
Prodromal Parkinsonian Features in Carriers of Gaucher Disease Compared to Controls

 ,
,  , , , , and
, , , , and 
Abstract
1. Introduction
2. Methods
2.1. Study Population
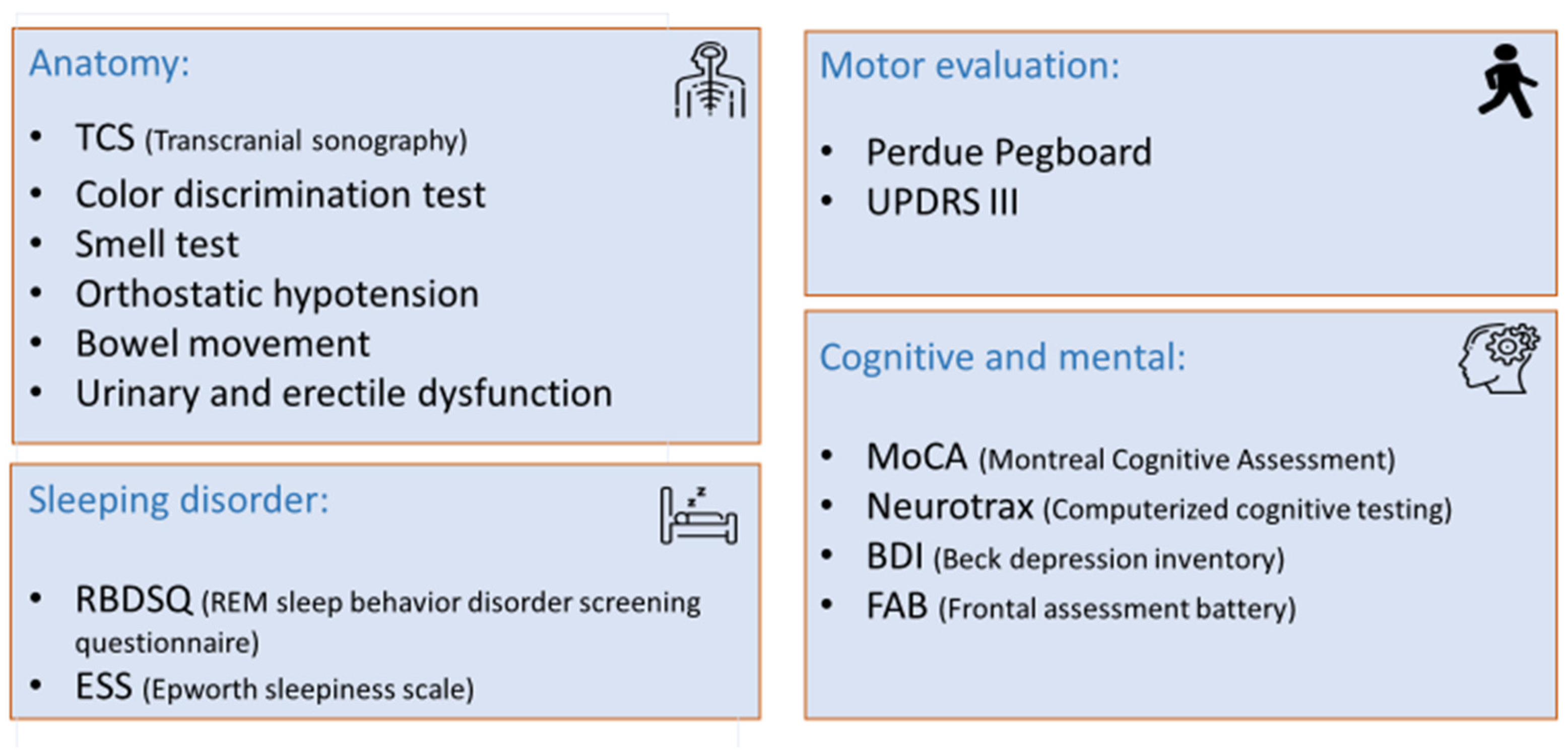
2.2. Prodromal PD Features Evaluation
2.3. Statistical Analysis
2.3.1. Rate of Abnormal Prodromal Tests
- The cutoff defined in the literature [9].
- 10th percentile—the top, worst 10% of each test in the controls ordered from best to worst.
- 25th percentile—the top, worst 25% of each test in the controls ordered from best to worst.
- Outliers—scores of >1.5 IQR (Inter Quartile Range) from Q3 (the third quartile) in the box plot values for the controls.
- Above 1.64 z-score—each test in the GBA1 carriers group was converted to z-score values, and the cutoff value was determined above 1.64 SD.
- Above 1.96 z-score—each test in the GBA1 carriers group was converted to z-score values, and the cutoff value was determined above 1.96 SD.
2.3.2. Risk Factors for Having Abnormal Prodromal Tests
2.3.3. Principal Component Analysis
3. Results
3.1. Participant Characteristics
3.2. Rate of Abnormal Testing in GBA1 Carriers Compared to Controls
3.3. Risk Factors for Abnormal Prodromal Tests
3.4. Patterns of Principal Component Analysis and Percentage of Variance Explained by Components
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Revel-Vilk, S.; Szer, J.; Zimran, A. Gaucher Disease and Related Lysosomal Storage Diseases. In Williams Hematology, 10th ed.; Kaushansky, K., Prchal, J.T., Burns, L.J., Lichtman, M.A., Levi, M., Linch, D.C., Eds.; McGraw-Hill Education: New York, NY, USA, 2021. [Google Scholar]
- Horowitz, M.; Braunstein, H.; Zimran, A.; Revel-Vilk, S.; Goker-Alpan, O. Lysosomal functions and dysfunctions: Molecular and cellular mechanisms underlying Gaucher disease and its association with Parkinson disease. Adv. Drug Deliv. Rev. 2022, 187, 114402. [Google Scholar] [CrossRef] [PubMed]
- Skrahin, A.; Horowitz, M.; Istaiti, M.; Skrahina, V.; Lukas, J.; Yahalom, G.; Cohen, M.E.; Revel-Vilk, S.; Goker-Alpan, O.; Becker-Cohen, M.; et al. GBA1-Associated Parkinson’s Disease Is a Distinct Entity. Int. J. Mol. Sci. 2024, 25, 7102. [Google Scholar] [CrossRef] [PubMed]
- Westenberger, A.; Skrahina, V.; Usnich, T.; Beetz, C.; Vollstedt, E.J.; Laabs, B.H.; Paul, J.J.; Curado, F.; Skobalj, S.; Gaber, H.; et al. Relevance of genetic testing in the gene-targeted trial era: The Rostock Parkinson’s disease study. Brain 2024, 147, 2652–2667. [Google Scholar] [CrossRef] [PubMed]
- Istaiti, M.; Yahalom, G.; Cohen, M.; Skrahina, V.; Skrahin, A.; Lukas, J.; Rolfs, A.; Zimran, A. The Sidransky Syndrome- GBA1 related Parkinson’s disease and its targeted therapies. Int. J. Mol. Sci. 2025, 26, 3435. [Google Scholar] [CrossRef] [PubMed]
- Sidransky, E.; Nalls, M.A.; Aasly, J.O.; Aharon-Peretz, J.; Annesi, G.; Barbosa, E.R.; Bar-Shira, A.; Berg, D.; Bras, J.; Brice, A.; et al. Multicenter Analysis of Glucocerebrosidase Mutations in Parkinson’s Disease. N. Engl. J. Med. 2009, 361, 1651–1661. [Google Scholar] [CrossRef] [PubMed]
- Gan-Or, Z.; Amshalom, I.; Kilarski, L.L.; Bar-Shira, A.; Gana-Weisz, M.; Mirelman, A.; Marder, K.; Bressman, S.; Giladi, N.; Orr-Urtreger, A. Differential effects of severe vs mild GBA mutations on Parkinson disease. Neurology 2015, 84, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.; Postuma, R.B.; Adler, C.H.; Bloem, B.R.; Chan, P.; Dubois, B.; Gasser, T.; Goetz, C.G.; Halliday, G.; Joseph, L.; et al. MDS research criteria for prodromal Parkinson’s disease. Mov. Disord. 2015, 30, 1600–1611. [Google Scholar] [CrossRef] [PubMed]
- Becker-Cohen, M.; Zimran, A.; Dinur, T.; Tiomkin, M.; Cozma, C.; Rolfs, A.; Arkadir, D.; Shulman, E.; Manor, O.; Paltiel, O.; et al. A Comprehensive Assessment of Qualitative and Quantitative Prodromal Parkinsonian Features in Carriers of Gaucher Disease—Identifying Those at the Greatest Risk. Int. J. Mol. Sci. 2022, 23, 12211. [Google Scholar] [CrossRef] [PubMed]
- Narita, A.; Shirai, K.; Itamura, S.; Matsuda, A.; Ishihara, A.; Matsushita, K.; Fukuda, C.; Kubota, N.; Takayama, R.; Shigematsu, H.; et al. Ambroxol chaperone therapy for neuronopathic Gaucher disease: A pilot study. Ann. Clin. Transl. Neurol. 2016, 3, 200–215. [Google Scholar] [CrossRef] [PubMed]
- Aries, C.; Lohmöller, B.; Tiede, S.; Täuber, K.; Hartmann, G.; Rudolph, C.; Muschol, N. Promising Effect of High Dose Ambroxol Treatment on Neurocognition and Motor Development in a Patient With Neuropathic Gaucher Disease 2. Front. Neurol. 2022, 13, 907317. [Google Scholar] [CrossRef] [PubMed]
- Maor, G.; Cabasso, O.; Krivoruk, O.; Rodriguez, J.; Steller, H.; Segal, D.; Horowitz, M. The contribution of mutant GBA to the development of Parkinson disease in Drosophila. Hum. Mol. Genet. 2016, 25, 2712–2727. [Google Scholar] [PubMed]
- Heinzel, S.; Berg, D.; Gasser, T.; Chen, H.; Yao, C.; Postuma, R.B. Update of the MDS research criteria for prodromal Parkinson’s disease. Mov. Disord. 2019, 34, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Ebina, J.; Ebihara, S.; Kano, O. Similarities, differences and overlaps between frailty and Parkinson’s disease. Geriatr. Amp. Gerontol. Int. 2022, 22, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Lock, E.A.; Zhang, J.; Checkoway, H. Solvents and Parkinson disease: A systematic review of toxicological and epidemiological evidence. Toxicol. Appl. Pharmacol. 2013, 266, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Aarsland, D.; Creese, B.; Politis, M.; Chaudhuri, K.R.; Ffytche, D.H.; Weintraub, D.; Ballard, C. Cognitive decline in Parkinson disease. Nat. Rev. Neurol. 2017, 13, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Gaenslen, A.; Prahl, K.; Srulijes, K.; Hauser, A.K.; Schulte, C.; Csoti, I.; Berg, D.; Brockmann, K. Patient’s Perception: Shorter and More Severe Prodromal Phase in GBA-Associated PD. Eur. J. Neurol. 2019, 26, 694–698. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| GBA-1 Carriers | Controls | p-Value | |
|---|---|---|---|
| Number | 164 | 49 | |
| Male | 76 (46%) | 23 (47%) | 0.94 |
| Age, median (range) | 51.5 (36–75) | 56 (38–78) | 0.07 |
| Relatives with PD | 47 (28.8%) | 14 (28.6%) | 0.99 |
| 1st relative | 32 | 8 | |
| 2nd relative | 21 | 8 | |
| Caffeine use * | 125 (86.2%) | 31 (91%) | 0.436 |
| Smoking * | 0.401 | ||
| Current | 14 (9.6%) | 3 (8.8%) | |
| Former | 31 (21.2%) | 5 (14.7%) | |
| Never | 101 (69.2%) | 26 (76.5%) | |
| Regular pesticide exposure * | 7 (4.8%) | 2 (5.9%) | 0.681 |
| Solvent exposure * | 8 (5.5%) | 8 (23.5%) | 0.003 |
| Carriers of GD | n = 123 | Patients with GD | n = 41 |
|---|---|---|---|
| N370S/wt | 87 (71%) | N370S/N370S | 28 (68%) |
| 84GG/wt | 13 (11%) | N370S/84GG | 4 (10%) |
| L444P/wt | 9 (7%) | N370S/L444P | 2 (5%) |
| R496H/wt | 4 (3%) | N370S/R496H | 0 (0%) |
| V394L/wt | 5 (4%) | N370S/V394L | 2 (5%) |
| Other/wt | 5 (4%) | N370S/Other | 5 (12%) |
| Prodromal Feature | Literature Cutoff ** | GBA1 Carriers | Controls | p-Value |
|---|---|---|---|---|
| Transcranial ultrasonography, cm2 | ≥0.2 | 30 (19.5%) | 12 (26.1%) | 0.41 * |
| Median (range) | 0.125 (0–0.42) | 0.135 (0–0.46) | 0.45 * | |
| Color discrimination test (TES) | 40–49 years >100 | 2 (1.3%) | 0 | 0.99 |
| 50–59 years >130 | ||||
| 60–69 years >170 | ||||
| 70–79 years >195 | ||||
| Median (range) | 40 (0–171) | 45.5 (8–154) | 0.59 | |
| UPSIT—smell test | <8 | 23 (14.4%) | 6 (12.5%) | 0.94 |
| Median (range) | 10 (0–12) | 10 (6–12) | 0.72 | |
| Orthostatic hypotension | >20 SBP or >10 mmHg DBP | 30 (21%) | 10 (25%) | 0.66 * |
| Bowel movement (daily) | ≤0.5 | 10 (6.4%) | 5 (10.6%) | 0.36 |
| Urinary dysfunction | Yes/No | 23 (16%) | 5 (14.7%) | 0.99 * |
| Erectile dysfunction | Yes/No | 5 (9.4%) | 0 (0%) | 0.57 * |
| Beck depression inventory | ≥14 | 15 (9.9%) | 3 (6.4%) | 0.57 * |
| Median (range) | 4 (0–25) | 4 (0–16.5) | 0.78 * | |
| Frontal assessment battery | <16 | 1 (0.7%) | 0 | 0.99 * |
| Median (range) | 18 (15–18) | 18 (16–18) | 0.26 * | |
| MoCA—Total score | ≤25 | 37 (23.9%) | 9 (20%) | 0.67 * |
| Median (range) | 27 (21–30) | 27 (22–30) | 0.63 * | |
| MoCA—Visuospatial/executive | ≤3 | 38 (24.8%) | 10 (21.7%) | 0.75 |
| Median (range) | 4 (2–5) | 4 (2–5) | 0.65 * | |
| Neurotrax—Memory | <85 | 12 (7.2%) | 4 (8.2%) | 0.93 |
| Median (range) | 104.5 (61.1–115.7) | 102.5 (68.8–111.8) | 0.57 | |
| Neurotrax—Executive function | <85 | 6 (3.6%) | 2 (4.1%) | 0.99 |
| Median (range) | 107.5 (77.7–134.2) | 107.9 (72.3–119) | 0.48 | |
| Neurotrax—Attention | <85 | 5 (3%) | 2 (4.1%) | 0.93 |
| Median (range) | 104.6 (63.5–119.4) | 104.2 (70.7–116.5) | 0.36 | |
| Neurotrax—Information processing speed | <85 | 15 (9.1%) | 4 (8.2%) | 0.51 |
| Median (range) | 102.95 (25–150.1) | 104.6 (25–133.7) | 0.75 | |
| Neurotrax—Visual spatial | <85 | 19 (11.4%) | 5 (10.2%) | 0.81 |
| Median (range) | 105.4 (59–138.6) | 108.9 (77.70–133.40) | 0.64 | |
| Neurotrax—Verbal function | <85 | 13 (7.9%) | 8 (16.3%) | 0.14 |
| Median (range) | 104.2 (25–116.4) | 101.8 (25–114.6) | 0.01 | |
| Neurotrax—Motor skills | <85 | 5 (3%) | 4 (8.2%) | 0.25 |
| Median (range) | 108.4 (25–120.8) | 106.7 (25–121) | 0.14 | |
| Neurotrax—Global cognitive score | <85 | 4 (2.4%) | 1 (2%) | 0.99 |
| Median (range) | 105.15 (75.20–121.3) | 103.80 (79.80–116.4) | 0.38 | |
| REM sleep behavior disorder | ≥5 | 18 (11.7%) | 11 (22.9%) | 0.15 |
| Median (range) | 2 (0–12) | 2 (0–7) | 0.49 * | |
| Epworth sleepiness scale | >10 | 24 (15.1%) | 4 (8.3%) | 0.34 |
| Median (range) | 6 (0–20) | 6 (1–20) | 0.48 * | |
| Purdue pegboard | <11 | 2 (1.3%) | 0 (0%) | 0.99 |
| Median (range) | 21 (9.7–32.3) | 20.8 (12.7–30.3) | 0.79 * | |
| UPDRS-III | >10 | 7 (5%) | 1 (2.5%) | 0.81 |
| Median (range) | 2 (0–18) | 2 (0–12) | 0.01 * |
| No Ab Tests | <20% Ab Tests | ≥20% Ab Tests | p-Value | |
|---|---|---|---|---|
| Number | 45 | 141 | 27 | |
| Age, median (range) | 46 (39–70) | 53 (36–78) | 58 (40–73) | 0.004 |
| Carriers | 34 (75.6%) | 111 (78.7%) | 19 (70.4%) | 0.74 ** |
| Male | 15 (33.3%) | 71 (50.4%) | 13 (48.1%) | 0.12 ** |
| Relatives with PD | 13 (29.5%) | 39 (27.7%) | 9 (33.3%) | 0.813 ** |
| Caffeine use * | 8 (18.2%) | 24 (17%) | 8 (29.6%) | 0.23 ** |
| Smoking * | 0.93 ** | |||
| Current | 4 (11.1%) | 10 (8.1%) | 3 (14.3%) | |
| Former | 7 (19.4%) | 26 (21.1%) | 3 (14.3%) | |
| Never | 25 (69.4%) | 87 (70.7%) | 15 (71.4%) | |
| Regular pesticides exposure * | 0 | 6 (4.9%) | 3 (14.3%) | 0.02 ** |
| Solvent exposure * | 3 (8.3%) | 7 (5.7%) | 6 (28.6%) | 0.04 ** |
| GBA1 Carriers | |||
|---|---|---|---|
| Component | Component 1 | Component 2 | Component 3 |
| Domain | Cognitive | Cognitive and Motor | Sleep and Cognitive |
| Tests | Executive function (0.804) | MoCA (0.590) | TCS (0.431) |
| Attention (0.768) | FAB Score (0.553) | Verbal function (0.366) | |
| Information processing speed (0.785) | Memory (0.456) | ESS (−0.514) | |
| Visual spatial (0.483) | Both hands (0.625) | BDI (−0.706) | |
| Motor skills (0.535) | Colour discrimination (−0.747) | RBD (−0.633) | |
| Smell test (0.351) | |||
| UPDRS (−0.384) | |||
| Variance explained | 23.40% | 11.10% | 8.70% |
| Control | |||
|---|---|---|---|
| Component | Component 1 | Component 2 | Component 3 |
| Domain | Cognitive, Sleep & Mood | Cognition | Motor & Autonomic Functions |
| Tests | Executive function (0.660) | MoCA (0.772) | Both hands (0.603) |
| Attention (0.690) | Memory (0.828) | Bowel movements (0.598) | |
| Information processing speed (0.529) | Visual spatial (0.705) | Motor skills (0.316) | |
| FAB Score (0.601) | Verbal function (0.455) | UPDRS (−0.556) | |
| ESS (−0.563) | Colour discrimination (−0.448) | TCS (−0.754) | |
| BDI (−0.542) | Smell test (0.304) | ||
| RBD (−0.554) | |||
| Variance explained | 20.60% | 12.60% | 10.10% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker-Cohen, M.; Zimran, A.; Dinur, T.; Tiomkin, M.; Rolfs, A.; Arkadir, D.; Bauer, P.; Shulman, E.; Yahalom, G.; Cohen, M.E.; et al. Prodromal Parkinsonian Features in Carriers of Gaucher Disease Compared to Controls. Life 2025, 15, 952. https://doi.org/10.3390/life15060952
Becker-Cohen M, Zimran A, Dinur T, Tiomkin M, Rolfs A, Arkadir D, Bauer P, Shulman E, Yahalom G, Cohen ME, et al. Prodromal Parkinsonian Features in Carriers of Gaucher Disease Compared to Controls. Life. 2025; 15(6):952. https://doi.org/10.3390/life15060952
Chicago/Turabian StyleBecker-Cohen, Michal, Ari Zimran, Tama Dinur, Maayan Tiomkin, Arndt Rolfs, David Arkadir, Peter Bauer, Elena Shulman, Gilad Yahalom, Mikhal E. Cohen, and et al. 2025. "Prodromal Parkinsonian Features in Carriers of Gaucher Disease Compared to Controls" Life 15, no. 6: 952. https://doi.org/10.3390/life15060952
APA StyleBecker-Cohen, M., Zimran, A., Dinur, T., Tiomkin, M., Rolfs, A., Arkadir, D., Bauer, P., Shulman, E., Yahalom, G., Cohen, M. E., Manor, O., Paltiel, O., & Revel-Vilk, S. (2025). Prodromal Parkinsonian Features in Carriers of Gaucher Disease Compared to Controls. Life, 15(6), 952. https://doi.org/10.3390/life15060952