
Platelet Activation and Inflammation in Patients with Papillary Thyroid Cancer

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
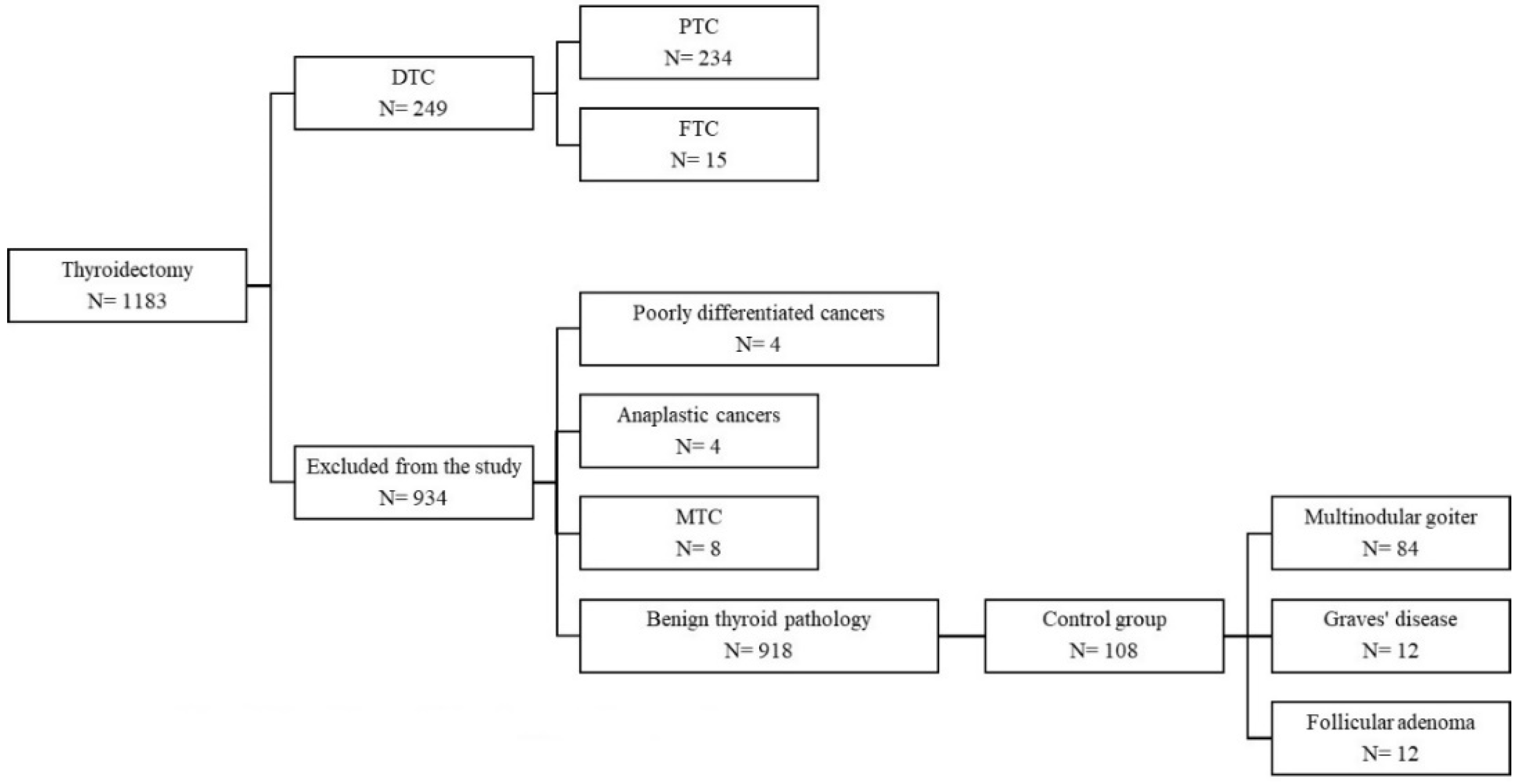
2.1. Patients and Study Protocol
2.2. Data Presentation and Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pellegriti, G.; Frasca, F.; Regalbuto, C.; Squatrito, S.; Vigneri, R. Worldwide increasing incidence of thyroid cancer: Update on epidemiology and risk factors. J. Cancer Epidemiol. 2013, 2013, 965212. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Mele, C.; Sama, M.T.; Zavattaro, M.; Caputo, M.; De Marchi, L.; Paggi, S.; Prodam, F.; Aimaretti, G.; Marzullo, P. Thyroid cancer phenotypes in relation to inflammation and autoimmunity. Front. Biosci. 2018, 23, 2267–2282. [Google Scholar] [CrossRef]
- Liotti, F.; Visciano, C.; Melillo, R.M. Inflammation in thyroid oncogenesis. Am. J. Cancer Res. 2012, 2, 286–297. [Google Scholar] [PubMed]
- Gonda, T.A.; Tu, S.; Wang, T.C. Chronic inflammation, the tumor microenvironment and carcinogenesis. Cell Cycle 2009, 8, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- Coussens, L.M.; Werb, Z. Inflammation and Cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Vakkila, J.; Lotze, M.T. Inflammation and necrosis promote tumour growth. Nat. Rev. Immunol. 2004, 4, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Takahashi, H.; Lin, W.W.; Descargues, P.; Grivennikov, S.; Kim, Y.; Luo, J.L.; Karin, M. Carcinoma-produced factors activate myeloid cells through TLR2 to stimulate metastasis. Nature 2009, 457, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, Z.; Xu, R. Human Cancer and Platelet Interaction, a Potential Therapeutic Target. Int. J. Mol. Sci. 2018, 19, 1246. [Google Scholar] [CrossRef]
- Xia, W.; Chen, W.; Tu, J.; Ni, C.; Meng, K. Prognostic Value and Clinicopathologic Features of Platelet Distribution Width in Cancer: A Meta-Analysis. Med. Sci. Monit. 2018, 24, 7130–7136. [Google Scholar] [CrossRef] [PubMed]
- Seretis, C.; Gourgiotis, S.; Gemenetzis, G.; Seretis, F.; Lagoudianakis, E.; Dimitrakopoulos, G. The significance of neutrophil/ lymphocyte ratio as a possible marker of underlying papillary microcarcinomas in thyroidal goiters: A pilot study. Am. J. Surg. 2013, 205, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Yang, S.; Yang, X.; Guo, F. Blood preoperative neutrophil-to-lymphocyte ratio is correlated with TNM stage in patients with papillary thyroid cancer. Clinics 2016, 71, 311–314. [Google Scholar] [CrossRef]
- Offi, C.; Romano, R.M.; Cangiano, A.; Candela, G.; Docimo, G. Clinical significance of neutrophil-to-lymphocyte ratio, lymphocyte-to-monocyte ratio, platelet-to-lymphocyte ratio and prognostic nutritional index in low-risk differentiated thyroid carcinoma. Acta Otorhinolaryngol. Ital. 2021, 41, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Cheong, T.Y.; Hong, S.D.; Jung, K.W.; So, Y.K. The diagnostic predictive value of neutrophil-to-lymphocyte ratio in thyroid cancer adjusted for tumor size. PLoS ONE 2021, 16, e0251446. [Google Scholar] [CrossRef] [PubMed]
- Bayhan, Z.; Zeren, S.; Ozbay, I.; Kahraman, C.; Yaylak, F.; Tiryaki, C.; Ekici, M. Mean Platelet Volume as a Biomarker for Thyroid Carcinoma. Int. Surg. 2016, 101, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Baldane, S.; Ipekci, S.H.; Sozen, M.; Kebapcilar, L. Mean platelet volume could be a possible biomarker for papillary thyroid carcinomas. Asian Pac. J. Cancer Prev. 2015, 16, 2671–2674. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dincel, O.; Bayraktar, C. Evaluation of platelet indices as a useful marker in papillary thyroid carcinoma. Bratislavske Lekarske Listy 2017, 118, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Fu, S.; Cui, M.M.; Niu, Y.; Li, B.; Liu, Z.P.; Liu, T.; Wang, R.T. Platelet Distribution Width and Serum Albumin Levels for Discrimination of Thyroid Cancer from Benign Thyroid Nodules. Asian Pac. J. Cancer Prev. 2017, 18, 1773–1777. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Wu, P.; Li, J.; Wang, H.; Sun, J.; Chen, H. Predictive values of the selected inflammatory index in elderly patients with papillary thyroid cancer. J. Transl. Med. 2018, 16, 261. [Google Scholar] [CrossRef] [PubMed]
- Yaylaci, S.; Tosun, O.; Sahin, O.; Genc, A.B.; Aydın, E.; Demiral, G.; Karahalil, F.; Olt, S.; Ergenç, H.; Varim, C. Lack of Variation in Inflammatory Hematological Parameters between Benign Nodular Goiter and Papillary Thyroid Cancer. Asian Pac. J. Cancer Prev. 2016, 17, 2321–2323. [Google Scholar] [CrossRef] [PubMed]
- Machairas, N.; Kostakis, I.D.; Prodromidou, A.; Stamopoulos, P.; Feretis, T.; Garoufalia, Z.; Damaskos, C.; Tsourouflis, G.; Kouraklis, G. Trends in white blood cell and platelet indices in a comparison of patients with papillary thyroid carcinoma and multinodular goiter do not permit differentiation between the conditions. Endocr. Res. 2017, 42, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Manatakis, D.K.; Tseleni-Balafouta, S.; Tzelves, L.; Balalis, D.; Tzortzopoulou, A.; Korkolis, D.P.; Sakorafas, G.H.; Gontikakis, E.; Plataniotis, G. Diagnostic Accuracy of Preoperative Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in Detecting Occult Papillary Thyroid Microcarcinomas in Benign Multinodular Goitres. J. Thyroid Res. 2018, 2018, 3470429. [Google Scholar] [CrossRef] [PubMed]
- Nikiforov, Y.E.; Seethala, R.R.; Tallini, G.; Baloch, Z.W.; Basolo, F.; Thompson, L.D.; Barletta, J.A.; Wenig, B.M.; Al Ghuzlan, A.; Kakudo, K.; et al. Nomenclature Revision for Encapsulated Follicular Variant of Papillary Thyroid Carcinoma: A Paradigm Shift to Reduce Overtreatment of Indolent Tumors. JAMA Oncol. 2016, 2, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, M.; Morris, L.F.; Haugen, B.; Shah, J.; Sosa, J.A.; Rohren, E.; Subramaniam, R.M.; Hunt, J.L.; Perrier, N.D. Thyroid-differentiated and anaplastic carcinoma. In AJCC Cancer Staging Manual, 8th ed.; Amin, M.B., Edge, S.B., Greene, F., Byrd, D., Brookland, R.K., Washington, M.K., Gershenwald, J.E., Compton, C.C., Hess, K.R., Sullivan, D.C., et al., Eds.; Springer International Publishing: New York, NY, USA, 2017; pp. 873–901. ISBN 9783319406176. [Google Scholar]
- Palacios-Acedo, A.L.; Mège, D.; Crescence, L.; Dignat-George, F.; Dubois, C.; Panicot-Dubois, L. Platelets, Thrombo-Inflammation, and Cancer: Collaborating with the Enemy. Front. Immunol. 2019, 10, 1805. [Google Scholar] [CrossRef] [PubMed]
- Schafer, A.I. Thrombocytosis. N. Engl. J. Med. 2004, 350, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Mizrak, S.; Kucuk, S. Platelet levels and neutrophil to lymphocyte ratio in thyroid nodules with and without cancer diagnosis. Medicine 2020, 9, 16–20. [Google Scholar] [CrossRef]
- Jianyong, L.; Zhihui, L.; Rixiang, G.; Jingqiang, Z. Using a nomogram based on preoperative serum fibrinogen levels to predict recurrence of papillary thyroid carcinoma. BMC Cancer 2018, 18, 390. [Google Scholar] [CrossRef] [PubMed]
- Ozmen, H.K.; Askin, S.; Simsek, E.; Carlioglu, A.; Arikan, Ș.; Utlu, M. Mean Platelet Volume and Red Cell Distribution Width in Differentiated Thyroid Cancer Patients. Open Med. J. 2019, 6, 94–100. [Google Scholar] [CrossRef]
- Yu, Y.J.; Li, N.; Yun, Z.Y.; Niu, Y.; Xu, J.J.; Liu, Z.P.; Liu, T.; Wang, R.T.; Yu, K.J. Preoperative mean platelet volume and platelet distribution associated with thyroid cancer. Neoplasma 2017, 64, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.K.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [PubMed]
- Kocer, D.; Karakukcu, C.; Karaman, H.; Gokay, F.; Bayram, F. May the Neutrophil/Lymphocyte Ratio Be a Predictor in the Differentiation of Different Thyroid Disorders? Asian Pac. J. Cancer Prev. 2015, 16, 3875–3879. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, Y.; Kumanlıoğlu, K.; Oral, A.; Ertan, Y.; Özcan, Z. The Correlation of Clinicopathological Findings and Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in Papillary Thyroid Carcinoma. Mol. Imaging Radionucl. Ther. 2019, 28, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Chae, I.H.; Kim, E.K.; Moon, H.J.; Yoon, J.H.; Park, V.Y.; Lee, H.S.; Moon, J.; Kwak, J.Y. Preoperative High Neutrophil-Lymphocyte Ratio May Be Associated with Lateral Lymph Node Metastasis in Patients with Papillary Thyroid Cancers. Int. J. Thyroid. 2018, 11, 41–48. [Google Scholar] [CrossRef]
- Feng, J.; Wang, Y.; Shan, G.; Gao, L. Clinical and prognostic value of neutrophil-lymphocyte ratio for patients with thyroid cancer: A meta-analysis. Medicine 2020, 99, e19686. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Kim, E.H.; Kim, B.H.; Kim, J.H.; Park, S.B.; Nam, Y.J.; Ahn, K.H.; Oh, M.Y.; Kim, W.J.; Jeon, Y.K.; et al. Association of the Preoperative Neutrophil-to-Lymphocyte Count Ratio and Platelet-to-Lymphocyte Count Ratio with Clinicopathological Characteristics in Patients with Papillary Thyroid Cancer. Endocrinol. Metab. 2015, 30, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Wakatsuki, K.; Matsumoto, S.; Migita, K.; Ito, M.; Kunishige, T.; Nakade, H.; Nakatani, M.; Kitano, M.; Sho, M. Preoperative Plasma Fibrinogen is Associated with Lymph Node Metastasis and Predicts Prognosis in Resectable Esophageal Cancer. World J. Surg. 2017, 41, 2068–2077. [Google Scholar] [CrossRef] [PubMed]
- Palaj, J.; Kečkéš, Š.; Marek, V.; Dyttert, D.; Waczulíková, I.; Durdík, Š. Fibrinogen Levels Are Associated with Lymph Node Involvement and Overall Survival in Gastric Cancer Patients. Anticancer Res. 2018, 38, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Resende de Paiva, C.; Grønhøj, C.; Feldt-Rasmussen, U.; von Buchwald, C. Association between Hashimoto’s Thyroiditis and Thyroid Cancer in 64,628 Patients. Front. Oncol. 2017, 7, 53. [Google Scholar] [CrossRef] [PubMed]
- Korniluk, A.; Koper-Lenkiewicz, O.M.; Kamińska, J.; Kemona, H.; Dymicka-Piekarska, V. Mean Platelet Volume (MPV): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions. Mediat. Inflamm. 2019, 2019, 9213074. [Google Scholar] [CrossRef] [PubMed]
- Pujani, M.; Chauhan, V.; Singh, K.; Rastogi, S.; Agarwal, C.; Gera, K. The effect and correlation of smoking with platelet indices, neutrophil lymphocyte ratio and platelet lymphocyte ratio. Hematol. Transfus. Cell Ther. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Shilpi, K.; Potekar, R.M. A Study of Platelet Indices in Type 2 Diabetes Mellitus Patients. Indian J. Hematol. Blood Transfus. 2018, 34, 115–120. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Control Group N = 108 | PTC N = 234 | p |
|---|---|---|---|
| Age, mean ± SD (years) | 52.07 ± 12.9 | 51.54 ± 13.10 | 0.726 |
| Sex, N (%) | |||
| Female | 90 (83.3) | 198 (84.6) | 0.762 |
| BMI, mean ± SD (kg/m2) | 28.45 ± 5.79 | 28.79 ± 5.7 | 0.730 |
| TSH, median (IQR) (µIU/mL) | 0.87 (1.23) | 1.21 (1.38) | 0.032 |
| FT4, median (IQR) (ng/dL) | 1.14 (0.37) | 1.08 (0.32) | 0.515 |
| Autoimmune thyroiditis, N (%) | 96 (88.9) | 114 (48.7) | <0.001 |
| Parameter | Control Group N = 108 | DTC N = 249 | p * | PTC N = 234 | p + | FTC N= 15 | p # | p ± |
|---|---|---|---|---|---|---|---|---|
| PLT, mean ± SD (×103/mm3) | 244.62 ± 61.59 | 263.12 ± 65.64 | 0.013 | 263.82 ± 65.44 | 0.011 | 252.2 ± 70.2 | 0.661 | 0.507 |
| PCT, mean ± SD (%) | 0.26 ± 0.06 | 0.28 ± 0.06 | 0.007 | 0.28 ± 0.06 | 0.006 | 0.27 ± 0.07 | 0.444 | 0.783 |
| MPV, mean ± SD (fL) | 10.68 ± 0.84 | 10.7 ± 1.02 | 0.821 | 10.7 ± 1.03 | 0.846 | 10.75 ± 0.83 | 0.762 | 0.855 |
| PDW, median (IQR) (%) | 12.4 (2.8) | 12.4 (3.1) | 0.997 | 12.45 (3.1) | 0.967 | 11.9 (1.7) | 0.925 | 0.987 |
| Neutrophil count, median (IQR) (×103/mm3) | 4.05 (1.83) | 4.42 (1.89) | 0.031 | 4.44 (1.91) | 0.022 | 4.09 (1.81) | 0.920 | 0.309 |
| Lymphocyte count, median (IQR) (×103/mm3) | 1.93 (0.8) | 1.94 (0.7) | 0.992 | 1.94 (0.7) | 0.976 | 2.09 (0.66) | 0.973 | 0.987 |
| NLR, median (IQR) | 2.04 (1.11) | 2.13 (1.26) | 0.218 | 2.13 (1.27) | 0.201 | 2.07 (1.16) | 0.973 | 0.987 |
| PLR, median (IQR) | 126.07 (49.68) | 128.86 (61.42) | 0.936 | 130.58 (61.56) | 0.727 | 116.29 (55.59) | 0.285 | 0.294 |
| ESR, median (IQR) (mm/h) | 13 (11) | 13 (13) | 0.743 | 13 (12) | 0.802 | 12 (12) | 0.759 | 0.857 |
| Fibrinogen, mean ± SD (mg/dL) | 307.9 ± 68.01 | 339.61 ± 70.08 | 0.003 | 338.29 ± 70.64 | 0.005 | 357 ± 62.59 | 0.029 | 0.395 |
| Parameter | Gender | Age | ||||
|---|---|---|---|---|---|---|
| Female N = 198 | Male N = 36 | p | <55 Years N = 124 | >55 Years N = 110 | p | |
| PLT, mean ± SD (×103/mm3) | 268.84 ± 65.11 | 236.19 ± 60.95 | 0.006 | 278.96 ± 62.84 | 246.75 ± 64.37 | <0.001 |
| PCT, mean ± SD (%) | 0.29 ± 0.06 | 0.24 ± 0.05 | <0.001 | 0.29 ± 0.05 | 0.27 ± 0.06 | 0.010 |
| MPV, mean ± SD (fL) | 10.73 ± 1.01 | 10.52 ± 1.12 | 0.253 | 10.56 ± 0.94 | 10.85 ± 1.11 | 0.032 |
| PDW, median (IQR) (%) | 12.6 (3.15) | 12.2 (3.4) | 0.696 | 12.25 (2.85) | 13.1 (3.43) | 0.199 |
| Neutrophil count, median (IQR) (×103/mm3) | 4.37 (1.87) | 4.82 (2.11) | 0.040 | 4.27 (1.69) | 4.86 (2.14) | 0.068 |
| Lymphocyte count, median (IQR) (×103/mm3) | 1.96 (0.69) | 1.81 (1.05) | 0.626 | 1.98 (0.67) | 1.87 (0.74) | 0.291 |
| NLR, median (IQR) | 2.12 (1.1) | 2.81 (2.06) | 0.587 | 2.06 (1.13) | 2.43 (1.29) | 0.013 |
| PLR, median (IQR) | 131.55 (56.99) | 118.96 (93.92) | 0.587 | 135.24 (64.51) | 125.88 (62.16) | 0.238 |
| ESR, median (IQR) (mm/h) | 13 (12) | 6 (9) | 0.005 | 9 (11) | 16 (13) | 0.005 |
| Fibrinogen, mean ± SD (mg/dL) | 338.25 ± 68.94 | 338.5 ± 82.49 | 0.988 | 325.09 ± 65.05 | 352.43 ± 74.05 | 0.019 |
| Parameter | Vascular Invasion | Capsular Invasion | Extracapsular Extension | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Present N = 30 | Absent N = 204 | p | Present N = 75 | Absent N = 159 | p | Present N = 49 | Absent N = 185 | p | |
| Age—mean ± SD (years) | 53.77 ± 16.08 | 51.22 ± 12.62 | 0.411 | 53.07 ± 13.65 | 50.82 ± 12.81 | 0.222 | 54.33 ± 12.77 | 50.81 ± 13.12 | 0.094 |
| Sex N (%) | |||||||||
| Female | 23 (76.7) | 175 (85.8) | 0.275 | 61 (81.3) | 137 (86.2) | 0.339 | 38 (77.6) | 160 (86.5) | 0.123 |
| Male | 7 (23.3) | 29 (14.2) | 0.275 | 14 (18.7) | 22 (13.8) | 0.339 | 11 (22.4) | 25 (13.5) | 0.123 |
| BMI—mean ± SD (kg/m2) | 26.89 ± 5.53 | 29.16 ± 5.69 | 0.147 | 28.67 ± 5.61 | 28.86 ± 5.8 | 0.871 | 28.84 ± 5.88 | 28.77 ± 5.68 | 0.961 |
| PLT—mean ± SD (×103/mm3) | 263.8 ± 62.66 | 263.82 ± 65.99 | 0.999 | 268.75 ± 67.78 | 261.50 ± 64.39 | 0.430 | 273.9 ± 72.54 | 261.15 ± 63.37 | 0.226 |
| MPV—mean ± SD (fL) | 10.58 ± 1.08 | 10.71 ± 1.02 | 0.505 | 10.6 ± 1.1 | 10.74 ± 0.99 | 0.328 | 10.44 ± 1.03 | 10.77 ± 1.02 | 0.051 |
| PCT—mean ± SD (%) | 0.27 ± 0.05 | 0.28 ± 0.06 | 0.604 | 0.278 ± 0.059 | 0.28 ± 0.06 | 0.788 | 0.281 ± 0.07 | 0.279 ± 0.006 | 0.840 |
| PDW—median (IQR) (%) | 12.75 (2.53) | 12.45 (3.20) | 0.828 | 12.3 (3.13) | 12.7 (3.2) | 0.643 | 12 (3) | 12.7 (3.1) | 0.302 |
| Neutrophil count—median (IQR) (×103/mm3) | 4.24 (2.38) | 4.44 (1.82) | 0.884 | 4.46 (2.13) | 4.39 (1.9) | 0.928 | 4.76 (2.17) | 4.39 (1.84) | 0.478 |
| Lymphocyte count—median (IQR) (×103/mm3) | 1.78 (0.72) | 1.97 (0.70) | 0.087 | 1.84 (0.93) | 1.97 (0.65) | 0.190 | 1.85 (0.9) | 1.97 (0.67) | 0.223 |
| NLR—median (IQR) | 2.29 (2.21) | 2.13 (1.14) | 0.845 | 2.2 (1.84) | 2.11 (1.03) | 0.889 | 2.31 (1.86) | 2.13 (1.07) | 0.872 |
| PLR—median (IQR) | 159.46 (89.74) | 128.42 (54.60) | 0.328 | 131.47 (62.9) | 127.98 (61.68) | 0.889 | 142.39 (62.58) | 127.59 (62.17) | 0.335 |
| ESR—median (IQR) (mm/h) | 13 (21) | 13 (12) | 0.791 | 12.5 (15) | 13 (12) | 0.999 | 13 (17) | 12.5 (12) | 0.976 |
| Fibrinogen—mean ± SD (mg/dL) | 319.18 ± 73.35 | 341.34 ± 70.01 | 0.194 | 324.82 ± 69.79 | 344.95 ± 70.46 | 0.107 | 327.66 ± 67.71 | 341.3 ± 71.45 | 0.337 |
| Parameter | Multifocality | Lymph Node Metastases | Autoimmune Thyroiditis (HP) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Present N = 73 | Absent N = 161 | p | Present N = 37 | Absent N = 197 | p | Present N = 93 | Absent N = 141 | p | |
| Age—mean ± SD (years) | 50.26 ± 14.17 | 52.12 ± 12.56 | 0.314 | 47.3 ± 12.91 | 52.34 ± 13.01 | 0.031 | 53.6 ± 11.26 | 50.18 ± 14.06 | 0.041 |
| Sex N (%) | |||||||||
| Female | 61 (83.6) | 137 (85.1) | 0.764 | 28 (75.7) | 170 (86.3) | 0.100 | 83 (89.2) | 115 (81.6) | 0.111 |
| Male | 12 (16.4) | 24 (14.9) | 0.764 | 9 (24.3) | 27 (13.7) | 0.100 | 10 (10.8) | 26 (18.4) | 0.111 |
| BMI—mean ± SD (kg/m2) | 29.27 ± 6.58 | 28.63 ± 5.41 | 0.630 | 29.31 ± 6.99 | 28.72 ± 5.54 | 0.739 | 27.82 ± 4.99 | 29.53 ± 6.13 | 0.139 |
| PLT—mean ± SD (×103/mm3) | 261.97 ± 66.33 | 264.66 ± 65.22 | 0.772 | 270.49 ± 62.78 | 262.57 ± 66 | 0.501 | 254.47 ± 68.75 | 269.99 ± 62.65 | 0.076 |
| MPV—mean ± SD (fL) | 10.78 ± 1.1 | 10.66 ± 1 | 0.425 | 10.4 ± 1.06 | 10.75 ± 1.01 | 0.057 | 10.95 ± 0.96 | 10.53 ± 1.04 | 0.002 |
| PCT—mean ± SD (%) | 0.27 ± 0.055 | 0.28 ± 0.062 | 0.350 | 0.278 ± 0.057 | 0.28 ± 0.06 | 0.847 | 0.27 ± 0.064 | 0.28 ± 0.057 | 0.359 |
| PDW—median (IQR) (%) | 12.75 (3.55) | 12.4 (2.97) | 0.440 | 11.8 (2.9) | 12.8 (3.1) | 0.137 | 13.3 (2.9) | 12 (3.4) | 0.009 |
| Neutrophil count—median (IQR) (×103/mm3) | 4.33 (1.62) | 4.57 (2.04) | 0.186 | 4.42 (2.12) | 4.44 (1.86) | 0.955 | 4.33 (1.97) | 4.46 (1.9) | 0.669 |
| Lymphocyte count—median (IQR) (×103/mm3) | 1.97 (0.88) | 1.93 (0.68) | 0.711 | 1.84 (0.57) | 1.97 (0.72) | 0.083 | 1.96 (0.6) | 1.91 (0.74) | 0.915 |
| NLR—median (IQR) | 2.09 (1.09) | 2.16 (1.28) | 0.778 | 2.31 (1.97) | 2.13 (1.12) | 0.858 | 2.09 (1.25) | 2.21 (1.28) | 0.593 |
| PLR—median (IQR) | 130.27 (62.66) | 131.63 (62.51) | 0.888 | 142.39 (62.76) | 127.59 (64.02) | 0.282 | 125.56 (52.7) | 135.05 (64.71) | 0.182 |
| ESR—median (IQR) (mm/h) | 13 (12) | 12.5 (14) | 0.750 | 9 (9) | 13 (14) | 0.138 | 13 (14) | 12 (12) | 0.843 |
| Fibrinogen—mean ± SD (mg/dL) | 324.22 ± 63.58 | 345.46 ± 73.26 | 0.087 | 314.98 ± 68.01 | 344.11 ± 70.36 | 0.047 | 346.43 ± 68.12 | 332.7 ± 72.18 | 0.251 |
| Parameter | TNM Staging—pT Classification | |||||||
|---|---|---|---|---|---|---|---|---|
| T1 N = 128 | T2 N = 28 | T3 N = 73 | T4 N = 5 | p | T1–T2 N = 156 | T3–T4 N = 78 | p | |
| Age—mean ± SD (years) | 51.54 ± 11.95 | 44.29 ± 15.65 | 54.19 ± 12.78 | 52.2 ± 16.57 | 0.008 | 50.28 ± 13.04 | 54.06 ± 12.94 | 0.037 |
| BMI—mean ± SD (kg/m2) | 28.89 ± 5.61 | 27.59 ± 4.82 | 29.36 ± 6.13 | 24.08 ± 6.86 | 0.493 | 28.53 ± 5.34 | 29.12 ± 6.18 | 0.612 |
| PLT, mean ± SD (×103/mm3) | 256.89 ± 63.72 | 274.25 ± 65.49 | 269.04 ± 67.51 | 309.8 ± 77.62 | 0.171 | 259.9 ± 63.78 | 271.65 ± 68.38 | 0.196 |
| PCT, mean ± SD (%) | 0.279 ± 0.061 | 0.287 ± 0.063 | 0.277 ± 0.058 | 0.31 ± 0.087 | 0.744 | 0.28 ± 0.061 | 0.276 ± 0.059 | 0.849 |
| MPV, mean ± SD (fL) | 10.81 ± 0.97 | 10.6 ± 1 | 10.58 ± 1.12 | 10.02 ± 1.09 | 0.174 | 10.78 ± 0.97 | 10.54 ± 1.12 | 0.100 |
| PDW, median (IQR) (%) | 12.8 (3.1) | 12.3 (3.65) | 12.2 (3.55) | 13.4 (-) | 0.491 | 12.7 (3.1) | 12.2 (3.5) | 0.539 |
| Neutrophil count, median (IQR) (×103/mm3) | 4.48 (1.9) | 4.2 (1.78) | 4.46 (2.16) | 5.04 (3.56) | 0.319 | 4.43 (1.88) | 4.51 (2.16) | 0.817 |
| Lymphocyte count, median (IQR) (×103/mm3) | 1.97 (0.68) | 2.01 (0.72) | 1.85 (0.81) | 1.66 (1.53) | 0.683 | 1.97 (0.68) | 1.85 (0.88) | 0.248 |
| NLR, median (IQR) | 2.16 (1.05) | 1.86 (1.16) | 2.13 (1.67) | 2.98 (3.35) | 0.149 | 2.11 (1.05) | 2.17 (1.72) | 0.890 |
| PLR, median (IQR) | 125.01 (55.25) | 126.65 (85.74) | 133.83 (49.73) | 186.92 (107.21) | 0.362 | 125.82 (62.7) | 136.24 (56.35) | 0.332 |
| ESR, median (IQR) (mm/h) | 13 (13) | 11.5 (12) | 13 (18) | 7 (23) | 0.439 | 12 (12) | 13 (18) | 0.952 |
| Fibrinogen, mean ± SD (mg/dL) | 345.35 ± 70.04 | 334.67 ± 64.53 | 329.87 ± 75.52 | 308.8 ± 67.95 | 0.518 | 343.54 ± 68.5 | 327.68 ± 74.37 | 0.204 |
| Parameter | Preoperative N = 234 | Postoperative N = 63 | p |
|---|---|---|---|
| PLT, mean ± SD (×103/mm3) | 266.35 ± 60.86 | 265.14 ± 69.39 | 0.865 |
| MPV, mean ± SD (fL) | 10.57 ± 1 | 10.51 ± 1.04 | 0.382 |
| PCT, mean ± SD (%) | 0.277 ± 0.054 | 0.275 ± 0.062 | 0.841 |
| PDW, median (IQR) (%) | 12.4 (3.5) | 12.5 (2.85) | 0.963 |
| ESR, median (IQR) (mm/h) | 12 (14) | 14 (14) | 0.088 |
| Neutrophil count, median (IQR) (×103/mm3) | 4.55 (1.92) | 4.46 (2.37) | 0.672 |
| Lymphocyte count, median (IQR) (×103/mm3) | 1.85 (0.76) | 1.83 (0.71) | 0.354 |
| NLR, median (IQR) | 2.49 (1.33) | 2.27 (1.28) | 0.653 |
| PLR, median (IQR) | 138.93 (51.38) | 143.48 (78.72) | 0.536 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, S.; Mustata, T.; Enache, O.; Ion, O.; Chifulescu, A.; Sirbu, A.; Barbu, C.; Miron, A.; Giulea, C.; Andrei, F.; et al. Platelet Activation and Inflammation in Patients with Papillary Thyroid Cancer. Diagnostics 2021, 11, 1959. https://doi.org/10.3390/diagnostics11111959
Martin S, Mustata T, Enache O, Ion O, Chifulescu A, Sirbu A, Barbu C, Miron A, Giulea C, Andrei F, et al. Platelet Activation and Inflammation in Patients with Papillary Thyroid Cancer. Diagnostics. 2021; 11(11):1959. https://doi.org/10.3390/diagnostics11111959
Chicago/Turabian StyleMartin, Sorina, Theodor Mustata, Oana Enache, Oana Ion, Andreea Chifulescu, Anca Sirbu, Carmen Barbu, Adrian Miron, Cosmin Giulea, Florin Andrei, and et al. 2021. "Platelet Activation and Inflammation in Patients with Papillary Thyroid Cancer" Diagnostics 11, no. 11: 1959. https://doi.org/10.3390/diagnostics11111959
APA StyleMartin, S., Mustata, T., Enache, O., Ion, O., Chifulescu, A., Sirbu, A., Barbu, C., Miron, A., Giulea, C., Andrei, F., & Fica, S. (2021). Platelet Activation and Inflammation in Patients with Papillary Thyroid Cancer. Diagnostics, 11(11), 1959. https://doi.org/10.3390/diagnostics11111959