Chemerin Is a Valuable Biomarker in Patients with HCV Infection and Correlates with Liver Injury


 and
and
Abstract

1. Introduction
2. Results
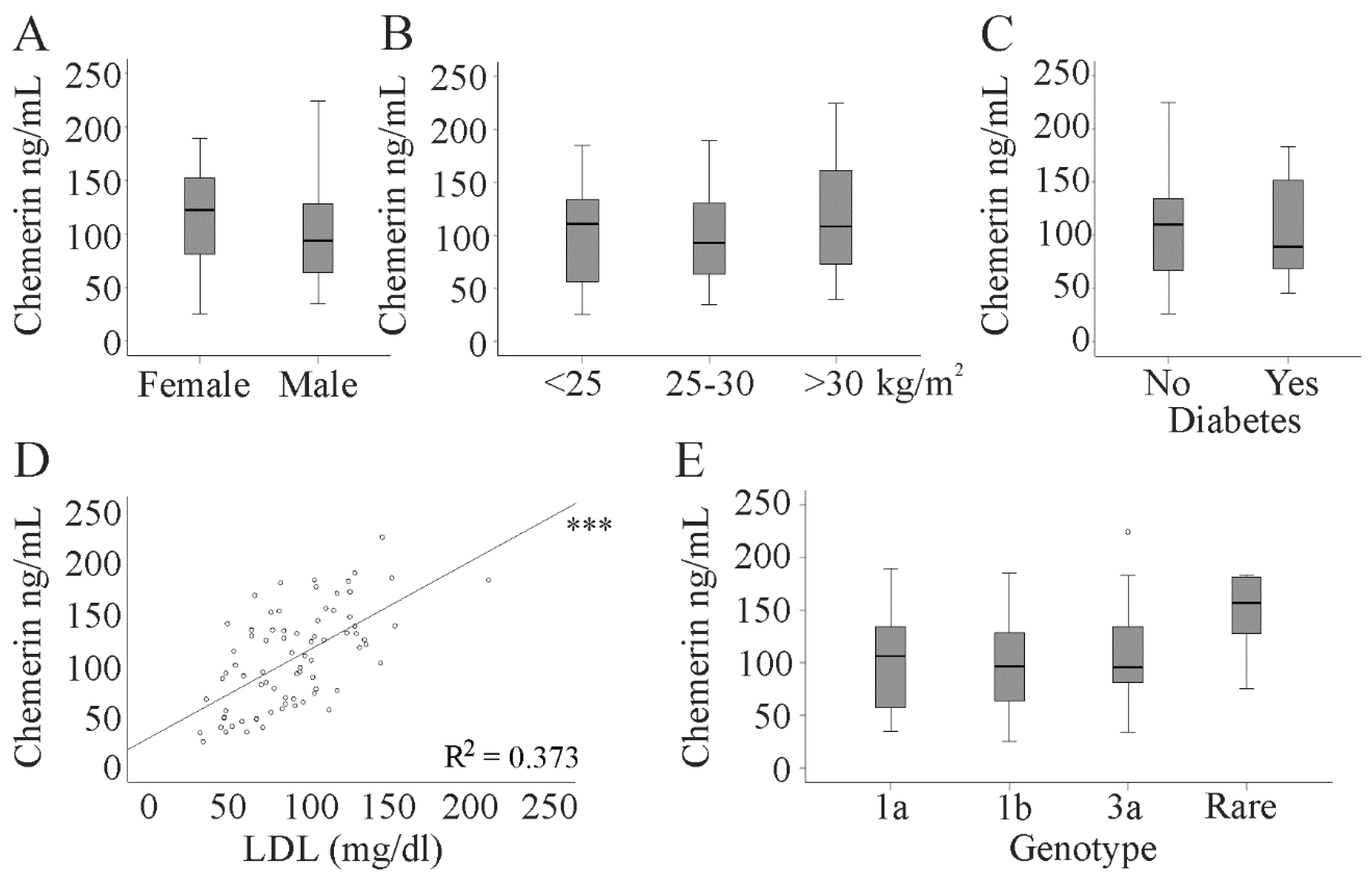
2.1. Serum Chemerin Levels in Patients with HCV
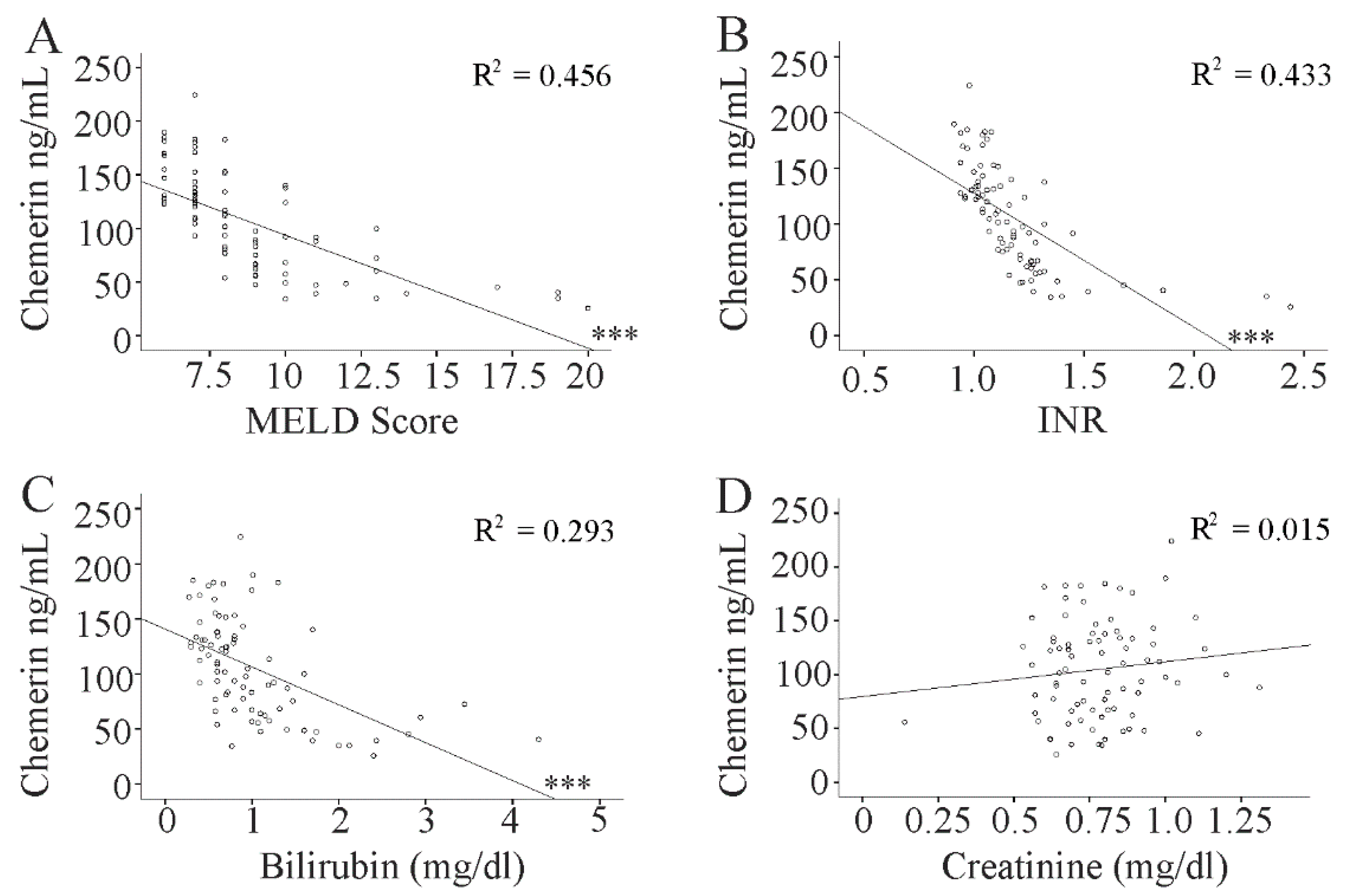
2.2. Association of Chemerin with the MELD Score
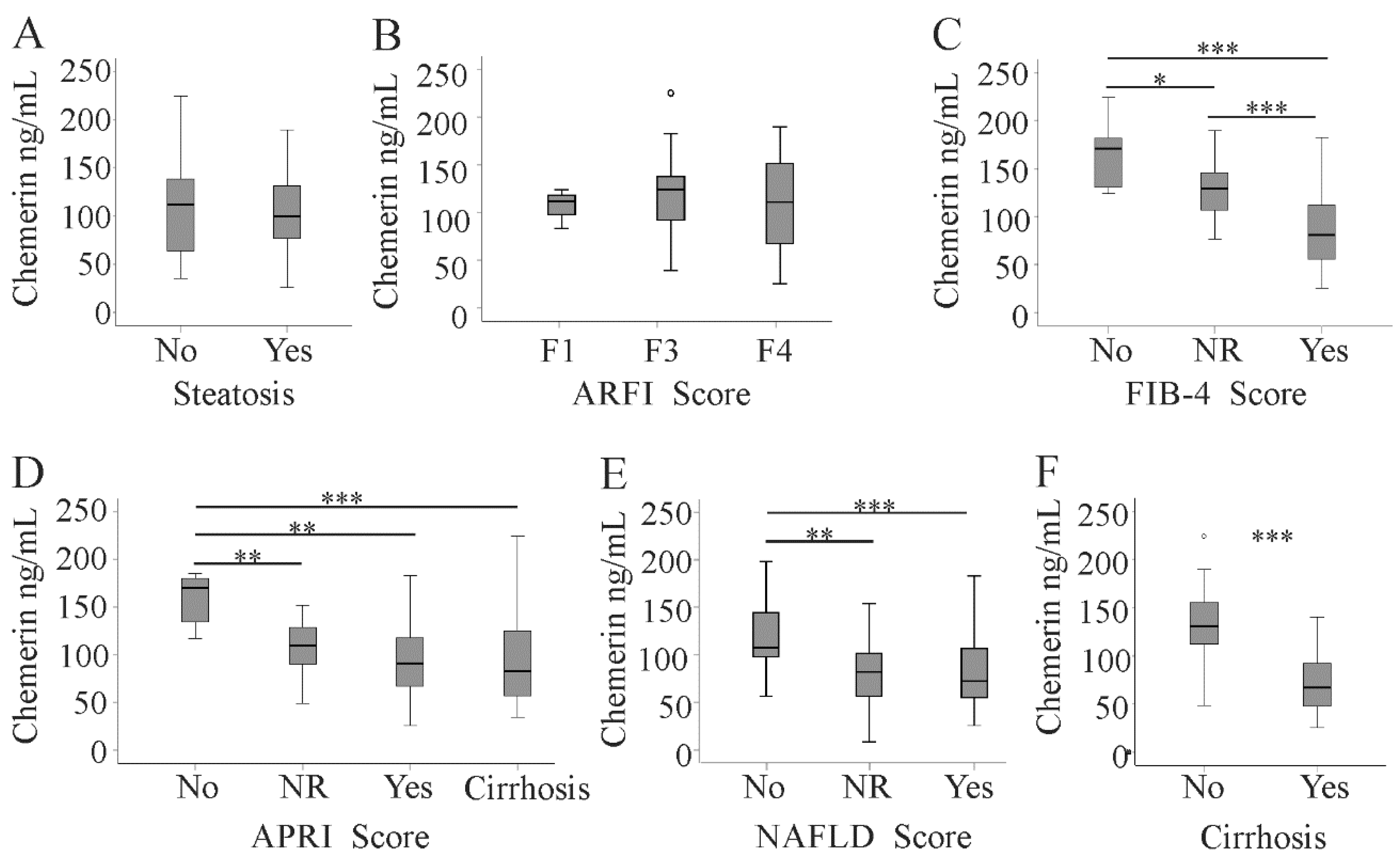
2.3. Serum Chemerin in Relation to Hepatic Steatosis and Liver Fibrosis
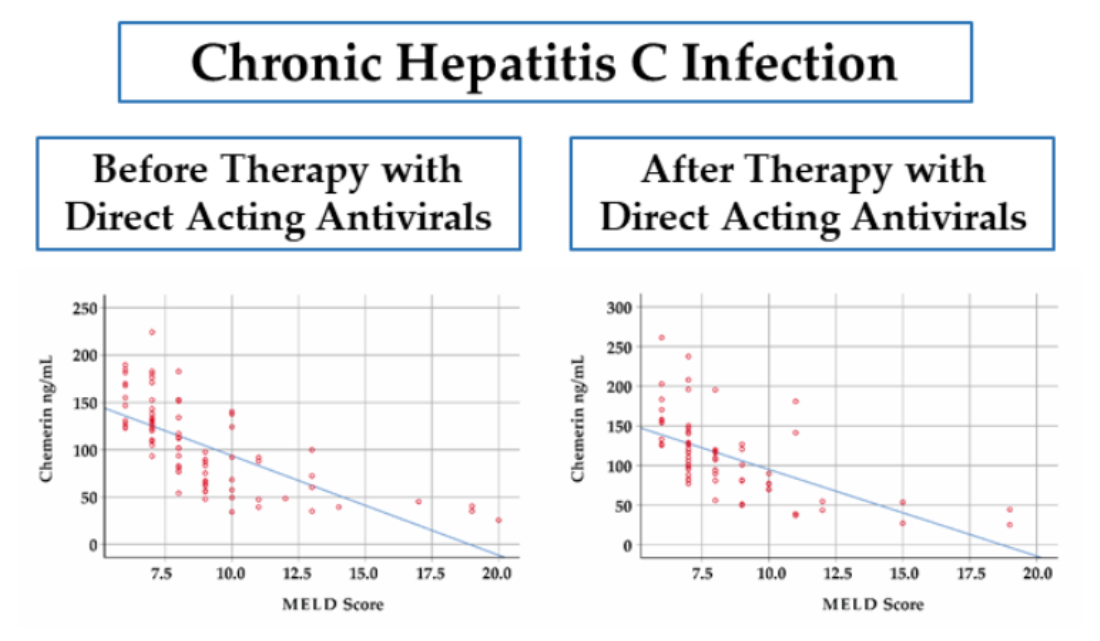
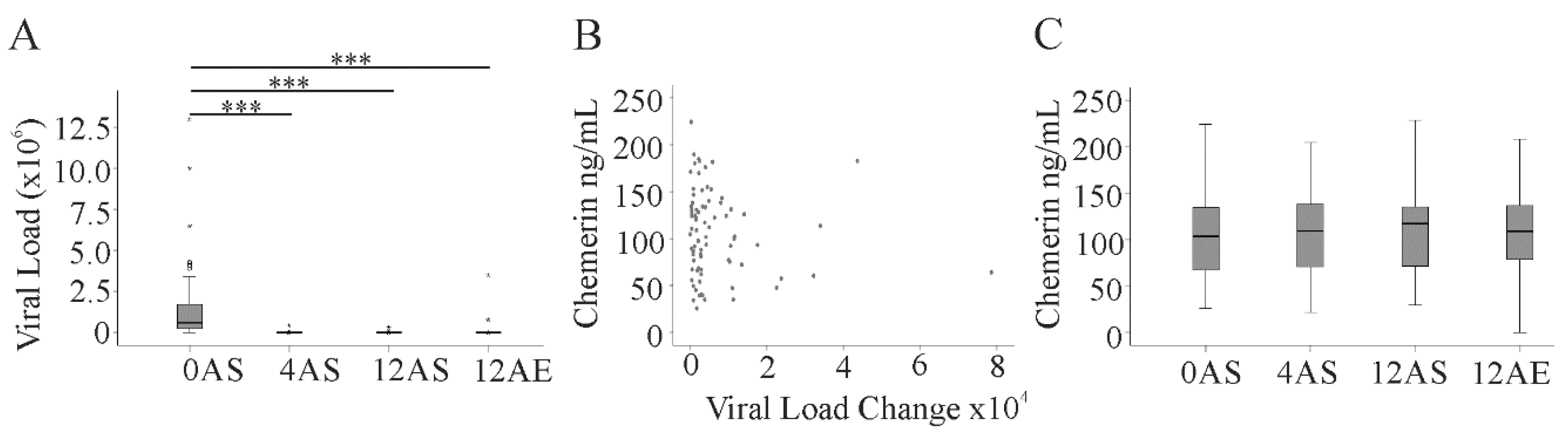
2.4. Effect of Direct-Acting Antivirals (DAAs) on Serum Chemerin during Therapy and up to 3 Months after the End of DAA Therapy
3. Discussion
4. Materials and Methods
4.1. Study Cohort
4.2. ELISA
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Casiraghi, M.A.; De Paschale, M.; Romano, L.; Biffi, R.; Assi, A.; Binelli, G.; Zanetti, A.R. Long-term outcome (35 years) of hepatitis C after acquisition of infection through mini transfusions of blood given at birth. Hepatology 2004, 39, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Roingeard, P. Hepatitis C virus diversity and hepatic steatosis. J. Viral Hepat. 2013, 20, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Charlton, M.R.; Pockros, P.J.; Harrison, S.A. Impact of obesity on treatment of chronic hepatitis C. Hepatology 2006, 43, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Buechler, C.; Feder, S.; Haberl, E.M.; Aslanidis, C. Chemerin Isoforms and Activity in Obesity. Int. J. Mol. Sci. 2019, 20, 1128. [Google Scholar] [CrossRef] [PubMed]
- Bozaoglu, K.; Bolton, K.; McMillan, J.; Zimmet, P.; Jowett, J.; Collier, G.; Walder, K.; Segal, D. Chemerin is a novel adipokine associated with obesity and metabolic syndrome. Endocrinology 2007, 148, 4687–4694. [Google Scholar] [CrossRef]
- Bozaoglu, K.; Segal, D.; Shields, K.A.; Cummings, N.; Curran, J.E.; Comuzzie, A.G.; Mahaney, M.C.; Rainwater, D.L.; VandeBerg, J.L.; MacCluer, J.W.; et al. Chemerin is associated with metabolic syndrome phenotypes in a Mexican-American population. J. Clin. Endocrinol. Metab. 2009, 94, 3085–3088. [Google Scholar] [CrossRef]
- Ernst, M.C.; Sinal, C.J. Chemerin: At the crossroads of inflammation and obesity. Trends Endocrinol. Metab. 2010, 21, 660–667. [Google Scholar] [CrossRef]
- Maghsoudi, Z.; Kelishadi, R.; Hosseinzadeh-Attar, M.J. Association of chemerin levels with anthropometric indexes and C-reactive protein in obese and non-obese adolescents. Arya Atheroscler. 2015, 11, 102–108. [Google Scholar]
- Stejskal, D.; Karpisek, M.; Hanulova, Z.; Svestak, M. Chemerin Is an Independent Marker of the Metabolic Syndrome in a Caucasian Population—A Pilot Study. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2008, 152, 217–221. [Google Scholar] [CrossRef]
- Weigert, J.; Neumeier, M.; Wanninger, J.; Filarsky, M.; Bauer, S.; Wiest, R.; Farkas, S.; Scherer, M.N.; Schaffler, A.; Aslanidis, C.; et al. Systemic chemerin is related to inflammation rather than obesity in type 2 diabetes. Clin. Endocrinol. (Oxf.) 2010, 72, 342–348. [Google Scholar] [CrossRef]
- Lorincz, H.; Katko, M.; Harangi, M.; Somodi, S.; Gaal, K.; Fulop, P.; Paragh, G.; Seres, I. Strong correlations between circulating chemerin levels and lipoprotein subfractions in nondiabetic obese and nonobese subjects. Clin. Endocrinol. (Oxf.) 2014, 81, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Shi, B.; Li, S. Association between serum chemerin concentrations and clinical indices in obesity or metabolic syndrome: A meta-analysis. PLoS ONE 2014, 9, e113915. [Google Scholar] [CrossRef] [PubMed]
- Eisinger, K.; Krautbauer, S.; Wiest, R.; Weiss, T.S.; Buechler, C. Reduced serum chemerin in patients with more severe liver cirrhosis. Exp. Mol. Pathol. 2015, 98, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Horn, P.; von Loeffelholz, C.; Forkert, F.; Stengel, S.; Reuken, P.; Aschenbach, R.; Stallmach, A.; Bruns, T. Low circulating chemerin levels correlate with hepatic dysfunction and increased mortality in decompensated liver cirrhosis. Sci. Rep. 2018, 8, 9242. [Google Scholar] [CrossRef]
- Krautbauer, S.; Wanninger, J.; Eisinger, K.; Hader, Y.; Beck, M.; Kopp, A.; Schmid, A.; Weiss, T.S.; Dorn, C.; Buechler, C. Chemerin is highly expressed in hepatocytes and is induced in non-alcoholic steatohepatitis liver. Exp. Mol. Pathol. 2013, 95, 199–205. [Google Scholar] [CrossRef]
- Buechler, C.; Haberl, E.M.; Rein-Fischboeck, L.; Aslanidis, C. Adipokines in Liver Cirrhosis. Int. J. Mol. Sci. 2017, 18, 1392. [Google Scholar] [CrossRef]
- Abdel-Messeih, P.L.; Mansour, H.H.; Ibrahim, D.R. Evaluation of chemerin and leptin in serum of chronic hepatitis C patients. Histol. Cell Biol. 2018, 1, 8–12. [Google Scholar]
- Kukla, M.; Zwirska-Korczala, K.; Gabriel, A.; Waluga, M.; Warakomska, I.; Szczygiel, B.; Berdowska, A.; Mazur, W.; Wozniak-Grygiel, E.; Kryczka, W. Chemerin, vaspin and insulin resistance in chronic hepatitis C. J. Viral Hepat. 2010, 17, 661–667. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address eee, Clinical Practice Guideline Panel C, Panel m, representative EGB. EASL Clinical Practice Guidelines: drug-induced liver injury. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Ho, S.Y.; Liu, P.H.; Hsu, C.Y.; Hsia, C.Y.; Su, C.W.; He, Y.J.; Lee, Y.H.; Huang, Y.H.; Hou, M.C.; Huo, T.I. Current noninvasive liver reserve models do not predict histological fibrosis severity in hepatocellular carcinoma. Sci. Rep. 2018, 8, 15074. [Google Scholar] [CrossRef] [PubMed]
- Ragazzo, T.G.; Paranagua-Vezozzo, D.; Lima, F.R.; de Campos Mazo, D.F.; Pessoa, M.G.; Oliveira, C.P.; Alves, V.A.F.; Carrilho, F.J. Accuracy of transient elastography-FibroScan(R), acoustic radiation force impulse (ARFI) imaging, the enhanced liver fibrosis (ELF) test, APRI, and the FIB-4 index compared with liver biopsy in patients with chronic hepatitis C. Clinics (Sao Paulo) 2017, 72, 516–525. [Google Scholar] [CrossRef]
- Asselah, T.; Rubbia-Brandt, L.; Marcellin, P.; Negro, F. Steatosis in chronic hepatitis C: Why does it really matter? Gut 2006, 55, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Heller, T.; Seeff, L.B. Viral load as a predictor of progression of chronic hepatitis C? Hepatology 2005, 42, 1261–1263. [Google Scholar] [CrossRef] [PubMed]
- Verna, E.C.; Morelli, G.; Terrault, N.A.; Lok, A.S.; Lim, J.K.; Di Bisceglie, A.M.; Zeuzem, S.; Landis, C.S.; Kwo, P.; Hassan, M.; et al. DAA therapy and long-term hepatic function in advanced/decompensated cirrhosis: Real-world experience from HCV-TARGET cohort. J. Hepatol. 2020, 73, 540–548. [Google Scholar] [CrossRef]
- Shawkey, A.; Ellakwa, D.; Emara, S.; El-Sabbagh, N. The role of chemerin and vaspin in Egyptian patients with viral hepatitis C. Meta Gene 2018, 18, 23–30. [Google Scholar] [CrossRef]
- Feder, S.; Kandulski, A.; Schacherer, D.; Weiss, T.S.; Buechler, C. Serum Chemerin Does Not Differentiate Colorectal Liver Metastases from Hepatocellular Carcinoma. Int. J. Mol. Sci. 2019, 20, 3919. [Google Scholar] [CrossRef]
- Foschi, F.G.; Domenicali, M.; Giacomoni, P.; Dall’Aglio, A.C.; Conti, F.; Borghi, A.; Bevilacqua, V.; Napoli, L.; Mirici, F.; Cucchetti, A.; et al. Is there an association between commonly employed biomarkers of liver fibrosis and liver stiffness in the general population? Ann. Hepatol. 2020, 19, 380–387. [Google Scholar] [CrossRef]
- Giuffre, M.; Fouraki, S.; Comar, M.; Masutti, F.; Croce, L.S. The Importance of Transaminases Flare in Liver Elastography: Characterization of the Probability of Liver Fibrosis Overestimation by Hepatitis C Virus-Induced Cytolysis. Microorganisms 2020, 8, 348. [Google Scholar] [CrossRef]
- Giuffre, M.; Fouraki, S.; Campigotto, M.; Colombo, A.; Visintin, A.; Buonocore, M.R.; Aversano, A.; Budel, M.; Tine, F.; Abazia, C.; et al. Alanine aminotransferase and spleno-portal dynamics affect spleen stiffness measured by point shear-wave elastography in patients with chronic hepatitis C in the absence of significant liver fibrosis. J. Ultrasound. 2020. [Google Scholar] [CrossRef]
- Li, H.; Huang, M.H.; Jiang, J.D.; Peng, Z.G. Hepatitis C: From inflammatory pathogenesis to anti-inflammatory/hepatoprotective therapy. World J. Gastroenterol. 2018, 24, 5297–5311. [Google Scholar] [CrossRef] [PubMed]
- Gastaldi, G.; Gomes, D.; Schneiter, P.; Montet, X.; Tappy, L.; Clement, S.; Negro, F. Treatment with direct-acting antivirals improves peripheral insulin sensitivity in non-diabetic, lean chronic hepatitis C patients. PLoS ONE 2019, 14, e0217751. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Li, L.; Hou, Z.; Zhang, Y.; Tang, Z.; Liu, S. Direct-acting Antiviral in the Treatment of Chronic Hepatitis C: Bonuses and Challenges. Int. J. Med. Sci. 2020, 17, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Yatsuhashi, H.; Abiru, S.; Yamasaki, K.; Komori, A.; Nagaoka, S.; Saeki, A.; Uchida, S.; Bekki, S.; Kugiyama, Y.; et al. Rapid Increase in Serum Low-Density Lipoprotein Cholesterol Concentration during Hepatitis C Interferon-Free Treatment. PLoS ONE 2016, 11, e0163644. [Google Scholar] [CrossRef]
- Alfadda, A.A. Circulating Adipokines in Healthy versus Unhealthy Overweight and Obese Subjects. Int. J. Endocrinol. 2014, 2014, 170434. [Google Scholar] [CrossRef] [PubMed]
- Gu, P.; Jiang, W.; Lu, B.; Shi, Z. Chemerin is associated with inflammatory markers and metabolic syndrome phenotypes in hypertension patients. Clin. Exp. Hypertens. 2014, 36, 326–332. [Google Scholar] [CrossRef]
- Marwa, O.E.-D.; Al-Aliaa, M.S. CHEMERIN IS AN INDISPENSABLE PRE-TREATMENT PREDICTOR OF SOFOSBUVIR, PEGYLATED INTERFERON-ALPHA AND RIBAVIRIN OUTCOMES IN CHRONIC HEPATITIS C EGYPTIAN PATIENTS. Az. J. Pharm. Sci. 2019, 60, 111–121. [Google Scholar]
- Keikha, M.; Eslami, M.; Yousefi, B.; Ali-Hassanzadeh, M.; Kamali, A.; Yousefi, M.; Karbalaei, M. HCV genotypes and their determinative role in hepatitis C treatment. Virusdisease 2020, 31, 235–240. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Baseline (82 patients) | 4 weeks (79 patients) | 12 weeks (81 patients) | 3 Months after End of Therapy (71 patients) |
|---|---|---|---|---|
| BMI kg/m2 | 0.046 (0.695) | 0.028 (0.816) | 0.054 (0.653) | −0.002 (0.987) |
| MELD Score | −0.777 (<0.001) | −0.749 (<0.001) | −0.752 (<0.001) | −0.578 (<0.001) |
| ALT U/L | 0.119 (0.286) | −0.067 (0.559) | −0.057 (0.612) | 0.198 (0.104) |
| AST U/L | −0.233 (0.035) | −0.379 (0.001) | −0.500 (<0.001) | −0.475 (<0.002) |
| Bilirubin mg/dL | −0.588 (<0.001) | −0.614 (<0.001) | −0.668 (<0.001) | −0.591 (<0.001) |
| Albumin g/L | 0.592 (<0.001) | 0.453 (<0.001) | 0.537 (<0.001) | 0.220 (0.071) |
| INR | −0.815 (<0.001) | −0.744 (<0.001) | −0.786 (<0.001) | −0.815 (<0.001) |
| Creatinine mg/dL | 0.099 (0.378) | 0.000 (0.997) | 0.111 (0.325) | 0.165 (0.175) |
| Leukocytes n/L | 0.628 (<0.001) | 0.515 (<0.001) | 0.572 (<0.001) | 0.360 (0.003) |
| CRP mg/L | 0.003 (0.979) | 0.079 (0.489) | −0.103 (0.362) | 0.199 (0.101) |
| HDL mg/dL | 0.021 (0.857) | 0.123 (0.292) | 0.129 (0.261) | 0.005 (0.971) |
| LDL mg/dL | 0.598 (<0.001) | 0.655 (<0.001) | 0.681 (<0.001) | 0.618 (<0.001) |
| Model | OR | 95% CI | p |
|---|---|---|---|
| Model 1 | 0.938 | 0.912–0.966 | <0.001 |
| Model 2 | 0.937 | 0.910–0.964 | <0.001 |
| Model 3 | 0.936 | 0.908–0.965 | <0.001 |
| Model 4 | 0.935 | 0.907–0.965 | <0.001 |
| Model 5 | 0.967 | 0.934–1.001 | 0.058 |
| Laboratory Parameter | Baseline (82 patients) | 4 weeks Therapy (79 patients) | 12 weeks Therapy (81 patients) | 3 Months after End of Therapy (71 patients) |
|---|---|---|---|---|
| Ferritin ng/mL | 141 (7.0–2309) 76,** | 122 (9.1–1638) | 97 (6.6–1161) 80 | 69.8 (6.4–1133) 70,** |
| ALT U/L | 86 (22–287) ***,%%%,$$$ | 28 (7–255) %%% | 27 (8–388) $$$ | 26 (6–443) *** |
| AST U/L | 75 (17–1230) $ | 28 (10–1140) | 26 (7–836) $ | 25 (11–1390) |
| Bilirubin mg/dL | 0.8 (0.3–4.3) | 0.8 (0.06–4.85) | 0.6 (0.05–7.5) | 0.6 (0.04–2.8) 71 |
| Albumin g/L | 36 (19–45) 81,*** | 37 (19–47) | 37 (16–45) 79 | 38.6 (26.1–46) 71,*** |
| INR | 1.13 (0.91–2.44) | 1.12 (0.90–3.15) | 1.13 (0.87–2.22) | 1.08 (0.88–2.81) |
| Creatinine mg/dL | 0.78 (0.14–1.31) 81 | 0.81 (0.21–1.54) | 0.77 (0.14–1.92) | 0.8 (0.1–1.4) |
| Leukocytes n/L | 5.9 (2.2–72.4) | 6.1 (2.0–72.5) | 5.9 (2.4–62.9) | 6.0 (1.9–38.6) 71 |
| CRP mg/L | 2.9 (2.9–29.9) | 2.9 (0–19.8) | 2.9 (2.9–19.1) 80 | 2.9 (2.9–46.3) |
| HDL mg/dL | 51 (19–103) 77 | 54 (25–102) 77 | 51 (13–96) 78 | 52 (23–86) 65 |
| LDL mg/dL | 88 (31–210) 77,*,%%,§§ | 113 (33–206) 77,%% | 106 (33–198) 78,§§ | 115 (38–185) 64,* |
| Model | OR | 95% CI | p |
|---|---|---|---|
| Model 1 | 0.966 | 0.947–0.985 | 0.001 |
| Model 2 | 0.966 | 0.947–0.985 | 0.001 |
| Model 3 | 0.963 | 0.943–0.984 | 0.001 |
| Model 4 | 0.969 | 0.935–1.004 | 0.082 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peschel, G.; Grimm, J.; Gülow, K.; Müller, M.; Buechler, C.; Weigand, K. Chemerin Is a Valuable Biomarker in Patients with HCV Infection and Correlates with Liver Injury. Diagnostics 2020, 10, 974. https://doi.org/10.3390/diagnostics10110974
Peschel G, Grimm J, Gülow K, Müller M, Buechler C, Weigand K. Chemerin Is a Valuable Biomarker in Patients with HCV Infection and Correlates with Liver Injury. Diagnostics. 2020; 10(11):974. https://doi.org/10.3390/diagnostics10110974
Chicago/Turabian StylePeschel, Georg, Jonathan Grimm, Karsten Gülow, Martina Müller, Christa Buechler, and Kilian Weigand. 2020. "Chemerin Is a Valuable Biomarker in Patients with HCV Infection and Correlates with Liver Injury" Diagnostics 10, no. 11: 974. https://doi.org/10.3390/diagnostics10110974
APA StylePeschel, G., Grimm, J., Gülow, K., Müller, M., Buechler, C., & Weigand, K. (2020). Chemerin Is a Valuable Biomarker in Patients with HCV Infection and Correlates with Liver Injury. Diagnostics, 10(11), 974. https://doi.org/10.3390/diagnostics10110974