Galectin-3 Plasma Levels Are Associated with Risk Profiles in Pulmonary Arterial Hypertension


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Blood Samples and Analysis
2.3. Echocardiographic Examination
2.4. Six-Minute Walk Test
2.5. Right Heart Catheterization
2.6. Clinical Evaluation
2.7. Risk Stratification
2.8. Statistical Analysis
3. Results
3.1. Clinical Characteristics
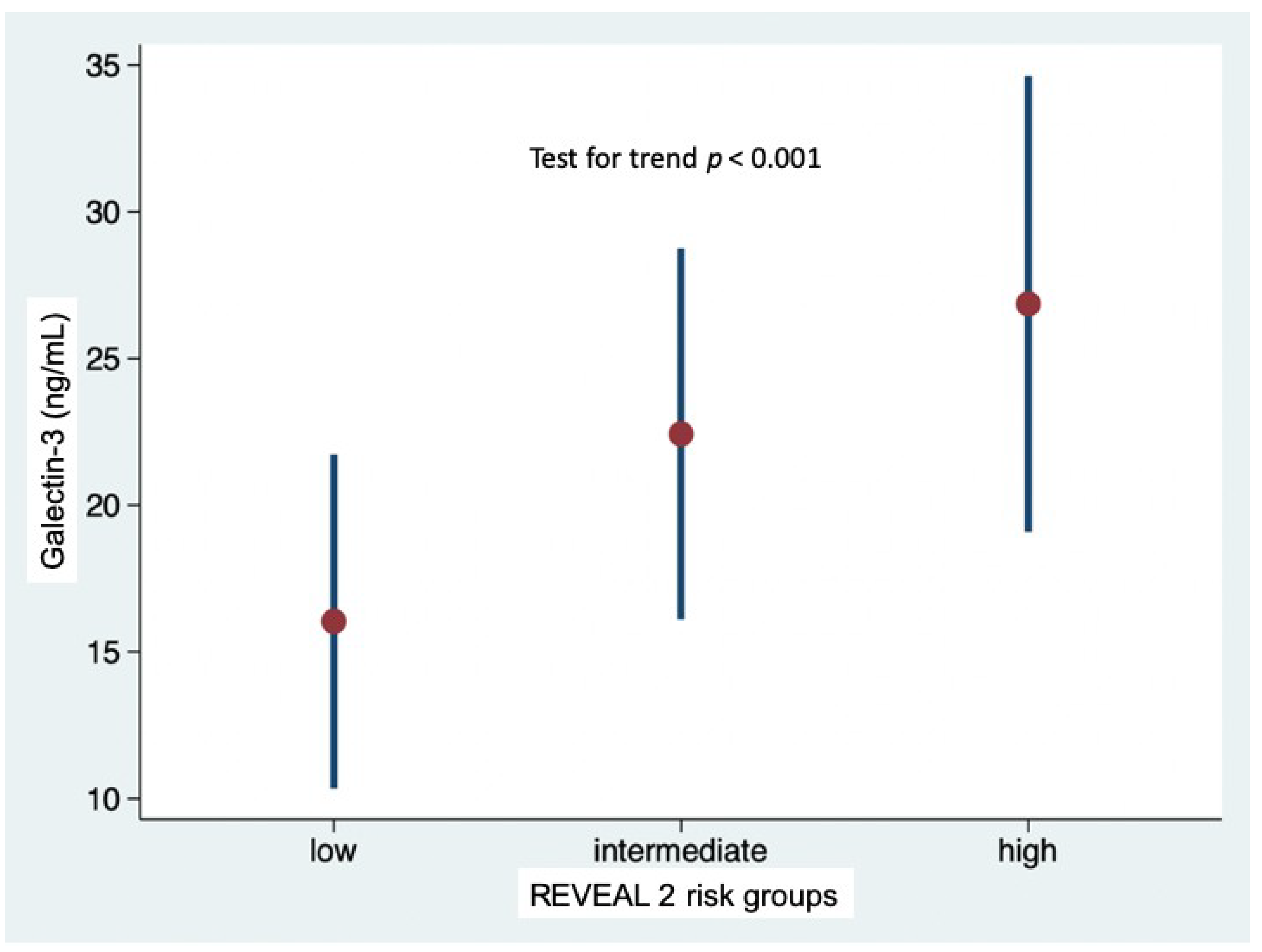
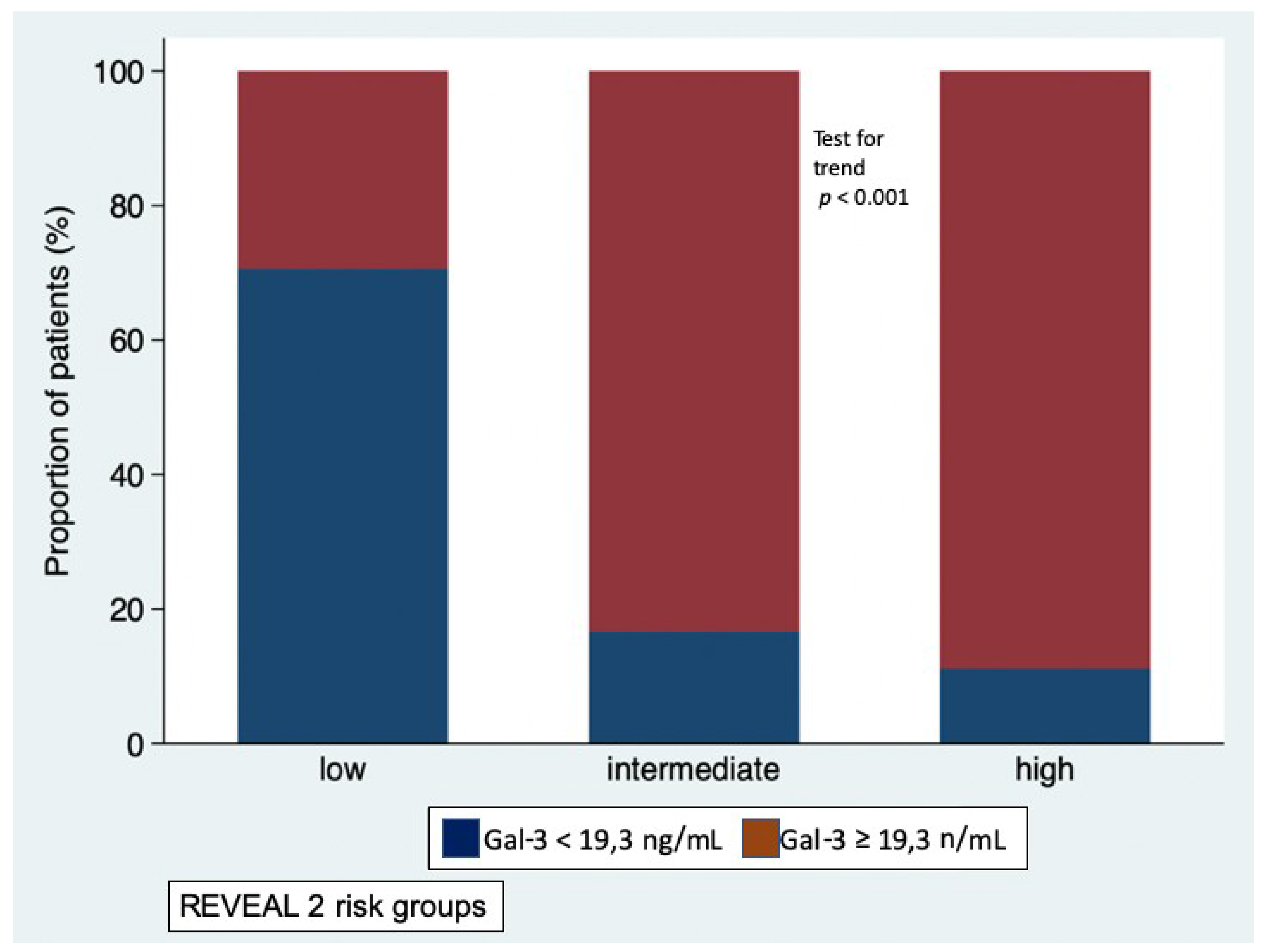
3.2. Galectin-3 Levels and Risk Profiles According to REVEAL 2.0 Risk Calculator
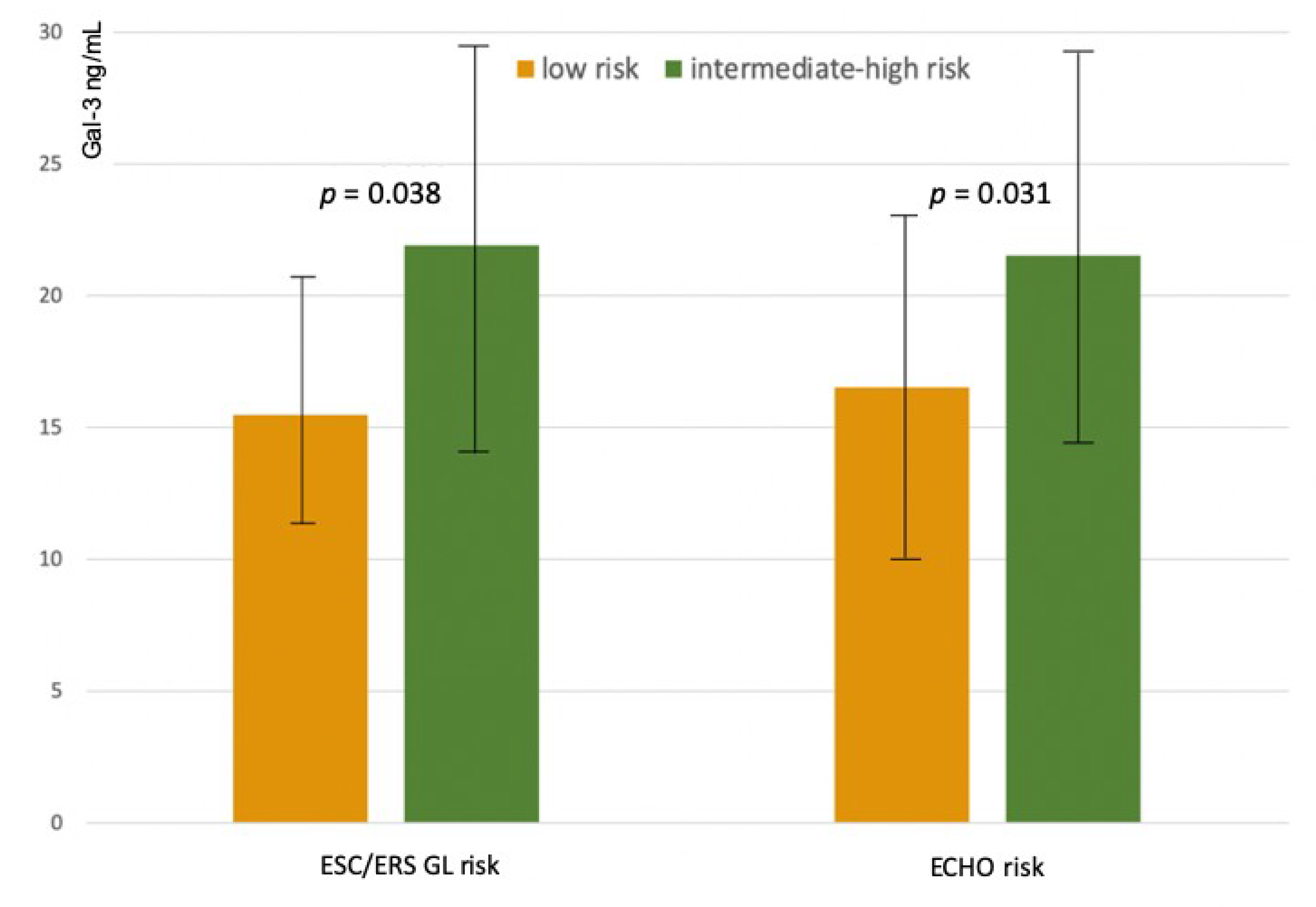
3.3. Galectin-3 Levels and Risk Profiles According to ESC/ERS Guidelines Criteria
3.4. Galectin-3 Levels and Risk Profiles According to the Echocardiographic Assessment of Right Heart
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Pediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [PubMed]
- Bogaard, H.J.; Abe, K.; Vonk Noordegraaf, A.; Voelkel, N.F. The right ventricle under pressure: Cellular and molecular mechanisms of right-heart failure in pulmonary hypertension. Chest 2009, 135, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.J.; Archer, S.L. The right ventricle in pulmonary arterial hypertension: Disorders of metabolism, angiogenesis and adrenergic signaling in right ventricular failure. Circ. Res. 2014, 115, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Calvier, L.; Miana, M.; Reboul, P.; Cachofeiro, V.; Martinez-Martinez, E.; de Boer, R.A.; Poirier, F.; Lacolley, P.; Zannad, F.; Rossignol, P.; et al. Galectin 3 mediates aldosterone induced vascular fibrosis. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Filipe, M.D.; Meijers, W.C.; Rogier van der Velde, A.; de Boer, R.A. Galectin-3 and heart failure prognosis, prediction and clinical utility. Clin. Chim. Acta 2015, 443, 48–56. [Google Scholar] [CrossRef]
- Edelmann, F.; Holzendorf, V.; Wachter, R.; Nolte, K.; Schmidt, A.G.; Kraigher-Krainer, E.; Duvinage, A.; Unkelbach, I.; Düngen, H.D.; Tschöpe, C.; et al. Galectin-3 in patients with heart failure with preserved ejection fraction: Results from the ALDO-DHF trial. Eur. J. Heart Fail. 2015, 17, 214–223. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. J. Am. Coll. Cardiol. 2017, 136, e137–e161. [Google Scholar]
- Ho, J.E.; Gao, W.; Levy, D.; Santhanakrishnan, R.; Araki, T.; Rosas, I.O.; Hatabu, H.; Latourelle, J.C.; Nishino, M.; Dupuis, J.; et al. Galectin-3 Is Associated with Restrictive Lung Disease and Interstitial Lung Abnormalities. Am. J. Respir. Crit. Care Med. 2016, 194, 77–83. [Google Scholar] [CrossRef]
- McGoon, M.D.; Krichman, A.; Farber, H.W.; Barst, R.J.; Raskob, G.E.; Liou, T.G.; Miller, D.P.; Feldkircher, K.; Giles, S. Design of the REVEAL registry for US patients with pulmonary arterial hypertension. Mayo Clin. Proc. 2008, 83, 923–931. [Google Scholar] [CrossRef]
- Benza, R.L.; Gomberg-Maitland, M.; Elliott, C.G.; Farber, H.W.; Foreman, A.J.; Frost, A.E.; McGoon, M.D.; Pasta, D.J.; Selej, M.; Burger, C.D.; et al. Predicting Survival in Patients With Pulmonary Arterial Hypertension: The REVEAL Risk Score Calculator 2.0 and Comparison With ESC/ERS-Based Risk Assessment Strategies. Chest 2019, 156, 323–337. [Google Scholar] [CrossRef]
- Boucly, A.; Weatherald, J.; Savale, L.; Jaïs, X.; Cottin, V.; Prevot, G.; Picard, F.; de Groote, P.; Jevnikar, M.; Bergot, E.; et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur. Respir. J. 2017, 50. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Klersy, C.; Magrini, G.; D’Armini, A.M.; Scelsi, L.; Raineri, C.; Pasotti, M.; Serio, A.; Campana, C.; Viganò, M. Prognostic relevance of the echocardiographic assessment of right ventricular function in patients with idiopathic pulmonary arterial hypertension. Int. J. Cardiol. 2010, 140, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Mercurio, V.; Fortuni, F.; Forfia, P.R.; Gall, H.; Ghofrani, A.; Mathai, S.C.; Mazurek, J.A.; Mukherjee, M.; Richter, M.; et al. TAPSE in PAH investigators. A comprehensive echocardiographic method for risk stratification in pulmonary arterial hypertension. Eur. Respir. J. 2020, 56, 2000513. [Google Scholar] [CrossRef]
- Torbicki, A.; Kurzyna, M.; Kuca, P.; Fijałkowska, A.; Sikora, J.; Florczyk, M.; Pruszczyk, P.; Burakowski, J.; Wawrzyńska, L. Detectable serum cardiac troponin T as a marker of poor prognosis among patients with chronic precapillary pulmonary hypertension. Circulation 2003, 108, 844–848. [Google Scholar] [CrossRef]
- Nagaya, N.; Nishikimi, T.; Okano, Y.; Uematsu, M.; Satoh, T.; Kyotani, S.; Kuribayashi, S.; Hamada, S.; Kakishita, M.; Nakanishi, N.; et al. Plasma brain natriuretic peptide levels increase in proportion to the extent of right ventricular dysfunction in pulmonary hypertension. J. Am. Coll. Cardiol. 1998, 31, 202–208. [Google Scholar] [CrossRef]
- Leuchte, H.H.; Holzapfel, M.; Baumgartner, R.A.; Ding, I.; Neurohr, C.; Vogeser, M.; Kolbe, T.; Schwaiblmair, M.; Behr, J. Clinical significance of brain natriuretic peptide in primary pulmonary hypertension. J. Am. Coll. Cardiol. 2004, 43, 764–770. [Google Scholar] [CrossRef]
- Leuchte, H.H.; Holzapfel, M.; Baumgartner, R.A.; Neurohr, C.; Vogeser, M.; Behr, J. Characterization of brain natriuretic peptide in long-term follow-up of pulmonary arterial hypertension. Chest 2005, 128, 2368–2374. [Google Scholar] [CrossRef]
- Fijalkowska, A.; Kurzyna, M.; Torbicki, A.; Szewczyk, G.; Florczyk, M.; Pruszczyk, P.; Szturmowicz, M. Serum N-terminal brain natriuretic peptide as a prognostic parameter in patients with pulmonary hypertension. Chest 2006, 129, 1313–1321. [Google Scholar] [CrossRef]
- Mauritz, G.J.; Rizopoulos, D.; Groepenhoff, H.; Tiede, H.; Felix, J.; Eilers, P.; Bosboom, J.; Postmus, P.E.; Westerhof, N.; Vonk-Noordegraaf, A. Usefulness of serial N-terminal pro-B-type natriuretic peptide measurements for determining prognosis in patients with pulmonary arterial hypertension. Am. J. Cardiol. 2011, 108, 1645–1650. [Google Scholar] [CrossRef]
- Mathai, S.C.; Bueso, M.; Hummers, L.K.; Boyce, D.; Lechtzin, N.; Le Pavec, J.; Campo, A.; Champion, H.C.; Housten, T.; Forfia, P.R.; et al. Disproportionate elevation of N-terminal pro-brain natriuretic peptide in scleroderma-related pulmonary hypertension. Eur. Respir. J. 2010, 35, 95–104. [Google Scholar] [CrossRef]
- Pezzuto, B.; Badagliacca, R.; Poscia, R.; Ghio, S.; D’Alto, M.; Vitulo, P.; Mulè, M.; Albera, C.; Volterrani, M.; Fedele, F.; et al. Circulating biomarkers in pulmonary arterial hypertension: Update and future direction. J. Heart Lung Transplant. 2015, 34, 282–305. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, T.; Asano, Y.; Akamata, K.; Noda, S.; Masui, Y.; Yamada, D.; Takahashi, T.; Ichimura, Y.; Toyama, T.; Tamaki, Z.; et al. Serum levels of galectin-3: Possible association with fibrosis, aberrant angiogenesis, and immune activation in patients with systemic sclerosis. J. Rheumatol. 2012, 39, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Koca, S.S.; Akbas, F.; Ozgen, M.; Yolbas, S.; Ilhan, N.; Gundogdu, B.; Isik, A. Serum galectin-3 level in systemic sclerosis. Clin. Rheumatol. 2014, 33, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Faludi, R.; Nagy, G.; Tőkés-Füzesi, M.; Kovács, K.; Czirják, L.; Komócsi, A. Galectin-3 is an independent predictor of survival in systemic sclerosis. Int. J. Cardiol. 2017, 233, 118–124. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Gal-3 < 19,3 (n = 35) | Gal-3 ≥ 19,3 (n = 35) | P Value | |
|---|---|---|---|
| Clinical and biochemical data | |||
| Age (y) | 51 ± 19 | 57 ± 15 | 0.36 |
| Sex (F) | 23 (66%) | 25 (71%) | 0.79 |
| WHO class III/IV | 4 (11%) | 18 (51%) | 0.002 |
| Aetiology (IPAH/SSc/others) | 25/3/7 | 12/14/9 | 0.015 |
| 6MWD (mt) | 413 ± 99 | 346 ± 99 | 0.007 |
| BNP (ng/mL) | 75 (38–135) | 235 (100–450) | 0.004 |
| Echocardiographic parameters | |||
| RV diameter (mm) | 34 ± 7 | 36 ± 6 | 0.24 |
| RVEDA (cm2) | 27 ± 8 | 28 ± 9 | 0.65 |
| FAC (%) | 32 ± 9 | 30 ± 8 | 0.35 |
| TAPSE (mm) | 20 ± 5 | 18 ± 3 | 0.03 |
| LVEI-d | 1.2 ± 0.3 | 1.4 ± 0.2 | 0.09 |
| RA area (cmq) | 22 ± 78 | 23 ± 6 | 0.74 |
| Systolic PAP (mmHg) | 65 ± 25 | 77 ± 18 | 0.02 |
| TR moderate-severe (n, %) | 10 (29%) | 15 (43%) | 0.06 |
| Pericardic effusion (n, %) | 8 (23%) | 9 (26%) | 0.37 |
| IVC plethora (n, %) | 5 (14%) | 7 (20%) | 0.06 |
| Hemodynamic parameters | |||
| CI (L/min/m2) | 2.8 ± 0.6 | 2.4 ± 0.6 | 0.009 |
| PAWP (mmHg) | 10 ± 3 | 10 ± 3 | 0.43 |
| Systolic PAP (mmHg) | 70 ± 22 | 81 ± 24 | 0.03 |
| Mean PAP (mmHg) | 42 ± 13 | 48 ± 15 | 0.06 |
| PVR (WU) | 6.8 ± 5 | 10.3 ± 5 | 0.02 |
| RAP (mmHg) | 7.1 ± 3 | 8 ± 5 | 0.43 |
| PCa (mL/mmHg) | 2± 1.1 | 1.1 ± 0.5 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scelsi, L.; Ghio, S.; Matrone, B.; Mannucci, L.; Klersy, C.; Valaperta, S.; Turco, A.; Greco, A.; Derosa, G.; Oltrona Visconti, L. Galectin-3 Plasma Levels Are Associated with Risk Profiles in Pulmonary Arterial Hypertension. Diagnostics 2020, 10, 857. https://doi.org/10.3390/diagnostics10110857
Scelsi L, Ghio S, Matrone B, Mannucci L, Klersy C, Valaperta S, Turco A, Greco A, Derosa G, Oltrona Visconti L. Galectin-3 Plasma Levels Are Associated with Risk Profiles in Pulmonary Arterial Hypertension. Diagnostics. 2020; 10(11):857. https://doi.org/10.3390/diagnostics10110857
Chicago/Turabian StyleScelsi, Laura, Stefano Ghio, Benedetta Matrone, Letizia Mannucci, Catherine Klersy, Serenella Valaperta, Annalisa Turco, Alessandra Greco, Giuseppe Derosa, and Luigi Oltrona Visconti. 2020. "Galectin-3 Plasma Levels Are Associated with Risk Profiles in Pulmonary Arterial Hypertension" Diagnostics 10, no. 11: 857. https://doi.org/10.3390/diagnostics10110857
APA StyleScelsi, L., Ghio, S., Matrone, B., Mannucci, L., Klersy, C., Valaperta, S., Turco, A., Greco, A., Derosa, G., & Oltrona Visconti, L. (2020). Galectin-3 Plasma Levels Are Associated with Risk Profiles in Pulmonary Arterial Hypertension. Diagnostics, 10(11), 857. https://doi.org/10.3390/diagnostics10110857