Pre-Radiotherapy Progression after Surgery of Newly Diagnosed Glioblastoma: Corroboration of New Prognostic Variable

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
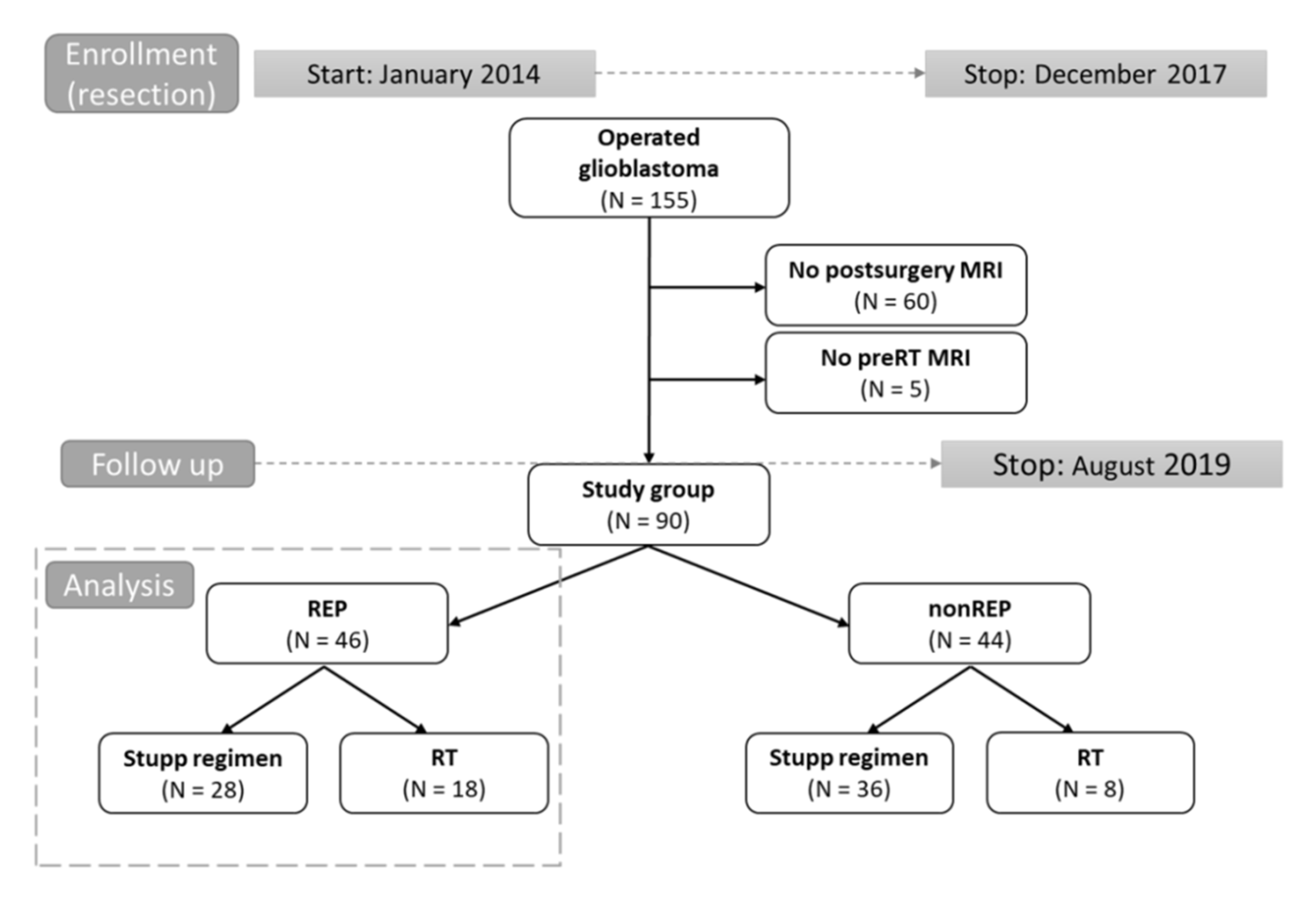
2.1. Patients and Treatment
2.2. Imaging Evaluation
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristics
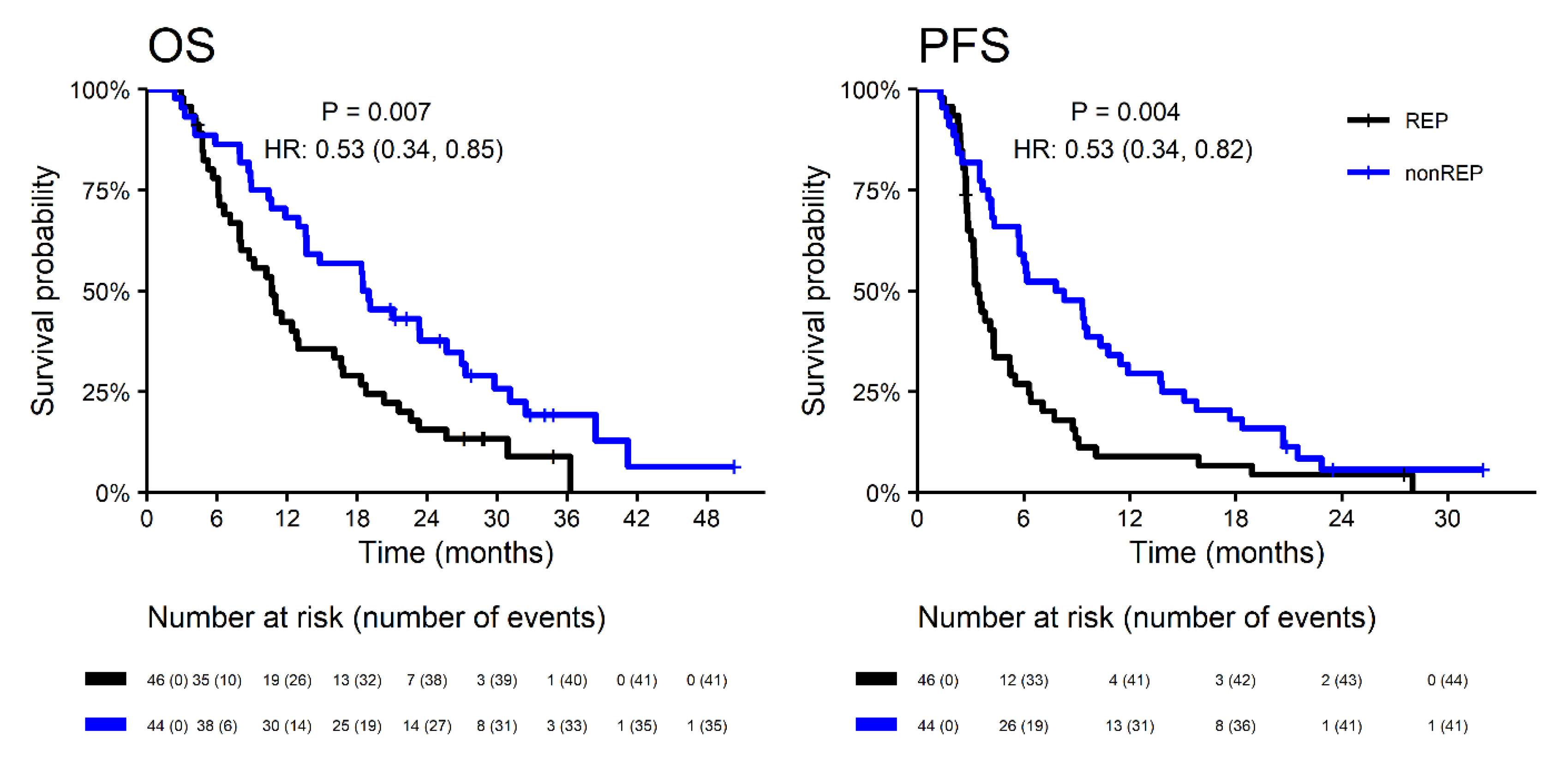
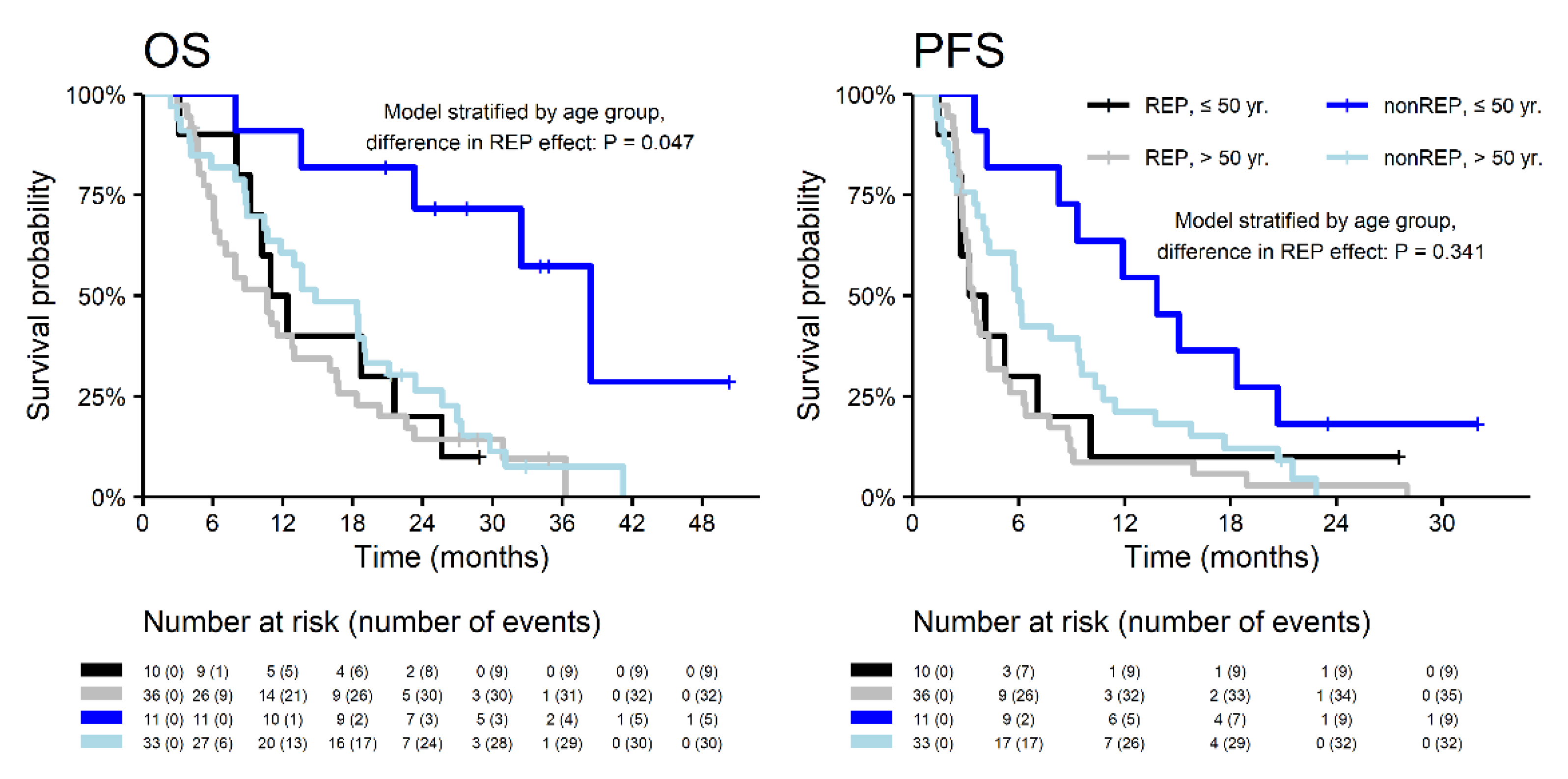
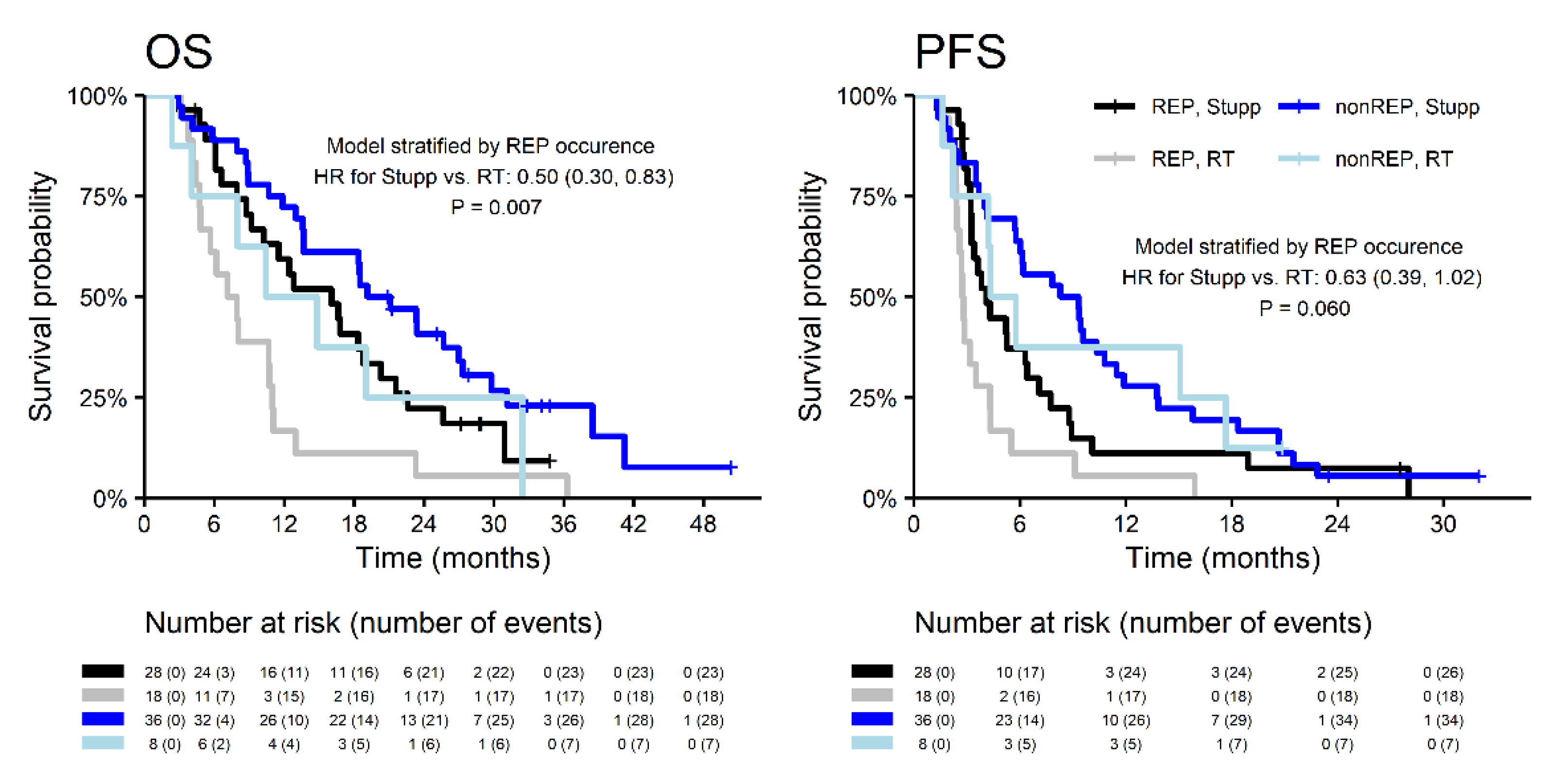
3.2. Rapid Early Progression
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Kazda, T.; Dziacky, A.; Burkon, P.; Pospisil, P.; Slavik, M.; Rehak, Z.; Jancalek, R.; Slampa, P.; Slaby, O.; Lakomy, R. Radiotherapy of Glioblastoma 15 Years after the Landmark Stupp’s Trial: More Controversies than Standards? Radiol. Oncol. 2018, 52, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of tumor-treating fields plus maintenance temozolomide vs maintenance temozolomide alone on survival in patients with glioblastoma: A randomized clinical trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.R.; Laperriere, N.; O’Callaghan, C.J.; Brandes, A.A.; Menten, J.; Phillips, C.; Fay, M.; Nishikawa, R.; Cairncross, J.G.; Roa, W.; et al. Short-course radiation plus temozolomide in elderly patients with glioblastoma. N. Engl. J. Med. 2017, 376, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- Herrlinger, U.; Tzaridis, T.; Mack, F.; Steinbach, J.; Schlegel, U.; Sabel, M.; Hau, P.; Kortman, R.D.; Krex, D.; Grauer, O.; et al. Phase III trial of CCNU/temozolomide (TMZ) combination therapy vs. standard TMZ therapy for newly diagnosed MGMT-methylated glioblastoma patients: The randomized, open-label CeTeG/NOA-09 trial. Lancet 2019, 393, 678–688. [Google Scholar] [CrossRef]
- Hegi, M.E.; Liu, L.; Herman, J.G.; Stupp, R.; Wick, W.; Weller, M.; Mehta, M.P.; Gilbert, M.R. Correlation of O6-methylguanine methyl-transferase (MGMT) promoter methylation with clinical outcomes in glioblastoma and clinical strategies to modulate MGMT activity. J. Clin. Oncol. 2008, 26, 4189–4199. [Google Scholar] [CrossRef] [PubMed]
- Sanson, M.; Marie, Y.; Paris, S.; Idbaih, A.; Laffaire, J.; Ducray, F.; El Hallani, S.; Boisselier, B.; Mokhtari, K.; Hoang-Xuan, K.; et al. Isocitrate dehydrogenase 1 codon 132 mutation is an important prognostic biomarker in gliomas. J. Clin. Oncol. 2009, 27, 4150–4154. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef]
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.A.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A.; et al. Glioblastoma in Adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) Consensus Review on Current Management and Future Directions. Neuro. Oncol. 2020, 8, 1073–1113. [Google Scholar] [CrossRef]
- Merkel, A.; Soeldner, D.; Wendl, C.; Urkan, D.; Kuramatsu, J.B.; Seliger, C.; Proescholdt, M.; Eyupoglu, I.Y.; Hau, P.; Uhl, M. Early postoperative tumor progression predicts clinical outcome in glioblastoma-implication for clinical trials. J. Neurooncol. 2017, 132, 249–254. [Google Scholar] [CrossRef]
- Villanueva-Meyer, J.E.; Han, S.J.; Cha, S.; Butowski, N.A. Early tumor growth between initial resection and radiotherapy of glioblastoma: Incidence and impact on clinical outcomes. J. Neurooncol. 2017, 134, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.D.; Bhamidipati, D.; Shukla, G.; Sharma, D.; Glass, J.; Kim, L.; Evans, J.J.; Judy, K.; Farrell, C.; Andrews, D.W. Rapid Early Tumor Progression is Prognostic in Glioblastoma Patients. Am. J. Clin. Oncol. 2019, 42, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Sulman, E.P.; Ismaila, N.; Armstrong, T.S.; Tsien, C.; Batchelor, T.T.; Cloughesy, T.; Galanis, E.; Gilbert, M.; Gondi, V.; Lovely, M. Radiation Therapy for Glioblastoma: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Society for Radiation Oncology Guideline. J. Clin. Oncol. 2017, 35, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Niyazi, M.; Brada, M.; Chalmers, A.J.; Combs, S.E.; Erridge, S.C.; Fiorentino, A.; Grosu, A.L.; Lagerwaard, F.J.; Minniti, G.; Mirimanoff, R.O.; et al. ESTRO-ACROP guideline “target delineation of glioblastomas”. Radiother. Oncol. 2016, 118, 35–42. [Google Scholar] [CrossRef]
- Chukwueke, U.N.; Wen, P.Y. Use of the Response Assessment in Neuro-Oncology (RANO) criteria in clinical trials and clinical practice. CNS Oncol. 2019, 8, CNS28. [Google Scholar] [CrossRef] [PubMed]
- Kazda, T.; Bulik, M.; Pospisil, P.; Lakomy, R.; Smrcka, M.; Slampa, P.; Jancalek, R. Advanced MRI increases the diagnostic accuracy of recurrent glioblastoma: Single institution thresholds and validation of MR spectroscopy and diffusion weighted MR imaging. Neuroimage Clin. 2016, 11, 316–321. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 6 April 2020).
- Irwin, C.; Hunn, M.; Purdie, G.; Hamilton, D. Delay in radiotherapy shortens survival in patients with high grade glioma. J. Neurooncol. 2007, 85, 339–343. [Google Scholar] [CrossRef]
- Gliński, B.; Urbański, J.; Hetnał, M.; Małecki, K.; Jarosz, M.; Mucha-Małecka, A.; Chrostowska, A.; Jakubowicz, E.; Frączek-Błachut, B.; Dymek, P. Prognostic value of the interval from surgery to initiation of radiation therapy in correlation with some histo-clinical parameters in patients with malignant supratentorial gliomas. Contemp Oncol. 2012, 16, 34–37. [Google Scholar] [CrossRef]
- Noel, G.; Huchet, A.; Feuvret, L.; Maire, J.P.; Verrelle, P.; Le Rhun, E.; Aumont, M.; Thillays, F.; Sunyach, M.P.; Henzen, C.; et al. Waiting times before initiation of radiotherapy might not affect outcomes for patients with glioblastoma: A French retrospective analysis of patients treated in the era of concomitant temozolomide and radiotherapy. J. Neurooncol. 2012, 109, 167–175. [Google Scholar] [CrossRef]
- Lutterbach, J.; Weigel, P.; Guttenberger, R.; Hinkelbein, W. Accelerated hyper-fractionated radiotherapy in 149 patients with glioblastoma multiforme. Radiother. Oncol. 1999, 53, 49–52. [Google Scholar] [CrossRef]
- Hulshof, M.C.; Koot, R.W.; Schimmel, E.C.; Dekker, F.; Bosch, D.A.; González González, D. Prognostic factors in glioblastoma multiforme. 10 years experience of a single institution. Strahlenther. Onkol. 2001, 177, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Lai, R.; Hershman, D.L.; Doan, T.; Neugut, A.I. The timing of cranial radiation in elderly patients with newly diagnosed glioblastoma multiforme. Neuro. Oncol. 2010, 12, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, D.T.; Won, M.; Mehta, M.P.; Curran, W.J.; Souhami, L.; Michalski, J.M.; Rogers, C.L.; Corn, B.W. Short delay in initiation of radiotherapy may not affect outcome of patients with glioblastoma: A secondary analysis from the radiation therapy oncology group database. J. Clin. Oncol. 2009, 27, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Burnet, N.G.; Jena, R.; Jefferies, S.J.; Stenning, S.P.; Kirkby, N.F. Mathematical modelling of survival of glioblastoma patients suggests a role for radiotherapy dose escalation and predicts poorer outcome after delay to start treatment. Clin. Oncol. 2006, 18, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Grewal, A.S.; Schonewolf, C.; Min, E.J.; Chao, H.H.; Both, S.; Lam, S.; Mazzoni, S.; Bekelman, J.; Christodouleas, J.; Vapiwala, N. The effect of delay in treatment on local control by radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1996, 34, 243–250. [Google Scholar] [CrossRef]
- Han, S.J.; Englot, D.J.; Birk, H.; Molinaro, A.M.; Chang, S.M.; Clarke, J.L.; Prados, M.D.; Taylor, J.W.; Berger, M.S.; Butowski, N.A. Impact of Timing of Concurrent Chemoradiation for Newly Diagnosed Glioblastoma: A Critical Review of Current Evidence. Neurosurgery 2015, 62, 160–165. [Google Scholar] [CrossRef]
- Marra, J.S.; Mendes, G.P.; Yoshinari, G.H., Jr.; da Silva Guimarães, F.; Mazin, S.C.; de Oliveira, H.F. Survival after radiation therapy for high-grade glioma. Rep. Pract. Oncol. Radiother. 2019, 24, 35–40. [Google Scholar] [CrossRef]
- Albert, N.L.; Weller, M.; Suchorska, B.; Galldiks, N.; Soffietti, R.; Kim, M.M.; la Fougère, C.; Pope, W.; Law, I.; Arbizu, J.; et al. Response Assessment in Neuro-Oncology working group and European Association for Neuro-Oncology recommendations for the clinical use of PET imaging in gliomas. Neuro. Oncol. 2016, 18, 1199–1208. [Google Scholar] [CrossRef]
- Grosu, A.L.; Weber, W.A.; Riedel, E.; Jeremic, B.; Nieder, C.; Franz, M.; Gumprecht, H.; Jaeger, R.; Schwaiger, M.; Molls, M. L-(methyl-11C) methionine positron emission tomography for target delineation in resected high-grade gliomas before radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 64–74. [Google Scholar] [CrossRef]
- Killela, P.J.; Pirozzi, C.J.; Healy, P.; Reitman, Z.J.; Lipp, E.; Ahmed Rasheed, B.; Yang, R.; Diplas, B.H.; Wang, Z.; Greeret, P.K.; et al. Mutations in IDH1, IDH2, and in the TERT promoter define clinically distinct subgroups of adult malignant gliomas. Oncotarget 2014, 5, 1515–1525. [Google Scholar] [CrossRef]
- Arita, H.; Yamasaki, K.; Matsushita, Y.; Nakamura, T.; Shimokawa, A.; Takami, H.; Tanaka, S.; Mukasa, A.; Shirahata, M.; Shimizu, S.; et al. A combination of TERT promoter mutation and MGMT methylation status predicts clinically relevant subgroups of newly diagnosed glioblastomas. Acta Neuropathol. Commun. 2016, 4, 79. [Google Scholar] [CrossRef] [PubMed]
- Houdova Megova, M.; Drábek, J.; Dwight, Z.; Trojanec, R.; Koudeláková, V.; Vrbková, J.; Kalita, O.; Mlcochova, S.; Rabcanova, M.; Hajdúch, M. Isocitrate Dehydrogenase Mutations Are Better Prognostic Marker Than O6-methylguanine-DNA Methyltransferase Promoter Methylation in Glioblastomas—A Retrospective, Single-centre Molecular Genetics Study of Gliomas. Klin. Onkol. 2017, 30, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; Butowski, N.; Tran, D.D.; Recht, L.D.; Lim, M.; Hirte, H.; Ashby, L.; Mechtler, L.; Goldlust, S.A.; Iwamoto, F.; et al. Rindopepimut and temozolomide for patients with newly diagnosed, EGFRvIII-expressing glioblastoma (ACT IV): A randomised, double blind, international phase 3 trial. Lancet Oncol. 2017, 18, 1373–1385. [Google Scholar] [CrossRef]
- Filley, A.C.; Henriquez, M.; Dey, M. Recurrent glioma clinical trial, CheckMate-143: The game is not over yet. Oncotarget 2017, 8, 91779–91794. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; Le Rhun, E.; Preusser, M.; Tonn, J.C.; Roth, P. How we treat glioblastoma. ESMO Open 2019, 4, e000520. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Cohort (n = 90) | All | REP | Non-REP | p-Value |
|---|---|---|---|---|
| No. of patients | 90 (100%) | 46 (51%) | 44 (49%) | |
| Age (years) | ||||
| median (IQR) | 59.3 (51.1, 65.2) | 60.0 (52.2, 67.8) | 57.1 (50.6, 63.5) | p = 0.180 |
| ≤50 | 21 (23%) | 10 (22%) | 11 (25%) | p = 0.805 |
| Men | 53 (59%) | 27 (59%) | 26 (59)% | p > 0.999 |
| Performance status (ECOG) and Karnofsky index | ||||
| ECOG 0 (KI 90–100%) | 34 (38%) | 17 (37%) | 17 (39%) | p = 0.868 |
| ECOG 1 (KI 70–80%) | 49 (54%) | 26 (57%) | 23 (52%) | |
| ECOG 2 (KI 50–60%) | 7 (8%) | 3 (7%) | 4 (9%) | |
| Tumor location | ||||
| deep brain location | 21 (23%) | 14 (30%) | 7 (16%) | p = 0.136 |
| Extent of resection | ||||
| GTR | 39 (43%) | 10 (22%) | 29 (66%) | p < 0.001 |
| STR | 44 (49%) | 31 (67%) | 13 (30%) | |
| Partial resection or biopsy | 7 (8%) | 5 (11%) | 2 (5%) | |
| Extent of resection | ||||
| GTR | 39 (43%) | 10 (22%) | 29 (66%) | p < 0.001 |
| Non-GTR | 51 (57%) | 36 (78%) | 15 (34%) | |
| IDH status | ||||
| Mutated/evaluated | 4/53 (8%) | 1/24 (4%) | 3/29 (10%) | |
| MGMT status | ||||
| Methylated/evaluated | 14/53 (26%) | 6/23 (26%) | 8/30 (27%) | p > 0.999 |
| Localization of REP | ||||
| Postsurgery residuum | 31/46 (67%) | |||
| New enhancing satellite | 6/46 (13%) | |||
| New enhancement in the wall of resection cavity | 22/46 (48%) | |||
| Not operated tumor in multicentric tumors | 10/46 (22%) |
| Study Cohort (n = 90) | All (n = 90) | REP (n = 46) | Non-REP (n = 44) | p-Value |
|---|---|---|---|---|
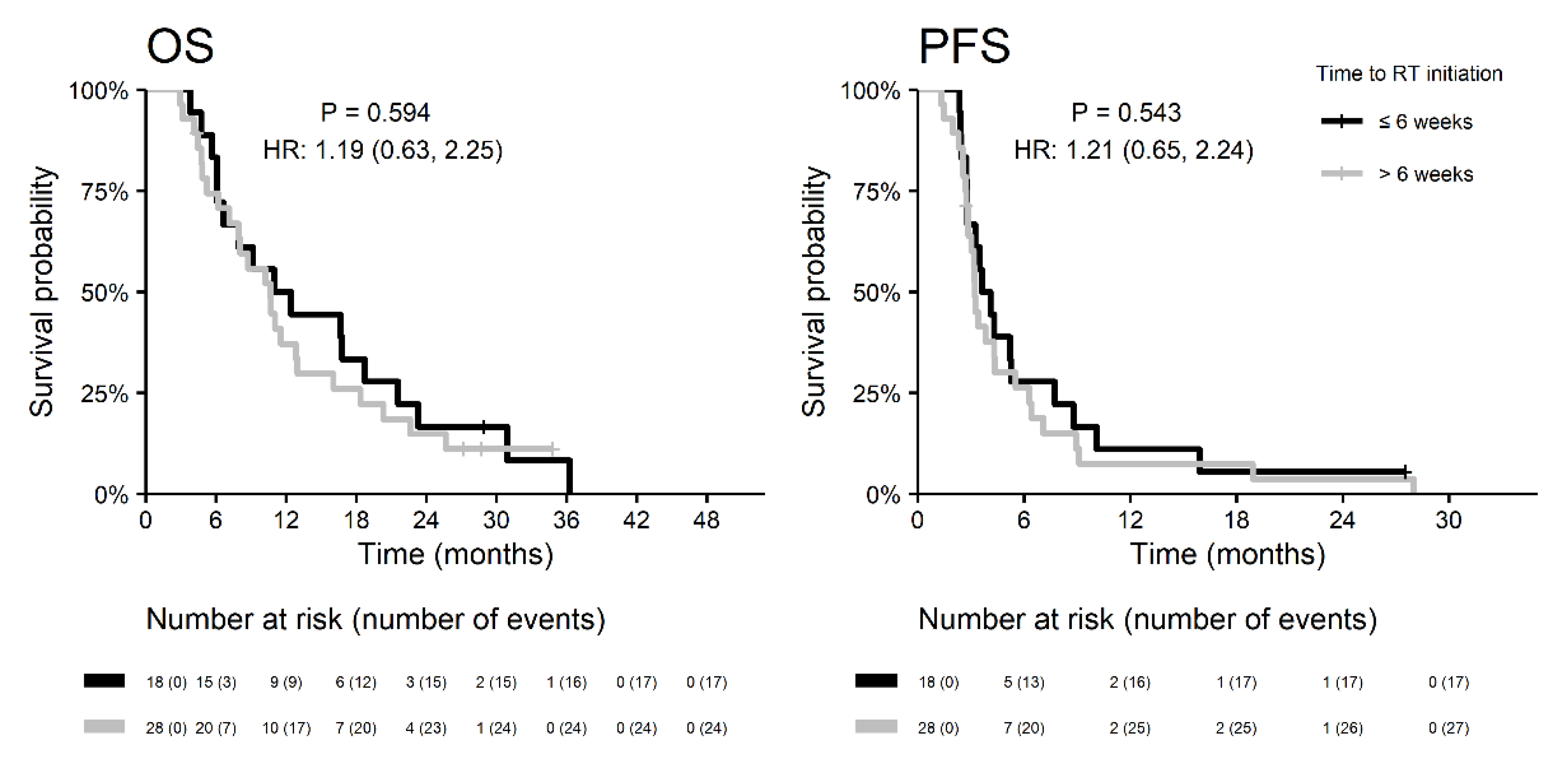
| Time to RT initiation | ||||
| Median (weeks; IQR) | 6.7 (5.9, 7.3) | 6.6 (5.9 7.1) | 6.8 (5.8, 7.5) | p = 0.981 |
| >6 weeks | 56 (62%) | 28 (61%) | 28 (64%) | p = 0.830 |
| Radiotherapy | ||||
| RT technique IMRT | 89 (99%) | 46 (100%) | 43 (98%) | |
| RT technique other | 1 (1%) | 0 (0) | 1 (2%) | |
| median dose (Gy; IQR) | 60 (50, 60) | 60 (43, 60) | 60 (60, 60) | p = 0.024 |
| pts. receiving ≥ 90% of prescribed dose | 82 (91%) | 43 (93%) | 39 (89%) | p = 0.480 |
| contouring approach EORTC | 46 (51%) | 30 (65%) | 16 (36%) | p = 0.011 |
| contouring approach RTOG | 43 (48%) | 16 (35%) | 27 (62%) | |
| contouring unknown | 1/90 (1%) | 0/46 (0) | 1/44 (2%) | |
| Chemoradiotherapy (Stupp regimen) | ||||
| No. of patients | 64 (71%) | 28 (61%) | 36 (82%) | p = 0.037 |
| median (days; IQR) | 42 (30, 45) | 41.5 (23, 43) | 43 (39, 46) | p = 0.095 |
| corticosteroids use | 62 (69%) | 35 (76%) | 27 (61%) | p = 0.151 |
| Adjuvant chemotherapy | ||||
| No. of patients | 43 (48%) | 16 (35%) | 27 (61%) | p = 0.020 |
| No. of cycles: median (IQR) | 4.5 (2, 6) | 3.5 (1, 6) | 5 (3, 6) | p = 0.242 |
| No. of cycles: ≥ 3 | 32/43 (74%) | 8/16 (50%) | 24/27 (89%) | p = 0.016 |
| No. of cycles: ≥ 6 | 21/43 (49%) | 7/16 (44%) | 14/27 (52%) | p = 0.761 |
| Treatment after progression | ||||
| No. of patients | 42 | 22 | 20 | p > 0.999 |
| surgery | 7 (17%) | 4 (18%) | 3 (15%) | |
| surgery + chemoradiotherapy | 1 (2%) | 0 (0) | 1 (5%) | |
| surgery + chemotherapy | 8 (19%) | 2 (9%) | 6 (30%) | |
| chemotherapy | 18 (43%) | 13 (59%) | 5 (25%) | |
| reirradiation | 6 (14%) | 2 (9%) | 4 (20%) | |
| reirradiation + chemotherapy | 2 (5%) | 1 (5%) | 1 (5%) |
| REP (n = 46) | Non-REP (n = 44) | |||
|---|---|---|---|---|
| Median follow up31.9 (28.7, NA) | Median follow up 34.1 (32.9, NA) | |||
| Stupp regimen (n = 28) | RT (n = 18) | Stupp regimen (n = 36) | RT (n = 8) | |
| Overall survival | ||||
| Median (months) | 16.0 (10.2, 21.6) | 7.5 (4.8, 11.0) | 20.1 (13.6, 29.8) | 12.6 (8.0, NA) |
| 1-year | 59.3 (43.4, 81.1) | 16.7 (5.9, 46.8) | 72.2 (59.0, 88.4) | 50.0 (25.0, 100.0) |
| 2-year | 22.3 (11.0, 45.1) | 5.6 (0.8, 37.3) | 40.8 (27.3, 60.9) | 25.0 (7.5, 83.0) |
| 3-year | 9.3 (1.9, 45.7) | 5.6 (0.8, 37.3) | 22.9 (11.9, 44.1) | 0.0 (NA, NA) |
| Progression-free survival | ||||
| Median (months) | 4.1 (3.2, 7.1) | 2.8 (2.4, 4.3) | 8.8 (5.8, 11.5) | 5.0 (4.2, NA) |
| 1-year | 11.2 (3.8, 32.4) | 5.6 (0.8, 37.3) | 27.8 (16.4, 47.0) | 37.5 (15.3, 91.7) |
| 2-year | 7.4 (2.0, 28.2) | 0.0 (NA, NA) | 5.6 (1.4, 21.4) | 12.5 (2.0, 78.2) |
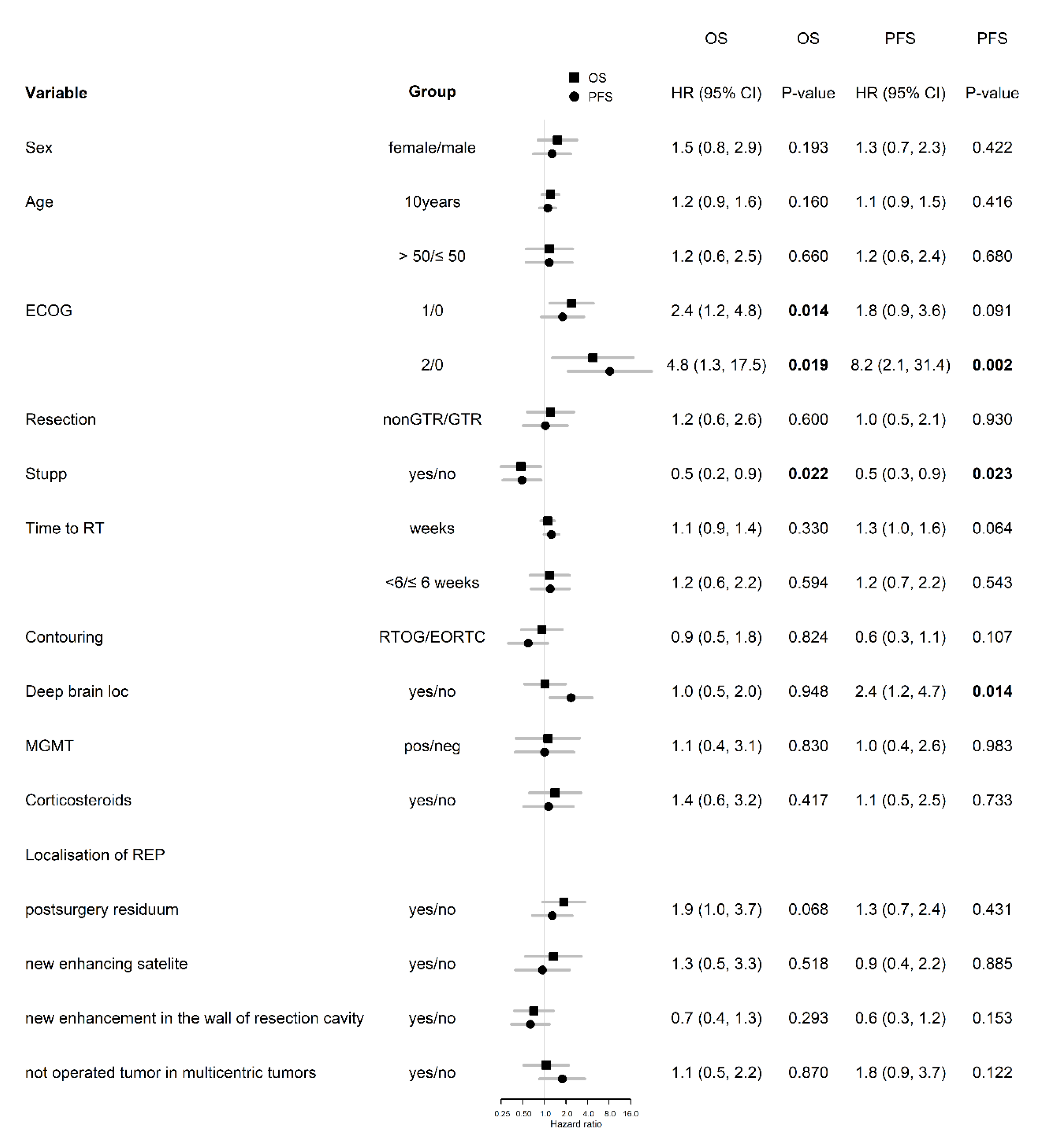
| OS | PFS | ||||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Performance status (ECOG) | 1/0 | 2.3 (1.1,4.5) | 0.033 | ||
| 2/0 | 16.6 (3.9,70) | <0.001 | |||
| Extent of resection | non-GTR/GTR | 2.2 (0.9,5.2) | 0.088 | ||
| Stupp regimen | yes/no | 0.3 (0.1,0.7) | 0.003 | ||
| deep brain location | yes/no | 3.1 (1.5,6.7) | 0.003 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakomy, R.; Kazda, T.; Selingerova, I.; Poprach, A.; Pospisil, P.; Belanova, R.; Fadrus, P.; Smrcka, M.; Vybihal, V.; Jancalek, R.; et al. Pre-Radiotherapy Progression after Surgery of Newly Diagnosed Glioblastoma: Corroboration of New Prognostic Variable. Diagnostics 2020, 10, 676. https://doi.org/10.3390/diagnostics10090676
Lakomy R, Kazda T, Selingerova I, Poprach A, Pospisil P, Belanova R, Fadrus P, Smrcka M, Vybihal V, Jancalek R, et al. Pre-Radiotherapy Progression after Surgery of Newly Diagnosed Glioblastoma: Corroboration of New Prognostic Variable. Diagnostics. 2020; 10(9):676. https://doi.org/10.3390/diagnostics10090676
Chicago/Turabian StyleLakomy, Radek, Tomas Kazda, Iveta Selingerova, Alexandr Poprach, Petr Pospisil, Renata Belanova, Pavel Fadrus, Martin Smrcka, Vaclav Vybihal, Radim Jancalek, and et al. 2020. "Pre-Radiotherapy Progression after Surgery of Newly Diagnosed Glioblastoma: Corroboration of New Prognostic Variable" Diagnostics 10, no. 9: 676. https://doi.org/10.3390/diagnostics10090676
APA StyleLakomy, R., Kazda, T., Selingerova, I., Poprach, A., Pospisil, P., Belanova, R., Fadrus, P., Smrcka, M., Vybihal, V., Jancalek, R., Kiss, I., Muckova, K., Hendrych, M., Knight, A., Sana, J., Slampa, P., & Slaby, O. (2020). Pre-Radiotherapy Progression after Surgery of Newly Diagnosed Glioblastoma: Corroboration of New Prognostic Variable. Diagnostics, 10(9), 676. https://doi.org/10.3390/diagnostics10090676