
- Voong, K.R.; Naidoo, J. Radiation pneumonitis after definitive chemoradiation and durvalumab for non-small cell lung cancer. Lung Cancer 2020, 150, 249–251. [Google Scholar] [CrossRef]
- Melosky, B.; Juergens, R.; McLeod, D.; Leighl, N.; Brade, A.; Card, P.B.; Chu, Q. Immune checkpoint-inhibitors and chemora-diation in stage III unresectable non-small cell lung cancer. Lung Cancer 2019, 134, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Miura, Y.; Mouri, A.; Kaira, K.; Yamaguchi, O.; Shiono, A.; Hashimoto, K.; Nishihara, F.; Shinomiya, S.; Akagami, T.; Mu-rayama, Y.; et al. Chemoradiotherapy followed by durvalumab in patients with unresectable advanced non-small cell lung cancer: Management of adverse events. Thorac. Cancer 2020, 11, 1280–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaverdian, N.; Thor, M.; Shepherd, A.F.; Offin, M.D.; Jackson, A.; Wu, A.J.; Gelblum, D.Y.; Yorke, E.D.; Simone, C.B., 2nd; Chaft, J.E.; et al. Radiation pneumonitis in lung cancer patients treated with chemoradiation plus durvalumab. Cancer Med. 2020, 9, 4622–4631. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Chambers, E.S.; Chong, C.R.; Ramaiya, N.H.; Gray, S.W.; Marcoux, J.P.; Hatabu, H.; Janne, P.A.; Hodi, F.S.; Awad, M.M. Anti-PD-1 Inhibitor-Related Pneumonitis in Non-Small Cell Lung Cancer. Cancer Immunol. Res. 2016, 4, 289–293. [Google Scholar] [CrossRef] [Green Version]
- Morimoto, M.; Nishino, K.; Wada, K.; Imamura, F.; Konishi, K.; Kuhara, H.; Tamiya, M.; Inoue, T.; Kunimasa, K.; Kimura, M.; et al. Elective Nodal Irradiation for Non-small Cell Lung Cancer Complicated with Chronic Obstructive Pulmonary Disease Affects Immunotherapy Alphafter Definitive Chemoradiotherapy. Anticancer Res. 2020, 40, 6957–6970. [Google Scholar] [CrossRef] [PubMed]
- Hassanzadeh, C.; Sita, T.; Savoor, R.; Samson, P.P.; Bradley, J.; Gentile, M.; Roach, M.; Mohindra, N.; Waqar, S.; Kruser, T.J.; et al. Implications of pneumonitis after chemoradiation and durvalumab for locally advanced non-small cell lung cancer. J. Thorac. Dis. 2020, 12, 6690–6700. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | |
|---|---|---|---|---|---|---|
| Gender | female | male | female | male | male | male |
| Age at diagnosis | 47 | 51 | 72 | 70 | 58 | 49 |
| Histology | Adenocarcinoma | Squamous cell carcinoma | Adenocarcinoma | Squamous cell carcinoma | Squamous cell carcinoma | Squamous cell carcinoma |
| PD-L1 | 80% | 10% | ≥1% | 60% | 0% | ≥1% |
| Tumor stage | cT3 cN3 cM0 (UICC IIIC) | cT3 cN2 cM0 (UICC IIIB) | cT4 pN2 cM0 (UICC IIIB) | Initial pT2a N0 M0 N3-relaps, (UICC IIIB) | cT4 cN3 cM0 (UICC IIIC) | cT4 cN3 cM0 (UICC IIIC) |
| ECOG staus at diagnosis | 0 | 1 | 1 | 2 | 0 | 0 |
| Smoking status | Former (20 py) | Former (30 py) | Former (30 py) | Former (50 py) | Former (27 py) | Active (35 py) |
| Irradiation protocol |
|
|
|
|
|
|
| Systemic treatment |
|
|
|
|
|
|
| Relapse or death after treatment | No | yes | no | Yes | yes | No |
| DFS (months) | 31.1 | 15.6 | 16.3 | 11.2 | 28.7 | 27.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kauffmann-Guerrero, D.; Taugner, J.; Eze, C.; Käsmann, L.; Li, M.; Tufman, A.; Manapov, F. Clinical Management and Outcome of Grade III Pneumonitis after Chemoradioimmunotherapy for Inoperable Stage III Non-Small Cell Lung Cancer—A Prospective Longitudinal Assessment. Diagnostics 2021, 11, 1968. https://doi.org/10.3390/diagnostics11111968
Kauffmann-Guerrero D, Taugner J, Eze C, Käsmann L, Li M, Tufman A, Manapov F. Clinical Management and Outcome of Grade III Pneumonitis after Chemoradioimmunotherapy for Inoperable Stage III Non-Small Cell Lung Cancer—A Prospective Longitudinal Assessment. Diagnostics. 2021; 11(11):1968. https://doi.org/10.3390/diagnostics11111968
Chicago/Turabian StyleKauffmann-Guerrero, Diego, Julian Taugner, Chukwuka Eze, Lukas Käsmann, Minglun Li, Amanda Tufman, and Farkhad Manapov. 2021. "Clinical Management and Outcome of Grade III Pneumonitis after Chemoradioimmunotherapy for Inoperable Stage III Non-Small Cell Lung Cancer—A Prospective Longitudinal Assessment" Diagnostics 11, no. 11: 1968. https://doi.org/10.3390/diagnostics11111968
APA StyleKauffmann-Guerrero, D., Taugner, J., Eze, C., Käsmann, L., Li, M., Tufman, A., & Manapov, F. (2021). Clinical Management and Outcome of Grade III Pneumonitis after Chemoradioimmunotherapy for Inoperable Stage III Non-Small Cell Lung Cancer—A Prospective Longitudinal Assessment. Diagnostics, 11(11), 1968. https://doi.org/10.3390/diagnostics11111968