
Effects of Different Interventions Using Taekwondo, Boxing, and Elastic Band Training on Body Composition and Physical Function in Chilean Older Women: A Randomized Controlled Trial

 ,
,  ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
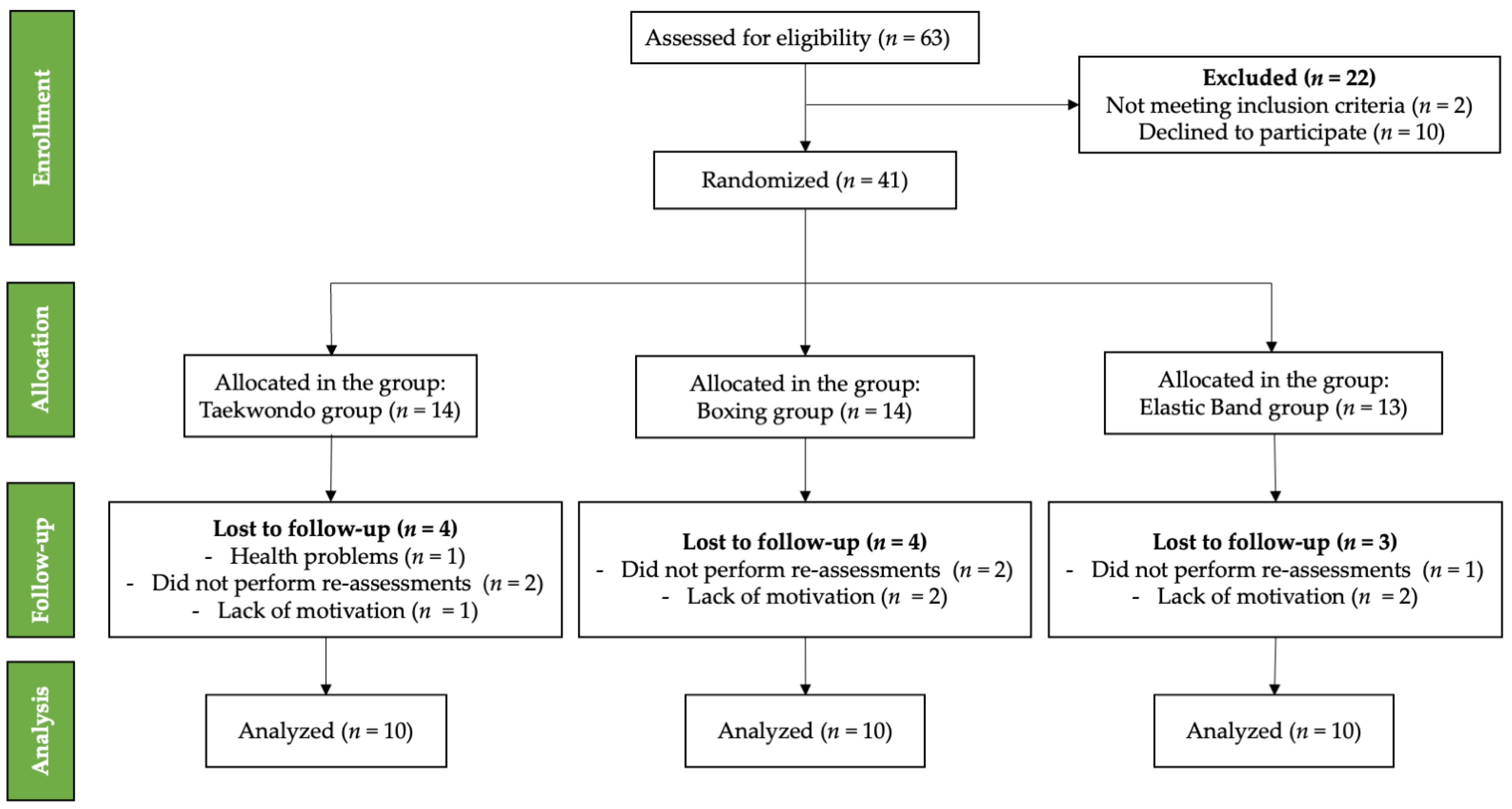
2.1. Study Design
2.2. Participants
2.3. Measurements and Interventions
2.3.1. Physical Performance
2.3.2. Anthropometric and Sociodemographic Parameters
2.3.3. Intervention
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Limitations and Strengths
4.2. Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gomes, D.; Santos, L.P.; Gonzalez, M.C.; Vieira, E.R.; Bielemann, R.M. Changes in Physical Performance among Community-Dwelling Older Adults in Six Years. Int. J. Environ. Res. Public Health 2023, 20, 5579. [Google Scholar] [CrossRef] [PubMed]
- Ponti, F.; Santoro, A.; Mercatelli, D.; Gasperini, C.; Conte, M.; Martucci, M.; Sangiorgi, L.; Franceschi, C.; Bazzocchi, A. Aging and Imaging Assessment of Body Composition: From Fat to Facts. Front. Endocrinol. 2019, 10, 861. [Google Scholar] [CrossRef]
- Briand, M.; Raffin, J.; Gonzalez-Bautista, E.; Ritz, P.; Abellan Van Kan, G.; Pillard, F.; Faruch-Bilfeld, M.; Guyonnet, S.; Dray, C.; Vellas, B.; et al. Body Composition and Aging: Cross-Sectional Results from the INSPIRE Study in People 20 to 93 Years Old. GeroScience 2025, 47, 863–875. [Google Scholar] [CrossRef]
- Kim, S.; Leng, X.I.; Kritchevsky, S.B. Body Composition and Physical Function in Older Adults with Various Comorbidities. Innov. Aging 2017, 1, igx008. [Google Scholar] [CrossRef]
- Jia, H.; Lubetkin, E.I.; DeMichele, K.; Stark, D.S.; Zack, M.M.; Thompson, W.W. Prevalence, risk factors, and burden of disease for falls and balance or walking problems among older adults in the US. Prev. Med. 2019, 126, 105737. [Google Scholar] [CrossRef] [PubMed]
- Cavusoglu, C.; Sendur, H.N.; Cerit, M.N.; Candemir, B.; Ileri, I.; Borazan, F.Y.; Dogrul, R.T.; Goker, B. Elasticity of leg muscles and incidence of falls in older adults: A prospective cohort analysis. Eur. Geriatr. Med. 2023, 14, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Salis, F.; Mandas, A. Physical Performance and Falling Risk Are Associated with Five-Year Mortality in Older Adults: An Observational Cohort Study. Medicina 2023, 59, 964. [Google Scholar] [CrossRef]
- Patiño-Villada, F.A.; González-Bernal, J.J.; González-Santos, J.; de Paz, J.A.; Jahouh, M.; Mielgo-Ayuso, J.; Romero-Pérez, E.M.; Soto-Cámara, R. Relationship of Body Composition with the Strength and Functional Capacity of People over 70 Years. Int. J. Environ. Res. Public Health 2020, 17, 7767. [Google Scholar] [CrossRef]
- Gutiérrez Monclus, P.; Frías Ortega, C. Políticas Públicas del Cuidado Dirigidas a Personas con Discapacidad y Dependencia en Chile, Universidad de Chile, Santiago, Chile, 2016. Available online: https://repositorio.uchile.cl/handle/2250/153145 (accessed on 20 January 2025).
- Hernandez-Martinez, J.; González-Castillo, C.; Herrera-Valenzuela, T.; Muñoz-Vásquez, C.; Magnani Branco, B.H.; Valdés-Badilla, P. Association between Physical Activity Habits with Cardiometabolic Variables, Body Composition, and Physical Performance in Chilean Older Women. Int. J. Environ. Res. Public Health 2023, 20, 6688. [Google Scholar] [CrossRef]
- Pinheiro, M.B.; Oliveira, J.S.; Baldwin, J.N.; Hassett, L.; Costa, N.; Gilchrist, H.; Wang, B.; Kwok, W.; Albuquerque, B.S.; Pivotto, L.R.; et al. Impact of physical activity programs and services for older adults: A rapid review. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 87. [Google Scholar] [CrossRef]
- Langhammer, B.; Bergland, A.; Rydwik, E. The importance of physical activity exercise among older people. BioMed Res. Int. 2018, 2018, 7856823. [Google Scholar] [CrossRef] [PubMed]
- Oppezzo, M.; Wegner, L.; Gross, J.J.; Schwartz, D.L.; Eckley, T.; King, A.C.; Mackey, S.; Stefanick, M.L. What Moves You? Physical Activity Strategies in Older Women. J. Health Psychol. 2022, 27, 2027–2040. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Hernández, B.M.; Rosas-Carrasco, O.; López-Teros, M.; González-Rocha, A.; Muñoz-Aguirre, P.; Palazuelos-González, R.; Ortiz-Rodríguez, A.; Luna-López, A.; Denova-Gutiérrez, E. Association between Physical Activity and Physical and Functional Performance in Non-Institutionalized Mexican Older Adults: A Cohort Study. BMC Geriatr. 2022, 22, 388. [Google Scholar] [CrossRef]
- Lau, L.K.; Tou, N.X.; Jabbar, K.A.; Tang, J.Y.; Gao, J.; Ding, Y.Y.; Ng, Y.S. Effects of Exercise Interventions on Physical Performance and Activities of Daily Living in Oldest-Old and Frail Older Adults: A Review of the Literature. Am. J. Phys. Med. Rehabil. 2023, 102, 939–949. [Google Scholar] [CrossRef]
- Subías-Perié, J.; Navarrete-Villanueva, D.; Gómez-Cabello, A.; Vicente-Rodríguez, G.; Casajús, J.A. Health Economic Evaluation of Exercise Interventions in People over 60 Years Old: A Systematic Review. Exp. Gerontol. 2022, 161, 111713. [Google Scholar] [CrossRef]
- Hernandez-Martinez, J.; Cid-Calfucura, I.; Chiguay, C.; Weinberger, M.; Delgado-Floody, P.; Muñoz-Vásquez, C.; Aristegui-Mondaca, J.; Levín-Catrilao, Á.; Herrera-Valenzuela, T.; Branco, B.H.M.; et al. Effects of Elastic Band Training on Body Composition and Physical Performance in Older People: A Systematic Review with Meta-Analysis. Exp. Gerontol. 2024, 196, 112553. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Ramirez-Campillo, R.; Herrera-Valenzuela, T.; Branco, B.H.M.; Guzmán-Muñoz, E.; Mendez-Rebolledo, G.; Concha-Cisternas, Y.; Hernandez-Martínez, J. Effectiveness of Olympic Combat Sports on Balance, Fall Risk or Falls in Older Adults: A Systematic Review. Biology 2022, 11, 74. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Herrera-Valenzuela, T.; Ramirez-Campillo, R.; Aedo-Muñoz, E.; Báez-San Martín, E.; Ojeda-Aravena, A.; Branco, B.H.M. Effects of Olympic Combat Sports on Older Adults’ Health Status: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7381. [Google Scholar] [CrossRef]
- Dunn, D.T.; Stirrup, O.T.; McCormack, S.; Glidden, D.V. Interpretation of Active-Control Randomised Trials: The Case for a New Analytical Perspective Involving Averted Events. BMC Med. Res. Methodol. 2023, 23, 149. [Google Scholar] [CrossRef]
- Hernandez-Martinez, J.; Guzmán-Muñoz, E.; Cid-Calfucura, I.; Villalobos-Fuentes, F.; Diaz-Saldaña, D.; Alvarez-Martinez, I.; Castillo-Cerda, M.; Herrera-Valenzuela, T.; Branco, B.H.M.; Valdés-Badilla, P. Elastic Band Training Versus Multicomponent Training and Group-Based Dance on Morphological Variables and Physical Performance in Older Women: A Randomized Controlled Trial. Life 2024, 14, 1362. [Google Scholar] [CrossRef] [PubMed]
- Valdés-Badilla, P.; Guzmán-Muñoz, E.; Hernandez-Martinez, J.; Núñez-Espinosa, C.; Delgado-Floody, P.; Herrera-Valenzuela, T.; Branco, B.H.M.; Zapata-Bastias, J.; Nobari, H. Effectiveness of Elastic Band Training and Group-Based Dance on Physical-Functional Performance in Older Women with Sarcopenia: A Pilot Study. BMC Public Health 2023, 23, 2113. [Google Scholar] [CrossRef]
- Combs, S.A.; Diehl, M.D.; Chrzastowski, C.; Didrick, N.; McCoin, B.; Mox, N.; Staples, W.H.; Wayman, J. Community-Based Group Exercise for Persons with Parkinson Disease: A Randomized Controlled Trial. NeuroRehabilitation 2013, 32, 117–124. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Herrera-Valenzuela, T.; Guzmán-Muñoz, E.; Hernandez-Martinez, J.; Cid-Calfucura, I.; Vásquez-Carrasco, E.; Aristegui-Mondaca, J.; Aravena-Sagardia, P.; Mota, J.; Zapata-Bastias, J.; et al. Adapted Taekwondo Improves Postural Balance and Health-Related Quality of Life Concerning Multicomponent Training and Walking Exercise in Older Females: A Randomized Controlled Trial (TKD and Aging Project). J. Clin. Med. 2024, 13, 7250. [Google Scholar] [CrossRef] [PubMed]
- Nixon, P.; Boß, L.; Heber, E.; Ebert, D.D.; Lehr, D. A Three-Armed Randomised Controlled Trial Investigating the Comparative Impact of Guidance on the Efficacy of a Web-Based Stress Management Intervention and Health Impairing and Promoting Mechanisms of Prevention. BMC Public Health 2021, 21, 1511. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Guzmán-Muñoz, E.; Herrera-Valenzuela, T.; Branco, B.H.M.; Hernandez-Martinez, J.; Nobari, H. Impact of Adapted Taekwondo vs. Multicomponent Training on Health Status in Independent Older Women: A Randomized Controlled Trial. Front. Public Health 2023, 11, 1236402. [Google Scholar] [CrossRef]
- Turner, L.; Shamseer, L.; Altman, D.G.; Weeks, L.; Peters, J.; Kober, T.; Dias, S.; Schulz, K.F.; Plint, A.C.; Moher, D. Consolidated Standards of Reporting Trials (CONSORT) and the Completeness of Reporting of Randomised Controlled Trials (RCTs) Published in Medical Journals. Cochrane Database Syst. Rev. 2012, 11, Mr000030. [Google Scholar] [CrossRef]
- Subsecretaría de Salud Pública. Manual de Aplicación del Examen de Medicina Preventiva del Adulto Mayor; Gobierno de Chile: Santiago, Chile, 2012.
- Fess, E. Clinical Assessment Recommendations; American Society of Hand Therapists: Mt. Laurel, NJ, USA, 1981; pp. 6–8. [Google Scholar]
- Hesseberg, K.; Bentzen, H.; Bergland, A. Reliability of the senior fitness test in community-dwelling older people with cognitive impairment. Physiother. Res. Int. 2015, 20, 37–44. [Google Scholar] [CrossRef]
- Mayorga-Vega, D.; Merino-Marban, R.; Viciana, J. Criterion-Related Validity of Sit-and-Reach Tests for Estimating Hamstring and Lumbar Extensibility: A Meta-Analysis. J. Sports Sci. Med. 2014, 13, 1–14. [Google Scholar] [PubMed]
- Marfell-Jones, M.; Olds, T.; De Ridder, J. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2001. [Google Scholar]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; De Ridder, H. International Society for Advancement of Kinanthropometry. Int. Stand. Anthr. Assess. 2011, 115. [Google Scholar]
- Kartikasari, R.D.; Pawana, I.P.A.; Utami, D.A.; Melaniani, S. The Effect of Adding Exergame Boxing to Balance Functions of Elderly Women. Bali Med. J. 2023, 12, 2642–2645. [Google Scholar] [CrossRef]
- Chrysagis, N.; Trompouki, G.; Petropaulis, D.; Koumantakis, G.A.; Krekoukias, G.; Theotokatos, G.; Skordilis, E.; Sakellari, V. Effect of Boxing Exercises on the Functional Ability and Quality of Life of Individuals with Parkinson’s Disease: A Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 1295–1310. [Google Scholar] [CrossRef]
- Colado, J.C.; Pedrosa, F.M.; Juesas, A.; Gargallo, P.; Carrasco, J.J.; Flandez, J.; Chupel, M.U.; Teixeira, A.M.; Naclerio, F. Concurrent Validation of the OMNI-Resistance Exercise Scale of Perceived Exertion with Elastic Bands in the Elderly. Exp. Gerontol. 2018, 103, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Oh, S.-L.; Kim, H.-J.; Woo, S.; Cho, B.-L.; Song, M.; Park, Y.-H.; Lim, J.-Y.; Song, W. Effects of an Integrated Health Education and Elastic Band Resistance Training Program on Physical Function and Muscle Strength in Community-Dwelling Elderly Women: Healthy Aging and Happy Aging II Study. Geriatr. Gerontol. Int. 2017, 17, 825–833. [Google Scholar] [CrossRef]
- Barbosa, S.S.; Sousa, L.C.M.; de Oliveira Silva, D.F.; Pimentel, J.B.; Evangelista, K.; Lyra, C.O.; Lopes, M.; Lima, S. A Systematic Review on Processed/Ultra-Processed Foods and Arterial Hypertension in Adults and Older People. Nutrients 2022, 14, 1215. [Google Scholar] [CrossRef] [PubMed]
- Lancha, A.H., Jr.; Zanella, R., Jr.; Tanabe, S.G.; Andriamihaja, M.; Blachier, F. Dietary Protein Supplementation in the Elderly for Limiting Muscle Mass Loss. Amino Acids 2017, 49, 33–47. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.M.; Hurr, C.; Kim, S. Effects of Elastic Band Exercise on Functional Fitness and Blood Pressure Response in the Healthy Elderly. Int. J. Environ. Res. Public Health 2020, 17, 7144. [Google Scholar] [CrossRef]
- Lee, S.H.; Scott, S.D.; Pekas, E.J.; Lee, S.; Lee, S.H.; Park, S.Y. Taekwondo Training Reduces Blood Catecholamine Levels and Arterial Stiffness in Postmenopausal Women with Stage-2 Hypertension: Randomized Clinical Trial. Clin. Exp. Hypertens. 2019, 41, 675–681. [Google Scholar] [CrossRef]
- Andersen, V.; Prieske, O.; Stien, N.; Cumming, K.; Solstad, T.E.J.; Paulsen, G.; van den Tillaar, R.; Pedersen, H.; Saeterbakken, A.H. Comparing the Effects of Variable and Traditional Resistance Training on Maximal Strength and Muscle Power in Healthy Adults: A Systematic Review and Meta-Analysis. J. Sci. Med. Sport 2022, 25, 1023–1032. [Google Scholar] [CrossRef]
- Bergquist, R.; Iversen, V.M.; Mork, P.J.; Fimland, M.S. Muscle Activity in Upper-Body Single-Joint Resistance Exercises with Elastic Resistance Bands vs. Free Weights. J. Hum. Kinet. 2018, 61, 5–13. [Google Scholar] [CrossRef]
- Baek, S.H.; Hong, G.R.; Min, D.K.; Kim, E.H.; Park, S.K. Effects of Functional Fitness Enhancement through Taekwondo Training on Physical Characteristics and Risk Factors of Dementia in Elderly Women with Depression. Int. J. Environ. Res. Public Health 2021, 18, 7961. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Aguilar, D.; Valdés-Badilla, P.; Herrera-Valenzuela, T.; Guzmán-Muñoz, E.; Magnani Branco, B.H.; Méndez-Rebolledo, G.; López-Fuenzalida, A. ¿Bandas Elásticas o Equipos de Gimnasio para el Entrenamiento de Adultos Mayores? (Elastic Bands or Gym Equipment for the Training of Older Adults?). Retos 2020, 37, 370–378. [Google Scholar] [CrossRef]
- Herman, T.; Giladi, N.; Hausdorff, J.M. Properties of the ‘timed up and go’ test: More than meets the eye. Gerontology 2011, 57, 203–210. [Google Scholar] [CrossRef]
- Fort Vanmeerhaeghe, A.; Romero Rodriguez, D. Rol del sistema sensoriomotor en la estabilidad articular durante las actividades deportivas. Apunts Med. Esport 2013, 48, 69–76. [Google Scholar] [CrossRef]
- Stanley, E.; Thomson, E.; Smith, G.; Lamb, K. An Analysis of the Three-Dimensional Kinetics and Kinematics of Maximal Effort Punches among Amateur Boxers. Int. J. Perform. Anal. Sport 2018, 18, 835–854. [Google Scholar] [CrossRef]
- Stojanović, M.D.M.; Mikić, M.J.; Milošević, Z.; Vuković, J.; Jezdimirović, T.; Vučetić, V. Effects of Chair-Based, Low-Load Elastic Band Resistance Training on Functional Fitness and Metabolic Biomarkers in Older Women. J. Sports Sci. Med. 2021, 20, 133–141. [Google Scholar] [CrossRef]
- Berlanga, L.A.; Matos-Duarte, M.; Abdalla, P.; Alves, E.; Mota, J.; Bohn, L. Validity of the two-minute step test for healthy older adults. Geriatr. Nurs. 2023, 51, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Ezzatvar, Y.; Ramírez-Vélez, R.; Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Izquierdo, M.; García-Hermoso, A. Physical Function and All-Cause Mortality in Older Adults Diagnosed with Cancer: A Systematic Review and Meta-Analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 76, 1447–1453. [Google Scholar] [CrossRef]
- Lohakare, P.K.; Jiandani, M.P. Two-Minute Step Test: Estimating Normative Reference Values in Healthy Adults. J. Soc. Indian Physiother. 2023, 7, 27–32. [Google Scholar] [CrossRef]
- Jofré-Saldía, E.; Villalobos-Gorigoitía, Á.; Gea-García, G. Methodological Proposal for Strength and Power Training in Older Athletes: A Narrative Review. Curr. Aging Sci. 2022, 15, 135–146. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Program | Duration (Weeks) | Frequency (Weekly) | Time × Session (min) | Physical Exercise | Sets and Repetitions | Recovery | Intensity |
|---|---|---|---|---|---|---|---|
| TKD | 1–2 | 2 | 60 | Upper limb | 3–8 | 2 min | OMNI-RES (5–8 points) |
| 3–5 | Lower limb | 4–8 | 2 min | ||||
| 6–8 | 4–12 | 90 s | |||||
| BOX | 1–2 | 60 | Upper limb | 3–8 | 2 min | OMNI-RES (5–8 points) | |
| 3–5 | Lower limb | 4–8 | 2 min | ||||
| 6–8 | 4–12 | 90 s | |||||
| EBT | 1–4 | 60 | Whole body | OMNI-RES (5–8 points) | |||
| 5–8 | 2–10 to 15 | 60 s |
| Variable | Assessment | TKD Group (n = 10) | BOX Group (n = 10) | EBT (n = 10) |
|---|---|---|---|---|
| Age (years) | 72 (7.09) | 71.8 (2.92) | 71.6 (2.88) | |
| Anthropometric parameters | Bipedal height (cm) | 1.58 (0.05) | 1.61 (0.07) | 1.60 (0.05) |
| Body mass (kg) | 71.7 (12.0) | 70.7 (13.0) | 71.4 (19.4) | |
| BMI (kg/m2) | 28.7 (8.1) | 27.3 (7.3) | 27.9 (9.2) | |
| Academic level | Primary (%) | 17 | 16 | 12 |
| Secondary (%) | 11 | 13 | 16 | |
| Bachelor (%) | 3 | 5 | 7 | |
| Postgraduate (%) | 0 | 0 | 0 | |
| Civil status | Married (%) | 32 | 16 | 18 |
| Separated (%) | 7 | 9 | 4 | |
| Widowed (%) | 3 | 5 | 6 | |
| Single (%) | 0 | 0 | 0 | |
| Group | Before | After | Time × Group p Value | Time × Group F Value | ηp2 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | |||||
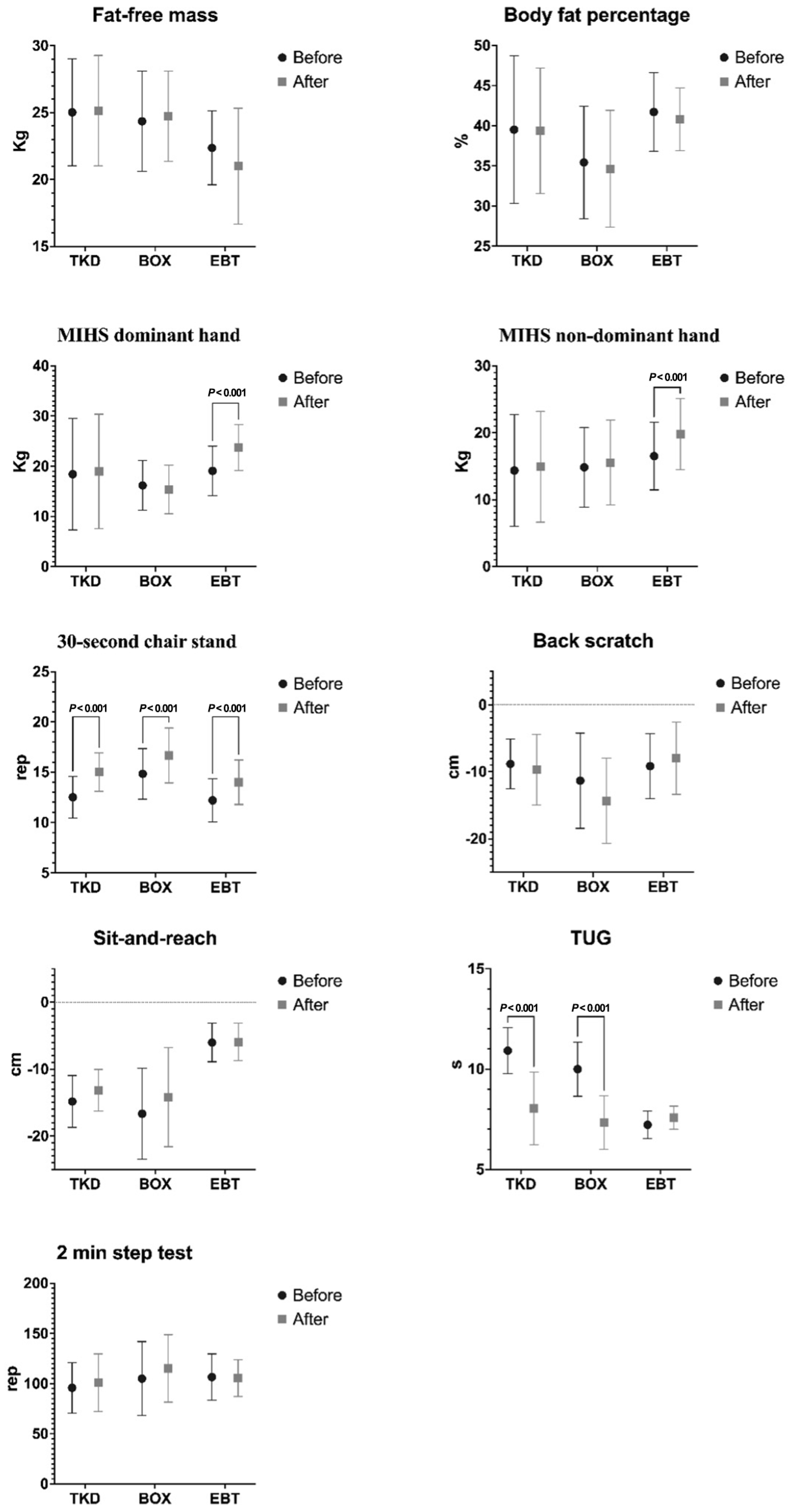
| Fat-free mass (kg) | TKD | 25.0 | 9.2 | 22.5–27.5 | 25.2 | 7.8 | 22.5–27.8 | 0.306 | 0.738 | 0.019 |
| BOX | 24.4 | 7.0 | 22.0–26.7 | 24.7 | 7.3 | 22.6–26.9 | ||||
| EBT | 22.4 | 4.9 | 20.4–24.3 | 21.0 | 3.9 | 17.9–24.1 | ||||
| Body fat percentage (%) | TKD | 39.5 | 9.2 | 33.7–45.4 | 39.4 | 7.8 | 34.4–44.4 | 0.091 | 2.588 | 0.143 |
| BOX | 35.4 | 7.0 | 31.0–39.9 | 34.6 | 7.3 | 30.0–39.3 | ||||
| EBT | 41.7 | 6.5 | 38.2–45.2 | 40.8 | 6.0 | 38.0–43.6 | ||||
| MIHS dominant hand (kg) | TKD | 18.4 | 4.3 | 11.4–25.5 | 19.0 | 3.1 | 11.7–26.2 | <0.001 | 55.940 | 0.783 |
| BOX | 16.2 | 4.6 | 13.0–19.3 | 15.4 | 3.6 | 12.3–18.4 | ||||
| EBT | 19.1 | 4.9 | 15.6–22.6 | 23.7 | 6.1 | 20.4–27.0 | ||||
| MIHS non-dominant hand (kg) | TKD | 14.4 | 11.1 | 9.1–19.7 | 14.9 | 11.4 | 9.7–20.2 | <0.001 | 29.180 | 0.652 |
| BOX | 14.8 | 5.0 | 11.1–18.6 | 15.6 | 4.8 | 11.5–19.6 | ||||
| EBT | 16.5 | 4.9 | 12.9–20.1 | 19.8 | 4.6 | 16.0–23.6 | ||||
| 30 s chair stand (rep) | TKD | 12.5 | 8.3 | 11.2–13.8 | 15.0 | 8.3 | 13.8–16.2 | 0.211 | 1.636 | 0.095 |
| BOX | 14.8 | 6.0 | 13.2–16.4 | 16.7 | 6.3 | 14.9–18.4 | ||||
| EBT | 12.2 | 5.0 | 10.7–13.7 | 14.0 | 5.3 | 12.4–15.6 | ||||
| Back scratch (cm) | TKD | −8.8 | 2.1 | −11.2–6.5 | −9.7 | 1.9 | −13.0–6.3 | 0.084 | 2.665 | 0.139 |
| BOX | −11.3 | 2.5 | −15.8–6.8 | −14.3 | 2.7 | −18.4–10.3 | ||||
| EBT | −9.2 | 2.1 | −12.3–6.1 | −8.0 | 2.2 | −11.4–4.6 | ||||
| Sit-and-reach (cm) | TKD | −14.8 | 3.7 | −17.3–12.4 | −13.2 | 5.3 | −15.2–11.2 | 0.168 | 1.882 | 0.102 |
| BOX | −16.7 | 7.1 | −21.0–12.4 | −14.2 | 6.4 | −18.9–9.5 | ||||
| EBT | −6.0 | 4.9 | −7.8–4.2 | −5.9 | 5.4 | −7.7–4.1 | ||||
| TUG (seg) | TKD | 10.9 | 3.9 | 10.2–11.6 | 8.0 | 3.1 | 6.9–9.2 | <0.001 | 21.770 | 0.584 |
| BOX | 10.0 | 6.8 | 9.1–10.9 | 7.3 | 7.4 | 6.5–8.2 | ||||
| EBT | 7.2 | 2.9 | 6.7–7.7 | 7.6 | 2.8 | 7.2–8.0 | ||||
| 2 min step test (rep) | TKD | 95.8 | 1.1 | 79.8–111.9 | 101.0 | 1.8 | 82.8–119.2 | 0.166 | 1.982 | 0.113 |
| BOX | 105.0 | 1.3 | 81.6–128.4 | 115.2 | 1.3 | 93.8–136.5 | ||||
| EBT | 106.6 | 0.7 | 90.1–123.1 | 105.4 | 0.6 | 92.3–118.5 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vásquez-Carrasco, E.; Hernandez-Martinez, J.; Cid-Calfucura, I.; Guzmán-Muñoz, E.; Ruiz, C.; Baeza, C.; Márquez, M.J.; Herrera-Valenzuela, T.; Branco, B.H.M.; Carmine-Peña, E.; et al. Effects of Different Interventions Using Taekwondo, Boxing, and Elastic Band Training on Body Composition and Physical Function in Chilean Older Women: A Randomized Controlled Trial. Life 2025, 15, 1049. https://doi.org/10.3390/life15071049
Vásquez-Carrasco E, Hernandez-Martinez J, Cid-Calfucura I, Guzmán-Muñoz E, Ruiz C, Baeza C, Márquez MJ, Herrera-Valenzuela T, Branco BHM, Carmine-Peña E, et al. Effects of Different Interventions Using Taekwondo, Boxing, and Elastic Band Training on Body Composition and Physical Function in Chilean Older Women: A Randomized Controlled Trial. Life. 2025; 15(7):1049. https://doi.org/10.3390/life15071049
Chicago/Turabian StyleVásquez-Carrasco, Edgar, Jordan Hernandez-Martinez, Izham Cid-Calfucura, Eduardo Guzmán-Muñoz, Camila Ruiz, Camila Baeza, María José Márquez, Tomás Herrera-Valenzuela, Braulio Henrique Magnani Branco, Eduardo Carmine-Peña, and et al. 2025. "Effects of Different Interventions Using Taekwondo, Boxing, and Elastic Band Training on Body Composition and Physical Function in Chilean Older Women: A Randomized Controlled Trial" Life 15, no. 7: 1049. https://doi.org/10.3390/life15071049
APA StyleVásquez-Carrasco, E., Hernandez-Martinez, J., Cid-Calfucura, I., Guzmán-Muñoz, E., Ruiz, C., Baeza, C., Márquez, M. J., Herrera-Valenzuela, T., Branco, B. H. M., Carmine-Peña, E., Sepúlveda, P., Sandoval, C., & Valdés-Badilla, P. (2025). Effects of Different Interventions Using Taekwondo, Boxing, and Elastic Band Training on Body Composition and Physical Function in Chilean Older Women: A Randomized Controlled Trial. Life, 15(7), 1049. https://doi.org/10.3390/life15071049