
Cardio-Respiratory, Functional and Antalgic Effects of the Integrated Thermal Care Protocol After Breast Cancer Surgery

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Sample
2.3. Assessment Methods
- -
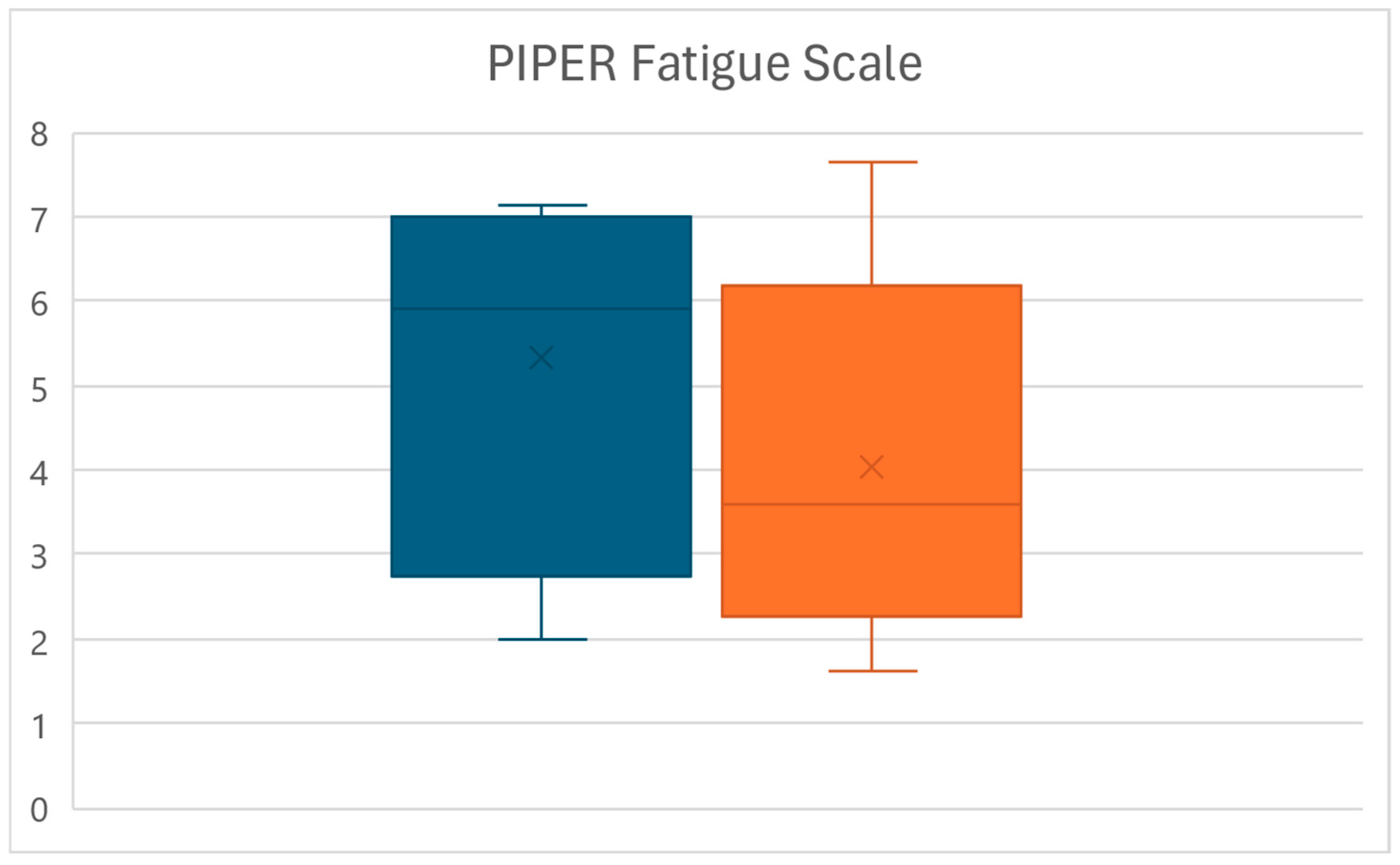
- Piper Fatigue Scale (PIPER): The revised version of the PFS consists of 22 items and four subscales: behavioral/severity (6 items), affective meaning (5 items), sensory (5 items) and cognitive/mood (6 items). These items are rated using a 0–10 numeric scale. The 22 items are used to calculate the fatigue score. Five additional items are not used to calculate subscale or total fatigue scores but are recommended to be kept on the scale as these items furnish rich, qualitative data [39] (Figures S2–S4). This scale is also useful for assessing fatigue in oncology [40].
- -
- -
- Five Times Sit-to-Stand (5STS): This test consists of measuring the time (expressed in seconds) taken by the patient to sit down and stand up 5 consecutive times from a chair or raised surface; the test allows to evaluate lower extremity strength, dynamic balance, fall risks, gait speed and eventually fatigability [42].
- -
- Numeric Pain Rating Scale (NPRS): It is one of the most widespread tools in clinical practice for assessing the pain subjectively perceived by patients. It is a derivate of the Visual Analogue Scale (VAS) divided into ten levels, usually distributed equidistant on a 10 cm long strip, which correspond to the level of pain perceived by the patient at the time of the evaluation. A value of 0 represents the total absence of pain, a value between 1 and 3 corresponds to mild pain, a value between 4 and 6 corresponds to moderate pain and a value between 7 and 10 corresponds to severe pain, where a score of 10 represents the maximum level of pain imaginable and/or ever experienced by the patient [43] (Figure S1).
- -
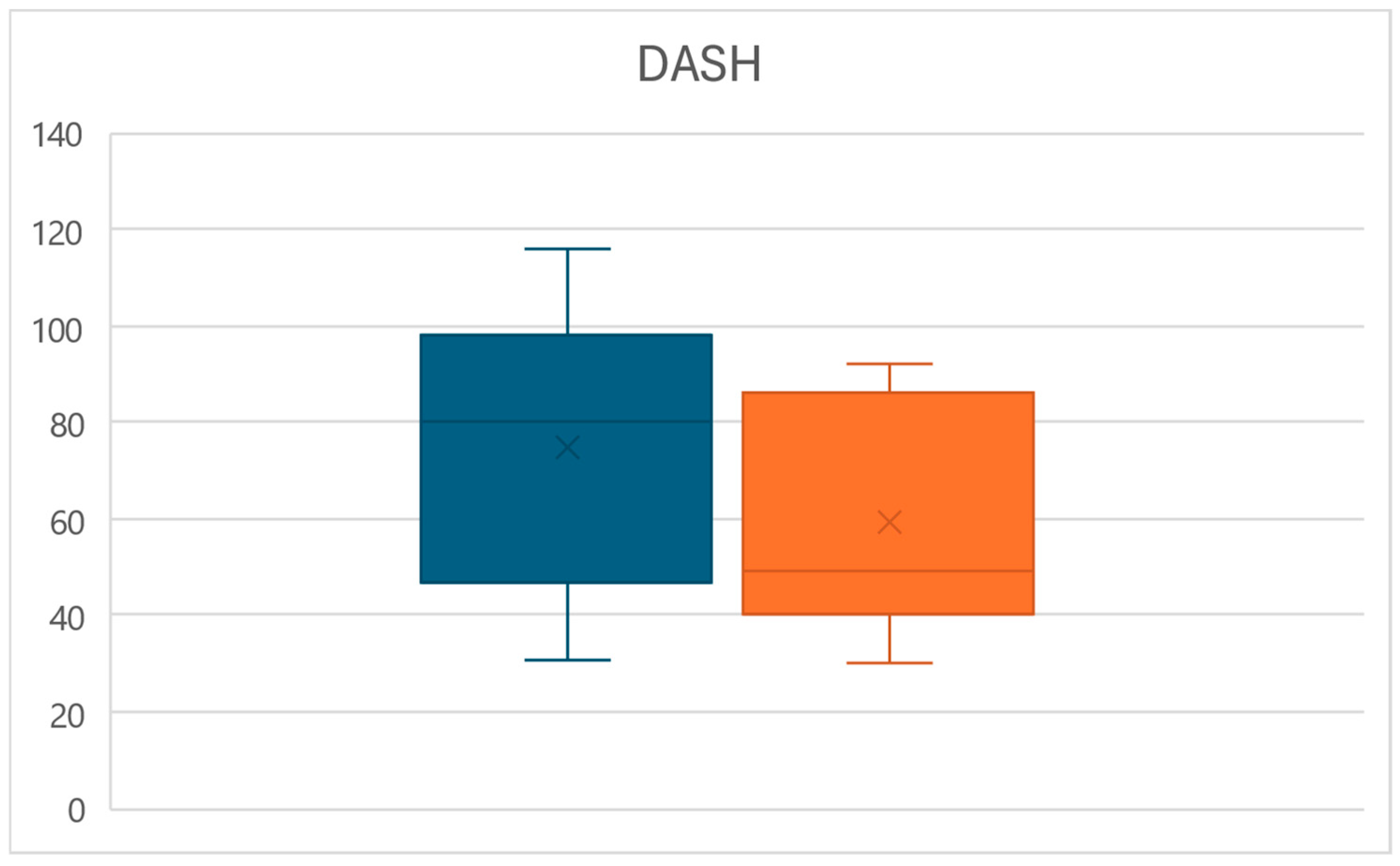
- Disability of the Arm–Shoulder–Hand Scale (DASH): This is a self-administered questionnaire of over 30 questions designed to measure function and symptoms in patients with any musculoskeletal disorder specific to the upper limb. Questions address the ability to perform certain actions in the past week and symptoms that have occurred while performing these actions [44] (Figures S5 and S6). It is also highly reliable in assessing upper limb function in patients with mastectomy/quadrantectomy and breast cancer [44].
- -
- Range of Arm Motion (ROM): The goniometric measurement (expressed in degrees) of the joint range of motion in the various planes of motion. In this case, the shoulder joint subjected to surgery was taken as a reference, considering flexion, extension, adduction, abduction, internal rotation and external rotation [45].
2.4. Treatment Methods
- -
- Hydroponic Treatments: These correspond to the crenotherapy treatment. Initially, the bicarbonate–sulfate–alkaline–earthy mineral water mineral water from the “Castelnuovo della Daunia Thermal Medicine Center” was given to patients in the study facility, at the beginning of each treatment session, by drinking a total of 500 cc as desired on an empty stomach for at least 6 h before each treatment session. After receiving the water to drink, patients underwent steam inhalations treatment with direct warm humid jets placed in front of their face. The bicarbonate–sulfate–alkaline–earthy mineral water jets come out from a nozzle in the form of a homogeneous mist (pressure of 1.5 atmospheres—temperature of 37–38 °C), lasting about 20 min.
- -
- Somatic stimulation: At the same time as the inhalations treatment, a contemporary manual somatic stimulation was performed by a physiotherapist on C1–C5 afferent areas of the neck of the patient for the whole 20 min of inhalation. This method consists of the digital pressure stimulation of the key MTrPs identified in the neck area of the patient, according to the Bio-Physico-Metric approach of hierarchical deactivation of the key and satellite MTrPs [46]. This method is based on palpation of the affected area in search of nodules in the muscle tissue, which are typically the site of MTrPs that can cause pain, functional limitation and possible irradiation symptoms that can also influence areas distant from the site of the MTrPs. Once the MTrPs of the anatomical area investigated have been identified, they are mechanically stimulated through pressure and massage techniques aimed at their resolution with cascading effects that have repercussions not only locally but also in the distant anatomical areas which are functionally influenced by the MTrPs defined as “key” [46]. In this way, it is possible to work on the tensions, pains and limitations of the cervical and shoulder areas as well as indirectly on further functions such as respiratory mechanics.
- -
- Hydrokinesitherapy: Treatment in water environment, according to the Safe Bearing Back [47], was conducted with 40 min treatment sessions carried out in the bicarbonate–sulfate–alkaline–earthy mineral water pools of the study facility. For the first 20 min of the session, patients were treated by the physiotherapist through mobilization maneuvers and the deactivation of KMTrPs in the shoulder and trunk area while floating on the water surface supported by the same physiotherapist. The remaining 20 min of the treatment was dedicated to the execution of guided active exercises in water, in particular for the spine and upper limbs, including the use of ankle weights and hand-held plates useful for exploiting the hydraulic resistance offered by the water. The exercises were personalized and adapted according to the necessities and abilities of each patients, mainly using exercises of flexion, abduction, extension and internal and external rotations of the arms with the patient immersed in water up to the level of the neck as well as flexion and extension exercises of the lower limbs on the pelvis with the torso immersed in water.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Routh, H.B.; Bhowmik, K.R.; Parish, L.C.; Witkowski, J.A. Balneology, mineral water, and spas in historical perspective. Clin. Dermatol. 1996, 14, 551–554. [Google Scholar] [CrossRef]
- Gianfaldoni, S.; Tchernev, G.; Wollina, U.; Roccia, M.G.; Fioranelli, M.; Gianfaldoni, R.; Lotti, T. History of the baths and thermal medicine. Open Access Maced. J. Med. Sci. 2017, 5, 566. [Google Scholar] [CrossRef]
- Bellometti, S. SPAs Thermal Treatments in Italy. Presse Therm. Clim. 2009, 146, 275–276. [Google Scholar]
- Gómez Pérez, C.P.; González Soutelo, S.; Mourelle Mosqueira, M.L.; Legido Soto, J.L. Spa techniques and technologies: From the past to the present. Sustain. Water Resour. Manag. 2019, 5, 71–81. [Google Scholar] [CrossRef]
- Bernetti, A.; Mangone, M.; Alviti, F.; Paolucci, T.; Attanasi, C.; Murgia, M.; Di Sante, L.; Agostini, F.; Vitale, M.; Paoloni, M. Spa therapy and rehabilitation of musculoskeletal pathologies: A proposal for best practice in Italy. Int. J. Biometeorol. 2020, 64, 905–914. [Google Scholar] [CrossRef]
- Maccarone, M.C.; Magro, G.; Solimene, U.; Masiero, S. Spa-therapy can improve quality of life in chronic musculoskeletal disorder subjects: A narrative review. Bull. Rehabil. Med. 2020, 2, 3–6. [Google Scholar] [CrossRef]
- Simões, J.F.; Castro, H.; Martins, M.J.; Miguéis, A. Thermal Waters in Otorhinolaryngology. In Mineral Water: From Basic Research to Clinical Applications; João Martins, M., Ed.; Nova Science Publishers Inc.: New York, NY, USA, 2022; Chapter 3; pp. 73–114. [Google Scholar]
- Passali, D.; De Corso, E.; Platzgummer, S.; Streitberger, C.; Lo Cunsolo, S.; Nappi, G.; Passali, G.C.; Bellussi, L. Spa therapy of upper respiratory tract inflammations. Eur. Arch. Otorhinolaryngol. 2013, 270, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Barassi, G.; Panunzio, M.; Di Iulio, A.; Di Iorio, A.; Pellegrino, R.; Colombo, A.; Di Stefano, G.; Galasso, P.; Spina, S.; Vincenzi, U.; et al. Integrated Thermal Rehabilitation Care: An Intervention Study. Healthcare 2023, 11, 2384. [Google Scholar] [CrossRef] [PubMed]
- Barassi, G.; Prosperi, L.; Pellegrino, R.; Di Iorio, A.; Guglielmi, V.; Younes, A.; Marinucci, C.; Della Rovere, M.P.; Panunzio, M. Integrated Thermal Care and Bio-Physico-Metric Approach for The Treatment of Long-Covid Patients. Eur. J. Musculoskelet. Dis. 2024, 13, 1–10. [Google Scholar]
- Jazani, A.M.; Azgomi, H.N.D.; Azgomi, A.N.D.; Azgomi, R.N.D. Effect of hydrotherapy, balneotherapy, and spa therapy on blood pressure: A mini-review. Int. J. Biometeorol. 2023, 67, 1387–1396. [Google Scholar] [CrossRef]
- Karampitsakos, T.; Dimakou, K.; Bouros, D. Role of aquatic therapy and speleotherapy as complementary therapies in the respiratory system. Pneumon 2016, 29, 269–273. [Google Scholar]
- Zajac, D. Inhalations with thermal waters in respiratory diseases. J. Ethnopharmacol. 2021, 281, 114505. [Google Scholar] [CrossRef] [PubMed]
- Kesiktas, N.; Karagülle, Z.; Erdogan, N.; Yazıcıoglu, K.; Yılmaz, H.; Paker, N. The efficacy of balneotherapy and physical modalities on the pulmonary system of patients with fibromyalgia. J. Back Musculoskelet. Rehabil. 2011, 24, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Aydemir, K.; Tok, F.; Peker, F.; Safaz, I.; Taskaynatan, M.A.; Ozgul, A. The effects of balneotherapy on disease activity, functional status, pulmonary function and quality of life in patients with ankylosing spondylitis. Acta Reumatol. Port. 2010, 35, 441–446. [Google Scholar] [PubMed]
- Rapolienė, L.; Razbadauskas, A.; Sąlyga, J.; Martinkėnas, A. Stress and Fatigue Management Using Balneotherapy in a Short-Time Randomized Controlled Trial. Evid.-Based Complement. Altern. Med. 2016, 2016, 9631684. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.F.; Xia, F. Long-term fatigue state in postoperative patients with breast cancer. Chin. J. Cancer Res. 2014, 26, 12. [Google Scholar] [PubMed]
- Berger, A.M.; Gerber, L.H.; Mayer, D.K. Cancer-related fatigue: Implications for breast cancer survivors. Cancer 2012, 118, 2261–2269. [Google Scholar] [CrossRef]
- Gomide, L.B.; Matheus, J.P.C.; Candido dos Reis, F.J. Morbidity after breast cancer treatment and physiotherapeutic performance. Int. J. Clin. Pract. 2007, 61, 972–982. [Google Scholar] [CrossRef]
- Farooqi, Y.N. Depression and anxiety in mastectomy cases. Illn. Cris. Loss 2005, 13, 267–278. [Google Scholar] [CrossRef]
- Roy, N.; Downes, M.H.; Ibelli, T.; Amakiri, U.O.; Li, T.; Tebha, S.S.; Balija, T.M.; Schnur, J.B.; Montgomery, G.H.; Henderson, P.W. The psychological impacts of post-mastectomy breast reconstruction: A systematic review. Ann. Breast Surg. Open Access J. Bridge Breast Surg. Across World 2023, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Kang, D.X.; Zhang, A.J.; Li, B.R. Effects of psychological intervention on negative emotions and psychological resilience in breast cancer patients after radical mastectomy. World J. Psychiatr. 2024, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Lamkin, D.M. Inflammation and cancer-related fatigue: Mechanisms, contributing factors, and treatment implications. Brain Behav. Immun. 2013, 30, S48–S57. [Google Scholar] [CrossRef]
- Passariello, A.; Di Costanzo, M.; Terrin, G.; Iannotti, A.; Buono, P.; Balestrieri, U.; Ascione, E.; Pedata, M.; Canani, F.B.; Canani, R.B. Crenotherapy modulates the expression of proinflammatory cytokines and immunoregulatory peptides in nasal secretions of children with chronic rhinosinusitis. Am. J. Rhinol. Allergy 2012, 26, e15–e19. [Google Scholar] [CrossRef] [PubMed]
- Błońska-Sikora, E.; Orlewska, E.; Klusek, J. The Influence of Crenotheraphy with SHS Water on the Concentration of Glutathione in Blood of People with Rheumatoid Arthritis. Preprints 2018. [Google Scholar] [CrossRef]
- Wrzochal, A.; Kalska, A.; Knefel, M.; Tworek, D. Crenotherapy with therapeutic sulfide water as a new direction of health resort treatment on the example of the Sulfide Reduction Diet. Acta Balneol. 2024, 181, 158–163. [Google Scholar] [CrossRef]
- Schmidt, O.P. Crenotherapy in inflammatory diseases of the upper air passages. Minerva Medica 1965, 56, 2996–2998. [Google Scholar] [PubMed]
- Costantino, M.; Conti, V.; Corbi, G.; Giudice, V.; Caro, F.D.; Filippelli, A. Marked Reduction of Oxidant Species after Sulfureous Crenotherapy in Females with Joint Diseases and Psoriasis: A Retrospective Real-Life Study. J. Clin. Med. 2023, 12, 5731. [Google Scholar] [CrossRef]
- Fernández-Lao, C.; Cantarero-Villanueva, I.; Fernández-de-Las-Peñas, C.; Del-Moral-Ávila, R.; Menjón-Beltrán, S.; Arroyo-Morales, M. Development of active myofascial trigger points in neck and shoulder musculature is similar after lumpectomy or mastectomy surgery for breast cancer. J. Bodyw. Mov. Ther. 2012, 16, 183–190. [Google Scholar] [CrossRef]
- Khoury, A.L.; Keane, H.; Varghese, F.; Hosseini, A.; Mukhtar, R.; Eder, S.E.; Weinstein, P.R.; Esserman, L.J. Trigger point injection for post-mastectomy pain: A simple intervention with high rate of long-term relief. NPJ Breast Cancer 2021, 7, 123. [Google Scholar] [CrossRef]
- Cantarero-Villanueva, I.; Fernández-Lao, C.; Cuesta-Vargas, A.I.; Del Moral-Avila, R.; Fernández-de-Las-Peñas, C.; Arroyo-Morales, M. The effectiveness of a deep water aquatic exercise program in cancer-related fatigue in breast cancer survivors: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2013, 94, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Baltag, O.M.; Singuran, A.I.; Apostu, M.; El-Bsat, R. The Contribution of Hydrotherapy and Swimming to Post-Mastectomy Functional Rehabilitation. Phys. Educ. Sports Kinetotherapy J. 2023, 62, 70–84. [Google Scholar]
- Naumann, J.; Sadaghiani, C. Therapeutic benefit of balneotherapy and hydrotherapy in the management of fibromyalgia syndrome: A qualitative systematic review and meta-analysis of randomized controlled trials. Arthritis Res. Ther. 2014, 16, R141. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Zarkadoulia, E.; Rafailidis, P.I. The therapeutic effect of balneotherapy: Evaluation of the evidence from randomised controlled trials. Int. J. Clin. Pract. 2009, 63, 1068–1084. [Google Scholar] [CrossRef] [PubMed]
- Reger, M.; Kutschan, S.; Freuding, M.; Schmidt, T.; Josfeld, L.; Huebner, J. Water therapies (hydrotherapy, balneotherapy or aqua therapy) for patients with cancer: A systematic review. J. Cancer Res. Clin. Oncol. 2022, 148, 1277–1297. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Winter, E.M.; Maughan, R.J. Requirements for ethics approvals. J. Sports Sci. 2009, 27, 985. [Google Scholar] [CrossRef] [PubMed]
- De Sanctis, V.; Soliman, A.T.; Daar, S.; Tzoulis, P.; Fiscina, B.; Kattamis, C. Retrospective observational studies: Lights and shadows for medical writers. Acta Bio-Medica Atenei Parm. 2022, 93, e2022319. [Google Scholar]
- Piper, B.F.; Dibble, S.L.; Dodd, M.J.; Weiss, M.C.; Slaughter, R.E.; Paul, S.M. The revised Piper Fatigue Scale: Psychometric evaluation in women with breast cancer. Oncol. Nurs. Forum 1998, 25, 677–684. [Google Scholar]
- Rehwaldt, M.A. Validity of the Revised Piper Fatigue Scale for Detecting Fatigue in Women with Breast Cancer Undergoing Treatment. D.N.Sc. Dissertation, Rush University, College of Nursing, Chicago, IL, USA, 1998. [Google Scholar]
- Galiano-Castillo, N.; Arroyo-Morales, M.; Ariza-Garcia, A.; Sánchez-Salado, C.; Fernández-Lao, C.; Cantarero-Villanueva, I.; Martín-Martín, L. The six-minute walk test as a measure of health in breast cancer patients. J. Aging Phys. Act. 2016, 24, 508–515. [Google Scholar] [CrossRef]
- van Cappellen-van Maldegem, S.J.; Hoedjes, M.; Seidell, J.C.; van de Poll-Franse, L.V.; Buffart, L.M.; Mols, F.; Beijer, S. Self-performed Five Times Sit-To-Stand test at home as (pre-) screening tool for frailty in cancer survivors: Reliability and agreement assessment. J. Clin. Nurs. 2023, 32, 1370–1380. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, S.W.; Kolber, M.J.; Mokha, M.; Hanney, W.J. Concurrent validity of pain scales in individuals with myofascial pain and fibromyalgia. J. Bodyw. Mov. Ther. 2018, 22, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.; Brockopp, D.; Moe, K. Internal consistency of the disability of arm, shoulder and hand (DASH) outcome measure in assessing functional status among breast cancer survivors. Rehabil. Oncol. 2013, 31, 6–12. [Google Scholar] [CrossRef]
- Harrington, S.; Padua, D.; Battaglini, C.; Michener, L.A. Upper extremity strength and range of motion and their relationship to function in breast cancer survivors. Physiother. Theory Pract. 2013, 29, 513–520. [Google Scholar] [CrossRef]
- Barassi, G.; Pokorski, M.; Di Matteo, C.; Supplizi, M.; Prosperi, L.; Guglielmi, V.; Younes, A.; Della Rovere, F.; Di Iorio, A. Manual Pressure Release and Low-Grade Electrical Peripheral Receptor Stimulation in Nonspecific Low Back Pain: A Randomized Controlled Trial. Adv. Exp. Med. Biol. 2021, 1324, 73–81. [Google Scholar]
- Barassi, G.; Bellomo, R.G.; Porreca, A.; Giannuzzo, G.; Irace, G.; Trivisano, L.; Saggini, R. Rehabilitation of neuromotor disabilities in aquatic microgravity environment. In Respiratory Ailments in Context; Pokorski, M., Ed.; Springer Nature: Cham, Switzerland, 2019; Volume 1113, pp. 61–73. [Google Scholar]
- Burguin, A.; Diorio, C.; Durocher, F. Breast cancer treatments: Updates and new challenges. J. Pers. Med. 2021, 11, 808. [Google Scholar] [CrossRef]
- Barrios, C.H. Global challenges in breast cancer detection and treatment. Breast 2022, 62, S3–S6. [Google Scholar] [CrossRef]
- Keene, M.R.; Heslop, I.M.; Sabesan, S.S.; Glass, B.D. Complementary and alternative medicine use in cancer: A systematic review. Complement. Ther. Clin. Pract. 2019, 35, 33–47. [Google Scholar] [CrossRef]
- Agishi, Y. Clinical usefulness of long-term thermohydrotherapy (balneotherapy). In Thermotherapy for Neoplasia, Inflammation, and Pain; Kosaka, M., Sugahara, T., Schmidt, K.L., Simon, E., Eds.; Springer Nature: Tokyo, Japan, 2001; Chapter 33; pp. 486–494. [Google Scholar]
- Khudoev, E.S.; Khodasevich, L.S.; Naslednikova, I.O.; Khodasevich, A.L. Balneotherapy in Post-Surgical Recovery for Patients with Breast Neoplasms at the Resort (Literature Review). Mod. Issues Biomed. 2021, 5. [Google Scholar] [CrossRef]
- Morer, C.; Roques, C.F.; Françon, A.; Forestier, R.; Maraver, F. The role of mineral elements and other chemical compounds used in balneology: Data from double-blind randomized clinical trials. Int. J. Biometeorol. 2017, 61, 2159–2173. [Google Scholar] [CrossRef] [PubMed]
- Rapolienė, L.; Razbadauskas, A.; Mockevičienė, D.; Varžaitytė, L.; Skarbalienė, A. Balneotherapy for musculoskeletal pain: Does the mineral content matter? Int. J. Biometeorol. 2020, 64, 965–979. [Google Scholar] [CrossRef] [PubMed]
- Cristalli, G.; Abramo, A.; Pollastrini, L. Treatment of chronic inflammation of the upper respiratory airways by inhalation thermal therapy with sulfur-sulfate-bicarbonate-carbonate-alkaline earth mineral water: A study of nasal cytology. Acta Otorhinolaryngol. Ital. 1996, 16 (Suppl. 55), 91–94. [Google Scholar]
- Albertini, M.C.; Teodori, L.; Accorsi, A.; Soukri, A.; Campanella, L.; Baldoni, F.; Dachà, M. Sulphurous mineral water oral therapy: Effects on erythrocyte metabolism. Food Chem. Toxicol. 2008, 46, 3343–3350. [Google Scholar] [CrossRef] [PubMed]
- Louati, K.; Berenbaum, F. Fatigue in chronic inflammation—A link to pain pathways. Arthritis Res. Ther. 2015, 17, 254. [Google Scholar] [CrossRef]
- Collado-Hidalgo, A.; Bower, J.E.; Ganz, P.A.; Cole, S.W.; Irwin, M.R. Inflammatory biomarkers for persistent fatigue in breast cancer survivors. Clin. Cancer Res. 2006, 12, 2759–2766. [Google Scholar] [CrossRef]
- Bender, C.M.; Sereika, S.M.; Gentry, A.L.; Duquette, J.E.; Casillo, F.E.; Marsland, A.; Brufsky, A.M.; Evans, S.; Gorantla, V.C.; Grahovac, T.L.; et al. Physical activity, cardiorespiratory fitness, and cognitive function in postmenopausal women with breast cancer. Support. Care Cancer 2021, 29, 3743–3752. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Danoff, J.V.; Desai, M.J.; Parikh, S.; Nakamura, L.Y.; Phillips, T.M.; Gerber, L.H. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Arch. Phys. Med. Rehabil. 2008, 89, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Lao, C.; Cantarero-Villanueva, I.; Fernández-de-Las-Peñas, C.; Del-Moral-Avila, R.; Arendt-Nielsen, L.; Arroyo-Morales, M. Myofascial trigger points in neck and shoulder muscles and widespread pressure pain hypersensitivtiy in patients with postmastectomy pain: Evidence of peripheral and central sensitization. Clin. J. Pain 2010, 26, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Fereydounnia, S.; Shadmehr, A.; Tahmasbi, A. Efficacy of myofascial release therapy on the cardiorespiratory functions in patients with COVID-19. J. Mod. Rehabil. 2022, 16, 77–84. [Google Scholar] [CrossRef]
- Ge, H.Y.; Arendt-Nielsen, L.; Madeleine, P. Accelerated muscle fatigability of latent myofascial trigger points in humans. Pain Med. 2012, 13, 957–964. [Google Scholar] [CrossRef]
- Bradley, H.; Esformes, J.D. Breathing pattern disorders and functional movement. Int. J. Sports Phys. Ther. 2014, 9, 28. [Google Scholar]
- Hansen-Honeycutt, J.; Chapman, E.B.; Nasypany, A.; Baker, R.T.; May, J. A clinical guide to the assessment and treatment of breathing pattern disorders in the physically active: Part 2, a case series. Int. J. Sports Phys. Ther. 2016, 11, 971. [Google Scholar]
- Nijs, J.; Adriaens, J.; Schuermans, D.; Buyl, R.; Vincken, W. Breathing retraining in patients with chronic fatigue syndrome: A pilot study. Physiother. Theory Pract. 2008, 24, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Zhang, W.; Tian, T.; Liu, Y.; Bai, H.; Hu, Q.; Qi, F. Latent myofascial trigger points injection therapy for adult cough variant asthma: A randomized controlled trial. Front. Med. 2023, 10, 937377. [Google Scholar] [CrossRef] [PubMed]
- Domaszewska, K.; Pieńkowski, T.; Janiak, A.; Bukowska, D.; Laurentowska, M. The influence of soft tissue therapy on respiratory efficiency and chest mobility of women suffering from breast cancer. Int. J. Environ. Res. Public Health 2019, 16, 5092. [Google Scholar] [CrossRef] [PubMed]
- Lunardi, A.C.; Marques da Silva, C.C.B.; Rodrigues Mendes, F.A.; Marques, A.P.; Stelmach, R.; Fernandes Carvalho, C.R. Musculoskeletal dysfunction and pain in adults with asthma. J. Asthma 2011, 48, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Morais, N.; Cruz, J.; Marques, A. Posture and mobility of the upper body quadrant and pulmonary function in COPD: An exploratory study. Braz. J. Phys. Ther. 2016, 20, 345–354. [Google Scholar] [CrossRef]
- Namdari, S.; Yagnik, G.; Ebaugh, D.D.; Nagda, S.; Ramsey, M.L.; Williams, G.R., Jr.; Mehta, S. Defining functional shoulder range of motion for activities of daily living. J. Shoulder Elb. Surg. 2012, 21, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Eidenberger, M. Physiotherapeutic Management in Breast Cancer Patients. In Breast Cancer Updates; Sözen, S., Emir, S., Eds.; IntechOpen: London, UK, 2022. [Google Scholar]
- Hack, T.F.; Kwan, W.B.; Thomas-MacLean, R.L.; Towers, A.; Miedema, B.; Tilley, A.; Chateau, D. Predictors of arm morbidity following breast cancer surgery. Psycho-Oncology 2010, 19, 1205–1212. [Google Scholar] [CrossRef]
- Money, M.E.; Matthews, C.M.; Tan-Shalaby, J. Review of under-recognized adjunctive therapies for cancer. Cancers 2022, 14, 4780. [Google Scholar] [CrossRef]
- Stubblefield, M.D. The underutilization of rehabilitation to treat physical impairments in breast cancer survivors. PMR 2017, 9, S317–S323. [Google Scholar] [CrossRef] [PubMed]
- Carlucci, F.; Cirà, A.; Forte, E.; Siviero, L. Infrastructure and logistics divide: Regional comparisons between North Eastern & Southern Italy. Technol. Econ. Dev. Econ. 2017, 23, 243–269. [Google Scholar]
- Dilekçi, E.; Özkuk, K.; Kaki, B. The short-term effects of balneotherapy on pain, disability and fatigue in patients with chronic low back pain treated with physical therapy: A randomized controlled trial. Complement. Ther. Med. 2020, 54, 102550. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.P.; Bierma-Zeinstra, S.M.A.; Boers, M.; Cardoso, J.R.; Lambeck, J.; de Bie, R.; de Vet, H.C.W. Balneotherapy for osteoarthritis. Cochrane Database Syst. Rev. 2007, 4, CD006864. [Google Scholar] [CrossRef] [PubMed]
- Aleksić-Milenković, I.; Stojanović, S.; Stamenković, B.; Jevtović-Stoimenov, T.; Šarić, S.; Danković, G. The impact of balneotherapy on IL-6 cytokine levels, disease activity, functional ability, fatigue and depression in patients with rheumatoid arthritis. Srpski Arhiv za Celokupno Lekarstvo 2025, 6. [Google Scholar] [CrossRef]
- Barassi, G.; Spina, S.; D’Alessandro, F.; Prosperi, L.; Lombardi, M.; Panunzio, M.; Santamato, A. Cardio-Respiratory, Functional and Antalgic Effects of the Integrated Thermal Care Protocol after Breast Cancer Surgery. In Proceedings of the 18th Conference “Advances in Pneumology”, Martin, Slovakia, 5–7 December 2024. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Categories | Frequencies |
|---|---|---|
| Total Patients | Women | 11 |
| Age (years) | 31–45 | 1 |
| 46–60 | 8 | |
| 61+ | 2 | |
| Body Mass Index | Normal (≥18.5 and <25) | 4 |
| Overweight (≥25 and <30) | 5 | |
| Obese: Class I (≥30 and < 35) | 1 | |
| Obese: Class II (≥35 and < 40) | 0 | |
| Obese: Class III (≥40) | 1 | |
| Cancer Side | Right | 5 |
| Left | 6 | |
| Cancer Type | Ductal in Situ | 3 |
| Ductal Infiltrative | 8 | |
| Surgery Type | Mastectomy | 4 |
| Quadrantectomy | 7 | |
| Radiotherapy | Yes | 8 |
| No | 3 | |
| Chemotherapy | Yes | 6 |
| No | 5 |
| Variable | T0 | T1 | p-Value | Δ% |
|---|---|---|---|---|
| Flexion | 166.4 ± 25° | 170.9 ± 21.2° | n.s. | +2.7% |
| Extension | 38.2 ± 5.1° | 39.1 ± 4.4° | n.s. | +2.4% |
| Adduction | 34.5 ± 6.5° | 36.4 ± 4.5° | n.s. | +5.3% |
| Abduction | 165.5 ± 25° | 170.9 ± 20.7° | n.s. | +3.3% |
| Internal Rotation | 88.2 ± 4° | 89.1 ± 3° | n.s. | +1% |
| External Rotation | 69.1 ± 8.3° | 73.6 ± 6.7° | <0.02 | +6.6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barassi, G.; Spina, S.; D’Alessandro, F.; Prosperi, L.; Marinucci, C.; Lombardi, M.; Panunzio, M.; Santamato, A. Cardio-Respiratory, Functional and Antalgic Effects of the Integrated Thermal Care Protocol After Breast Cancer Surgery. Life 2025, 15, 374. https://doi.org/10.3390/life15030374
Barassi G, Spina S, D’Alessandro F, Prosperi L, Marinucci C, Lombardi M, Panunzio M, Santamato A. Cardio-Respiratory, Functional and Antalgic Effects of the Integrated Thermal Care Protocol After Breast Cancer Surgery. Life. 2025; 15(3):374. https://doi.org/10.3390/life15030374
Chicago/Turabian StyleBarassi, Giovanni, Stefania Spina, Francesco D’Alessandro, Loris Prosperi, Celeste Marinucci, Massimo Lombardi, Maurizio Panunzio, and Andrea Santamato. 2025. "Cardio-Respiratory, Functional and Antalgic Effects of the Integrated Thermal Care Protocol After Breast Cancer Surgery" Life 15, no. 3: 374. https://doi.org/10.3390/life15030374
APA StyleBarassi, G., Spina, S., D’Alessandro, F., Prosperi, L., Marinucci, C., Lombardi, M., Panunzio, M., & Santamato, A. (2025). Cardio-Respiratory, Functional and Antalgic Effects of the Integrated Thermal Care Protocol After Breast Cancer Surgery. Life, 15(3), 374. https://doi.org/10.3390/life15030374