The Appropriate Opportunity for Evaluating Liver Fibrosis by Using the FIB-4 Index in Patients with Nonalcoholic Fatty Liver Disease in Japan

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Laboratory and Clinical Parameters
2.3. Liver Histology
2.4. DNA Preparation and SNP Genotyping
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
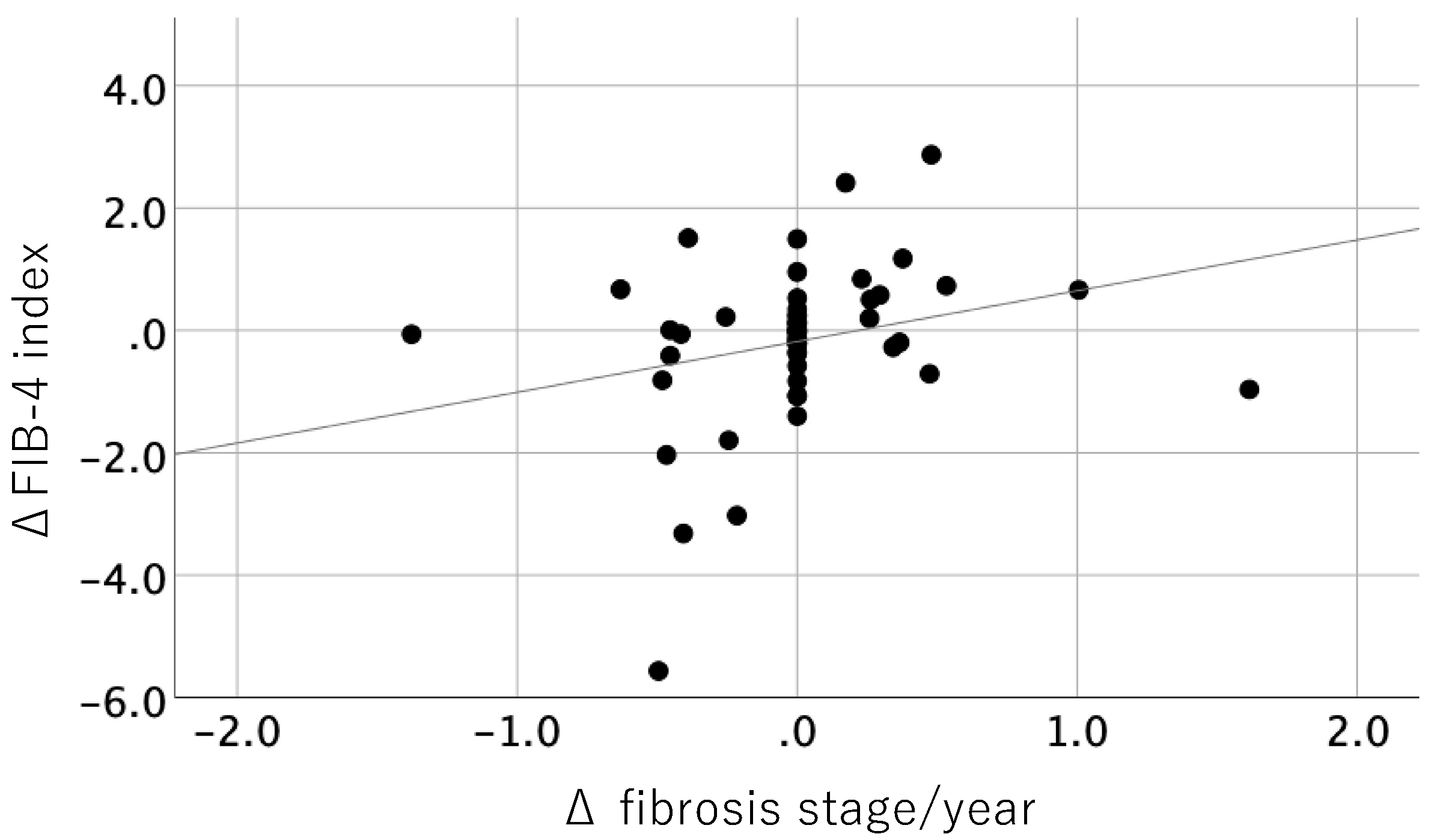
3.2. Correlation between Histological Change and Change in FIB-4 Index
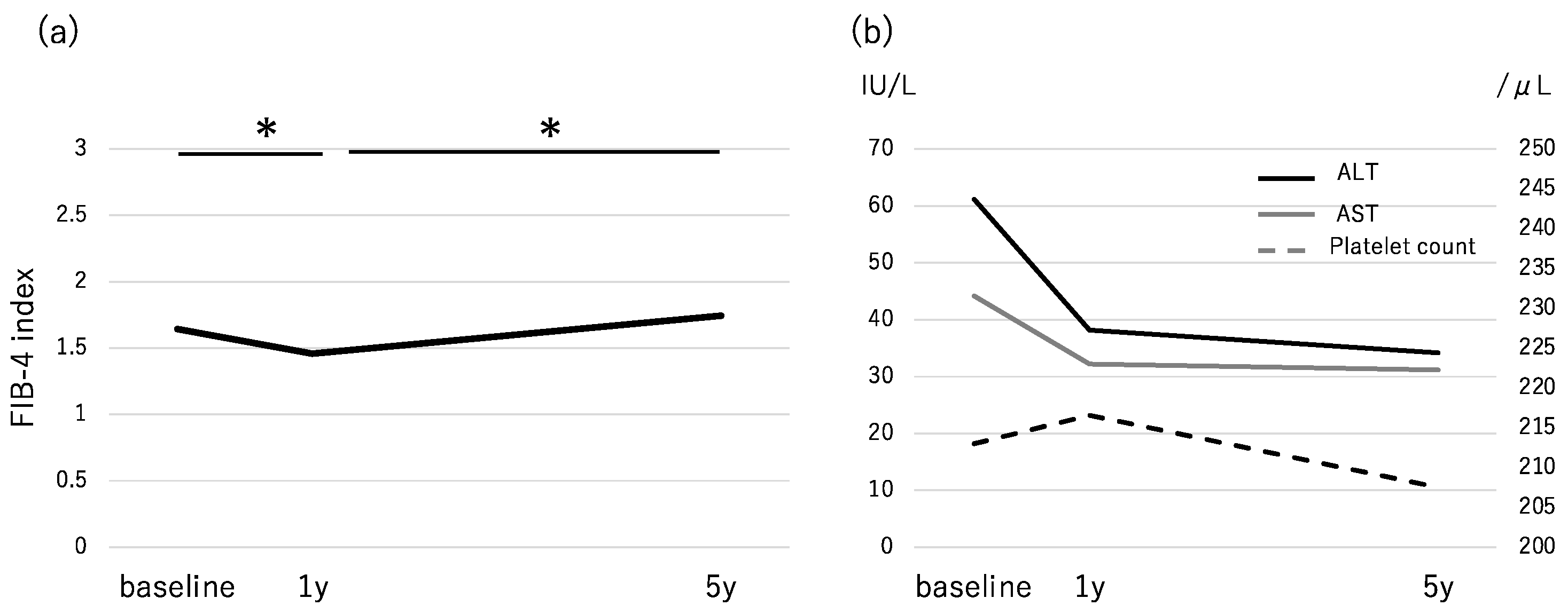
3.3. Changes in the FIB-4 Index During the Follow-Up Period and Accuracy for Advanced Fibrosis
3.4. Factors Associated with a FIB-4 Index >2.67 at 5 Years
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 2015, 149, 389–397. [Google Scholar] [CrossRef]
- Pais, R.; Charlotte, F.; Fedchuk, L.; Bedossa, P.; Lebray, P.; Poynard, T.; Ratziu, V.; LIDO Study Group. A systematic review of follow-up biopsies reveals disease progression in patients with non-alcoholic fatty liver. J. Hepatol. 2013, 59, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Wong, G.L.; Choi, P.C.; Chan, A.W.; Li, M.K.; Chan, H.Y.; Chim, A.M.; Yu, J.; Sung, J.J.; Chan, H.L. Disease progression of non-alcoholic fatty liver disease: A prospective study with paired liver biopsies at 3 years. Gut 2010, 59, 969–974. [Google Scholar] [CrossRef]
- Ekstedt, M.; Franzén, L.E.; Mathiesen, U.L.; Thorelius, L.; Holmqvist, M.; Bodemar, G.; Kechagias, S. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006, 44, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Argo, C.K.; Northup, P.G.; Al-Osaimi, A.M.; Caldwell, S.H. Systematic review of risk factors for fibrosis progression in non-alcoholic steatohepatitis. J. Hepatol. 2009, 51, 371–379. [Google Scholar] [CrossRef]
- Fassio, E.; Alvarez, E.; Domínguez, N.; Landeira, G.; Longo, C. Natural history of nonalcoholic steatohepatitis: A longitudinal study of repeat liver biopsies. Hepatology 2004, 40, 820–826. [Google Scholar] [CrossRef]
- Hoofnagle, J.H.; Van Natta, M.L.; Kleiner, D.E.; Clark, J.M.; Kowdley, K.V.; Loomba, R.; Neuschwander-Tetri, B.A.; Sanyal, A.J.; Tonascia, J.; Non-alcoholic Steatohepatitis Clinical Research Network (NASH CRN). Vitamin E and changes in serum alanine aminotransferase levels in patients with non-alcoholic steatohepatitis. Aliment. Pharmacol. Ther. 2013, 38, 134–143. [Google Scholar] [CrossRef]
- Adams, L.A.; Sanderson, S.; Lindor, K.D.; Angulo, P. The histological course of nonalcoholic fatty liver disease: A longitudinal study of 103 patients with sequential liver biopsies. J. Hepatol. 2005, 42, 132–138. [Google Scholar] [CrossRef]
- Hamaguchi, E.; Takamura, T.; Sakurai, M.; Mizukoshi, E.; Zen, Y.; Takeshita, Y.; Kurita, S.; Arai, K.; Yamashita, T.; Sasaki, M.; et al. Histological course of nonalcoholic fatty liver disease in Japanese patients: Tight glycemic control, rather than weight reduction, ameliorates liver fibrosis. Diabetes Care 2010, 33, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Rockey, D.C.; Caldwell, S.H.; Goodman, Z.D.; Nelson, R.C.; Smith, A.D.; American Association for the Study of Liver Diseases. Liver biopsy. Hepatology 2009, 49, 1017–1044. [Google Scholar] [CrossRef]
- Bravo, A.A.; Sheth, S.G.; Chopra, S. Liver biopsy. N. Engl. J. Med. 2001, 344, 495–500. [Google Scholar] [CrossRef]
- Vuppalanchi, R.; Ünalp, A.; Van Natta, M.; Cummings, O.W.; Sandrasegaran, K.E.; Hameed, T.; Tonascia, J.; Chalasani, N. Effects of liver biopsy sample length and number of readings on sampling variability in nonalcoholic Fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Ratziu, V.; Charlotte, F.; Heurtier, A.; Gombert, S.; Giral, P.; Bruckert, E.; Grimaldi, A.; Capron, F.; Poynard, T.; LIDO Study Group. Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology 2005, 128, 1898–1906. [Google Scholar] [CrossRef]
- Sumida, Y.; Yoneda, M.; Hyogo, H.; Itoh, Y.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Aoki, N.; Kanemasa, K.; et al. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC Gastroenterol. 2012, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J. NASH Clinical Research Network: Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef]
- Foschi, F.G.; Domenicali, M.; Giacomoni, P.; Dall’Aglio, A.C.; Conti, F.; Borghi, A.; Bevilacqua, V.; Napoli, L.; Mirici, F.; Cucchetti, A.; et al. Is there an association between commonly employed biomarkers of liver fibrosis and liver stiffness in the general population? Ann. Hepatol. 2020, 19, 380–387. [Google Scholar] [CrossRef]
- Seko, Y.; Yamaguchi, K.; Mizuno, N.; Okuda, K.; Takemura, M.; Taketani, H.; Hara, T.; Umemura, A.; Nishikawa, T.; Moriguchi, M.; et al. Combination of PNPLA3 and TLL1 polymorphism can predict advanced fibrosis in Japanese patients with nonalcoholic fatty liver disease. J. Gastroenterol. 2018, 53, 438–448. [Google Scholar] [CrossRef]
- Nishioji, K.; Mochizuki, N.; Kobayashi, M.; Kamaguchi, M.; Sumida, Y.; Nishimura, T.; Yamaguchi, K.; Kadotani, H.; Itoh, Y. The impact of PNPLA3 rs738409 genetic polymorphism and weight gain >10 kg after age 20 on non-alcoholic fatty liver disease in non-obese Japanese individuals. PLoS ONE 2015, 10, e0140427. [Google Scholar] [CrossRef] [PubMed]
- Imajo, K.; Kessoku, T.; Honda, Y.; Tomeno, W.; Ogawa, Y.; Mawatari, H.; Fujita, K.; Yoneda, M.; Taguri, M.; Hyogo, H.; et al. Magnetic Resonance Imaging More Accurately Classifies Steatosis and Fibrosis in Patients with Nonalcoholic Fatty Liver Disease Than Transient Elastography. Gastroenterology 2016, 150, 626–637. [Google Scholar] [CrossRef] [PubMed]
- Giuffrè, M.; Macor, D.; Masutti, F.; Abazia, C.; Tinè, F.; Patti, R.; Buonocore, M.R.; Colombo, A.; Visintin, A.; Campigotto, M.; et al. Evaluation of spleen stiffness in healthy volunteers using point shear wave elastography. Ann. Hepatol. 2019, 18, 736–741. [Google Scholar] [CrossRef]
- Giuffrè, M.; Fouraki, S.; Comar, M.; Masutti, F.; Crocè, L.S. The Importance of Transaminases Flare in Liver Elastography: Characterization of the Probability of Liver Fibrosis Overestimation by Hepatitis C Virus-Induced Cytolysis. Microorganisms 2020, 29, 348. [Google Scholar] [CrossRef]
- Yoneda, M.; Imajo, K.; Takahashi, H.; Ogawa, Y.; Eguchi, Y.; Sumida, Y.; Yoneda, M.; Kawanaka, M.; Saito, S.; Tokushige, K.; et al. Clinical strategy of diagnosing and following patients with nonalcoholic fatty liver disease based on invasive and noninvasive methods. J. Gastroenterol. 2018, 53, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Davyduke, T.; Tandon, P.; Al-Karaghouli, M.; Abraldes, J.G.; Ma, M.M. Impact of implementing a “FIB-4 First” strategy on a pathway for patients with NAFLD referred from primary care. Hepatol. Commun. 2019, 29, 1322–1333. [Google Scholar] [CrossRef]
- European Association for Study of the Liver; Asociación Latinoamericana para el Estudio del Hígado. EASL-ALEH clinical practice guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef] [PubMed]
- Seko, Y.; Sumida, Y.; Sasaki, K.; Itoh, Y.; Iijima, H.; Hashimoto, T.; Ishii, S.; Inagaki, N. Effects of canagliflozin, an SGLT2 inhibitor, on hepatic function in Japanese patients with type 2 diabetes mellitus: Pooled and subgroup analyses of clinical trials. J. Gastroenterol. 2018, 53, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, Y.; Kitajima, Y.; Hyogo, H.; Takahashi, H.; Kojima, M.; Ono, M.; Araki, N.; Tanaka, K.; Yamaguchi, M.; Matsuda, Y.; et al. Pilot study of liraglutide effects in non-alcoholic steatohepatitis and non-alcoholic fatty liver disease with glucose intolerance in Japanese patients (LEAN-J). Hepatol. Res. 2015, 45, 269–278. [Google Scholar] [CrossRef]
- Seko, Y.; Sumida, Y.; Tanaka, S.; Mori, K.; Taketani, H.; Ishiba, H.; Hara, T.; Okajima, A.; Umemura, A.; Nishikawa, T.; et al. Effect of 12-week dulaglutide therapy in Japanese patients with biopsy-proven non-alcoholic fatty liver disease and type 2 diabetes mellitus. Hepatol. Res. 2017, 47, 1206–1211. [Google Scholar] [CrossRef] [PubMed]
- Dongiovanni, P.; Petta, S.; Mannisto, V.; Mancina, R.M.; Pipitone, R.; Karja, V.; Maggioni, M.; Kakela, P.; Wiklund, O.; Mozzi, E.; et al. Statin use and non-alcoholic steatohepatitis in at risk individuals. J. Hepatol. 2015, 63, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Abdelmalek, M.F.; Loomba, R.; Kowdley, K.V.; McCullough, A.J.; Dasarathy, S.; Neuschwander-Tetri, B.A.; Terrault, N.; Ferguson, B.; Shringarpure, R.; et al. Relationship between three commonly used non-invasive fibrosis biomarkers and improvement in fibrosis stage in patients with non-alcoholic steatohepatitis. Liver Int. 2019, 39, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Seko, Y.; Sumida, Y.; Tanaka, S.; Mori, K.; Taketani, H.; Ishiba, H.; Hara, T.; Okajima, A.; Yamaguchi, K.; Moriguchi, M.; et al. Serum alanine aminotransferase predicts the histological course of non-alcoholic steatohepatitis in Japanese patients. Hepatol. Res. 2015, 45, E53–E61. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Allen, A.M.; Wang, Z.; Prokop, L.J.; Murad, M.H.; Loomba, R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: A systematic review and meta-analysis of paired-biopsy studies. Clin. Gastroenterol. Hepatol. 2015, 13, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Wong, G.L.; Chim, A.M.; Tse, A.M.; Tsang, S.W.; Hui, A.Y.; Choi, P.C.; Chan, A.W.; So, W.Y.; Chan, F.K.; et al. Validation of the NAFLD fibrosis score in a Chinese population with low prevalence of advanced fibrosis. Am. J. Gastroenterol. 2008, 103, 1682–1688. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable n = 272 | Baseline | 1 Year | 5 Years | p (Baseline and 5 Years) |
|---|---|---|---|---|
| Sex, male | 122 (44.9%) | |||
| Age, years | 60 (21–83) | |||
| PNPLA3, CC/CG/GG | 35/93/87 | |||
| Hyperlipidemia | 184 (67.6%) | |||
| T2DM | 137 (50.4%) | |||
| Hypertension | 112 (41.2%) | |||
| BMI, kg/m2 | 26.9 (18.9–43.0) | 26.5 (17.2–43.0) | 26.4 (17.4–46.2) | <0.001 |
| Albumin, g/dL | 4.4 (3.1–5.3) | 4.4 (3.0–5.6) | 4.3 (2.5–5.6) | 0.013 |
| AST, IU/L | 44 (12–217) | 32 (14–166) | 31 (11–158) | <0.001 |
| ALT, IU/L | 62 (7–266) | 38 (4–278) | 34 (3–180) | <0.001 |
| GGT, IU/L | 61 (14–533) | 47 (15–415) | 39 (8–405) | <0.001 |
| Platelet count, ×103/μL | 213 (46–454) | 217 (46–393) | 207 (25–433) | 0.089 |
| Total cholesterol, mg/dL | 202 (66–350) | 202 (74–334) | 198 (87–301) | 0.061 |
| Triglycerides, mg/dL | 146 (18–739) | 140 (32–692) | 132 (37–593) | 0.179 |
| LDL-C, mg/dL | 124 (44–301) | 120 (48–286) | 118 (38–232) | 0.007 |
| HDL-C, mg/dL | 54 (21-151) | 54 (23–138) | 54 (23–134) | 0.490 |
| FPG, mg/dL | 102 (60–420) | 106 (68–258) | 111 (62–279) | <0.001 |
| FIB-4 index | 1.64 (0.31–9.84) | 1.45 (0.32–11.73) | 1.74 (0.31–15.86) | 0.099 |
| Type IV collagen 7s, ng/mL | 4.6 (2.6–11.0) | 4.8 (2.8–17.0) | 4.8 (1.6–17.0) | 0.557 |
| Fibrosis stage (0/1/2/3/4) | 83/99/44/30/16 |
| Variable n = 52 | At Initial Biopsy | At Second Biopsy | p |
|---|---|---|---|
| Sex, male | 22 (42.3%) | ||
| Age, years | 68 (21–83) | ||
| Hyperlipidemia | 33 (63.5%) | ||
| T2DM | 26 (50.0%) | ||
| Hypertension | 24 (46.2%) | ||
| BMI, kg/m2 | 26.4 (18.9––43.0) | 26.6 (19.0–49.5) | 0.486 |
| Albumin, g/dL | 4.3 (3.2–4.9) | 4.1 (3.4–5.1) | 0.001 |
| AST, IU/L | 57 (22–186) | 38 (15–211) | <0.001 |
| ALT, IU/L | 83 (20–358) | 46 (7–251) | <0.001 |
| GGT, IU/L | 73 (22–306) | 45 (8–316) | 0.009 |
| Platelet count, ×103/μL | 207 (105–417) | 195 (93–403) | 0.040 |
| Total cholesterol, mg/dL | 201 (117–292) | 191 (93–436) | 0.203 |
| Triglycerides, mg/dL | 153 (71–559) | 130 (60–351) | 0.022 |
| LDL-C, mg/dL | 104 (43–225) | 124 (43–209) | 0.035 |
| HDL-C, mg/dL | 50 (22–85) | 51 (28–95) | 0.748 |
| FPG, mg/dL | 94 (60–260) | 96 (65–182) | 0.664 |
| FIB-4 index | 2.12 (0.31–9.04) | 2.20 (0.26–3.14) | 0.973 |
| Type IV collagen 7s, ng/mL | 5.3 (2.7–13.0) | 4.4 (2.6–9.5) | 0.002 |
| Fibrosis stage (0/1/2/3/4) | 0/24/14/14/0 | 2/18/21/8/3 |
| Stage at Second Biopsy | ||||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | Total | |
| Stage at initial biopsy | ||||||
| 1 | 2 | 13 | 7 | 2 | 0 | 24 |
| 2 | 0 | 4 | 8 | 1 | 1 | 14 |
| 3 | 0 | 1 | 6 | 5 | 2 | 14 |
| Total | 2 | 18 | 21 | 8 | 3 | 52 |
| (a) | |||||
| Baseline | 1 Year | ||||
| Stage 3,4 | Stage 0–2 | Stage 3,4 | Stage 0–2 | ||
| <1.30 | 8 | 75 | 11 | 100 | |
| ≧1.30 | 38 | 151 | 35 | 126 | |
| ≦2.67 | 17 | 147 | 26 | 186 | |
| >2.67 | 29 | 79 | 20 | 40 | |
| (b) | |||||
| Sensitivity | Specificity | PPV | NPV | ||
| Baseline | Low cut-off | 82.6 | 33.2 | 20.1 | 90.4 |
| High cut-off | 63.0 | 65.0 | 26.9 | 89.6 | |
| 1 year | Low cut-off | 76.9 | 44.2 | 21.7 | 90.1 |
| High cut-off | 43.4 | 82.3 | 33.3 | 87.7 | |
| Variable | Category | p Value | OR (95% CI) a | p Value |
|---|---|---|---|---|
| Age, year | Per 1 year | 1.05 (0.99–1.11) | 0.086 | |
| BMI, kg/m2 | Per 1 kg/m2 | 0.97 (0.86–1.11) | 0.679 | |
| Sex | 1: male | 0.002 | 0.34 (0.11–1.05) | 0.060 |
| 2: female | ||||
| T2DM | 1: no | 0.089 | 0.86 (0.31–2.36) | 0.765 |
| 2: yes | ||||
| PNPLA3 | 1: CC | 1 | ||
| 2: CG | 0.088 | 1.89 (0.31–11.41) | 0.490 | |
| 3: GG | 0.040 | 4.50 (0.74–27.32) | 0.102 | |
| FIB-4 index at baseline | 1: −2.67 | <0.01 | 2.61 (0.88–7.69) | 0.082 |
| 2: >2.67 | ||||
| FIB-4 index at 1 year | 1: −2.67 | <0.01 | 41.65 (13.11–132.33) | <0.01 |
| 2: >2.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seko, Y.; Yano, K.; Takahashi, A.; Okishio, S.; Kataoka, S.; Okuda, K.; Umemura, A.; Yamaguchi, K.; Moriguchi, M.; Tanaka, S.; et al. The Appropriate Opportunity for Evaluating Liver Fibrosis by Using the FIB-4 Index in Patients with Nonalcoholic Fatty Liver Disease in Japan. Diagnostics 2020, 10, 842. https://doi.org/10.3390/diagnostics10100842
Seko Y, Yano K, Takahashi A, Okishio S, Kataoka S, Okuda K, Umemura A, Yamaguchi K, Moriguchi M, Tanaka S, et al. The Appropriate Opportunity for Evaluating Liver Fibrosis by Using the FIB-4 Index in Patients with Nonalcoholic Fatty Liver Disease in Japan. Diagnostics. 2020; 10(10):842. https://doi.org/10.3390/diagnostics10100842
Chicago/Turabian StyleSeko, Yuya, Kota Yano, Aya Takahashi, Shinya Okishio, Seita Kataoka, Keiichiroh Okuda, Atsushi Umemura, Kanji Yamaguchi, Michihisa Moriguchi, Saiyu Tanaka, and et al. 2020. "The Appropriate Opportunity for Evaluating Liver Fibrosis by Using the FIB-4 Index in Patients with Nonalcoholic Fatty Liver Disease in Japan" Diagnostics 10, no. 10: 842. https://doi.org/10.3390/diagnostics10100842
APA StyleSeko, Y., Yano, K., Takahashi, A., Okishio, S., Kataoka, S., Okuda, K., Umemura, A., Yamaguchi, K., Moriguchi, M., Tanaka, S., & Itoh, Y. (2020). The Appropriate Opportunity for Evaluating Liver Fibrosis by Using the FIB-4 Index in Patients with Nonalcoholic Fatty Liver Disease in Japan. Diagnostics, 10(10), 842. https://doi.org/10.3390/diagnostics10100842