Video Laryngoscopic Intubation Using the King VisionTM Laryngoscope in a Simulated Cervical Spine Trauma: A Comparison Between Non-Channeled and Channeled Disposable Blades



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Procedures
2.3. Study Outcomes
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Boehringer, B.; Choate, M.; Hurwitz, S.; Tilney, P.V.; Judge, T. Impact of video laryngoscopy on advanced airway management by critical care transport paramedics and nurses using the CMAC pocket monitor. BioMed. Res. Int. 2015, 2015, 821302. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Wilson, M.E. Orotracheal intubation in patients with potential cervical spine injuries. Anaesthesia 1993, 48, 630–633. [Google Scholar] [CrossRef] [PubMed]
- Kill, C.; Risse, J.; Wallot, P.; Seidl, P.; Steinfeldt, T.; Wulf, H. Videolaryngoscopy with glidescope reduces cervical spine movements in patients with unsecured cervical spine. J. Emerg. Med. 2013, 44, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Suppan, L.; Tramer, M.R.; Niquille, M.; Grosgurin, O.; Marti, C. Alternative intubation techniques vs Macintosh laryngoscopy in patients with cervical spine immobilization: Systematic review and meta-analysis of randomized controlled trials. Br. J. Anaesth 2016, 116, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: A multicentre randomized controlled trial. Br. J. Anaesth 2016, 116, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Akihisa, Y.; Maruyama, K.; Koyama, Y.; Yamada, R.; Ogura, A.; Andoh, T. Comparison of intubation performance between the King Vision and Macintosh laryngoscopes in novice personnel: A randomized, crossover manikin study. J. Anesth. 2014, 28, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Kriege, M.; Alflen, C.; Noppens, R.R. Using King Vision video laryngoscope with a channeled blade prolongs time for tracheal intubation in different training levels, compared to non-channeled blade. Plos ONE 2017, 12, e0183382. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, J.L.; McClure, S.F.; Johns, D. EMS intubation improves with King Vision video laryngoscopy. Prehosp. Emerg. Care 2015, 19, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Bradley, W.P.; Bain, C.; Mehra, R.; Symons, J. Scoring systems for videolaryngoscopes. Anaesth Intensive Care 2013, 41, 122. [Google Scholar] [PubMed]
- Levitan, R.M.; Ochroch, E.A.; Kush, S.; Shofer, F.S.; Hollander, J.E. Assesment of airway visualisation, validation of the percentage of glottic opening (POGO) scale. Acad. Emerg. Med. 1998, 5, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Cormack, R.S.; Lehane, L. Difficult tracheal intubation in obstetrics. Anaesthesia 1984, 39, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Okada, D.; Komasawa, N.; Fujiwara, S.; Minami, T. Comparison of tube-guided and guideless videolaryngoscope for tracheal intubation during chest compression in a manikin: A randomized crossover trial. J. Anesth 2015, 29, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Murphy, L.D.; Kovacs, G.J.; Reardon, P.M.; Law, J.A. Comparison of the king vision video laryngoscope with the macintosh laryngoscope. J. Emerg Med. 2014, 47, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Shravanalakshmi, D.; Bidkar, P.U.; Narmadalakshmi, K.; Lata, S.; Mishra, S.K.; Adinarayanan, S. Comparison of intubation success and and glottic visualization using King Vision and C-MAC videolaryngoscopes in patients with cervical immobilization: A randomized clinical trial. Surg. Neurol. Int. 2017, 8, 19. [Google Scholar] [PubMed]
- El-Tahan, M.R.; El Kenany, S.; Khidr, A.M.; Al Ghamdi, A.A.; Tawfik, A.M.; Al Mulhim, A.S. Cervical spine motion during tracheal intubation with King VisionTM video laryngoscopy and conventional laryngoscopy: A crossover randomized study. Minerva Anestesiol 2017, 83, 1152–1160. [Google Scholar] [PubMed]
- Aleksandrowicz, D.; Wieczorek, A.; Gaszynski, T. Intubation with cervical spine immobilisation: A comparison between the KingVision videolaryngoscope and the Macintosh laryngoscope. Eur. J. Anaesthesiol. 2018, 35, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Reviriego-Agudo, L.; de Togores-Lopez, A.R.; Charco-Mora, P. The significance and weight of manikin studies in airway management. Trends Anaesth. Crit. Care 2018, 21, 43–46. [Google Scholar] [CrossRef]
- Burnett, A.M.; Frascone, R.J.; Wewerka, S.S.; Kealey, S.E.; Evens, Z.N.; Griffith, K.R.; Salzman, J.G. Comparison of success rates between two video laryngoscope systems used in a prehospital clinical trial. Prehosp. Emerg. Care 2014, 18, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Escott, M.E.; Gleisberg, G.R.; Gillum, L.S.; Kosper, J.; Traynor, K.M.; Aulbert, L.; Vartanian, L.; Jenks, S.P.; Monroe, B.J. Seeing the difference. Deploying the video laryngoscope into a ground EMS system. J. Emerg. Medic Serv. 2014, 39, 34–39. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Gender | ||
| Males | 26 | 55 |
| Females | 32 | 45 |
| Level of training | ||
| Less than 1 year | 13 | 22 |
| 1–2 years | 12 | 21 |
| 2–3 years | 18 | 31 |
| 3–5 years | 11 | 19 |
| More than 5 years | 4 | 7 |
| Experience in videolaryngoscopy | ||
| None | 5 | 9 |
| 1–10 intubations | 27 | 46 |
| 11–50 intubations | 19 | 37 |
| 51–100 intubations | 4 | 7 |
| More than 100 intubations | 3 | 5 |
| Parameter | Non-Channeled Blade | Channeled Blade | p |
|---|---|---|---|
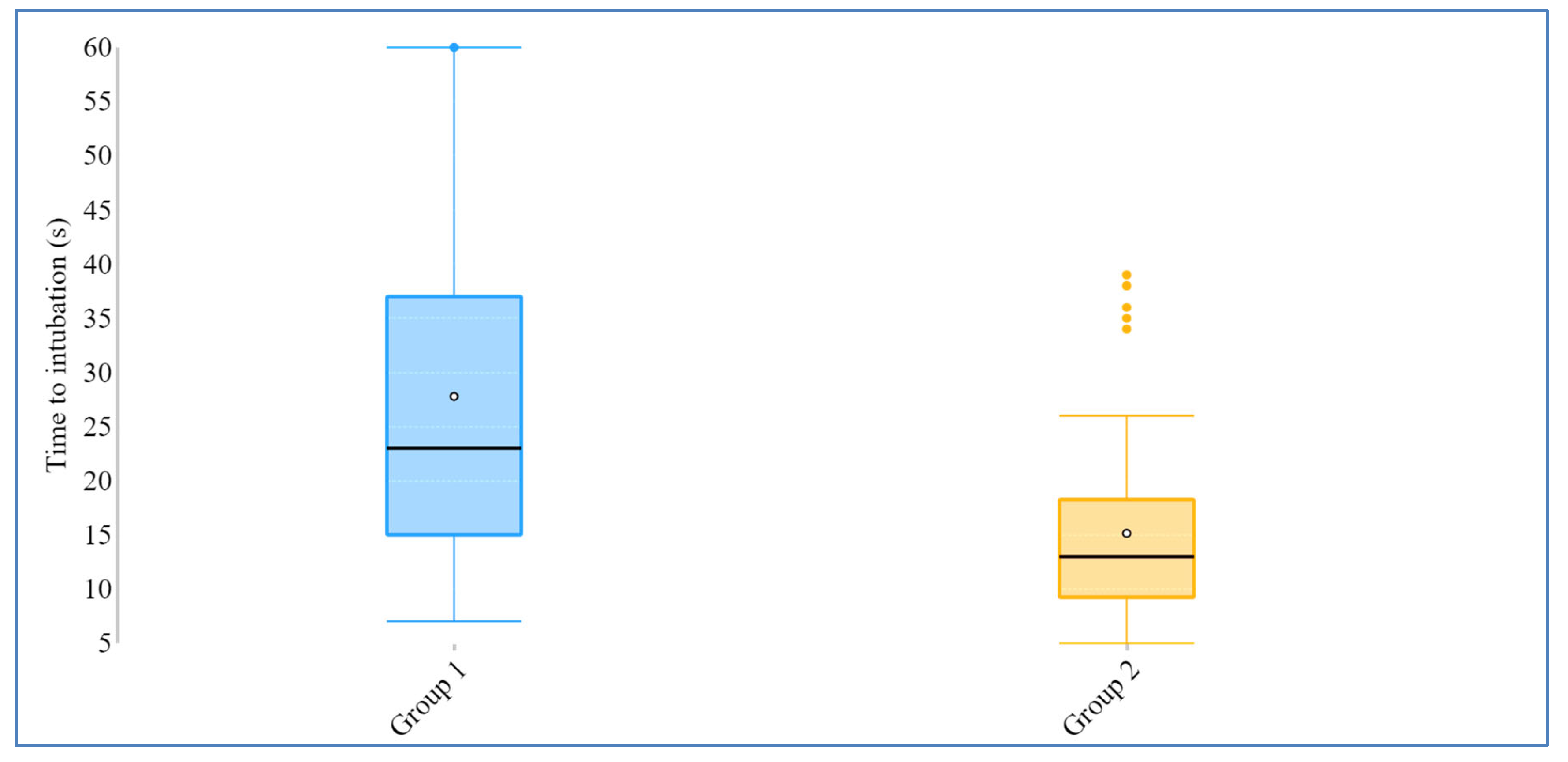
| Time to intubation (s) | 23 (7–91) [14.5–37.5] | 13 (5–39) [9–19] | <0.001 * |
| Time to visualization (s) | 8 (3–26) [5.75–11] | 9 (4–36) [6–12] | 0.54 |
| Time to ventilation (s) | 29 (13–99) [21.5–45] | 20 (12–46) [16.75–26] | <0.001 * |
| Total success rate (%) | 98.3 | 100 | 1.00 |
| Number of attempts | 1 (1–4) [1–2] | 1 (1–2) [1] | <0.001 * |
| /Mean ± SD/ | /1.52 ± 0.7/ | /1.05 ± 0.22/ | |
| Percentage of glottic opening | 2 (1–5) [2–3] | 2 (1–4)[1.75–2] | 0.055 |
| Cormack–Lehane score | 1 (1–2)[1–1] | 1 (1–2)[1–1] | 0.42 |
| Parameter | Non-Channeled Blade | Channeled Blade |
|---|---|---|
| p | ||
| Quality of visualization | 2 (1–4) [1–2] | 2 (1–4) [1–2] |
| 0.47 | ||
| Ease of intubation | 3 (1–5) [2–4] | 1 (1–4) [1–2] |
| <0.001 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Votruba, J.; Brozek, T.; Blaha, J.; Henlin, T.; Vymazal, T.; Donaldson, W.; Michalek, P. Video Laryngoscopic Intubation Using the King VisionTM Laryngoscope in a Simulated Cervical Spine Trauma: A Comparison Between Non-Channeled and Channeled Disposable Blades. Diagnostics 2020, 10, 139. https://doi.org/10.3390/diagnostics10030139
Votruba J, Brozek T, Blaha J, Henlin T, Vymazal T, Donaldson W, Michalek P. Video Laryngoscopic Intubation Using the King VisionTM Laryngoscope in a Simulated Cervical Spine Trauma: A Comparison Between Non-Channeled and Channeled Disposable Blades. Diagnostics. 2020; 10(3):139. https://doi.org/10.3390/diagnostics10030139
Chicago/Turabian StyleVotruba, Jiri, Tomas Brozek, Jan Blaha, Tomas Henlin, Tomas Vymazal, Will Donaldson, and Pavel Michalek. 2020. "Video Laryngoscopic Intubation Using the King VisionTM Laryngoscope in a Simulated Cervical Spine Trauma: A Comparison Between Non-Channeled and Channeled Disposable Blades" Diagnostics 10, no. 3: 139. https://doi.org/10.3390/diagnostics10030139
APA StyleVotruba, J., Brozek, T., Blaha, J., Henlin, T., Vymazal, T., Donaldson, W., & Michalek, P. (2020). Video Laryngoscopic Intubation Using the King VisionTM Laryngoscope in a Simulated Cervical Spine Trauma: A Comparison Between Non-Channeled and Channeled Disposable Blades. Diagnostics, 10(3), 139. https://doi.org/10.3390/diagnostics10030139