

Impact of SGLT2 Inhibitors on Cardiovascular Risk Scores, Metabolic Parameters, and Laboratory Profiles in Type 2 Diabetes


Abstract
1. Introduction
2. Methods
2.1. Ethical Considerations
2.2. Study Design and Setting
2.3. Study Population
2.4. Data Collection and Measurements
2.5. SCORE-2 DM Calculation
2.6. Intervention
2.7. Outcomes
2.8. Statistical Analysis
2.9. Generalized Estimating Equation (GEE) Modeling
2.10. Sample Size Determination
3. Results
3.1. Anthropometric and Blood Pressure Changes
3.2. Glycemic Control and Lipid Profile
3.3. Liver and Renal Function
3.4. Transition Analysis of Demographic and Laboratory Values (Table 2)

{kind=link}
{kind=link}
| 3rd–0th | 6th–3rd | 6th–0th | |
|---|---|---|---|
| Weight, kg, Δ (%) | −1.69 (−1.95) | −1.87 (−2.2) | −3.56 (−4.11) |
| BMI, kg/m2, Δ (%) | −0.6 (−1.9) | −0.67 (−2.16) | −1.27 (−4.02) |
| SBP, mmHg, Δ (%) | −5.21 (−3.96) | −4.0 (−3.16) | −9.21 (−7) |
| DBP, mmHg, Δ (%) | −4.51 (−5.5) | −1.65 (−2.13) | −6.16 (−7.51) |
| HbA1c, %, Δ (%) | −0.84 (−9.23) | −0.54 (−6.54) | −1.38 (−15.16) |
| FBG, mg/dL, Δ (%) | −38.56 (−17.63) | −17.83 (−9.89) | −56.39 (−25.77) |
| Urea, mg/dL, Δ (%) | 0.34 (1.01) | 0.02 (0.06) | 0.36 (1.06) |
| Creatinine, mg/dL, Δ (%) | 0.07 (7.87) | −0.01 (−1.04) | 0.06 (6.74) |
| AST, IU/L, Δ (%) | −1.49 (−4.26) | −1.31 (−3.91) | −2.8 (−8) |
| ALT, IU/L, Δ (%) | 0.79 (2.35) | 0.28 (0.82) | 1.07 (3.19) |
| Triglycerides, mg/dL, Δ (%) | −14.61 (−8.4) | −8.3 (−5.21) | −22.91 (−13.18) |
| HDL, mg/dL, Δ (%) | 0.49 (1.12) | 0.04 (0.09) | 0.53 (1.21) |
| LDL, mg/dL, Δ (%) | −9.84 (−7.81) | −4.43 (−3.81) | −14.27 (−11.32) |
3.5. Cardiovascular Risk Score
3.6. Cardiovascular Risk Transition
3.7. Very-High Risk and High-Moderate Risk Comparisons
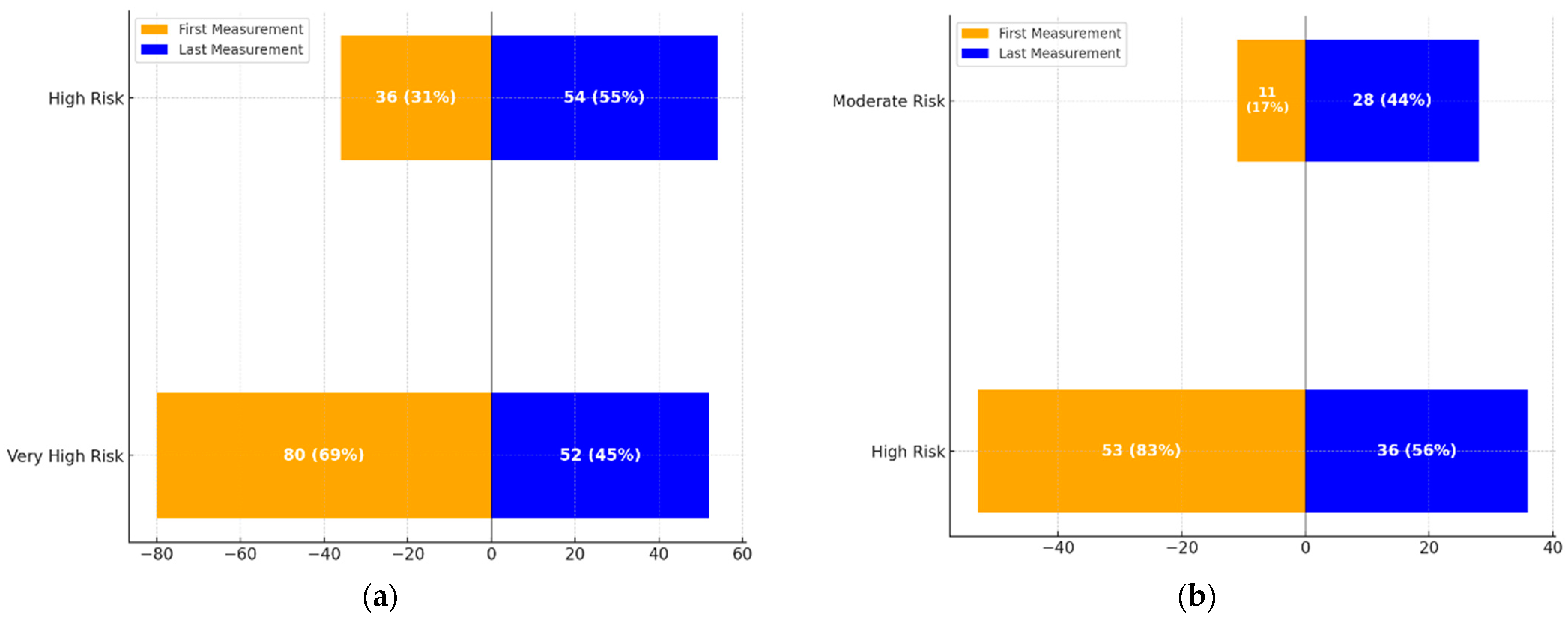
- Figure 1a: This graph demonstrates the transition dynamics between the High-Risk and Very High-Risk categories. The proportion of individuals in the High-Risk group increased from 36 (31%) to 54 (55%), while those in the Very High-Risk group decreased from 80 (69%) to 52 (45%).
- Figure 1b: This graph highlights transitions between Moderate and High-Risk categories. The Moderate-Risk group expanded from 11 (17%) to 28 (44%), while the High-Risk group saw a reduction from 53 (83%) to 36 (56%).
3.8. General Estimating Equation (GEE)
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karadeniz, A.; Babayigit, E. Effects of Sodium-Glucose Co-Transporter 2 Inhibitors on Renal and Cardiovascular Outcomes: Systematic Review. Turk. Klin. J. Med. Sci. 2021, 41, 346–352. [Google Scholar] [CrossRef]
- Vallon, V.; Verma, S. Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function. Annu. Rev. Physiol. 2021, 83, 503–528. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Gupta, A. SGLT2 inhibitors for treatment of type 2 diabetes mellitus: Focus on canagliflozin. Muller J. Med. Sci. Res. 2014, 5, 166. [Google Scholar] [CrossRef]
- The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N. Engl. J. Med. 2008, 358, 2545–2559. [Google Scholar] [CrossRef]
- Wang, X.X.; Levi, J.; Luo, Y.; Myakala, K.; Herman-Edelstein, M.; Qiu, L.; Wang, D.; Peng, Y.; Grenz, A.; Lucia, S.; et al. SGLT2 protein expression is increased in human diabetic nephropathy: SGLT2 protein inhibition decreases renal lipid accumulation, inflammation, and the development of nephropathy in diabetic mice. J. Biol. Chem. 2017, 292, 5335–5348. [Google Scholar] [CrossRef]
- Brady, J.A.; Hallow, K.M. Model-based evaluation of proximal sodium reabsorption through SGLT2 in health and diabetes and the effect of inhibition with canagliflozin. J. Clin. Pharmacol. 2018, 58, 377–385. [Google Scholar] [CrossRef]
- Ferrannini, E. Sodium-glucose co-transporters and their inhibition: Clinical physiology. Cell Metab. 2017, 26, 27–38. [Google Scholar] [CrossRef]
- Rieg, T.; Masuda, T.; Gerasimova, M.; Mayoux, E.; Platt, K.; Powell, D.R.; Thomson, S.C.; Koepsell, H.; Vallon, V. Increase in SGLT1-mediated transport explains renal glucose reabsorption during genetic and pharmacological SGLT2 inhibition in euglycemia. Am. J. Physiol.-Ren. Physiol. 2014, 306, F188–F193. [Google Scholar] [CrossRef]
- Nielsen, R.; Møller, N.; Gormsen, L.C.; Tolbod, L.P.; Hansson, N.H.; Sorensen, J.; Harms, H.J.; Frøkiær, J.; Eiskjaer, H.; Jespersen, N.R.; et al. Cardiovascular Effects of Treatment With the Ketone Body 3-Hydroxybutyrate in Chronic Heart Failure Patients. Circulation 2019, 139, 2129–2141. [Google Scholar] [CrossRef]
- Dick, S.A.; Epelman, S. Chronic Heart Failure and Inflammation: What Do We Really Know? Circ. Res. 2016, 119, 159–176. [Google Scholar] [CrossRef]
- Sossalla, S.; Fluschnik, N.; Schotola, H.; Ort, K.R.; Neef, S.; Schulte, T.; Wittköpper, K.; Renner, A.; Schmitto, J.D.; Gummert, J.; et al. Inhibition of elevated Ca2+/calmodulin-dependent protein kinase II improves contractility in human failing myocardium. Circ. Res. 2010, 107, 1150–1161. [Google Scholar] [CrossRef] [PubMed]
- Kolijn, D.; Pabel, S.; Tian, Y.; Lódi, M.; Herwig, M.; Carrizzo, A.; Zhazykbayeva, S.; Kovács, Á.; Fülöp, G.Á.; Falcão-Pires, I.; et al. Empagliflozin improves endothelial and cardiomyocyte function in human heart failure with preserved ejection fraction via reduced pro-inflammatory-oxidative pathways and protein kinase Gα oxidation. Cardiovasc. Res. 2021, 117, 495–507. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapaglifozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Biomath, D.; Devins, T.; Johansen, O.E.; et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Verma, S.; Sharma, A.; Kanumilli, N.; Butler, J. Predictors of heart failure development in type 2 diabetes: A practical approach. Curr. Opin. Cardiol. 2019, 34, 578–583. [Google Scholar] [CrossRef]
- Opingari, E.; Verma, S.; Connelly, K.A.; Mazer, C.D.; Teoh, H.; Quan, A.; Zuo, F.; Pan, Y.; Bhatt, D.L.; Zinman, B.; et al. The impact of empagliflozin on kidney injury molecule-1: A subanalysis of the Effects of Empagliflozin on Cardiac Structure, Function, and Circulating Biomarkers in Patients with Type 2 Diabetes (CardioLink-6 trial). Nephrol. Dial. Transplant. 2020, 35, 895–897. [Google Scholar] [CrossRef]
- Patel, V.B.; Shah, S.; Verma, S.; Oudit, G.Y. Epicardial adipose tissue as a metabolic transducer: Role in heart failure and coronary artery disease. Heart Fail. Rev. 2017, 22, 889–902. [Google Scholar] [CrossRef]
- Ferrannini, E.; Muscelli, E.; Frascerra, S.; Baldi, S.; Mari, A.; Heise, T.; Broedl, U.C.; Woerle, H.-J. Metabolic response to sodium-glucose cotransporter 2 inhibition in type 2 diabetic patients. J. Clin. Investig. 2014, 124, 499–508. [Google Scholar] [CrossRef]
- Lopaschuk, G.D.; Verma, S. Empagliflozin’s fuel hypothesis: Not so soon. Cell Metab. 2016, 24, 200–202. [Google Scholar] [CrossRef]
- Santos-Gallego, C.G.; Requena-Ibanez, J.A.; San, A.R.; Ishikawa, K.; Watanabe, S.; Picatoste, B.; Flores, E.; Garcia-Ropero, A.; Sanz, J.; Hajjar, R.J.; et al. Empagliflozin ameliorates adverse left ventricular remodeling in nondiabetic heart failure by enhancing myocardial energetics. J. Am. Coll. Cardiol. 2019, 73, 1931–1944. [Google Scholar] [CrossRef] [PubMed]
- Verma, S. Are the cardiorenal benefits of SGLT2 inhibitors due to inhibition of the sympathetic nervous system? JACC Basic Transl. Sci. 2020, 5, 180–182. [Google Scholar] [CrossRef] [PubMed]
- Herat, L.Y.; Magno, A.L.; Rudnicka, C.; Hricova, J.; Carnagarin, R.; Ward, N.C.; Arcambal, A.; Kiuchi, M.G.; Head, G.A.; Schlaich, M.P.; et al. SGLT2 inhibitor-induced sympathoinhibition: A novel mechanism for cardiorenal protection. JACC Basic Transl. Sci. 2020, 5, 169–179. [Google Scholar] [CrossRef]
- Marx, N.; Federici, M.; Schütt, K.; Müller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; Christodorescu, R.M.; Crawford, C.; Di Angelantonio, E.; Eliasson, B.; et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur. Heart J. 2023, 44, 4043–4140. [Google Scholar]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Hageman, S.; Pennells, L.; Ojeda, F.; Kaptoge, S.; Kuulasmaa, K.; de Vries, T.; Xu, Z.; Kee, F.; Chung, R.; Wood, A.; et al. SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [Google Scholar]
- Li, X.; Liang, J.; Hu, J.; Ma, L.; Yang, J.; Zhang, A.; Jing, Y.; Song, Y.; Yang, Y.; Feng, Z.; et al. Screening for primary aldosteronism on and off interfering medications. Endocrine 2023, 83, 178–187. [Google Scholar] [CrossRef]
- Zaccardi, F.; Webb, D.R.; Htike, Z.Z.; Youssef, D.; Khunti, K.; Davies, M.J. Efficacy and safety of sodium-glucose co-transporter-2 inhibitors in type 2 diabetes mellitus: Systematic review and network meta-analysis. Diabetes Obes. Metab. 2016, 18, 783–794. [Google Scholar] [CrossRef]
- Scheen, A.J. Reduction in HbA1c with SGLT2 inhibitors vs. DPP-4 inhibitors as add-ons to metformin monotherapy according to baseline HbA1c: A systematic review of randomized controlled trials. Diabetes Metab. 2020, 46, 186–196. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, C.; Ye, Y.; Yu, M.; Qu, X. Prospect of sodium–glucose co-transporter 2 inhibitors combined with insulin for the treatment of type 2 diabetes. Front. Endocrinol. 2020, 10, 3389. [Google Scholar] [CrossRef]
- Chen, J.; Fan, F.; Wang, J.Y.; Long, Y.; Gao, C.L.; Stanton, R.C.; Xu, Y. The efficacy and safety of SGLT2 inhibitors for adjunctive treatment of type 1 diabetes: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 44128. [Google Scholar] [CrossRef] [PubMed]
- Kamin, M.; Ishtiaq, O.; Raashid, K.; Wahab, M.U.; Khan, S.A.; Raja, U. The outcomes of dapagliflozin use in real-life clinical settings in endocrinology clinics of Islamabad, Pakistan. Cureus 2020, 12, e8565. [Google Scholar] [CrossRef] [PubMed]
- Sohail, E.; Ahsan, T.; Ghaus, S.; Aijaz, W. SGLT2 Inhibitors; glycemic control, weight loss and safety profile in patients with type 2 Diabetes, at Medicell Institute (MIDEM). Pak. J. Med. Sci. 2021, 37, 87–92. [Google Scholar]
- Prasanna Kumar, K.M.; Mohan, V.; Sethi, B.; Gandhi, P.; Bantwal, G.; Xie, J.; Meininger, G.; Qiu, R. Efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus from India. Indian J. Endocrinol. Metab. 2016, 20, 372–380. [Google Scholar] [CrossRef]
- Cai, X.; Yang, W.; Gao, X.; Chen, Y.; Zhou, L.; Zhang, S.; Han, X.; Ji, L. The association between the dosage of SGLT2 inhibitor and weight reduction in type 2 diabetes patients: A meta-analysis. Obesity 2018, 26, 70–80. [Google Scholar] [CrossRef]
- Schork, A.; Saynisch, J.; Vosseler, A.; Jaghutriz, B.A.; Heyne, N.; Peter, A.; Häring, H.-U.; Stefan, N.; Fritsche, A. Effect of SGLT2 inhibitors on body composition, fluid status and renin–angiotensin–aldosterone system in type 2 diabetes: A prospective study using bioimpedance spectroscopy. Cardiovasc. Diabetol. 2019, 18, 46. [Google Scholar] [CrossRef]
- Ghosh, A.; Gupta, R.; Singh, P.; Dutta, A.; Misra, A. Sodium-glucose cotransporter-2 inhibitors in patients with type 2 diabetes in North India: A 12-month prospective study in real-world setting. Int. J. Clin. Pract. 2018, 72, e13237. [Google Scholar] [CrossRef]
- Mayne, K.J.; Staplin, N.; Keane, D.F.; Wanner, C.; Brenner, S.; Cejka, V.; Stegbauer, J.; Judge, P.K.; Preiss, D.; Emberson, J.; et al. Effects of Empagliflozin on Fluid Overload, Weight, and Blood Pressure in CKD. J. Am. Soc. Nephrol. 2024, 35, 202–215. [Google Scholar] [CrossRef]
- Zanchi, A.; Pruijm, M.; Muller, M.E.; Ghajarzadeh-Wurzner, A.; Maillard, M.; Dufour, N.; Bonny, O.; Wuerzner, G.; Burnier, M. Twenty-Four Hour Blood Pressure Response to Empagliflozin and Its Determinants in Normotensive Non-Diabetic Subjects. Front. Cardiovasc. Med. 2022, 9, 854230. [Google Scholar] [CrossRef]
- Georgianos, P.I.; Agarwal, R. Ambulatory Blood Pressure Reduction With SGLT-2 Inhibitors: Dose-Response Meta-Analysis and Comparative Evaluation with Low-Dose Hydrochlorothiazide. Diabetes Care 2019, 42, 693–700. [Google Scholar] [CrossRef]
- Sánchez-García, A.; Simental-Mendía, M.; Millán-Alanís, J.M.; Simental-Mendía, L.E. Effect of Sodium-Glucose Co-Transporter 2 Inhibitors on Lipid Profile: A Systematic Review and Meta-Analysis of 48 Randomized Controlled Trials. Pharmacol. Res. 2020, 160, 105068. [Google Scholar] [CrossRef] [PubMed]
- Bechmann, L.E.; Emanuelsson, F.; Nordestgaard, B.G.; Benn, M. SGLT2-Inhibition Increases Total, LDL, and HDL Cholesterol and Lowers Triglycerides: Meta-Analyses of 60 Randomized Trials, Overall and by Dose, Ethnicity, and Drug Type. Atherosclerosis 2024, 394, 117236. [Google Scholar] [CrossRef] [PubMed]
- Tewari, J.; Qidwai, K.A.; Rana, A.; Tewari, A.; Tewari, V.; Maheshwari, A. Safety and Efficacy of Remogliflozin in People with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Cureus 2024, 16, e66145. [Google Scholar] [CrossRef]
- Premji, R.; Nylen, E.S.; Naser, N.; Gandhi, S.; Burman, K.D.; Sen, S. Lipid Profile Changes Associated with SGLT-2 Inhibitors and GLP-1 Agonists in Diabetes and Metabolic Syndrome. Metab. Syndr. Relat. Disord. 2022, 20, 321–328. [Google Scholar] [CrossRef]
- Xie, L.; Xia, W. Characteristics and Molecular Mechanisms through Which SGLT2 Inhibitors Improve Metabolic Diseases: A Mechanism Review. Life Sci. 2022, 300, 120543. [Google Scholar]
- Hayashi, T.; Fukui, T.; Nakanishi, N.; Yamamoto, S.; Tomoyasu, M.; Osamura, A.; Ohara, M.; Yamamoto, T.; Ito, Y.; Hirano, T. Dapagliflozin Decreases Small Dense Low-Density Lipoprotein-Cholesterol and Increases High-Density Lipoprotein 2-Cholesterol in Patients with Type 2 Diabetes: Comparison with Sitagliptin. Cardiovasc. Diabetol. 2017, 16, 8. [Google Scholar] [CrossRef]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui, K.J.; Singh, M.K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801–1808. [Google Scholar] [CrossRef]
- He, K.; Li, J.; Xi, W.; Ge, J.; Sun, J.; Jing, Z. Dapagliflozin for nonalcoholic fatty liver disease: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2022, 185, 109791. [Google Scholar] [CrossRef]
- Xu, Z.; Hu, W.; Wang, B.; Xu, T.; Wang, J.; Wei, D. Canagliflozin Ameliorates Nonalcoholic Fatty Liver Disease by Regulating Lipid Metabolism and Inhibiting Inflammation through Induction of Autophagy. Yonsei Med. J. 2022, 63, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.; Handelsman, Y.; Bakris, G.; Verma, S. Use of sodium–glucose co-transporter-2 inhibitors in patients with and without type 2 diabetes: Implications for incident and prevalent heart failure. Eur. J. Heart Fail. 2020, 22, 604–617. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Garg, A.; Yan, A.T.; Gupta, A.K.; Al-Omran, M.; Sabongui, A.; Teoh, H.; Mazer, C.D.; Connelly, K.A. Effect of Empagliflozin on Left Ventricular Mass and Diastolic Function in Individuals With Diabetes: An Important Clue to the EMPA-REG OUTCOME Trial? Diabetes Care 2016, 39, e212–e213. [Google Scholar] [CrossRef] [PubMed]
- Youm, Y.H.; Nguyen, K.Y.; Grant, R.W.; Goldberg, E.L.; Bodogai, M.; Kim, D.; D’Agostino, D.; Planavsky, N.; Lupfer, C.; Kanneganti, T.-D.; et al. The ketone metabolite β-hydroxybutyrate blocks NLRP3 inflammasome-mediated inflammatory disease. Nat. Med. 2015, 21, 263–269. [Google Scholar] [CrossRef]
- Dai, B.; Wu, Q.; Zeng, C.; Zhang, J.; Cao, L.; Xiao, Z.; Yang, M. The effect of Liuwei Dihuang decoction on PI3K/Akt signaling pathway in liver of type 2 diabetes mellitus (T2DM) rats with insulin resistance. J. Ethnopharmacol. 2016, 192, 382–389. [Google Scholar] [CrossRef]
- Wang, X.-F.; Chen, X.; Tang, Y.; Wu, J.-M.; Qin, D.-L.; Yu, L.; Yu, C.-L.; Zhou, X.-G.; Wu, A.-G. The Therapeutic Potential of Plant Polysaccharides in Metabolic Diseases. Pharmaceuticals 2022, 15, 1329. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Chen, Y.; Tang, Y.; Chen, T.; Zhou, C.; Wang, S.; Chang, R.; Chen, Z.; Yang, W.; et al. From physiology to pathology: Emerging roles of GPER in cardiovascular disease. Pharmacol. Ther. 2025, 267, 108801. [Google Scholar] [CrossRef]
- He, K.; Chen, R.; Xu, S.; Ding, Y.; Wu, Z.; Bao, M.; He, B.; Li, S. Environmental endocrine disruptor-induced mitochondrial dysfunction: A potential mechanism underlying diabetes and its complications. Front. Endocrinol. 2024, 15, 1422752. [Google Scholar] [CrossRef]
- Liang, J.; He, Y.; Huang, C.; Ji, F.; Zhou, X.; Yin, Y. The Regulation of Selenoproteins in Diabetes: A New Way to Treat Diabetes. Curr. Pharm. Des. 2024, 30, 1541–1547. [Google Scholar] [CrossRef]
- Zeng, Q.; Zhang, Y.; Zheng, J.; Lin, J.; Li, N.; Zhao, M.; Chen, X.; Li, X.; Zhao, M.; Huang, J.; et al. Stem cells vesicles-loaded type I pro-photosensitizer for synergetic oxygen-independent phototheranostics and microenvironment regulation in infected diabetic wounds. Chem. Eng. J. 2025, 505, 159239. [Google Scholar] [CrossRef]
- Maan, A.; Heist, E.K.; Passeri, J.; Inglessis, I.; Baker, J.; Ptaszek, L.; Vlahakes, G.; Ruskin, J.N.; Palacios, I.; Sundt, T.; et al. Impact of Atrial Fibrillation on Outcomes in Patients Who Underwent Transcatheter Aortic Valve Replacement. Am. J. Cardiol. 2015, 115, 220–226. [Google Scholar] [CrossRef]
- Çavuşoğlu, Y.; Altay, H.; Çelik, A.; Güvenç, T.S.; Kılıçarslan, B.; Nalbantgil, S.; Temizhan, A.; Yıldırımtürk, Ö.; Yılmaz, M.B. Current Use of Sodium Glucose Co-transporter 2 Inhibitors in Heart Failure Therapy. Turk. Kardiyol. Dern Ars. 2024, 52, 429–454. [Google Scholar] [CrossRef] [PubMed]
- Hallow, K.M.; Helmlinger, G.; Greasley, P.J.; McMurray, J.J.V.; Boulton, D.W. Why do SGLT2 inhibitors reduce heart failure hospitalization? A differential volume regulation hypothesis. Diabetes Obes. Metab. 2018, 20, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Verma, S.; Hassanabad, A.F.; Teng, G.; Belke, D.D.; Dundas, J.A.; Guzzardi, D.G.; Svystonyuk, D.A.; Pattar, S.S.; Park, D.S.; et al. Direct Effects of Empagliflozin on Extracellular Matrix Remodelling in Human Cardiac Myofibroblasts: Novel Translational Clues to Explain EMPA-REG OUTCOME Results. Can. J. Cardiol. 2020, 36, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Shiou, Y.L.; Jhuo, S.J.; Chang, C.-Y.; Liu, P.-L.; Jhuang, W.-J.; Dai, Z.-K.; Chen, W.-Y.; Chen, Y.-F.; Lee, A.-S. The sodium-glucose co-transporter 2 inhibitor empagliflozin attenuates cardiac fibrosis and improves ventricular hemodynamics in hypertensive heart failure rats. Cardiovasc. Diabetol. 2019, 18, 45. [Google Scholar] [CrossRef]
- Brown, A.J.M.; Gandy, S.; McCrimmon, R.; Houston, J.G.; Struthers, A.D.; Lang, C.C. A randomized controlled trial of dapagliflozin on left ventricular hypertrophy in people with type two diabetes: The DAPA-LVH trial. Eur. Heart J. 2020, 41, 3421–3432. [Google Scholar] [CrossRef]
- Verma, S.; Maitland, A.; Weisel, R.D.; Li, S.-H.; Fedak, P.W.; Pomroy, N.C.; Mickle, D.A.; Li, R.-K.; Ko, L.; Rao, V. Hyperglycemia exaggerates ischemia-reperfusion-induced cardiomyocyte injury: Reversal with endothelin antagonism. J. Thorac. Cardiovasc. Surg. 2002, 123, 1120–1124. [Google Scholar] [CrossRef]
- Uthman, L.; Homayr, A.; Juni, R.P.; Spin, E.L.; Kerindongo, R.; Boomsma, M.; Hollmann, M.W.; Preckel, B.; Koolwijk, P.; Van Hinsbergh, V.W.M.; et al. Empagliflozin and Dapagliflozin Reduce ROS Generation and Restore NO Bioavailability in Tumor Necrosis Factor α-Stimulated Human Coronary Arterial Endothelial Cells. Cell. Physiol. Biochem. 2019, 53, 865–886. [Google Scholar]
- Jabczyk, M.; Nowak, J.; Mielcarska, S.; Hudzik, B.; Wołkowska-Pokrywa, K.; Świętochowska, E.; Zubelewicz-Szkodzińska, B. Evaluation of Cardiometabolic Risk in Patients with Non-Functioning Adrenal Adenomas Using the Systematic Coronary Risk Evaluation 2 (SCORE2) and the Systematic Coronary Risk Evaluation 2-Older Persons (SCORE2-OP) Algorithms. Med. Sci. Monit. 2024, 30, e945899. [Google Scholar] [CrossRef]
- Wei, Y.; Xu, S.; Wu, Z.; Zhang, M.; Bao, M.; He, B. Exploring the causal relationships between type 2 diabetes and neurological disorders using a Mendelian randomization strategy. Medicine 2024, 103, e40412. [Google Scholar] [CrossRef]
- Ding, Y.; Cai, X.; Ou, Y.; Liang, D.; Guan, Q.; Zhong, W.; Lin, X. The Burden of Diabetes in the Southeastern Coastal Region of China From 1990 to 2019 and Projections for 2030: A Systematic Analysis of the 2019 Global Burden of Disease Study. Diabetes/Metab. Res. Rev. 2025, 41, e70031. [Google Scholar] [CrossRef]
- Li, C.; Zhang, Z.; Luo, X.; Xiao, Y.; Tu, T.; Liu, C.; Liu, Q.; Wang, C.; Dai, Y.; Zhang, Z.; et al. The triglyceride–glucose index and its obesity-related derivatives as predictors of all-cause and cardiovascular mortality in hypertensive patients: Insights from NHANES data with machine learning analysis. Cardiovasc. Diabetol. 2025, 24, 47. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, S.; Zhang, X.; Xiong, J.; Han, X.; Wu, Z.; Zhao, D.; Li, Y.; Xu, Y.; Chen, D. Fast Virtual Stenting for Thoracic Endovascular Aortic Repair of Aortic Dissection Using Graph Deep Learning. IEEE J. Biomed. Health Inform. 2025, 29, 1–13. [Google Scholar] [CrossRef]

| 0 Months | 3rd Months | 6th Months | P1 | P2 | P3 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (min–max) | Mean ± SD | Median (min–max) | Mean ± SD | Median (min–max) | ||||
| Age, years | 58.47 ± 9.86 | 58(38–79) | |||||||
| Gender, n(%) | |||||||||
| Male | 80 (52.6) | ||||||||
| Female | 72 (47.4) | ||||||||
| Education, n (%) | |||||||||
| Literate | 12 (7.9) | ||||||||
| Primary | 91 (59.9) | ||||||||
| High School | 33 (21.7) | ||||||||
| University | 16 (10.5) | ||||||||
| Smoking, n (%) | 96 (63.2) | ||||||||
| Height, cm | 165.87 ± 9.17 | 165 (149–184) | |||||||
| Weight, kg | 86.57 ± 11.43 | 85.5 (63–114) | 84.88 ± 10.75 | 86 (63–105) | 83.01 ± 9.59 | 83.5 (62–101) | <0.001 | <0.001 | <0.001 |
| BMI, kg/m2 | 31.59 ± 4.45 | 31.25 (23.2–46.75) | 30.99 ± 4.33 | 30.83 (22.84–45.45) | 30.32 ± 4.04 | 29.61 (22.28–42.85) | <0.001 * | <0.001 * | <0.001 * |
| SBP, mmHg | 131.64 ± 8.15 | 130 (110–155) | 126.43 ± 6.93 | 125 (110–145) | 122.43 ± 8.14 | 125 (100–145) | <0.001 * | <0.001 * | <0.001 * |
| DBP, mmHg | 82.04 ± 6.49 | 80 (60–95) | 77.53 ± 6.18 | 80 (60–93) | 75.88 ± 6.82 | 75 (55–91) | <0.001 | 0.003 | <0.001 |
| HbA1c, % | 9.1 ± 1.6 | 9.05 (6.8–12.9) | 8.26 ± 1.25 | 8.2 (5.7–11) | 7.72 ± 1.04 | 7.7 (5.8–11) | <0.001 | <0.001 | <0.001 |
| FBG, mg/dL | 218.78 ± 76.4 | 199.5 (96–441) | 180.22 ± 49.03 | 171 (111–343) | 162.39 ± 35.27 | 154.5 (99–302) | <0.001 | <0.001 | <0.001 |
| Urea, mg/dL | 33.81 ± 7.79 | 33 (16–64) | 34.15 ± 7.14 | 34 (15–55) | 34.17 ± 8.02 | 33 (16–56) | 0.475 | 0.746 | 0.625 |
| Creatinine, mg/dL | 0.89 ± 0.14 | 0.9 (0.57–1.24) | 0.96 ± 0.17 | 0.93 (0.6–1.4) | 0.95 ± 0.22 | 0.98 (0.55–1.8) | <0.001 | 0.395 | <0.001 |
| AST, IU/L | 35.01 ± 9.87 | 35 (11–59) | 33.52 ± 7.88 | 34 (15–51) | 32.21 ± 6.63 | 33 (16–45) | <0.001 | <0.001 | <0.001 |
| ALT, IU/L | 33.55 ± 7.02 | 34 (14–45) | 34.34 ± 6.1 | 35 (15–44) | 34.62 ± 5.8 | 35 (15–45) | 0.014 | 0.308 | 0.001 |
| Triglycerides, mg/dL | 173.84 ± 57.6 | 165.5 (82–367) | 159.23 ± 47.81 | 154 (78–340) | 150.93 ± 37.13 | 144 (84–301) | <0.001 | <0.001 | <0.001 |
| HDL, mg/dL | 43.93 ± 8.58 | 42 (28–73) | 44.42 ± 8.02 | 42 (33–70) | 44.46 ± 7.49 | 42 (33–68) | 0.052 | 0.707 | 0.298 |
| LDL, mg/dL | 126.07 ± 29.07 | 131 (49–191) | 116.23 ± 23.04 | 116 (61–168) | 111.8 ± 21.43 | 110 (70–159) | <0.001 * | <0.001 * | <0.001 * |
| SCORE-2 DM | 21.68 ± 9.83 | 20.95 (2.8–49.7) | 17.43 ± 8.72 | 16.35 (2.7–40.5) | <0.001 | ||||
| 6th Month | |||
|---|---|---|---|
| Low Risk | Moderate Risk | High Risk | Very High Risk |
| 5 | 0 | 0 | 0 |
| 3 | 11 | 0 | 0 |
| 0 | 17 | 36 | 0 |
| 0 | 0 | 28 | 52 |
| Adj p | |
|---|---|
| Low Risk–Moderate Risk | 0.75 |
| Low Risk–High Risk | 1 |
| Low Risk–Very High Risk | 1 |
| Moderate Risk–High Risk | <0.001 |
| Moderate Risk–Very High Risk | 1 |
| High Risk–Very High Risk | <0.001 |
| 6th Month | p | ||
|---|---|---|---|
| 0th month | High Risk | Very High Risk | <0.001 |
| High Risk | 36 | 0 | |
| Very High Risk | 28 | 52 | |
| Moderate Risk | High Risk | <0.001 | |
| Moderate Risk | 11 | 0 | |
| High Risk | 17 | 36 | |
| Parameters | β | SE | 95% Confidence Interval | Wald (χ2) | p |
|---|---|---|---|---|---|
| Threshold | |||||
| Score2-DM (1 = High Risk) | −0.777 | 0.219 | (−1.206: −0.347) | 12.555 | <0.001 |
| Score2-DM (2 = Low Risk) | −0.597 | 0.220 | (−1.029: −0.165) | 7.337 | 0.007 |
| Score2-DM (3 = Moderate Risk) | −0.026 | 0.232 | (−0.482: −0.429) | 0.013 | 0.910 |
| Main effects | |||||
| Measurement (Before) | −0.724 | 0.222 | (−1.159: −0.288) | 10.624 | 0.001 |
| Measurement (After) | |||||
| Drug (0 = Empagliflozin) | −0.031 | 0.317 | (−0.652: 0.590) | 0.010 | 0.922 |
| Drug (1 = Dapagliflozin) | |||||
| Interaction | |||||
| Measurement (Before) × Drug (0 = Empagliflozin) | 0.374 | 0.309 | (−0.232: 0.980) | 1.462 | 0.227 |
| Measurement (Before) × Drug (1 = Dapagliflozin) | 0 | - | - | - | - |
| Measurement (After) × Drug (0 = Empagliflozin) | 0 | - | - | - | - |
| Measurement (After) × Drug (1 = Dapagliflozin) | 0 | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yalçın, N.; Aktaş, S.; Uyar, S.; Koca, N. Impact of SGLT2 Inhibitors on Cardiovascular Risk Scores, Metabolic Parameters, and Laboratory Profiles in Type 2 Diabetes. Life 2025, 15, 722. https://doi.org/10.3390/life15050722
Yalçın N, Aktaş S, Uyar S, Koca N. Impact of SGLT2 Inhibitors on Cardiovascular Risk Scores, Metabolic Parameters, and Laboratory Profiles in Type 2 Diabetes. Life. 2025; 15(5):722. https://doi.org/10.3390/life15050722
Chicago/Turabian StyleYalçın, Nazif, Selman Aktaş, Seyit Uyar, and Nizameddin Koca. 2025. "Impact of SGLT2 Inhibitors on Cardiovascular Risk Scores, Metabolic Parameters, and Laboratory Profiles in Type 2 Diabetes" Life 15, no. 5: 722. https://doi.org/10.3390/life15050722
APA StyleYalçın, N., Aktaş, S., Uyar, S., & Koca, N. (2025). Impact of SGLT2 Inhibitors on Cardiovascular Risk Scores, Metabolic Parameters, and Laboratory Profiles in Type 2 Diabetes. Life, 15(5), 722. https://doi.org/10.3390/life15050722