Azygos Lobe: Prevalence of an Anatomical Variant and Its Recognition among Postgraduate Physicians

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
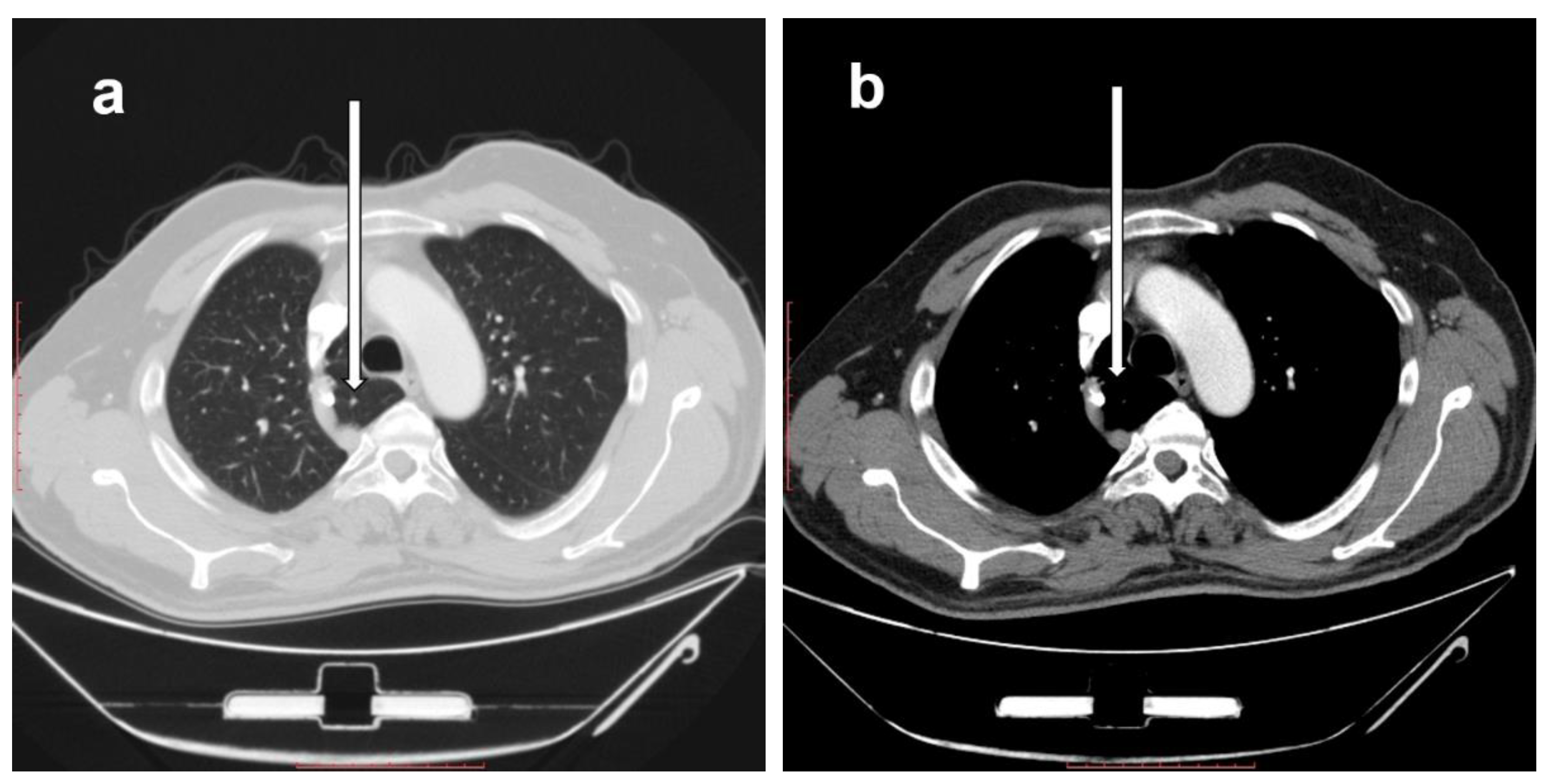
2.1. Prevalence of Right Azygos Lobe
2.2. Description of the Right Azygos Lobe
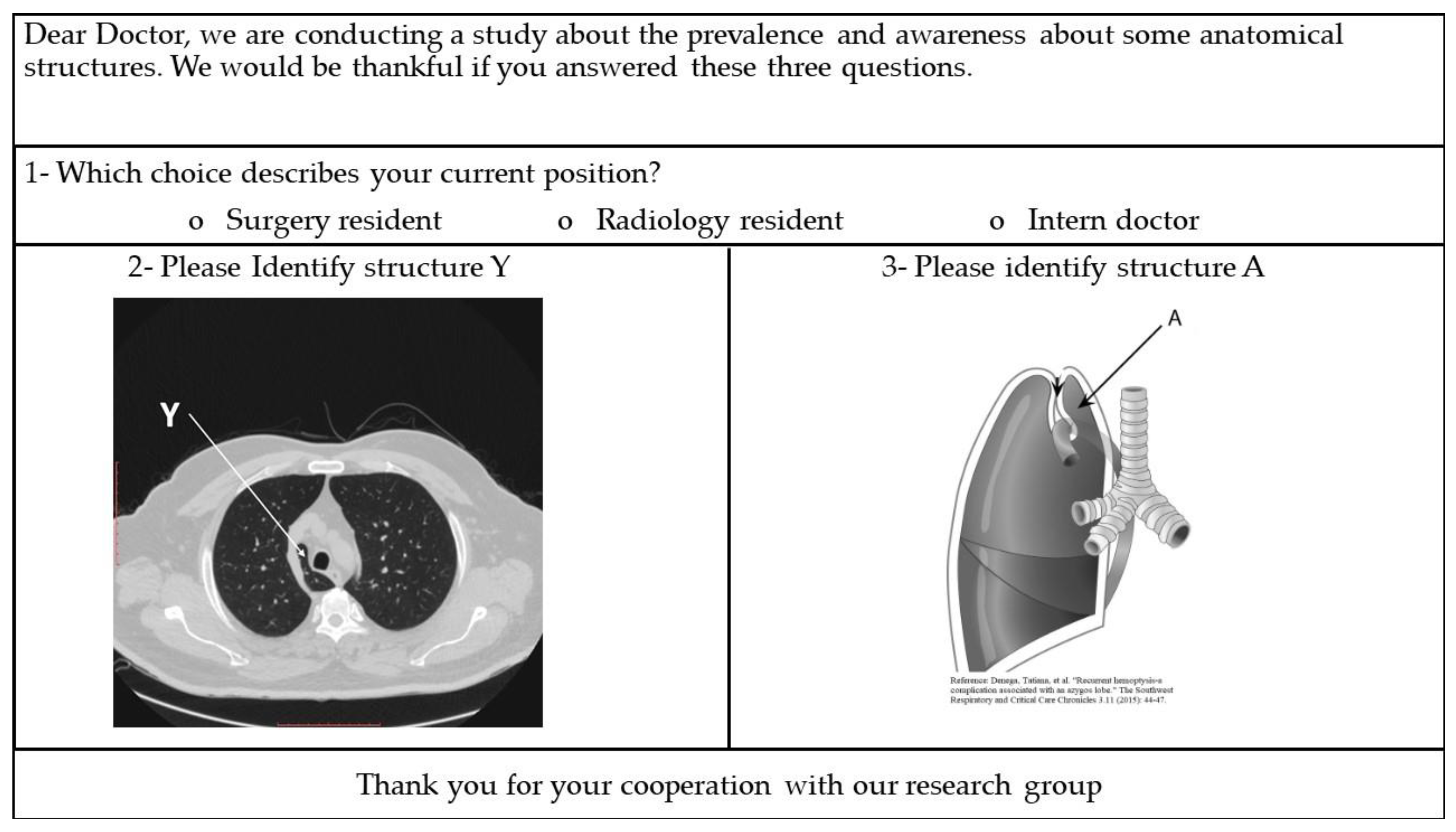
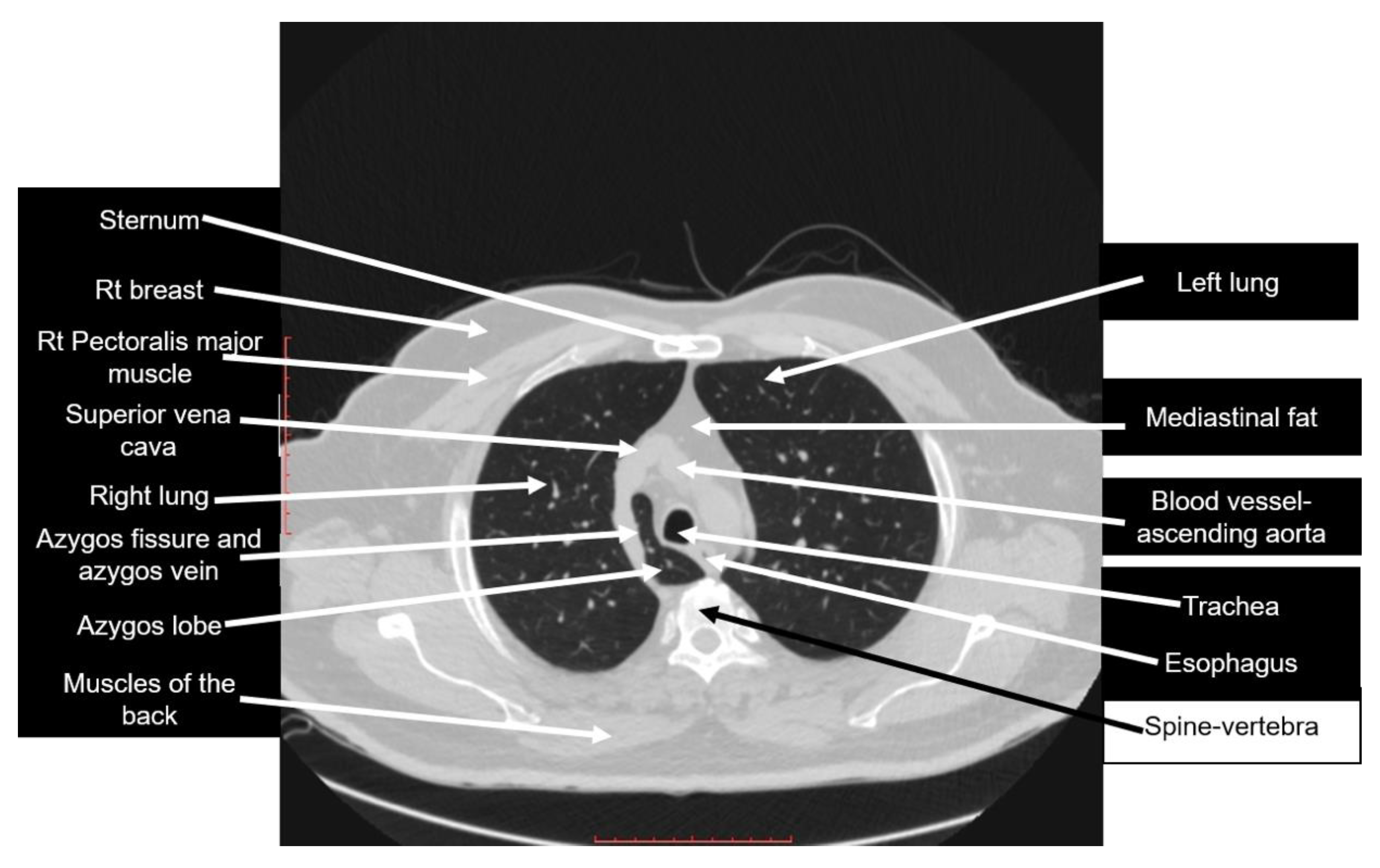
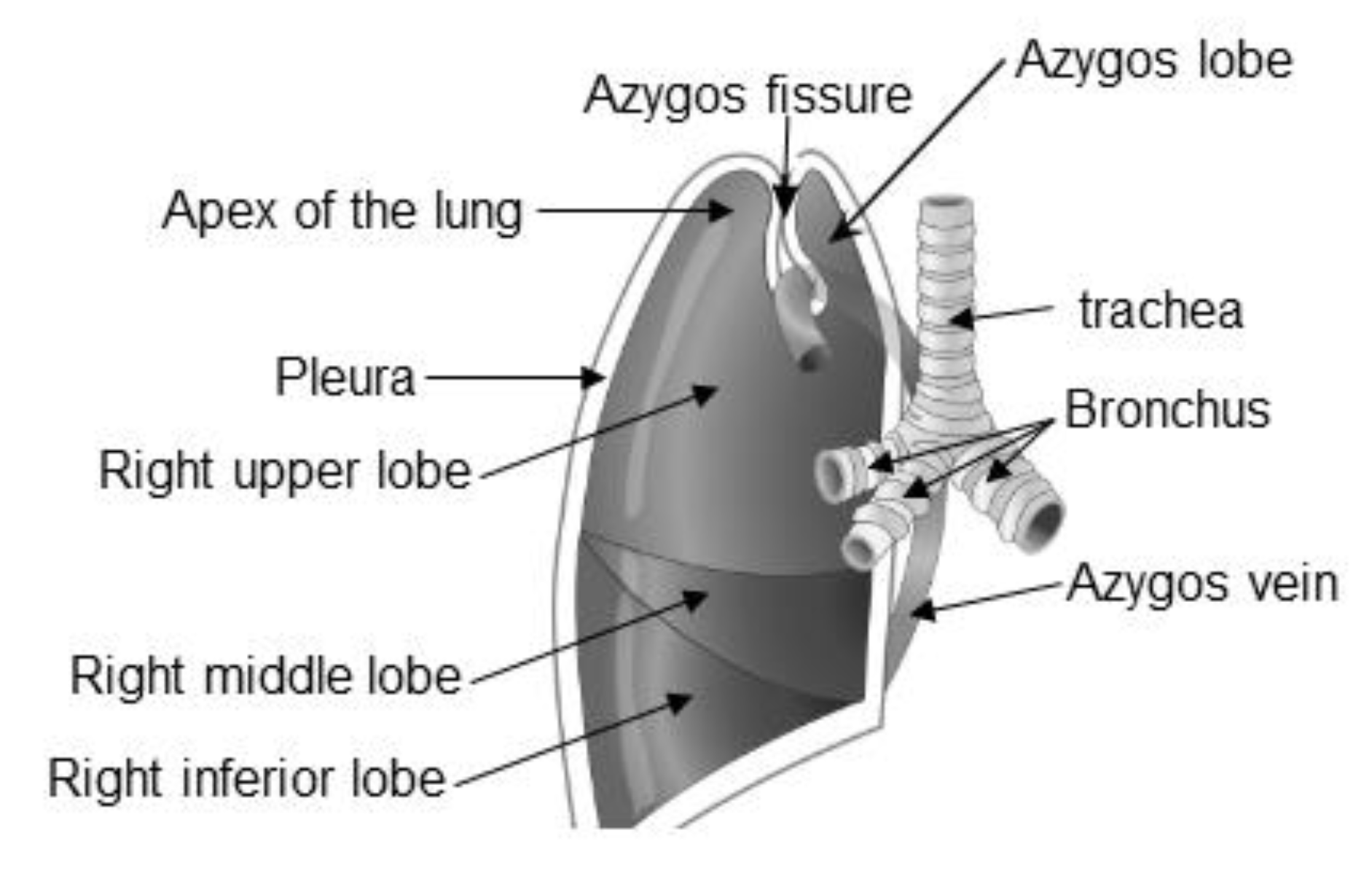
2.3. Identifying the Right Azygos Lobe Using CT and Anatomy Images
3. Results
3.1. The Prevalence of the Right Azygos Lobe
3.2. Knowledge of Postgraduate Physicians about the Right Azygos Lobe
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Caceres, J.; Mata, J.M.; Andreu, J. The azygos lobe: Normal variants that may simulate disease. Eur. J. Radiol. 1998, 27, 15–20. [Google Scholar] [CrossRef]
- Imsirovic, B.; Mekic-Abazovic, A.; Omerhodzic, I.; Zerem, E.; Vegar-Zubović, S. Atypical localization of lung cancer located in lobus v. azygos. Med. Glas. (Zenica) 2012, 9, 408–411. [Google Scholar] [PubMed]
- Kotov, G.; Dimitrova, I.N.; Iliev, A.; Groudeva, V. A Rare Case of an Azygos Lobe in the Right Lung of a 40-year-old Male. Cureus 2018, 10, e2780. [Google Scholar] [CrossRef]
- Pradhan, G.; Sahoo, S.; Mohankudo, S.; Dhanurdhar, Y.; Jagaty, S.K. Azygos lobe-a rare anatomical variant. J. Clin. Diagn. Res. 2017, 11, TJ02. [Google Scholar] [CrossRef]
- Akhtar, J.; Lal, A.; Martin, K.B.; Popkin, J. Azygos lobe: A rare cause of right paratracheal opacity. Respir. Med. Case Rep. 2018, 23, 136–137. [Google Scholar] [CrossRef] [PubMed]
- Felson, B. The azygos lobe: Its variation in health and disease. Semin. Roentgenol. 1989, 24, 56–66. [Google Scholar] [CrossRef]
- Chabot-Naud, A.; Rakovich, G.; Chagnon, K.; Ouellette, D.; Beauchamp, G. A curious lobe. Can. Respir. J. 2011, 18, 79–80. [Google Scholar] [CrossRef] [PubMed]
- Munn, S. Pseudoazygos lobe caused by lymph node pneumatocele. J. Thorac. Imaging 2002, 17, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, G.G.; Gandhi, M.S.; Gandhi, S.D. Excessive anteriorisation of the superior vena cava associated with an azygos lobe. Surg. Radiol. Anat. 1995, 17, 173–175. [Google Scholar] [CrossRef] [PubMed]
- Arslan, G.; Çubuk, M.; Özkaynak, C.; Sindel, T.; Lüleci, E. Intrapulmonary right brachiocephalic vein associated with azygos lobe. Clin. Imaging 2000, 24, 84–85. [Google Scholar] [CrossRef]
- Eradi, B.; Cusick, E. Azygos lobe associated with esophageal atresia: A trap for the unwary. J. Pediatr. Surg. 2005, 40, e11–e12. [Google Scholar] [CrossRef] [PubMed]
- Sadikot, R.T.; Cowen, M.E.; Arnold, A.G. Spontaneous pneumothorax in a patient with an azygos lobe. Thorax 1997, 52, 579–580; discussion 5–6. [Google Scholar] [CrossRef] [PubMed]
- Rauf, A.; Rauf, W.U.; Navsa, N.; Ashraf, K.T.A. Azygos lobe in a South African cadaveric population. Clin. Anat. 2012, 25, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Reisfeld, R. Azygos lobe in endoscopic thoracic sympathectomy for hyperhidrosis. Surg. Endosc. 2005, 19, 964–966. [Google Scholar] [CrossRef] [PubMed]
- Möller, T.B.; Reif, E. Pocket Atlas of Sectional Anatomy: Computed Tomography and Magnetic Resonance Imaging; Volume II: Thorax, Heart, Abdomen and Pelvis, 4th ed.; Thieme Medical Publishers: Stuttgart, Germany, 2007. [Google Scholar]
- Leslie, K. Survey Sampling, 1st ed.; John Wiley and Sons Inc.: New York, NY, USA, 1965; pp. 87–91. [Google Scholar]
- Denega, T.; Alkul, S.; Islam, E.; Alalawi, R. Recurrent hemoptysis-a complication associated with an azygos lobe. Southwest Respir. Crit. Care Chron. 2015, 3, 44–47. [Google Scholar]
- Özdemir, L.; Özdemir, B.; Duman, T. Prevalence of an azygos lobe using thoracic computed tomography. Cyprus J. Med. Sci. 2016, 1, 55–57. [Google Scholar] [CrossRef]
- Asai, K.; Urabe, N.; Takeichi, H. Spontaneous pneumothorax and a coexistent azygos lobe. Jpn. J. Thorac. Cardiovasc. Surg. 2005, 53, 604–606. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men | Women | Total | |
|---|---|---|---|
| Total number of patients (n) | 908 | 801 | 1709 |
| Cases with an azygos lobe (n) | 10 | 5 | 15 |
| Prevalence (%) | 1.01 | 0.62 | 0.88 |
| Type | Intern Doctors | Surgery Residents | Radiology Residents | |
|---|---|---|---|---|
| Total number of physicians in the teaching hospital (n) | 309 | 39 | 31 | |
| Total number of physicians who responded to the survey n (%) a | 173 (56.0) | 26 (66.7) | 28 (90.3) | |
| Correct answer n (%) b | CT scan | 0 (0.0) | 0 (0.0) | 16 (57.1) |
| Anatomy | 0 (0.0) | 0 (0.0) | 16 (57.1) | |
| Incorrect answer n (%) b | CT scan | 18 (10.4) | 12 (46.2) | 6 (21.4) |
| Anatomy | 7 (4.05) | 7 (26.9) | 3 (10.7) | |
| No answer n (%) b | CT scan | 155 (89.6) | 14 (53.8) | 6 (21.4) |
| Anatomy | 166 (96.0) | 19 (73.1) | 9 (32.1) | |
| Incorrect Answers about the CT Image | Incorrect Answers about the Anatomy Figure | ||||
|---|---|---|---|---|---|
| Structure | N | % | Structure | N | % |
| Bronchus/right bronchus/right pulmonary bronchus/right main bronchus | 9 | 25.0 | Apex of the lung or right lung apex | 3 | 17.7 |
| Aortic arch | 4 | 11.1 | Superior vena cava | 3 | 17.7 |
| Pulmonary trunk | 4 | 11.1 | Avascular ring | 2 | 11.8 |
| Superior vena cava | 3 | 8.33 | Pleura | 1 | 5.88 |
| Esophagus | 3 | 8.33 | Azygous fissure | 1 | 5.88 |
| Inferior vena cava | 3 | 8.33 | Apical lung | 1 | 5.88 |
| Trachea | 2 | 5.56 | Bronchus/right bronchus/right pulmonary bronchus/right main bronchus | 1 | 5.88 |
| Lung | 2 | 5.56 | Aortic arch | 1 | 5.88 |
| Avascular ring | 2 | 5.56 | Right upper lobe | 1 | 5.88 |
| Apex of the lung or right lung apex | 1 | 2.78 | Lingula | 1 | 5.88 |
| Azygous fissure | 1 | 2.78 | Right lung | 1 | 5.88 |
| Apical lung | 1 | 2.78 | Circulating aorta | 1 | 5.88 |
| Right upper lobe | 1 | 2.78 | |||
| Total | 36 | 100.00 | 17 | 100.00 | |
| Structure | CT-Based Description |
|---|---|
| Bronchus | For its location, please refer to the labeling in Figure 3 |
| Aortic arch | In the provided image, it is not seen as a complete arch, as the level of this image is at its most inferior aspect |
| Pulmonary trunk | Not seen, as it is just above the level of the provided CT image |
| Superior vena cava | For its location, please refer to the labeling in Figure 3 |
| Esophagus | A posterior mediastinal structure; for its location, please refer to the labeling in Figure 3 |
| Inferior vena cava | Cannot be in the same image; seen at the level of diaphragm |
| Trachea | For its location, please refer to the labeling in Figure 3 |
| Lung | This answer is correct, but because it was not specific, it was considered an incorrect answer |
| Avascular ring | There is no such anatomical term; one possibility could be that the doctor meant a vascular ring, which is a vascular anomaly of the aortic arch system; vascular rings are not present in Figure 3 |
| Apex of the right lung | The apex of the lung is not shown in Figure 3 |
| Azygous fissure | For its location, please refer to the labeling in Figure 3 |
| Apical lung | There is no such anatomical term; it seems that the doctor meant the apex of the lung, which is not shown in Figure 3 |
| Right upper lobe | This answer is correct, but because it was not specific, it was considered an incorrect answer |
| Structure | Anatomy Figure-Based Description |
|---|---|
| Apex of the lung | For its usual location, please refer to the labeling in Figure 4. |
| Superior vena cava | The superior vena cava is not shown in Figure 4 |
| Avascular ring | There is no such anatomical term; one possibility could be that the doctor meant a vascular ring, which is the vascular anomaly of the aortic arch system; vascular rings are not shown in Figure 4 |
| Pleura | For its usual location, please refer to the labeling in Figure 4 |
| Azygous fissure | For its usual location, please refer to the labeling in Figure 4 |
| Apical lung | There no such anatomical term; it seems that the doctor meant the apex of the lung, which is labeled in Figure 4 |
| Bronchus | For its usual location, please refer to the labeling in Figure 4 |
| Aortic arch | The aortic arch is not shown in Figure 4 |
| Right upper lobe | This answer is correct, but because it was not specific, it was considered an incorrect answer; please refer to the labeling in Figure 4 |
| Lingula | The ligula is a tongue-like structure near the base of the left lung; Figure 4 is an image of a right lung |
| Right lung | The answer is correct, but because it was not specific, it was considered an incorrect answer |
| Circulating aorta | The aorta is not shown in Figure 4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Mnayyis, A.; Al-Alami, Z.; Altamimi, N.; Alawneh, K.Z.; Aleshawi, A. Azygos Lobe: Prevalence of an Anatomical Variant and Its Recognition among Postgraduate Physicians. Diagnostics 2020, 10, 470. https://doi.org/10.3390/diagnostics10070470
Al-Mnayyis A, Al-Alami Z, Altamimi N, Alawneh KZ, Aleshawi A. Azygos Lobe: Prevalence of an Anatomical Variant and Its Recognition among Postgraduate Physicians. Diagnostics. 2020; 10(7):470. https://doi.org/10.3390/diagnostics10070470
Chicago/Turabian StyleAl-Mnayyis, Asma’a, Zina Al-Alami, Neveen Altamimi, Khaled Z. Alawneh, and Abdelwahab Aleshawi. 2020. "Azygos Lobe: Prevalence of an Anatomical Variant and Its Recognition among Postgraduate Physicians" Diagnostics 10, no. 7: 470. https://doi.org/10.3390/diagnostics10070470
APA StyleAl-Mnayyis, A., Al-Alami, Z., Altamimi, N., Alawneh, K. Z., & Aleshawi, A. (2020). Azygos Lobe: Prevalence of an Anatomical Variant and Its Recognition among Postgraduate Physicians. Diagnostics, 10(7), 470. https://doi.org/10.3390/diagnostics10070470