
Radial Basis Function for Breast Lesion Detection from MammoWave Clinical Data

 ,
,  ,
, 
 ,
, 
Abstract
:1. Introduction
- The experimentation was completed on 61 breasts, allowing the exploration of lesions with different dimensions.
- The newly collected data appear differently in the hyperplane, motivating the authors to explore a radial basis function (RBF) kernel of SVM instead of a quadratic kernel, where SVM with an RBF kernel is found to be more efficient.
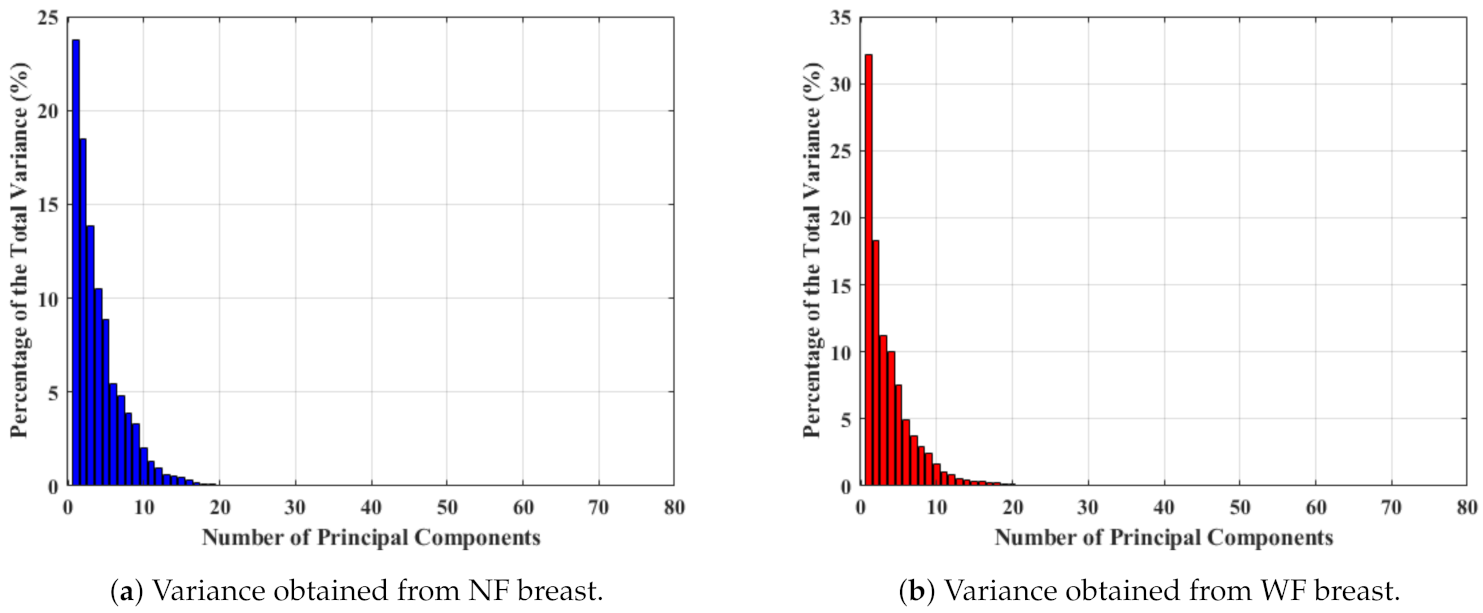
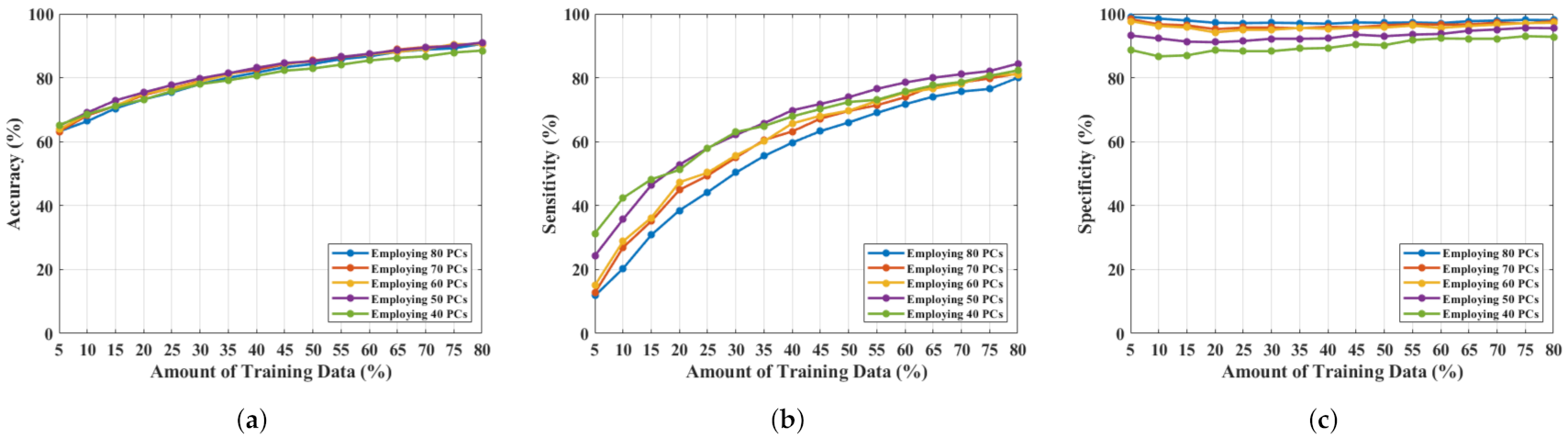
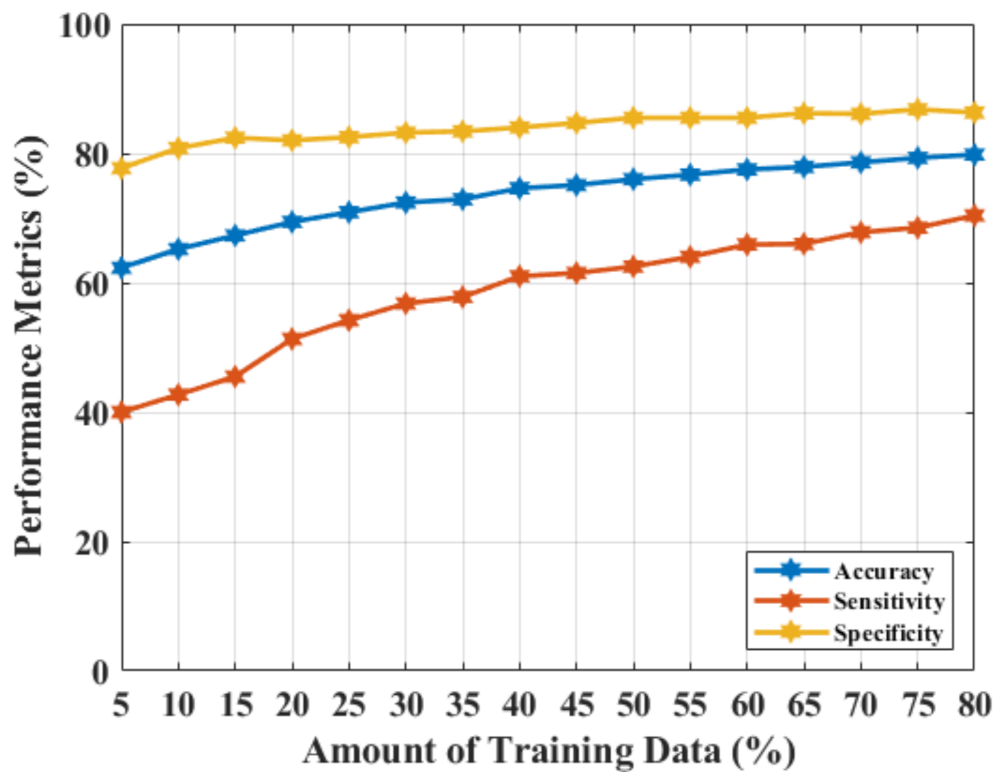
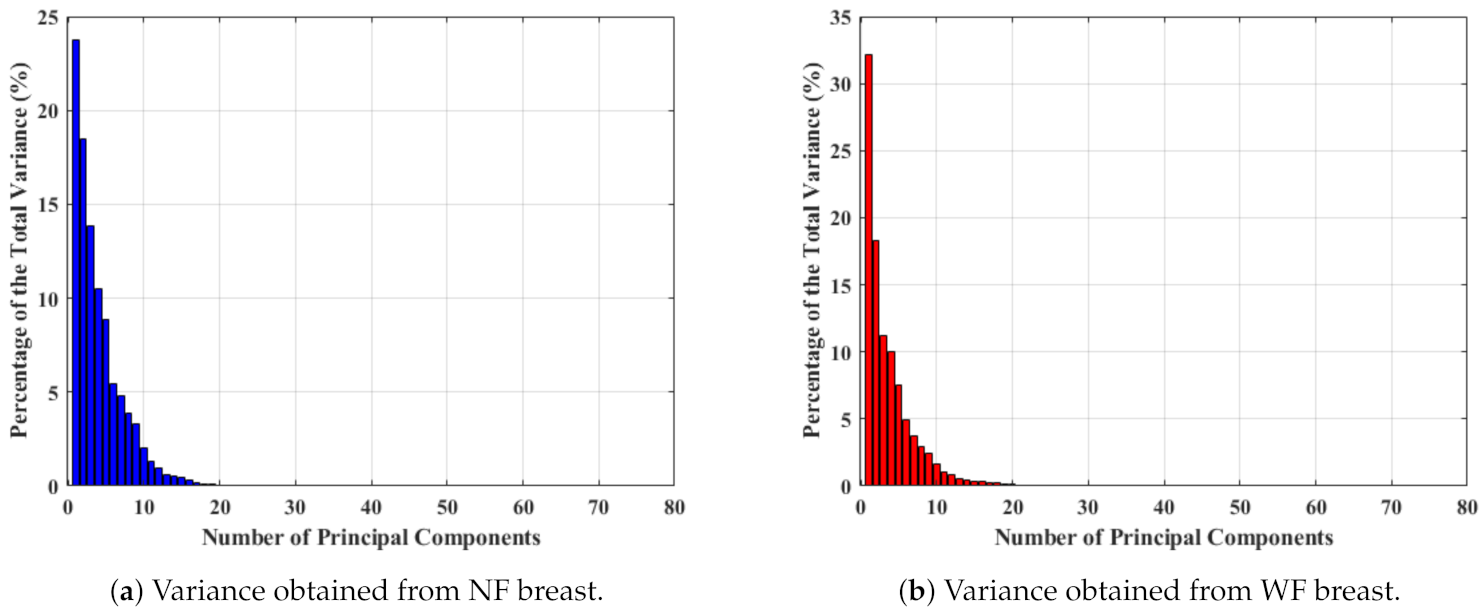
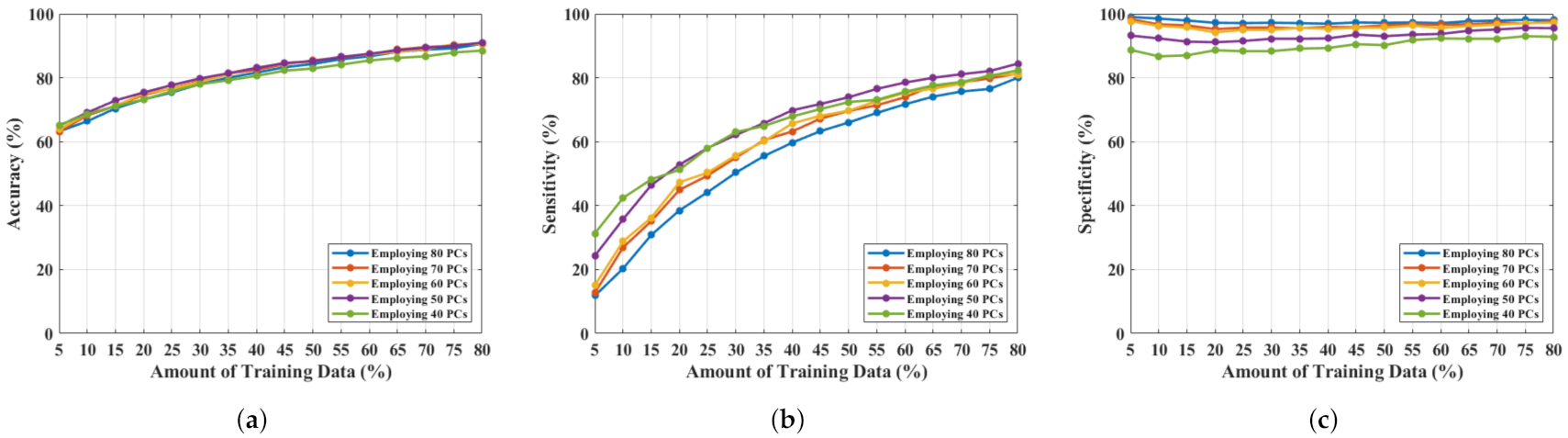
- The optimal method for using the frequency response signals was explored. The experiment shows that the 50 components obtained by applying a principal component analysis (PCA) from the real-parts of the parameters (engaging SVM with an RBF kernel) is the best possible combination to classify NF and WF signals.
- The prediction results have been analyzed by the team of researchers and radiologists through statistical measurements to understand the false positive and negative classifications, revealing that lesion size and breast density have an effect on microwave response, as well as ML predictions.
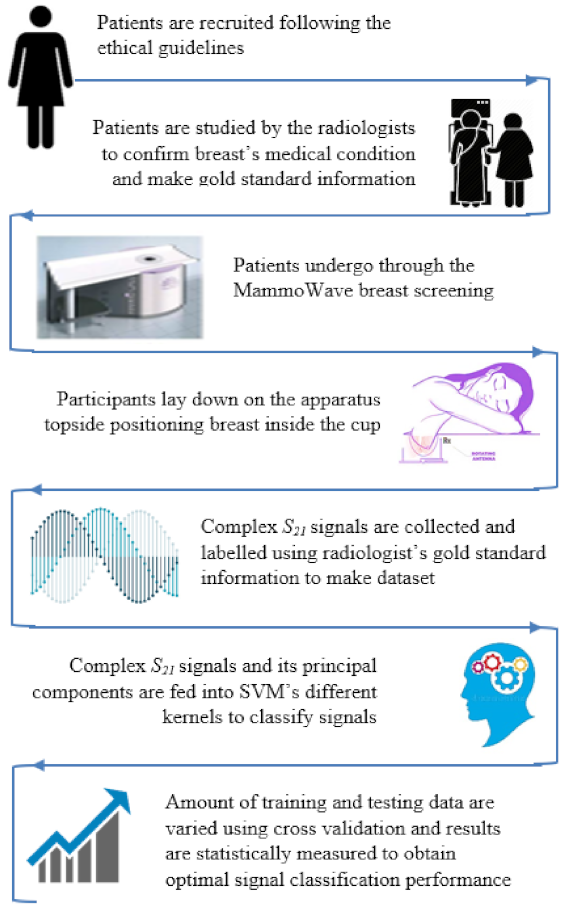
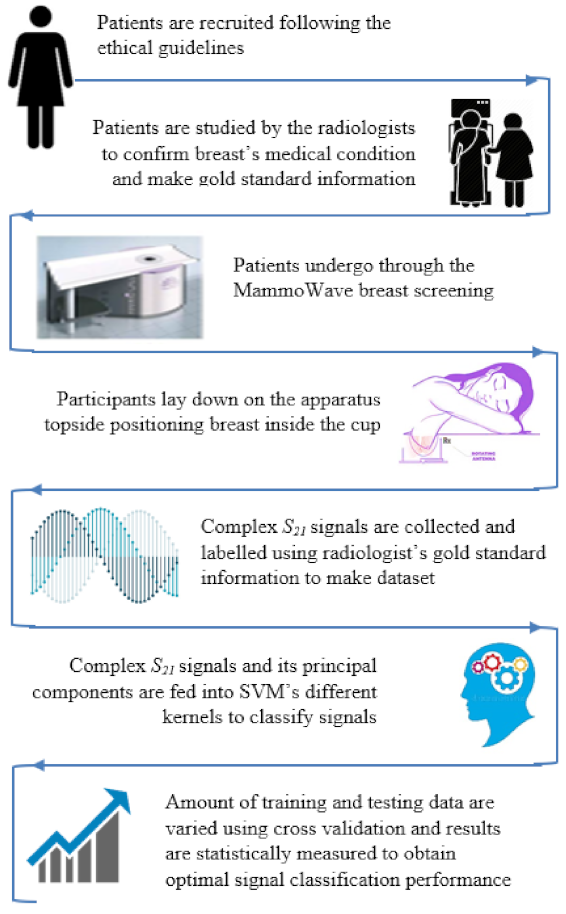
2. Methods
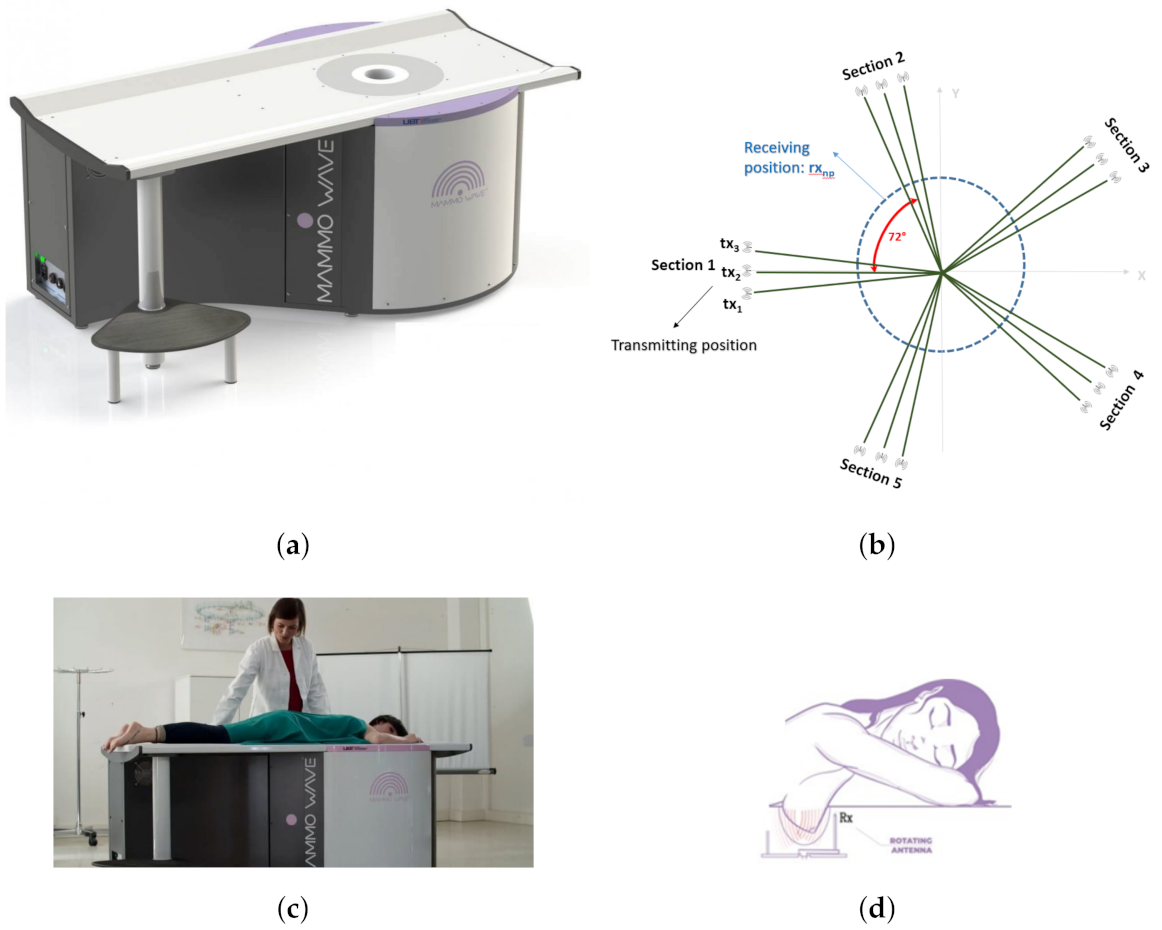
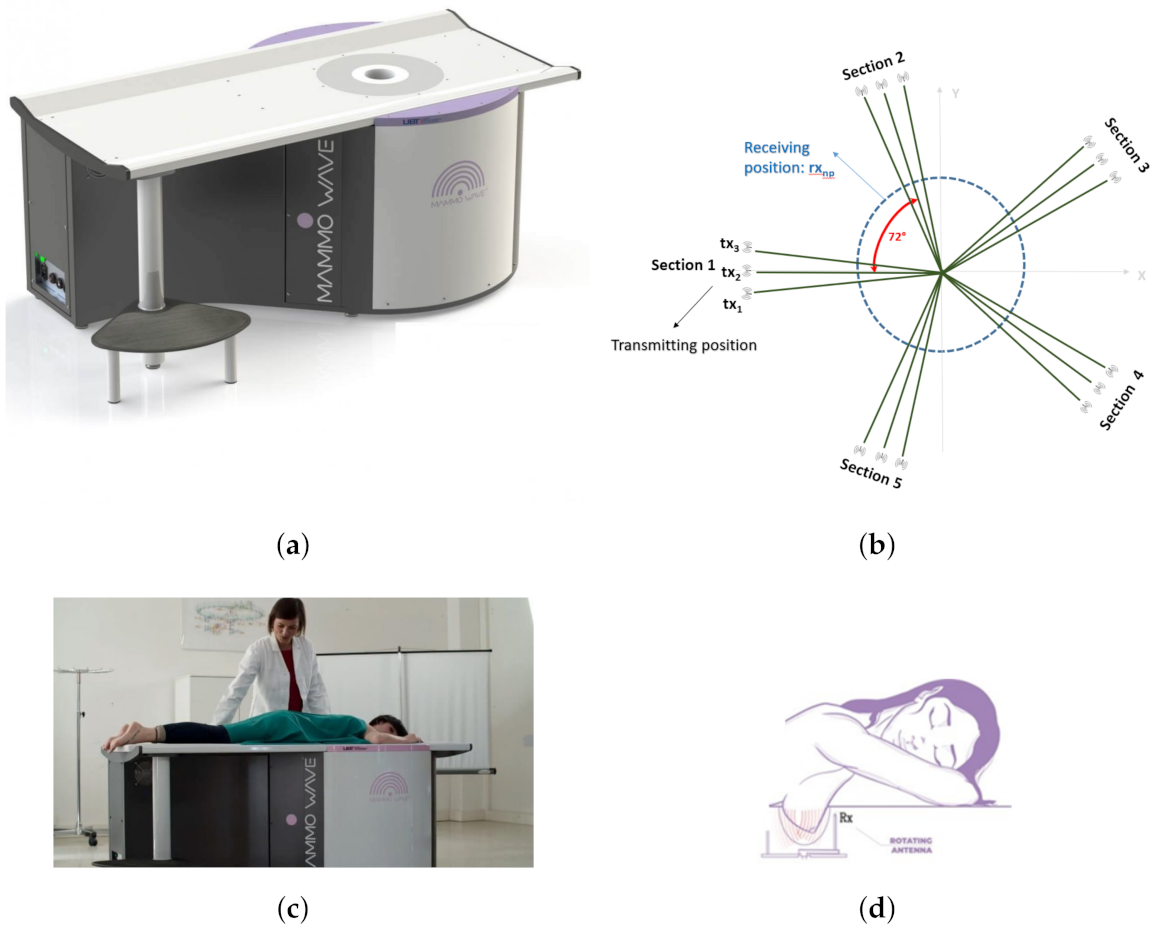
3. Device Description
4. Data Collection
5. MammoWave Signal Classification: Real-Parts of & RBF Kernel Approach
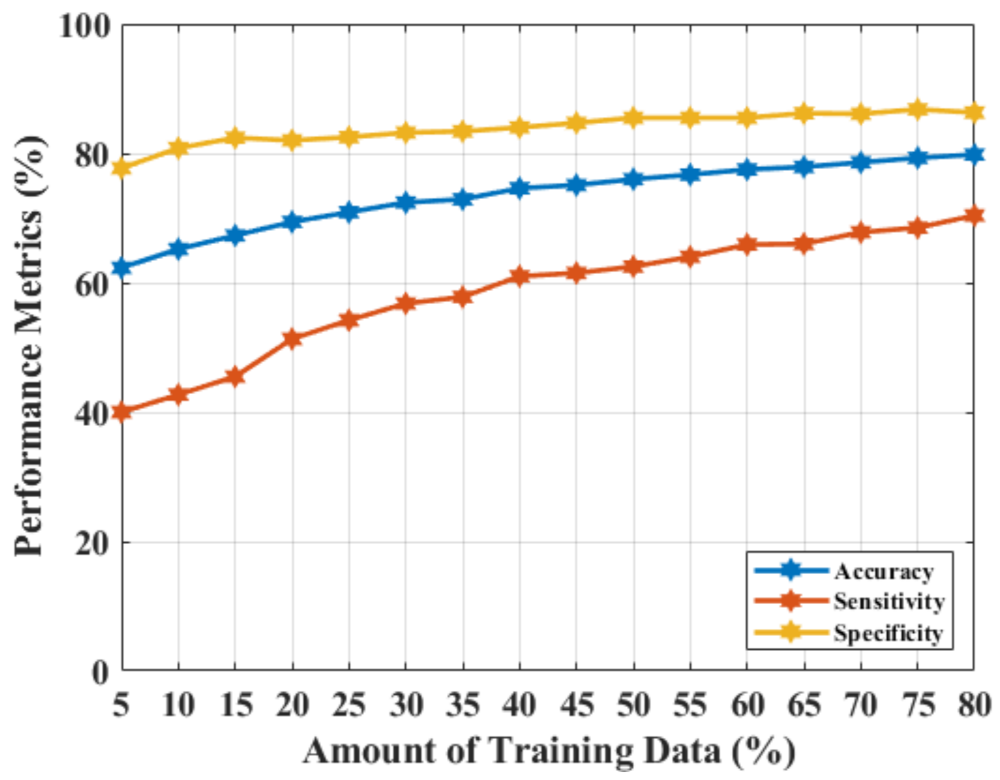
6. MammoWave Signal Classification Results: PCA on Real-Parts of & RBF Kernel Approach
7. Discussion & Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marino, M.A.; Leithner, D.; Sung, J.; Avendano, D.; Morris, E.A.; Pinker, K.; Jochelson, M.S. Radiomics for tumor characterization in breast cancer patients: A feasibility study comparing contrast-enhanced mammography and magnetic resonance imaging. Diagnostics 2020, 10, 492. [Google Scholar] [CrossRef] [PubMed]
- La Forgia, D.; Fanizzi, A.; Campobasso, F.; Bellotti, R.; Didonna, V.; Lorusso, V.; Moschetta, M.; Massafra, R.; Tamborra, P.; Tangaro, S.; et al. Radiomic analysis in contrast-enhanced spectral mammography for predicting breast cancer histological outcome. Diagnostics 2020, 10, 708. [Google Scholar] [CrossRef] [PubMed]
- Thigpen, D.; Kappler, A.; Brem, R. The role of ultrasound in screening dense breasts—A review of the literature and practical solutions for implementation. Diagnostics 2018, 8, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Source: Cancer Research UK-Breast Screening. Available online: https://www.cancerresearchuk.org/about-cancer/breast-cancer/getting-diagnosed/screening/breast-screening (accessed on 10 April 2021).
- Chen, T.H.H.; Yen, A.M.F.; Fann, J.C.Y.; Gordon, P.; Chen, S.L.S.; Chiu, S.Y.H.; Hsu, C.Y.; Chang, K.J.; Lee, W.C.; Yeoh, K.G.; et al. Clarifying the debate on population-based screening for breast cancer with mammography: A systematic review of randomized controlled trials on mammography with Bayesian meta-analysis and causal model. Medicine 2017, 96, e5684. [Google Scholar] [CrossRef]
- McGuire, A.; Brown, J.A.; Malone, C.; McLaughlin, R.; Kerin, M.J. Effects of age on the detection and management of breast cancer. Cancers 2015, 7, 908–929. [Google Scholar] [CrossRef]
- Wang, J.; Zheng, S.; Ding, L.; Liang, X.; Wang, Y.; Greuter, M.J.; de Bock, G.H.; Lu, W. Is Ultrasound an Accurate Alternative for Mammography in Breast Cancer Screening in an Asian Population? A Meta-Analysis. Diagnostics 2020, 10, 985. [Google Scholar] [CrossRef]
- Duffy, S.W.; Vulkan, D.; Cuckle, H.; Parmar, D.; Sheikh, S.; Smith, R.A.; Evans, A.; Blyuss, O.; Johns, L.; Ellis, I.O.; et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): Final results of a randomised, controlled trial. Lancet Oncol. 2020, 21, 1165–1172. [Google Scholar] [CrossRef]
- Wang, L. Early diagnosis of breast cancer. Sensors 2017, 17, 1572. [Google Scholar] [CrossRef]
- Wörtge, D.; Moll, J.; Krozer, V.; Bazrafshan, B.; Hübner, F.; Park, C.; Vogl, T.J. Comparison of X-ray-mammography and planar UWB microwave imaging of the breast: First results from a patient study. Diagnostics 2018, 8, 54. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, B.L.; Godinho, D.; O’Halloran, M.; Glavin, M.; Jones, E.; Conceição, R.C. Diagnosing Breast Cancer with Microwave Technology: Remaining challenges and potential solutions with machine learning. Diagnostics 2018, 8, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conceição, R.C.; Mohr, J.J.; O’Halloran, M. An Introduction to Microwave Imaging for Breast Cancer Detection; Springer: Basel, Switzerland, 2016. [Google Scholar]
- Nikolova, N.K. Microwave imaging for breast cancer. IEEE Microw. Mag. 2011, 12, 78–94. [Google Scholar] [CrossRef]
- Lazebnik, M.; McCartney, L.; Popovic, D.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Magliocco, A.; Booske, J.H.; Okoniewski, M.; et al. A large-scale study of the ultrawideband microwave dielectric properties of normal breast tissue obtained from reduction surgeries. Phys. Med. Biol. 2007, 52, 2637. [Google Scholar] [CrossRef] [Green Version]
- Lazebnik, M.; Popovic, D.; McCartney, L.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Ogilvie, T.; Magliocco, A.; Breslin, T.M.; et al. A large-scale study of the ultrawideband microwave dielectric properties of normal, benign and malignant breast tissues obtained from cancer surgeries. Phys. Med. Biol. 2007, 52, 6093. [Google Scholar] [CrossRef] [PubMed]
- Aldhaeebi, M.A.; Alzoubi, K.; Almoneef, T.S.; Bamatraf, S.M.; Attia, H.; Ramahi, O.M. Review of microwaves techniques for breast cancer detection. Sensors 2020, 20, 2390. [Google Scholar] [CrossRef] [Green Version]
- Meaney, P.M.; Kaufman, P.A.; Muffly, L.S.; Click, M.; Poplack, S.P.; Wells, W.A.; Schwartz, G.N.; di Florio-Alexander, R.M.; Tosteson, T.D.; Li, Z.; et al. Microwave imaging for neoadjuvant chemotherapy monitoring: Initial clinical experience. Breast Cancer Res. 2013, 15, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Preece, A.W.; Craddock, I.; Shere, M.; Jones, L.; Winton, H.L. MARIA M4: Clinical evaluation of a prototype ultrawideband radar scanner for breast cancer detection. J. Med. Imaging 2016, 3, 033502. [Google Scholar] [CrossRef]
- Shere, M.; Lyburn, I.; Sidebottom, R.; Massey, H.; Gillett, C.; Jones, L. MARIA® M5: A multicentre clinical study to evaluate the ability of the Micrima radio-wave radar breast imaging system (MARIA®) to detect lesions in the symptomatic breast. Eur. J. Radiol. 2019, 116, 61–67. [Google Scholar] [CrossRef]
- Massey, H.; Ridley, N.; Lyburn, I.; Taylor, S.; Schoenleber-Lewis, M.; Bannister, P.; Shere, M.H. Radio-wave detection of breast cancer in the symptomatic clinic—A multi-centre study. In Proceedings of the International Cambridge Conference on Breast Imaging, Cambridge, UK, 3–4 July 2017; pp. 3–4. [Google Scholar]
- Rana, S.P.; Dey, M.; Tiberi, G.; Sani, L.; Vispa, A.; Raspa, G.; Duranti, M.; Ghavami, M.; Dudley, S. Machine learning approaches for automated lesion detection in microwave breast imaging clinical data. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Curtis, C.; Lavoie, B.R.; Fear, E. An analysis of the assumptions inherent to near-field beamforming for biomedical applications. IEEE Trans. Comput. Imaging 2017, 3, 953–965. [Google Scholar] [CrossRef]
- Yang, F.; Sun, L.; Hu, Z.; Wang, H.; Pan, D.; Wu, R.; Zhang, X.; Chen, Y.; Zhang, Q. A large-scale clinical trial of radar-based microwave breast imaging for Asian women: Phase I. In Proceedings of the 2017 IEEE International Symposium on Antennas and Propagation &USNC/URSI National Radio Science Meeting, San Diego, CA, USA, 9–14 July 2017; pp. 781–783. [Google Scholar]
- Kurrant, D.; Bourqui, J.; Fear, E. Surface estimation for microwave imaging. Sensors 2017, 17, 1658. [Google Scholar] [CrossRef] [Green Version]
- Song, H.; Sasada, S.; Kadoya, T.; Okada, M.; Arihiro, K.; Xiao, X.; Kikkawa, T. Detectability of breast tumor by a hand-held impulse-radar detector: Performance evaluation and pilot clinical study. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, E.; Duff, K.; Popovic, M.; Coates, M. Investigation of time-domain microwave radar with breast clinic patients. In Proceedings of the 2016 10th European Conference on Antennas and Propagation (EuCAP), Davos, Switzerland, 10–15 April 2016; pp. 1–3. [Google Scholar]
- Kuwahara, Y.; Malik, A. Microwave imaging for early breast cancer detection. In New Perspect; Breast Imaging; IntechOpen: London, UK, 2017; pp. 45–71. [Google Scholar]
- Sani, L.; Vispa, A.; Loretoni, R.; Duranti, M.; Ghavami, N.; Alvarez Sánchez-Bayuela, D.; Caschera, S.; Paoli, M.; Bigotti, A.; Badia, M.; et al. Breast lesion detection through MammoWave device: Empirical detection capability assessment of microwave images’ parameters. PLoS ONE 2021, 16, e0250005. [Google Scholar] [CrossRef] [PubMed]
- Picard, R.R.; Cook, R.D. Cross-validation of regression models. J. Am. Stat. Assoc. 1984, 79, 575–583. [Google Scholar] [CrossRef]
- Source: ClinicalTrials.gov, United States National Library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT04253366 (accessed on 30 August 2021).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Breast (L/R) | ACR Breast Density | Mammography BI-RADS | Echography BI-RADS | Radiologist’s Output Details: Sizes (mm) and Notes (If Available) | Pathology or 1-Year Clinical Follow-Up Output |
|---|---|---|---|---|---|---|
| 48 | L | D | 3 | - | Microcalcifications | Benign |
| 65 | L | C | 4 | - | Cluster of microcalcifications | Benign |
| 40 | L | B | 2 | 2 | Three masses: 15 mm, 21 mm, and 23 mm | Benign |
| R | B | 2 | 2 | Microcalcifications | Not available | |
| 52 | L | C | 5 | - | Microcalcifications | Malignant |
| 47 | L | D | 2 | 2 | Microcalcifications | Benign |
| 55 | R | C | 2 | 2 | 1.6 mm microcalcifications | Benign |
| L | C | 2 | 2 | 3.8 mm microcalcifications | Benign | |
| 51 | L | C | 2 | 2 | Presence of metallic marker | Benign |
| 54 | R | A | 2 | 2 | Microcalcifications | Benign |
| 77 | R | D | - | 5 | 17 mm mass | Malignant |
| 61 | R | C | 4 | - | Multifocal lobular type suspected carcinoma (MRI BI-RADS 4) | Malignant |
| L | C | 2 | - | Macrocalcification and Focal contrast enh. (MRI BI-RADS 3) | Not available | |
| 50 | L | B | 2 | 2 | 10 mm mass | Benign |
| 67 | L | C | 4 | - | Microcalcifications | Malignant |
| 49 | L | A | 3 | - | Microcalcifications | Benign |
| 70 | L | D | 3 | 4 | Mass | Malignant |
| 42 | L | C | 2 | 3 | 7 mm mass, hypoechoic | Benign |
| 67 | L | B | 3 | - | Architectural distortion | Benign |
| 56 | R | B | 4 | 4 | 31 mm mass, hypoechoic, irregular borders | Malignant |
| 43 | R | D | 1 | 3 | 12 mm mass | Benign |
| 51 | L | C | 3 | - | Microcalcifications | Benign |
| 59 | L | B | - | 4 | 11 mm areolar, suspicious of malignancy | Malignant |
| 40 | L | D | 2 | 2 | 30 mm mass | Benign |
| 35 | R | C | 2 | 3 | 7 mm, hypoechoic | Benign |
| 37 | L | A | 2 | 3 | 25 mm mass | Benign |
| 43 | R | B | 3 | 2 | Microcalcifications | Malignant |
| 54 | R | B | 2 | 2 | 18 mm mass | Benign |
| 49 | L | A | 2 | 3 | 16 mm mass | Benign |
| 56 | L | D | 4 | 4 | 27 mm mass | Malignant |
| 63 | L | A | 3 | 4 | 6 mm mass | Malignant |
| 55 | R | C | 4 | 4 | 23 mm mass | Malignant |
| L | C | 2 | 2 | Multiple cysts | Benign | |
| 64 | R | B | 3 | - | 1.6 mm microcalcifications | Benign |
| 37 | R | - | - | 3 | 15.4 mm mass | Benign |
| L | - | - | 2 | Multiple cysts | Not available |
| Null Hypothesis () | Probabilty (p) | Confidence Interval-Lower Boundary () | Confidence Interval-Upper Boundary () |
|---|---|---|---|
| 1 |
| Null Hypothesis () | Probabilty (p) | Confidence Interval-Lower Boundary () | Confidence Interval-Upper Boundary () |
|---|---|---|---|
| 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rana, S.P.; Dey, M.; Loretoni, R.; Duranti, M.; Sani, L.; Vispa, A.; Ghavami, M.; Dudley, S.; Tiberi, G. Radial Basis Function for Breast Lesion Detection from MammoWave Clinical Data. Diagnostics 2021, 11, 1930. https://doi.org/10.3390/diagnostics11101930
Rana SP, Dey M, Loretoni R, Duranti M, Sani L, Vispa A, Ghavami M, Dudley S, Tiberi G. Radial Basis Function for Breast Lesion Detection from MammoWave Clinical Data. Diagnostics. 2021; 11(10):1930. https://doi.org/10.3390/diagnostics11101930
Chicago/Turabian StyleRana, Soumya Prakash, Maitreyee Dey, Riccardo Loretoni, Michele Duranti, Lorenzo Sani, Alessandro Vispa, Mohammad Ghavami, Sandra Dudley, and Gianluigi Tiberi. 2021. "Radial Basis Function for Breast Lesion Detection from MammoWave Clinical Data" Diagnostics 11, no. 10: 1930. https://doi.org/10.3390/diagnostics11101930
APA StyleRana, S. P., Dey, M., Loretoni, R., Duranti, M., Sani, L., Vispa, A., Ghavami, M., Dudley, S., & Tiberi, G. (2021). Radial Basis Function for Breast Lesion Detection from MammoWave Clinical Data. Diagnostics, 11(10), 1930. https://doi.org/10.3390/diagnostics11101930