
What Is a Solitary Keratoacanthoma? A Benign Follicular Neoplasm, Frequently Associated with Squamous Cell Carcinoma


Abstract
:1. Introduction
2. Clinical and Histopathological Characteristics of Solitary KA
2.1. Clinical Findings
2.2. Histopathological Findings
2.2.1. Histopathological Stages
2.2.2. Mutual Findings among Stages
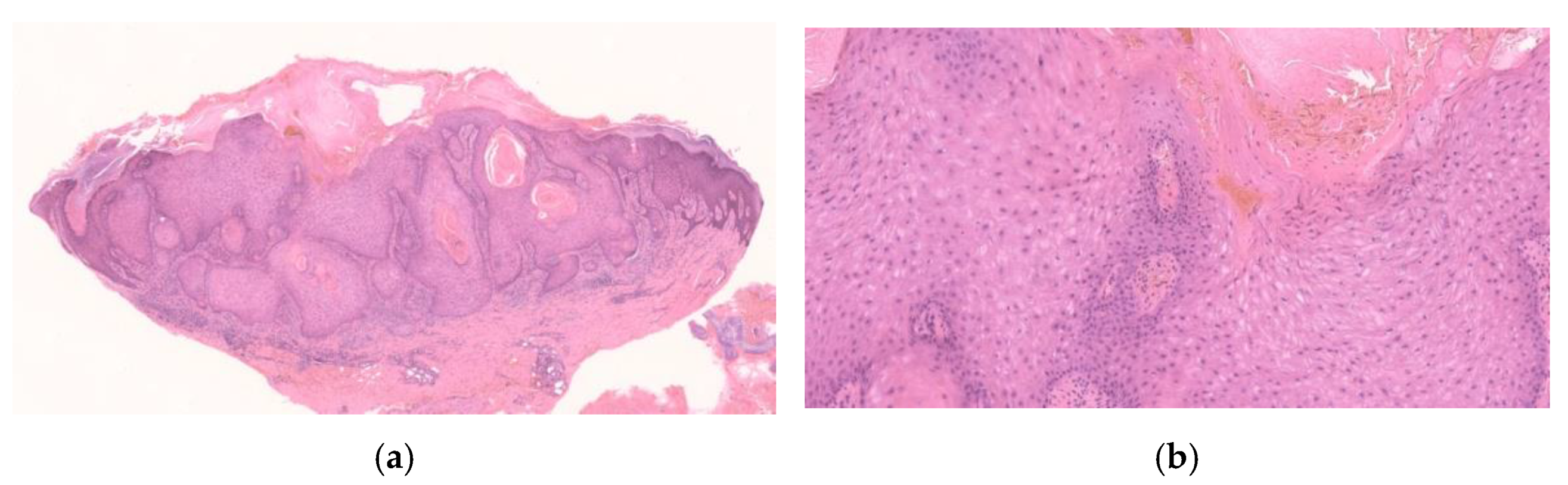
2.2.3. Early/Proliferative Stage
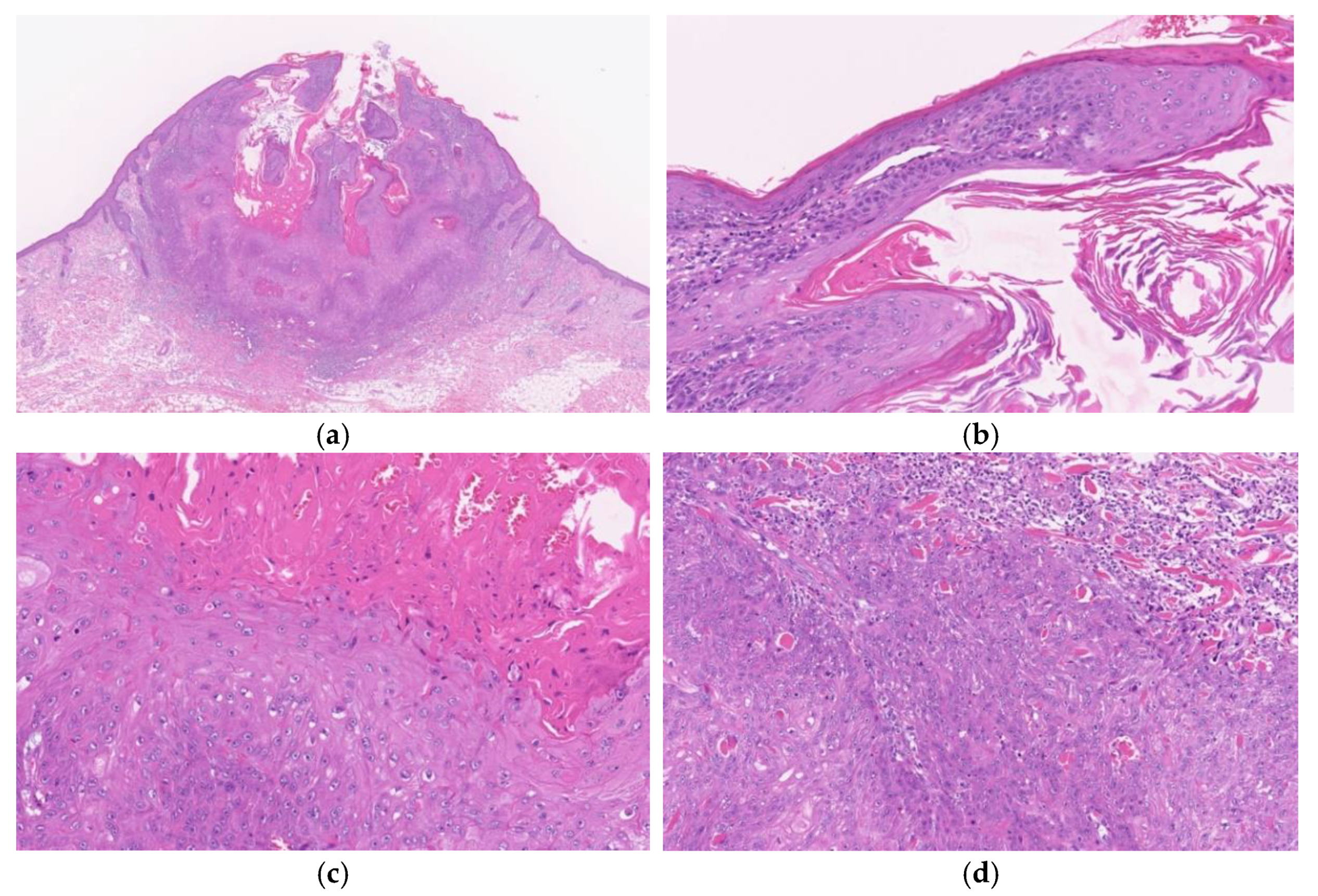
2.2.4. Well-Developed Stage
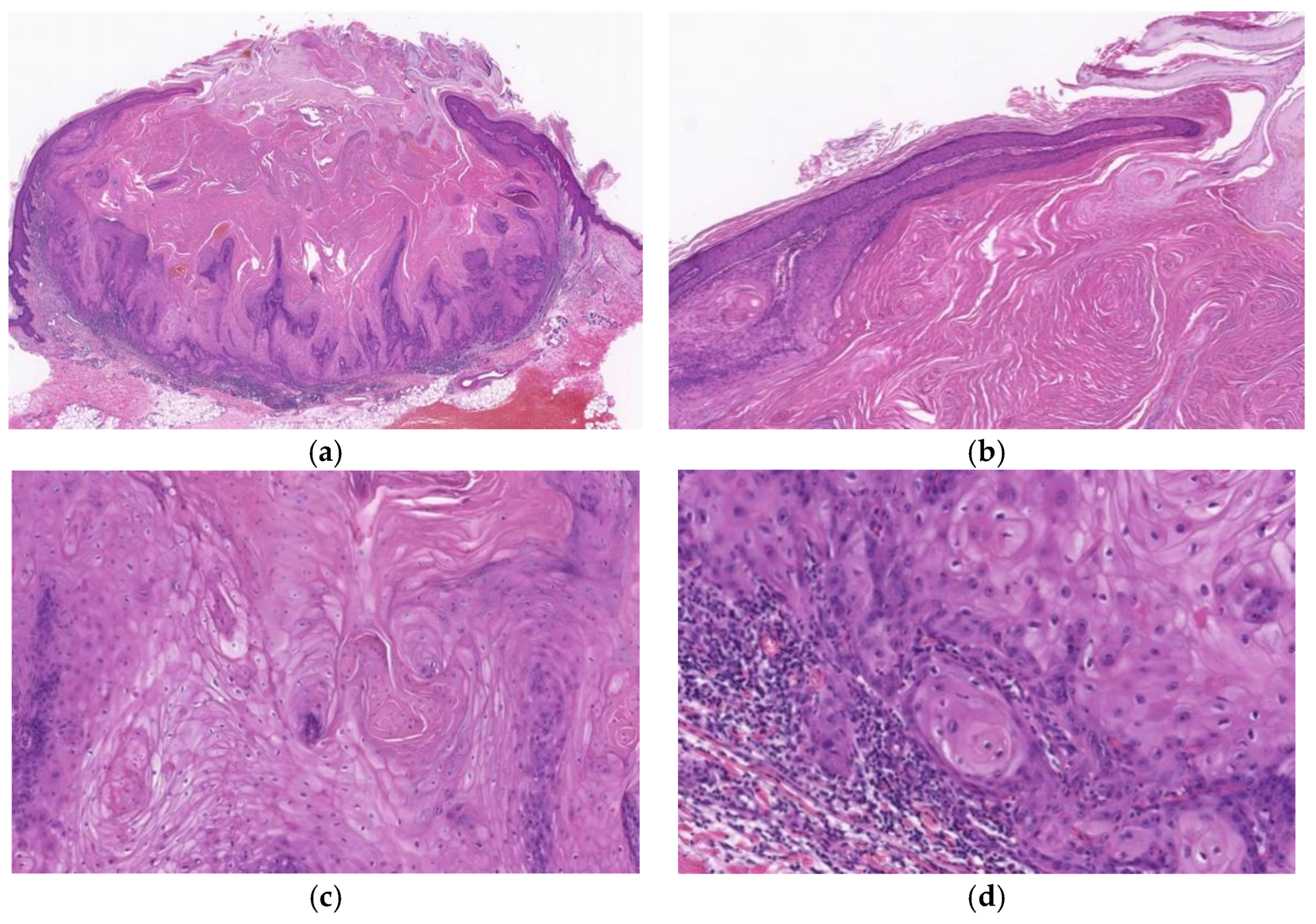
2.2.5. Regressing Stage
2.2.6. Regressed Stage
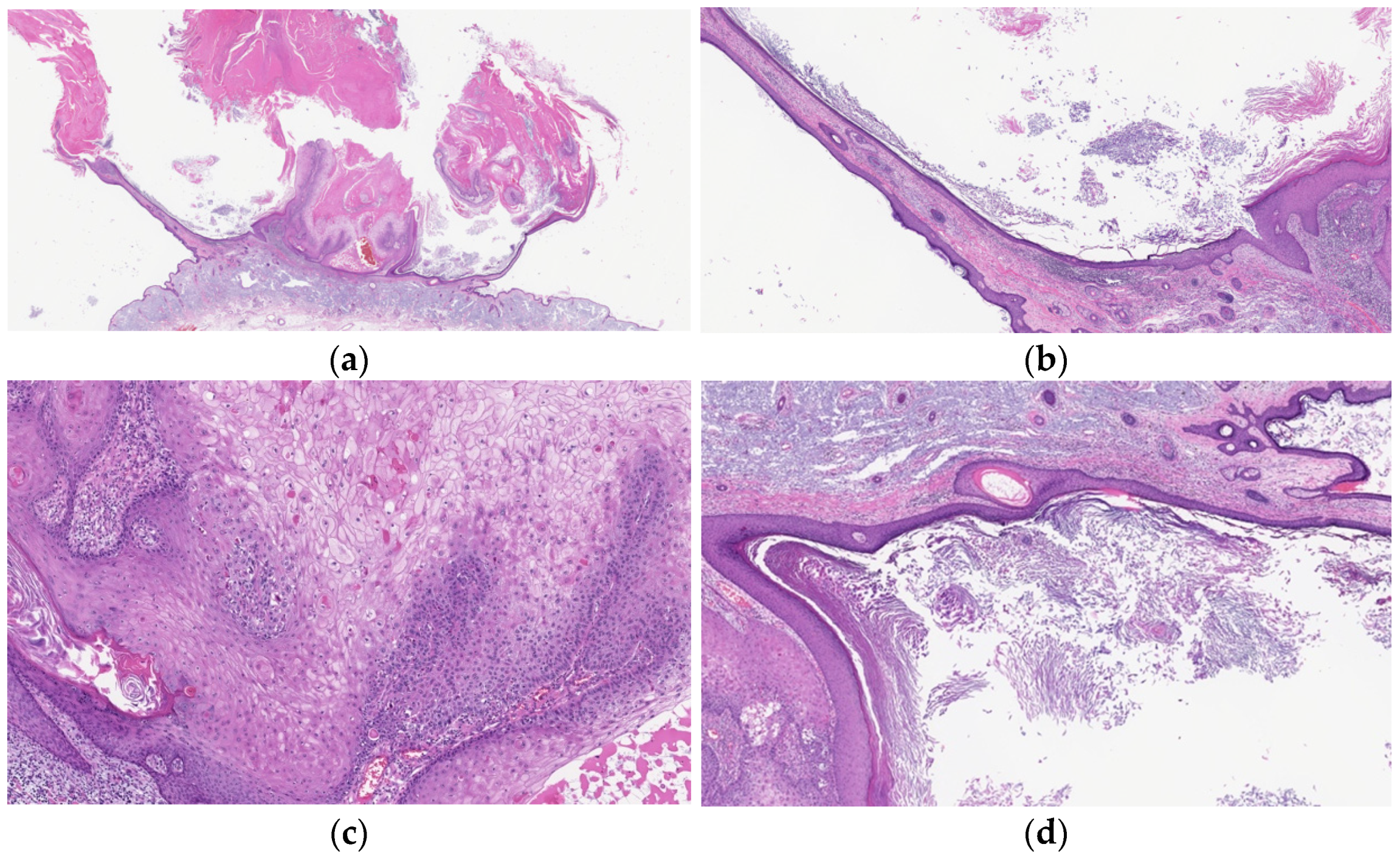
3. Diagnostically Problematic Lesions, KA with a Conventional SCC Component (KASCC)
4. Other Crateriform Tumors
4.1. Benign Neoplasms
4.1.1. Crateriform Verruca (CFV)
4.1.2. Crateriform Seborrheic Keratosis (CSK)
4.2. Other Malignant Neoplasms
4.2.1. Crateriform (Papillated) Bowen Disease
4.2.2. Crateriform SCC Arising from Actinic Keratosis (cSCC)
4.2.3. Crater Form of Infundibular SCC
5. Data of Histopathological Diagnosis of Lesions Clinically Diagnosed as KA
6. Natural Course of KA and Related Lesions after Partial Biopsy
7. Incidence of Crateriform Epithelial Neoplasms
8. Conclusions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murphy, G.F.; Beer, T.W.; Cerio, R.; Kao, G.F.; Nagore, E.; Pulitzer, M.P. Squamous cell carcinoma. In World Health Organization Classification of Tumours, 4th ed.; Elder, D.E., Massi, D., Scolyer, R.A., Willemze, R., Eds.; IARC Press: Lyon, France, 2018; pp. 35–45. [Google Scholar]
- Bennardo, L.; Bennardo, F.; Giudice, A.; Passante, M.; Dastoli, S.; Morrone, P.; Provensano, E.; Patruno, C.; Nisticò, S.P. Local chemotherapy as an adjuvant treatment in unresectable squamous cell carcinoma: What do we know so far? Curr. Oncol. 2021, 28, 2317–2325. [Google Scholar] [CrossRef]
- Tisak, A.; Fotouhi, A.; Fidai, C.; Fridman, B.J.; Ozog, D.; Veenstra, J. A clinical and biological review of keratoacanthoma. Br. J. Dermatol. 2021, 185, 487–498. [Google Scholar] [CrossRef]
- Cribier, B.; Asch, P.-H.; Grosshans, E. Differentiating squamous cell carcinoma from keratoacanthoma using histopathological criteria. Is it possible? A study of 296 cases. Dermatology 1999, 199, 208–212. [Google Scholar] [CrossRef]
- Hodak, E.; Jones, R.E.; Ackerman, A.B. Solitary keratoacanthoma is a squamous-cell carcinoma: Three examples with metastasis. Am. J. Dermatopathol. 1993, 15, 332–342. [Google Scholar] [CrossRef]
- Ansai, S.; Manabe, M. Possible spontaneous regression of a metastatic lesion of keratoacanthoma-like squamous cell carcinoma in a regional lymph node. J. Dermatol. 2005, 32, 899–903. [Google Scholar] [CrossRef]
- Misago, N.; Takai, T.; Toda, S.; Narisawa, Y. The histopathologic changes in keratoacanthoma depend on its stage. J. Cutan. Pathol. 2014, 41, 617–619. [Google Scholar] [CrossRef] [PubMed]
- Misago, N.; Takai, T.; Toda, S.; Narisawa, Y. The changes in the expression levels of follicular markers in keratoacanthoma depend on the stage: Keratoacanthoma is a follicular neoplasm exhibiting infundibular/isthmic differentiation without expression of CK15. J. Cutan. Pathol. 2014, 41, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Misago, N.; Inoue, T.; Koba, S.; Narisawa, Y. Keratoacanthoma and other types of squamous cell carcinoma with crateriform architecture: Classification and identification. J. Dermatol. 2013, 40, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Takai, T.; Misago, N.; Murata, Y. Natural course of keratoacanthoma and related lesions after partial biopsy: The clinical analysis of the 66 lesions. J. Dermatol. 2015, 42, 353–362. [Google Scholar] [CrossRef]
- Misago, N.; Inoue, T.; Nagase, K.; Tsuruta, N.; Tara-Hashimoto, A.; Kimura, H.; Takahara, K.; Narita, T.; Narisawa, Y. Crater/ulcerated form of infundibular squamous cell carcinoma: A possible distinct entity as a malignant (or high-grade) counterpart to keratoacanthoma. J. Dermatol. 2015, 42, 667–673. [Google Scholar] [CrossRef]
- Ogita, A.; Ansai, S.; Misago, N.; Anan, T.; Fukumoto, T.; Saeki, H. Histopathological diagnosis of epithelial crateriform tumors: Keratoacanthoma and other epithelial crateriform tumors. J. Dermatol. 2016, 43, 1321–1331. [Google Scholar] [CrossRef]
- Takai, T. Advances in histopathological diagnosis of keratoacanthoma. J. Dermatol. 2017, 44, 304–314. [Google Scholar] [CrossRef] [Green Version]
- Misago, N.; Ansai, S.; Fukumoto, T.; Anan, T.; Nakao, T. Keratoacanthoma en plaque/nodule: A brief report of the clinicopathological features of five cases. J. Dermatol. 2017, 44, 803–807. [Google Scholar] [CrossRef]
- Sáchez Yus, E.; Simón, P.; Requena, L.; Ambrojo, P.; de Eusebio, E. Solitary keratoacanthoma: A self-healing proliferation that frequently becomes malignant. Am. J. Dermatopathol. 2000, 22, 305–310. [Google Scholar]
- Weedon, D.D.; Malo, J.; Brooks, D.; Williamson, R. Squamous cell carcinoma arising in keratoacanthoma: A neglected phenomenon in the elderly. Am. J. Dermatopathol. 2010, 32, 423–426. [Google Scholar] [CrossRef]
- Ogita, A.; Ansai, S.; Misago, N.; Anan, T.; Fukumoto, T.; Saeki, H. Clinicopathological study of crateriform verruca: Crateriform epithelial lesions histopathologically distinct from keratoacanthoma. J. Dermatol. 2016, 43, 1154–1159. [Google Scholar] [CrossRef]
- Poblet, E.; Jimenez-Reyes, J.; Gonzalez-Herrada, C.; Granados, R. Trichilemmal keratosis. A clinicopathologic and immunohistochemical study of two cases. Am. J. Dermatopathol. 1996, 18, 543–547. [Google Scholar] [CrossRef]
- Kimura, S. Trichilemmal keratosis (horn): A light and electron microscopic study. J. Cutan. Pathol. 1983, 10, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.D.; Barr, R.J. Papillated Bowen disease, a distinct variant. Am. J. Dermatopathol. 2006, 28, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Cascajo, C.; Borghi, S.; Weyers, W.; Bastida-Inarrea, J. Follicular squamous cell carcinoma of the skin: A poorly recognized neoplasm arising from the wall of hair follicles. J. Cutan. Pathol. 2004, 31, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Kossard, S.; Tan, K.B.; Choy, C. Keratoacanthoma and infundibulocystic squamous cell carcinoma. Am. J. Dermatopathol. 2008, 30, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Misago, N.; Inoue, T.; Toda, S.; Narisawa, Y. Infundibular (follicular) and infundibulocystic squamous cell carcinoma: A clinicopathological and immunohistochemical study. Am. J. Dermatopahtol. 2011, 33, 687–694. [Google Scholar] [CrossRef]
- Ansai, S.; Fukumoto, T.; Anan, T.; Kimura, T.; Kawana, S. Histopathological diagnosis of lesions clinically diagnosed as keratoacanthoma. Jpn. J. Dermmtol. 2013, 123, 1775–1784. [Google Scholar]
- Ansai, S.; Umebayashi, Y.; Katsumata, N.; Kato, H.; Kadono, T.; Takai, T.; Namiki, T.; Nakagawa, M.; Soejima, T.; Koga, H.; et al. Japanese dermatological association guidelines: Outlines of guidelines for cutaneous squamous cell carcinoma 2020. J. Dermatol. 2021, 48, e288–e311. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Benign Neoplasms | Malignant Neoplasms |
|---|---|
| Crateriform verruca (CFV) | Crateriform (Papillated) Bowen disease |
| Crateriform seborrheic keratosis (CSK) | |
| KA with conventional SCC component (KASCC) | |
| Keratoacanthoma (KA) | Crateriform SCC arising from actinic keratosis (cSCC) |
| Crater form of infundibular SCC |
| Tumor | Case | |
|---|---|---|
| CFV | 76 (20.0%) | |
| CSK | 12 (3.2%) | |
| KA | early/proliferative | 85 (22.4%) |
| well-developed | 82 (21.6%) | |
| regressing/regressed | 47 (12.4%) | |
| total | 214 (56.3%) | |
| Crateriform Bowen disease | 12 (3.2%) | |
| KAs with a conventional SCC | 45 (11.8%) | |
| cSCC | 11 (2.9%) | |
| Crateriform infundibular SCC | 10 (2.6%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogita, A.; Ansai, S.-i. What Is a Solitary Keratoacanthoma? A Benign Follicular Neoplasm, Frequently Associated with Squamous Cell Carcinoma. Diagnostics 2021, 11, 1848. https://doi.org/10.3390/diagnostics11101848
Ogita A, Ansai S-i. What Is a Solitary Keratoacanthoma? A Benign Follicular Neoplasm, Frequently Associated with Squamous Cell Carcinoma. Diagnostics. 2021; 11(10):1848. https://doi.org/10.3390/diagnostics11101848
Chicago/Turabian StyleOgita, Azusa, and Shin-ichi Ansai. 2021. "What Is a Solitary Keratoacanthoma? A Benign Follicular Neoplasm, Frequently Associated with Squamous Cell Carcinoma" Diagnostics 11, no. 10: 1848. https://doi.org/10.3390/diagnostics11101848
APA StyleOgita, A., & Ansai, S.-i. (2021). What Is a Solitary Keratoacanthoma? A Benign Follicular Neoplasm, Frequently Associated with Squamous Cell Carcinoma. Diagnostics, 11(10), 1848. https://doi.org/10.3390/diagnostics11101848