
Pattern Analysis of Benign and Malignant Atypical Melanocytic Skin Lesions of Palms and Soles: Variations of Dermoscopic Features According to Anatomic Site and Personal Experience

 , , ,
, , ,  ,
,  , ,
, ,  , ,
, ,  , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Testing Dataset
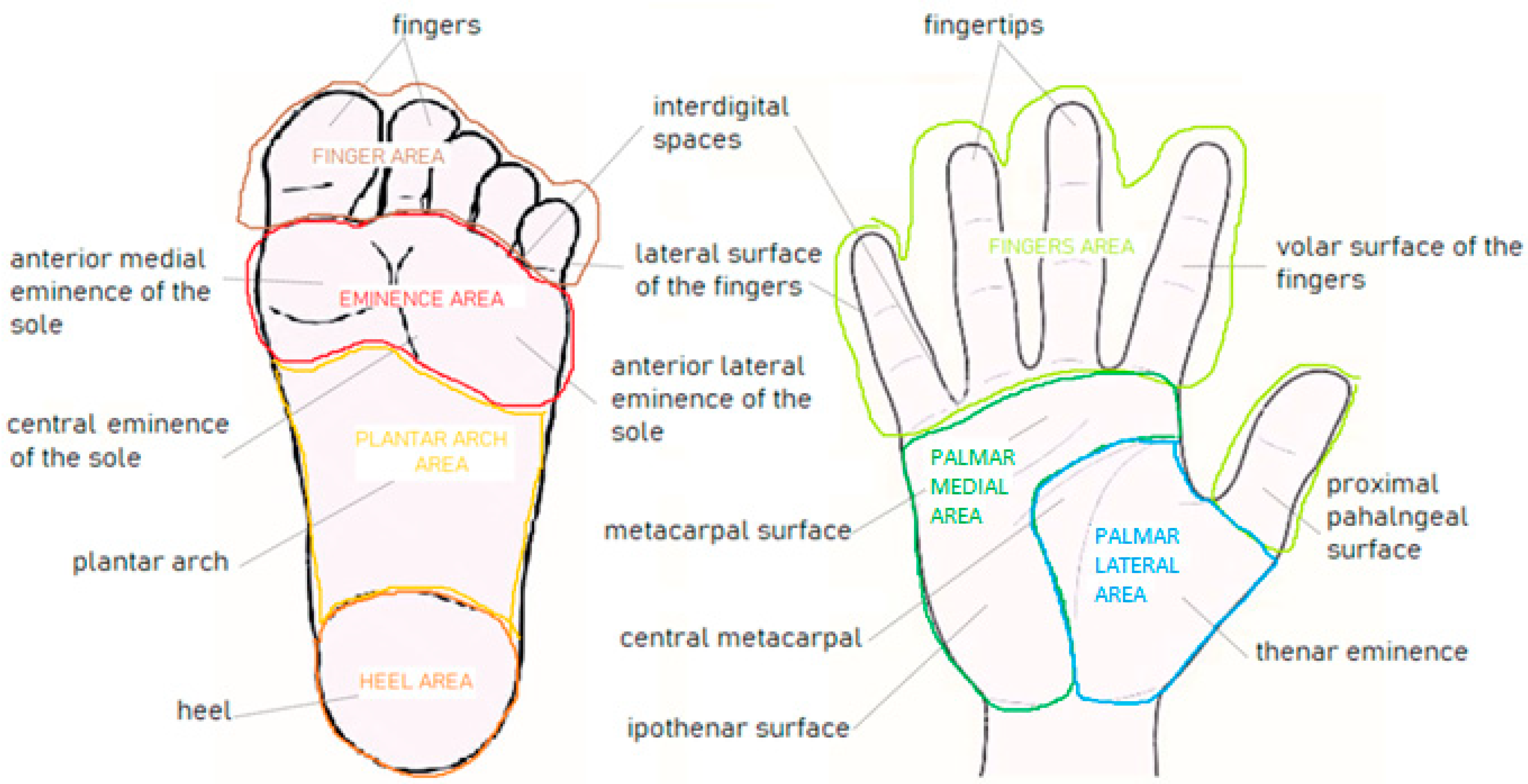
2.3. Anatomic, Functional, and Anatomo-Functional Classifications
2.4. Web Platform for Tele-Dermoscopy
2.5. Participants’ Data
2.6. Tele-Dermoscopic Pattern Analysis
2.7. Statistical Analysis
3. Results
3.1. Tele-Dermoscopic Tests
3.2. Case Study Characteristics
3.3. Anatomic Distribution of aMPPLs
3.4. Anatomo-Functional Distribution of aMPPLs
3.5. Pattern and Anatomic Distribution
3.5.1. Variation of Dermoscopic Features through Plantar Areas
3.5.2. Variation of Dermoscopic Features through Palmar Areas
- Skill-levels I–II
- Skill-levels III–IV
3.6. Dermoscopic Features and Anatomo-Functional Distribution
3.6.1. Distribution Analysis of Dermoscopic Patterns According to Histology and Plantar Location
- Eminence of the sole
- Toe
- Plantar arch
3.6.2. Distribution Analysis of Dermoscopic Patterns according to Histology and Palmar Location
4. Discussion
- (i)
- (ii)
- The anatomo-functional classification derived on this basis was also new as no cross-analysis was previously carried out between the anatomic location of MPPLs and their pattern analysis according to the pressure/traumatism/friction entity and according to the histopathology. [51,52,53,54,55] Here, we found the significant association of EM cases distribution on the macroareas “heel” (40.3% of cases, p < 0.0001) and “eminence of the sole” area (34% of cases). Of note, these two macroareas also have the highest degree of friction/traumatism and pressure among the sole areas. These distribution trends are in line with Japanese [54,57], Korean [58], and U.S. [59] monocentric studies on melanoma distribution on the soles concerning a predominance of the heel site, which can be considered the weight-bearing area subjected to major pressure/cm2.
- (iii)
- The majority of AN cases were distributed on the “plantar area” (87% of cases), followed by the toe area (“interdigital spaces” + “lateral surface of the fingers” + “plantar surface of the fingers” subareas). Of note, the “plantar area” and the “toe area” were subjected to no and mild pressure, respectively. Instead, in a Japanese population study by Miyazaki et al., the quote of acral nevi (n = 298) was similar among non-pressure-bearing (“plantar arch”) and pressure-bearing areas (eminence of the “sole” + ”heel” areas). [56] To date, only one study by Ghanavatian et al. took into account atypical nevi (25) beside typical ones (137), but cases were classified by histopathology and not by dermoscopy, and globally produced similar results in the comparison with 73 EM cases [54]. Similar literature data were reported in ethnic studies on benign-looking acral nevi in Mexican [41] and Korean [53] populations, where the plantar arch hosted the majority of acquired nevi cases.
- (iv)
- Concerning the anatomic and anatomo-functional distribution of aMPPLs on the palms, the highest relative quote of EM/aMPPLs was found in the “fingers area” (33%), mainly due to cases on the fingertips, where traumatism/friction is intense. Conversely, the subarea hosting the majority of AN was the “hypothenar surface”, corresponding to a site of moderate traumatism. These data are otherwise in line with the unique study investigating the anatomic density of melanomas and clear-cute benign acquired acral nevi on the palms, carried out on 34 Japanese patients [55]. The present anatomo-functional classification seems to confirm the hypothesis of a causative role in chronic traumatism/friction and mechanical stress in eliciting the malignant clone proliferation in predisposed subjects that was only raised based on monocentric studies but never confirmed on a large dataset [54,57,58,59,60]. Intense/unique traumatism was only reported anecdotally as inducing nodular melanoma at palms [61,62] but further data are needed, and the current knowledge is biased because of the fact that palmar melanoma is relatively rare in Caucasians. In addition, a melanomatous proliferation borderline with in situ acrolentiginous melanoma was recently described in a non-bearing area such as the plantar arch, induced by a unique curettage-related trauma [61]. Nevertheless, the investigation of anamnestic data concerning the “Chronic traumatism of palms” and the “Chronic traumatism of soles” performed during case collection produced poor data, which was inadequate for performing detailed statistical analysis. This can be attributed to the fact that most dermatologists usually do not collect/write down this kind of data in clinical reports during mole check visits [27].
- (v)
- The tele-dermoscopic setting allowed a huge number of dermatologists (61) and dermatology residents (95), performing pattern analysis over a series of 471 aMPPLs corresponding to the testing subset of the iDscore palmoplantar dataset of 542 cases [27]. In the pattern analysis of 86 dermoscopic images of EM cases of the sole, the evaluations of dermatologists’ and residents were not significantly different. The overall highest degree of concordance between the residents and dermatologists was obtained from the assessment of the parameters asymmetry of structures, followed by asymmetry of colors, considering all subareas.
- (vi)
- Notably, a series of dermoscopic findings appeared to be new compared with previous literature, essentially based on clear-cut lesions in different populations, as mentioned previously.
- (vii)
- Taking into account the pattern analysis data derived from experts evaluations, two features appeared to vary significantly (p < 0.05) among EM cases (asymmetry of structures predominates on the “toe” versus other three areas, parallel furrow pattern on the “toe + eminence of the sole” compared with the other areas) and two features among AN cases (p < 0.05): the parallel furrow pattern on the “eminence of the sole” + “toe” versus other areas; the lattice-like pattern on the “plantar arch” + “heel” versus other areas.
- (viii)
- It should also be noted that, in AN cases of the plantar area and toe, both residents and experts more frequently recognized two malignancy-suggestive patterns (asymmetry of colors and asymmetry of structures), than benignity-suggestive patterns such as parallel furrow pattern, regular fibrillar pattern.
- (ix)
- Concerning palmar aMPPLs, there were no significant differences in pattern recognition as performed by residents or dermatologists, in both EM and AN cases. Since the group of aMPPLs of the palms was not large, only descriptive analysis can be considered and data concerning the concordance analysis between dermatologists’ and residents cannot be performed. Globally, the “palmar medial area” composed of the “hypothenar surface” and “metacarpal surface”, subjected to moderate pressure, hosted the highest rate of aMPPLs. Among them, either challenging AN cases (that is, lesions exhibiting an asymmetry of structures and asymmetry of colors) and AN with parallel furrow pattern. Differently, in the lesions on the ”fingers area”, it was easier to recognize the benignity-suggestive pattern in AN cases and the malignancy-suggestive pattern in EM cases. These data may suggest that a degree of pattern interpretability/dermoscopic difficulty of aMPPLs of the palmar area is lower than the aMPPLs of the finger area [52,55].
- (x)
- The cross-analysis of dermoscopic pattern distribution through soles/palms subareas according to histologic output produced interesting results. In palms, where subgroups’ numerosity was very reduced, the data from descriptive analysis suggests that the parallel furrow pattern was easily recognized in all cases, independently from histologic outcome, and particularly at palmar medial area. On the other hand, AN cases were actually equivocal, having the parallel ridge pattern in 4/6 and the asymmetry of colors in 5/12 AN cases. We found two dermoscopic patterns able to statistically discriminate malignant from benign aMPPLs located in any area of the sole, namely asymmetry of colors and regression structures. Previous analysis also demonstrated that these two criteria were easily recognized by both groups of participants in malignant cases, and were often described in challenging AN cases, such as those on the plantar arch. No pattern was highly specific for benignity in all cases.
- ₋
- The toe area (interdigital spaces + lateral surface fingers + plantar surface fingers), subjected to none-to-moderate pressure/traumatism, was characterized by the easiest-to-diagnose EM cases, having the highest number of discriminant malignant features, i.e., asymmetry of structures, asymmetry of colors, irregular blotches, regression structures, and irregular diffuse pigmentation. Conversely, AN cases in this area were moderately difficult-to-diagnose, having similar rates of benign and malignant features.
- ₋
- In the heel area (subjected to the major pressure/cm2), the parallel furrow pattern and the lattice-like patterns were able to statistically differentiate benign from malignant aMPPLs (p = 0.014 and p = 0.001, respectively). In parallel, two patterns discriminated malign from benign aMPPLs, the asymmetry of colors (p = 0.002) and the regression structures (p = 0.025). This suggests that the differential diagnosis according to pattern analysis between AMs and EMs is somehow easiest in the heel area, where there are two malignant and two benign features available: this may be ascribed both to the highest number of melanoma cases overall and to the anatomical structure of heel skin undergoing intense/chronic pressure that determines a more polarized profile than other aMPPLs cases.
- ₋
- In the eminence of the sole area (anterior lateral eminence + anterior medial eminence + central eminence, subjected to moderate–intense pressure, Figure 1), three patterns statistically discriminated malignant from benign aMPPLs, namely asymmetry of colors (p = 0.025), regression structures (p = 0.003), and blue-white veil (p = 0.001). On the other hand, the features suggestive of benignity were not specific, with the parallel-furrow pattern recognized in 40% of AN cases versus 23.5% EM cases. Thus, this area can be characterized as a moderately difficult area.
- ₋
- In the plantar arch, the lattice-like pattern was statistically significant in distinguishing benign cases (p = 0.012): this trend was specific for this plantar area, where AN cases turned out to be particularly equivocal/difficult-to-describe. Moreover, four discriminant malignant features (p < 0.05) were detected (asymmetry of structures, asymmetry of colors, regression structures, and blue-white veil) but these data can be determined by the high number of AN cases (165) compared to EM cases (27) in this area.
5. Conclusions
- Concerning pattern analysis, the recognition rates of 12 dermoscopic patterns were not statistically different between residents and dermatologists. Thus, a series of consideration can be derived:
- The group of AN cases collected herein actually exhibited equivocal features and this was independent from the examiners’ personal experience in dermoscopy
- The asymmetry of colors and regression structures turned out to be statistically significant in the differentiation of EMs from AN, in any area of the sole, suggesting that these two dermoscopic patterns are more specific because they are more easily recognizable in EM than in AN, whereas the parallel ridge pattern appears as an equivocally interpreted feature.
- The parallel furrow pattern was globally poorly recognized in AN cases, probably due to a combination with another pattern.
- There was is an objective difficulty in discriminating the irregular fibrillar pattern from the regular fibrillar pattern among aMPPLs, both in dermatologists and residents’ evaluation, in line with recent reports [18,64] (nevertheless, the discrimination between regular and irregular fibrillar pattern and between parallel furrow pattern appearing as a regular fibrillar in weight-bearing areas is still a matter of debate) [64]. We should also consider that the prevalence of fibrillar patterns frequently detected on ANs of the plantar arch, a non-weight-bearing area, in this study, may be biased by the subgroup numerosity.
- The “plantar arch” ended up being the more challenging area for both residents and dermatologists, hosting the more “difficult” and equivocal lesions such as ANs exhibiting asymmetry of structures, colors, irregular blotches and irregular diffuse pigmentation, or EM cases exhibiting parallel-furrow pattern and/or more regression structures than in other areas.
- When looking at an aMPPL of the heel area, parallel furrow pattern (p = 0.014) or lattice-like (p = 0.001), patterns should be searched in order to identify benign cases, while asymmetry of colors (p = 0.002) and regression structures (p = 0.025) for malignant ones; if an aMPPLs in plantar arch exhibits a lattice-like pattern, it is likely to be benign (p = 0.012), while it is likely to be an EM if one observes either asymmetry of structures, asymmetry of colors, regression structures, or blue-white veil.
- Then, in the other macro areas, only malignancy-suggestive features were really different (p < 0.05) between EMs and ANs, namely in the toe area, the asymmetry of structures, asymmetry of colors, irregular blotches, regression structures, or irregular diffuse pigmentation; in the eminence of the sole area, the asymmetry of colors, regression structures, and blue-white veil.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Viale, P.H. The American Cancer Society’s Facts & Figures: 2020 Edition. J. Adv. Pract. Oncol. 2020, 11, 135–136. [Google Scholar] [PubMed]
- Huang, K.; Fan, J.; Misra, S. Acral lentiginous melanoma: Incidence and survival in the United States, 2006–2015, an analysis of the SEER registry. J. Surg. Res. 2020, 251, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Yeh, I.; Bastian, B.C. Melanoma pathology: New approaches and classification. Br. J. Dermatol. 2021, 185, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Yun, S.-J. Acral Melanocytic Neoplasms: A Comprehensive Review of Acral Nevus and Acral Melanoma in Asian Perspective. Dermatopathology 2022, 9, 292–303. [Google Scholar] [CrossRef] [PubMed]
- Madankumar, R.; Gumaste, P.V.; Martires, K.; Schaffer, P.R.; Choudhary, S.; Falto-Aizpurua, L.; Arora, H.; Kallis, P.J.; Patel, S.; Damanpour, S.; et al. Acral melanocytic lesions in the United States: Prevalence, awareness, and dermoscopic patterns in skin-of-color and non-Hispanic white patients. J. Am. Acad. Dermatol. 2016, 74, 724–730.e1. [Google Scholar] [CrossRef] [PubMed]
- Saida, T. Heterogeneity of the site of origin of malignant melanoma in ungual areas: “Subungual” malignant melanoma may be a misnomer. Br. J. Dermatol. 1992, 126, 529. [Google Scholar] [PubMed]
- Phan, A.; Touzet, S.; Dalle, S.; Ronger-Savlé, S.; Balme, B.; Thomas, L. Acral lentiginous melanoma: A clinicoprognostic study of 126 cases. Br. J. Dermatol. 2006, 155, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Nagore, E.; Pereda, C.; Botella-Estrada, R.; Requena, C.; Guillén, C. Acral lentiginous melanoma presents distinct clinical profile with high cancer susceptibility. Cancer Causes Control 2009, 20, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Durbec, F.; Martin, L.; Derancourt, C.; Grange, F. Melanoma of the hand and foot: Epidemiological, prognostic and genetic features. A systematic review. Br. J. Dermatol. 2012, 166, 727–739. [Google Scholar] [CrossRef]
- Moon, K.R.; Choi, Y.D.; Kim, J.M.; Jin, S.; Shin, M.-H.; Shim, H.-J.; Lee, J.-B.; Yun, S.J. Genetic Alterations in Primary Acral Melanoma and Acral Melanocytic Nevus in Korea: Common Mutated Genes Show Distinct Cytomorphological Features. J. Investig. Dermatol. 2018, 138, 933–945. [Google Scholar] [CrossRef]
- Hao, X.; Yim, J.; Chang, S.; Schwartz, E.; Rubenstein, S.; Friske, C.; Shamim, S.; Masternick, E.; Mirkin, G. Acral Lentiginous Melanoma of Foot and Ankle: A Clinicopathological Study of 7 Cases. Anticancer Res. 2019, 39, 6175–6181. [Google Scholar] [CrossRef]
- Smalley, K.S.M.; Teer, J.K.; Chen, Y.A.; Wu, J.-Y.; Yao, J.; Koomen, J.M.; Chen, W.-S.; Rodriguez-Waitkus, P.; Karreth, F.A.; Messina, J.L. A Mutational Survey of Acral Nevi. JAMA Dermatol. 2021, 157, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Fukushima, S.; Sheen, Y.S.; Ramelyte, E.; Pacheco, N.C.; Shi, C.; Liu, S.; Banik, I.; Aquino, J.D.; Acosta, M.S.; et al. The genetic evolution of acral melanoma. bioRxiv 2023. [Google Scholar] [CrossRef] [PubMed]
- Darmawan, C.C.; Jo, G.; Montenegro, S.E.; Kwak, Y.; Cheol, L.; Cho, K.H.; Mun, J.-H. Early detection of acral melanoma: A review of clinical, dermoscopic, histopathologic, and molecular characteristics. J. Am. Acad. Dermatol. 2019, 81, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.R.; Choi, S.H.; Jang, K.T.; Kim, J.H.; Mun, G.H.; Lee, J.; Lee, D.Y. Acral malignant melanoma; emphasis on the primary metastasis and the usefulness of preoperative ultrasound for sentinel lymph node metastasis. Sci. Rep. 2019, 9, 15894. [Google Scholar] [CrossRef]
- Bernardes, S.S.; Ferreira, I.; Elder, D.E.; Nobre, A.B.; Martínez-Said, H.; Adams, D.J.; Robles-Espinoza, C.D.; Possik, P.A. More than just acral melanoma: The controversies of defining the disease. J. Pathol. Clin. Res. 2021, 7, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Gumaste, P.V.; Fleming, N.H.; Silva, I.; Shapiro, R.L.; Berman, R.S.; Zhong, J.; Osman, I.; Stein, J.A. Analysis of recurrence patterns in acral versus nonacral melanoma: Should histologic subtype influence treatment guidelines? J. Natl. Compr. Cancer Netw. 2014, 12, 1706–1712. [Google Scholar] [CrossRef] [PubMed]
- Costello, C.M.; Ghanavatian, S.; Temkit, M.; Buras, M.R.; DiCaudo, D.J.; Swanson, D.L.; Mangold, A.R. Educational and practice gaps in the management of volar melanocytic lesions. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1450–1455. [Google Scholar] [CrossRef] [PubMed]
- Ingrassia, J.P.; Stein, J.A.; Levine, A.; Liebman, T.N. Diagnosis and Management of Acral Pigmented Lesions. Dermatol. Surg. Off. Publ. Am. Soc. Dermatol. Surg. 2023, 49, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Criscito, M.C.; Stein, J.A. Improving the diagnosis and treatment of acral melanocytic lesions. Melanoma Manag. 2017, 4, 113–123. [Google Scholar] [CrossRef]
- Metzger, S.; Ellwanger, U.; Stroebel, W.; Schiebel, U.; Rassner, G.; Fierlbeck, G. Extent and consequences of physician delay in the diagnosis of acral melanoma. Melanoma Res. 1998, 8, 181–186. [Google Scholar] [CrossRef]
- Argenyi, Z.B. Dermoscopy (epiluminescence microscopy) of pigmented skin lesions. Current status and evolving trends. Dermatol. Clin. 1997, 15, 79–95. [Google Scholar] [CrossRef]
- Longo, C.; Pampena, R.; Moscarella, E.; Chester, J.; Starace, M.; Cinotti, E.; Piraccini, B.M.; Argenziano, G.; Peris, K.; Pellacani, G. Dermoscopy of melanoma according to different body sites: Head and neck, trunk, limbs, nail, mucosal and acral. J. Eur. Acad. Dermatol. Venereol. 2023, 37, 1718–1730. [Google Scholar] [CrossRef]
- Tognetti, L.; Cartocci, A.; Cinotti, E.; Moscarella, E.; Farnetani, F.; Carrera, C.; Lallas, A.; Tiodorovic, D.; Longo, C.; Puig, S.; et al. Dermoscopy of early melanomas: Variation according to the anatomic site. Arch. Dermatol. Res. 2022, 314, 183–190. [Google Scholar] [CrossRef]
- Tognetti, L.; Cartocci, A.; Cinotti, E.; Moscarella, E.; Farnetani, F.; Lallas, A.; Tiodorovic, D.; Carrera, C.; Longo, C.; Puig, S.; et al. The impact of anatomical location and sun exposure on the dermoscopic recognition of atypical nevi and early melanomas: Usefulness of an integrated clinical-dermoscopic method (iDScore). J. Eur. Acad. Dermatol. Venereol. 2021, 35, 650–657. [Google Scholar] [CrossRef]
- Tognetti, L.; Cartocci, A.; Cinotti, E.; D’Onghia, M.; Żychowska, M.; Moscarella, E.; Dika, E.; Farnetani, F.; Guida, S.; Paoli, J.; et al. Dermoscopy of atypical pigmented lesions of the face: Variation according to facial areas. Exp. Dermatol. 2023, 32, 2166–2172. [Google Scholar] [CrossRef]
- Tognetti, L.; Cartocci, A.; Lallas, A.; Moscarella, E.; Stanganelli, I.; Nazzaro, G.; Paoli, J.; Fargnoli, M.C.; Broganelli, P.; Kittler, H.; et al. A European Multicentric Investigation of Atypical Melanocytic Skin Lesions of Palms and Soles: The iDScore-PalmoPlantar Database. Diagnostics 2024, 14, 460. [Google Scholar] [CrossRef]
- Phadungsaksawasdi, P.; Kasuya, A.; Fukuchi, K.; Aoshima, M.; Nakazawa, S.; Suzuki, T.; Fujiyama, T.; Tokura, Y.; Honda, T. Three-dimensional histological explanation of the dermoscopy patterns in acral melanocytic lesions. J. Dermatol. 2021, 48, 1193–1200. [Google Scholar] [CrossRef]
- Ozdemir, F.; Karaarslan, I.K.; Akalin, T. Variations in the dermoscopic features of acquired acral melanocytic nevi. Arch. Dermatol. 2007, 143, 1378–1384. [Google Scholar] [CrossRef] [PubMed]
- Malvehy, J.; Puig, S. Dermoscopic Patterns of Benign Volar Melanocytic Lesions in Patients with Atypical Mole Syndrome. Arch. Dermatol. 2004, 140, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Mikoshiba, Y.; Minagawa, A.; Koga, H.; Yokokawa, Y.; Uhara, H.; Okuyama, R. Clinical and Histopathologic Characteristics of Melanocytic Lesions on the Volar Skin without Typical Dermoscopic Patterns. JAMA Dermatol. 2019, 155, 578–584. [Google Scholar] [CrossRef]
- Altamura, D.; Zalaudek, I.; Sera, F.; Argenziano, G.; Fargnoli, M.C.; Rossiello, L.; Peris, K. Dermoscopic Changes in Acral Melanocytic Nevi during Digital Follow-up. Arch. Dermatol. 2007, 143, 1372–1376. [Google Scholar] [CrossRef]
- Rubegni, P.; Cevenini, G.; Nami, N.; Argenziano, G.; Saida, T.; Burroni, M.; Bono, R.; Quaglino, P.; Barbini, P.; Miracco, C.; et al. Dermoscopy and Digital Dermoscopy Analysis of Palmoplantar ‘Equivocal’ Pigmented Skin Lesions in Caucasians. Dermatology 2012, 225, 248–255. [Google Scholar] [CrossRef]
- Yun, S.J.; Bastian, B.C. Melanocytic tumours in acral skin. In WHO Classification of Skin Tumours; Elder, D.E., Massi, D., Scolyer, R.A., Willemze, R., Eds.; World Health Organization Classification of Tumours; International Agency for Research on Cancer: Lyon, France, 2018; Chapter 2; ISBN 978-92-832-2440-2. [Google Scholar]
- Lozeau, D.F.; Farber, M.J.; Lee, J.B. A nongrading histologic approach to Clark (dysplastic) nevi: A potential to decrease the excision rate. J. Am. Acad. Dermatol. 2016, 74, 68–74. [Google Scholar] [CrossRef]
- Minagawa, A.; Koga, H.; Saida, T. Dermoscopic characteristics of congenital melanocytic nevi affecting acral volar skin. Arch. Dermatol. 2011, 147, 809–813. [Google Scholar] [CrossRef]
- Roh, D.; Shin, K.; Kim, W.I.; Yang, M.Y.; Lee, W.K.; Kim, H.S.; Ko, H.C.; Kim, B.S.; Kim, M.B. Comparison of dermoscopic features between congenital and acquired acral melanocytic nevi in Korean patients. J. Eur. Acad. Dermatol. Venereol. JEADV 2020, 34, 1004–1009. [Google Scholar] [CrossRef]
- Altamura, D.; Altobelli, E.; Micantonio, T.; Piccolo, D. Dermoscopic patterns of acral melanocytic nevi and melanomas in a white population in central Italy. Arch. Dermatol. 2006, 142, 1123–1128. [Google Scholar] [CrossRef]
- EUR-Lex-32016R0679-EN-EUR-Lex Regulation—2016/679—EN—Gdpr—EUR-Lex. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 16 January 2024).
- Tognetti, L.; Cartocci, A.; Żychowska, M.; Savarese, I.; Cinotti, E.; Pizzichetta, M.A.; Moscarella, E.; Longo, C.; Farnetani, F.; Guida, S.; et al. A risk-scoring model for the differential diagnosis of lentigo maligna and other atypical pigmented facial lesions of the face: The facial iDScore. Acad. Dermatol. Venereol. 2023, 37, 2301–2310. [Google Scholar] [CrossRef]
- González-Ramírez, R.A.; Guerra-Segovia, C.; Garza-Rodríguez, V.; Garza-Báez, P.; Gómez-Flores, M.; Ocampo-Candiani, J. Dermoscopic features of acral melanocytic nevi in a case series from Mexico. Ann. Bras. Dermatol. 2018, 93, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Phan, A.; Dalle, S.; Touzet, S.; Ronger-Savlé, S.; Balme, B.; Thomas, L. Dermoscopic features of acral lentiginous melanoma in a large series of 110 cases in a white population. Br. J. Dermatol. 2010, 162, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Mun, J.-H.; Jo, G.; Darmawan, C.C.; Park, J.; Bae, J.M.; Jin, H.; Kim, W.-I.; Kim, H.-S.; Ko, H.-C.; Kim, B.-S.; et al. Association between Breslow thickness and dermoscopic findings in acral melanoma. J. Am. Acad. Dermatol. 2018, 79, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Saida, T.; Miyazaki, A.; Oguchi, S.; Ishihara, Y.; Yamazaki, Y.; Murase, S.; Yoshikawa, S.; Tsuchida, T.; Kawabata, Y.; Tamaki, K. Significance of Dermoscopic Patterns in Detecting Malignant Melanoma on Acral Volar Skin: Results of a Multicenter Study in Japan. Arch. Dermatol. 2004, 140, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Margolis, R.J.; Tong, A.K.F.; Byers, H.R.; Mihm, M.C. Comparison of acral nevomelanocytic proliferations in Japanese and whites. J. Investig. Dermatol. 1989, 92 (Suppl. S5), 222S–226S. [Google Scholar] [CrossRef]
- Saida, T.; Oguchi, S.; Miyazaki, A. Dermoscopy for acral pigmented lesions. Clin. Dermatol. 2002, 20, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, C.; Kyrgidis, A.; Ilut, P.A.; Gkentsidi, T.; Manoli, S.-M.; Camela, E.; Apalla, Z. Acral Melanocytic Nevi in a High-Risk Population: Prevalence, Clinical Characteristics and Dermatoscopic Patterns. Dermatology 2023, 239, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Saida, T.; Oguchi, S.; Ishihara, Y. In vivo observation of magnified features of pigmented lesions on volar skin using video macroscope: Usefulness of epiluminescence techniques in clinical diagnosis. Arch. Dermatol. 1995, 131, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Bravo Puccio, F.; Chian, C. Acral junctional nevus versus acral lentiginous melanoma in situ: A differential diagnosis that should be based on clinicopathologic correlation. Arch. Pathol. Lab. Med. 2011, 135, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Tognetti, L.; Cevenini, G.; Moscarella, E.; Cinotti, E.; Farnetani, F.; Lallas, A.; Tiodorovic, D.; Carrera, C.; Puig, S.; Perrot, J.L.; et al. Validation of an integrated dermoscopic scoring method in an European teledermoscopy web platform: The iDScore project for early detection of melanoma. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Tognetti, L.; Cinotti, E.; Farnetani, F.; Lallas, A.; Paoli, J.; Longo, C.; Pampena, R.; Moscarella, E.; Argenziano, G.; Tiodorovic, D.; et al. Development and Implementation of a Web-Based International Registry Dedicated to Atypical Pigmented Skin Lesions of the Face: Teledermatologic Investigation on Epidemiology and Risk Factors. Telemed. J. E Health 2023, 29, 1356–1365. [Google Scholar] [CrossRef]
- Emiroglu, N.; Cengiz, F.P.; Onsun, N. Age and Anatomical Location-Related Dermoscopic Patterns of 210 Acral Melanocytic Nevi in a Turkish Population. J. Cutan. Med. Surg. 2017, 21, 388–394. [Google Scholar] [CrossRef]
- Kim, N.H.; Choi, Y.D.; Seon, H.J.; Lee, J.-B.; Yun, S.J. Anatomic mapping and clinicopathologic analysis of benign acral melanocytic neoplasms: A comparison between adults and children. J. Am. Acad. Dermatol. 2017, 77, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Ghanavatian, S.; Costello, C.M.; Buras, M.R.; Cumsky, H.J.L.; Pittelkow, M.R.; Swanson, D.L.; Mangold, A.R. Density and distribution of acral melanocytic nevi and acral melanomas on the plantar surface of the foot. J. Am. Acad. Dermatol. 2019, 80, 790–792.e2. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, M.; Yamamoto, Y.; Hara, T.; Okuhira, H.; Inaba, Y.; Kunimoto, K.; Mikita, N.; Kaminaka, C.; Kanazawa, N.; Jinnin, M. Difference in distribution of malignant melanoma and melanocytic nevus in the palm and finger. Biosci. Trends 2019, 13, 361–363. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, A.; Saida, T.; Koga, H.; Oguchi, S.; Suzuki, T.; Tsuchida, T. Anatomical and dermoscopic patterns seen in melanocytic nevi on the soles: A retrospective study. J. Am. Acad. Dermatol. 2005, 53, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, A.; Omodaka, T.; Okuyama, R. Melanomas and Mechanical Stress Points on the Plantar Surface of the Foot. N. Engl. J. Med. 2016, 374, 2404–2406. [Google Scholar] [CrossRef]
- Jung, H.J.; Kweon, S.S.; Lee, J.B.; Lee, S.C.; Yun, S.J. A clinicopathologic analysis of 177 acral melanomas in Koreans: Relevance of spreading pattern and physical stress. JAMA Dermatol. 2013, 149, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Costello, C.M.; Pittelkow, M.R.; Mangold, A.R. Acral Melanoma and Mechanical Stress on the Plantar Surface of the Foot. N. Engl. J. Med. 2017, 377, 395–396. [Google Scholar] [CrossRef] [PubMed]
- Tognetti, L.; La Marca, F.; Rubegni, P. Acral lentiginous in situ melanoma arising after trauma of the plantar arch. Dermatol. Pract. Concept. 2024, in press.
- Feibleman, C.E.; Stoll, H.; Maize, J.C. Melanomas of the palm, sole, and nailbed: A clinicopathologic study. Cancer 1980, 46, 2492–2504. [Google Scholar] [CrossRef] [PubMed]
- Jaroonwanichkul, S.; Fan, E.; Matthews, S.; Ho, B.V.; Hall, J.C. Acral Nodular Melanoma at a Site of Trauma. Kans. J. Med. 2023, 25, 187–188. [Google Scholar] [CrossRef]
- Koga, H.; Saida, T. Revised 3-step dermoscopic algorithm for the management of acral melanocytic lesions. Arch. Dermatol. 2011, 147, 741–743. [Google Scholar] [CrossRef]
- Saida, T.; Koga, H.; Uhara, H. Dermoscopy for Acral Melanocytic Lesions: Revision of the 3-step Algorithm and Refined Definition of the Regular and Irregular Fibrillar Pattern. Dermatol. Pract. Concept. 2022, 12, e2022123. [Google Scholar] [CrossRef] [PubMed]
- Lallas, A.; Kyrgidis, A.; Koga, H.; Moscarella, E.; Tschandl, P.; Apalla, Z.; Di Stefani, A.; Ioannides, D.; Kittler, H.; Kobayashi, K.; et al. The BRAAFF checklist: A new dermoscopic algorithm for diagnosing acral melanoma. Br. J. Dermatol. 2015, 173, 1041–1049. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| LESION DATA | aMPPLs N= 471 | MM N = 94 | AN N = 377 | p |
|---|---|---|---|---|
| N (%)/Mean ± SD | ||||
| Maximum diameter (mm) | 8.24 ± 6.3 | 15.30 ± 9.95 | 6.49 ± 3.08 | <0.001 |
| PATIENT DATA | ||||
| Age | 45.39 ± 18.96 | 63.97 ± 14.87 | 40.75 ± 16.94 | <0.001 |
| Male | 307 (65.2%) | 45 (47.9%) | 119 (31.6%) | 0.004 |
| Female | 164 (34.8%) | 49 (52.1%) | 258 (68.4%) | |
| ANAMNESTIC DATA/RISK FACTORS * | ||||
| Personal/family history of melanoma—1st degree relative | 11 (2.3%) | 0 (0.0%) | 11 (13.6%) | 0.520 |
| Presence of >100 common nevi or >10 AN on the body | 24 (5.1%) | 3 (30%) | 21 (25.9%) | 1.000 |
| Chronic traumatism of palms | 1 (0.2%) | 0 (0%) | 1 (1.1%) | 1.000 |
| Chronic traumatism of soles | 10 (2.1%) | 0 (0%) | 10 (7.2%) | 0.601 |
| Patients’ phototype | 355 (75.4%) | 0.717 | ||
| II | 94 (20%) | 19 (29.7%) | 75 (25.8%) | |
| III | 248 (52.7%) | 44 (68.8%) | 204 (70.1%) | |
| IV | 11 (2.3%) | 1 (1.6%) | 10 (3.4%) | |
| V | 2 (0.4%) | 0 (0.0%) | 2 (0.7%) | |
| Anatomic Classification | Histopathologic Classification | Functional Classification (Pressure /chronic traumatism) | Anatomo-Functional Classification | Histopathologic-Functional Classification | ||||
| MM | AN | p | MM | AN | p | |||
| All areas | 94 | 377 | 94 | 377 | ||||
| 8 subareas of the sole | 86 (19.7%) | 349 (80.2%) | 4 areas—sole | 17 (18.1%) | 56 (14.9%) | 0.422 | ||
| Anterior lateral eminence | 2 (2.1) | 13 (3.4) | 0.746 | Intense | Eminence of the sole area (intense) | |||
| Anterior medial eminence | 12 (12.8) | 25 (6.6) | 0.055 | Intense | ||||
| Central eminence | 3 (3.2) | 18 (4.8) | 0.780 | Moderate | ||||
| Heel | 23 (24.5) | 34 (9.0) | <0.001 | Intense | Heel area | 23 (24.5%) | 34 (9.0%) | <0.001 |
| Plantar region | 27 (28.7) | 180 (47.7) | 0.001 | None | Plantar area | 27 (28.7%) | 180 (47.7%) | 0.001 |
| Interdigital spaces | 2 (2.1) | 25 (6.6) | 0.134 | None | Toe area (moderate) | 19 (20.2%) | 79 (21%) | 1.000 |
| Lateral surface fingers | 8 (8.5) | 26 (6.9) | 0.655 | Mild | ||||
| Plantar surface fingers | 9 (9.6) | 28 (7.4) | 0.520 | Moderate | ||||
| 9 Subareas of the palms | 8 | 28 | 3 areas—palms | 8 | 28 | 0.392 | ||
| Fingertips (hand) | 2 (2.1) | 0 (0.0%) | 0.039 | Intense | Fingers area (moderate) | |||
| Interdigital spaces | 0 (0.0%) | 3 (0.8) | 1.000 | Mild | 3 (3.2%) | 6 (1.6%) | ||
| Lateral surface fingers | 1 (1.1%) | 0 (0.0%) | 0.200 | Moderate | ||||
| Volar surface fingers | 0 (0.0%) | 3 (0.8%) | 1.000 | Intense | ||||
| Proximal phalangeal surface | 0 (0%) | 0 (0%) | intense | |||||
| Ipothenar surface | 0 (0.0%) | 8 (2.1%) | 0.367 | Moderate | Palmar medial area (moderate) | 3 (3.2%) | 14 (3.7%) | 1.000 |
| Metacarpal surface | 3 (3.2%) | 6 (1.6%) | 0.392 | Moderate | ||||
| Central metacarpal | 0 (0.0%) | 2 (0.5%) | 1.000 | Mild | Palmar lateral area (moderate-mild) | 2 (2.1%) | 8 (2.1%) | 1.000 |
| Thenar surface | 2 (2.1%) | 6 (1.6%) | 0.663 | Moderate | ||||
| Dermoscopic Pattern Analysis | Skill Levels I–II (n = 87) ° | Skill Levels III–IV (n = 61) ° | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 4 Subareas * | Eminence Sole | Heel | Plantar arch | Toe | p | EminenceSole | Heel | PlantarArch | Toe | p |
| Melanoma cases (n) | 17 | 23 | 27 | 19 | 17 | 23 | 27 | 19 | ||
| Asymmetry of structures | 9 (52.9) | 15 (65.2) | 21 (77.8) | 14 (73.7) | 0.342 | 9 (52.9) | 12 (52.2) | 22 (81.5) | 18 (94.7) | 0.004 |
| Asymmetry of colors | 13 (76.5) | 15 (65.2) | 25 (92.6) | 14 (73.7) | 0.124 | 11 (64.7) | 16 (69.6) | 23 (85.2) | 15 (78.9) | 0.391 |
| Parallel ridge pattern | 3 (17.6) | 3 (13.0) | 2 (7.4) | 3 (15.8) | 0.749 | 2 (11.8) | 8 (34.8) | 5 (18.5) | 2 (10.5) | 0.171 |
| irregular blotches | 3 (17.6) | 6 (26.1) | 8 (29.6) | 6 (31.6) | 0.786 | 6 (35.3) | 6 (26.1) | 9 (33.3) | 12 (63.2) | 0.080 |
| regression structures | 8 (47.1) | 8 (34.8) | 13 (48.1) | 5 (26.3) | 0.416 | 8 (47.1) | 9 (39.1) | 15 (55.6) | 7 (36.8) | 0.558 |
| Blue-white veil | 5 (29.4) | 5 (21.7) | 11 (40.7) | 7 (36.8) | 0.515 | 8 (47.1) | 6 (26.1) | 10 (37.0) | 6 (31.6) | 0.564 |
| Irregular streaks | 2 (11.8) | 1 (4.3) | 4 (14.8) | 3 (15.8) | 0.621 | 3 (17.6) | 3 (13.0) | 6 (22.2) | 3 (15.8) | 0.856 |
| Irregular diffuse Pigmentation | 5 (29.4) | 5 (21.7) | 3 (11.1) | 5 (26.3) | 0.448 | 4 (23.5) | 3 (13.0) | 7 (25.9) | 5 (26.3) | 0.673 |
| Irregular fibrillar pattern | 0 (0.0) | 1 (4.3) | 1 (3.7) | 0 (0.0) | 0.683 | 3 (17.6) | 1 (4.3) | 3 (11.1) | 2 (10.5) | 0.601 |
| Parallel furrow pattern | 1 (5.9) | 1 (4.3) | 0 (0.0) | 0 (0.0) | 0.483 | 4 (23.5) | 0 (0.0) | 0 (0.0) | 4 (21.1) | 0.006 |
| Regular fibrillar pattern | 2 (11.8) | 2 (8.7) | 0 (0.0) | 1 (5.3) | 0.373 | 0 (0.0) | 1 (4.3) | 0 (0.0) | 2 (10.5) | 0.218 |
| Lattice-like pattern | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | 1 (5.9) | 0 (0.0) | 1 (3.7) | 1 (5.3) | 0.729 |
| Nevi cases (n) | 55 | 32 | 179 | 77 | 50 | 31 | 165 | 68 | ||
| Asymmetry of structures | 17 (30.9) | 3 (9.4) | 44 (24.6) | 21 (27.3) | 0.142 | 16 (32.0) | 9 (29.0) | 45 (27.3) | 22 (32.4) | 0.847 |
| Asymmetry of colors | 15 (27.3) | 4 (12.5) | 52 (29.1) | 23 (29.9) | 0.256 | 15 (30.0) | 7 (22.6) | 45 (27.3) | 22 (32.4) | 0.752 |
| Parallel ridge pattern | 4 (7.3) | 2 (6.2) | 10 (5.6) | 10 (13.0) | 0.229 | 7 (14.0) | 3 (9.7) | 15 (9.1) | 9 (13.2) | 0.685 |
| Irregular blotches | 6 (10.9) | 2 (6.2) | 15 (8.4) | 7 (9.1) | 0.893 | 13 (26.0) | 3 (9.7) | 24 (14.5) | 14 (20.6) | 0.150 |
| Regression structures | 6 (10.9) | 1 (3.1) | 19 (10.6) | 8 (10.4) | 0.608 | 5 (10.0) | 3 (9.7) | 21 (12.7) | 5 (7.4) | 0.672 |
| Blue-white veil | 8 (14.5) | 1 (3.1) | 14 (7.8) | 11 (14.3) | 0.139 | 4 (8.0) | 2 (6.5) | 12 (7.3) | 8 (11.8) | 0.694 |
| Irregular streaks | 9 (16.4) | 1 (3.1) | 6 (3.4) | 8 (10.4) | 0.004 | 4 (8.0) | 2 (6.5) | 19 (11.5) | 9 (13.2) | 0.678 |
| Irregular diffuse Pigmentation | 4 (7.3) | 0 (0.0) | 16 (8.9) | 6 (7.8) | 0.375 | 3 (6.0) | 3 (9.7) | 16 (9.7) | 1 (1.5) | 0.159 |
| Irregular fibrillar pattern | 7 (12.7) | 2 (6.2) | 17 (9.5) | 0 (0.0) | 0.024 | 4 (8.0) | 4 (12.9) | 21 (12.7) | 8 (11.8) | 0.833 |
| Parallel furrow pattern | 12 (21.8) | 9 (28.1) | 50 (27.9) | 23 (29.9) | 0.769 | 20 (40.0) | 9 (29.0) | 37 (22.4) | 26 (38.2) | 0.027 |
| Regular fibrillar pattern | 5 (9.1) | 8 (25.0) | 25 (14.0) | 4 (5.2) | 0.024 | 9 (18.0) | 7 (22.6) | 17 (10.3) | 5 (7.4) | 0.079 |
| Lattice-like pattern | 7 (12.7) | 11 (34.4) | 38 (21.2) | 14 (18.2) | 0.105 | 9 (18.0) | 13 (41.9) | 47 (28.5) | 13 (19.1) | 0.047 |
| Dermoscopic Pattern Analysis | Skill Levels I–II (n = 26) ° | Skill Levels III–IV (n = 30) ° | ||||
|---|---|---|---|---|---|---|
| 3 Subareas * | Fingers | Palmar Lateral | PalmarMedial | Fingers | PalmarLateral | PalmarMedial |
| Melanoma cases (n) | 3 | 3 | 2 | 3 | 3 | 2 |
| Asymmetry of structures | 2 (66.7) | 2 (66.7) | 2 (100.0) | 2 (66.7) | 2 (66.7) | 1 (50.0) |
| Asymmetry of colors | 3 (100.0) | 2 (66.7) | 2 (100.0) | 3 (100.0) | 2 (66.7) | 1 (50.0) |
| Parallel ridge pattern | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (100.0) | 0 (0.0) | 0 (0.0) |
| Irregular blotches | 1 (33.3) | 2 (66.7) | 1 (50.0) | 2 (66.7) | 1 (33.3) | 0 (0.0) |
| Regression structures | 1 (33.3) | 1 (33.3) | 1 (50.0) | 2 (66.7) | 2 (66.7) | 0 (0.0) |
| Blue-white veil | 1 (33.3) | 1 (33.3) | 0 (0.0) | 1 (33.3) | 1 (33.3) | 0 (0.0) |
| Irregular streaks | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Irregular diffuse pigmentation | 2 (66.7) | 1 (33.3) | 1 (50.0) | 1 (33.3) | 1 (33.3) | 0 (0.0) |
| Irregular fibrillar pattern | 1 (33.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Parallel furrow pattern | 1 (33.3) | 0 (0.0) | 0 (0.0) | 1 (33.3) | 0 (0.0) | 0 (0.0) |
| Regular fibrillar pattern | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Lattice-like pattern | 0 (0.0) | 1 (33.3) | 0 (0.0) | 0 (0.0) | 1 (33.3) | 0 (0.0) |
| Nevi cases (n) | 6 | 14 | 8 | 6 | 12 | 8 |
| Asymmetry of structures | 0 (0.0) | 6 (42.9) | 4 (50.0) | 1 (16.7) | 4 (33.3) | 1 (12.5) |
| Asymmetry of colors | 0 (0.0) | 5 (35.7) | 2 (25.0) | 1 (16.7) | 5 (41.7) | 2 (25.0) |
| Parallel ridge pattern | 0 (0.0) | 1 (7.1) | 1 (12.5) | 4 (66.7) | 0 (0.0) | 0 (0.0) |
| Irregular blotches | 0 (0.0) | 1 (7.1) | 1 (12.5) | 2 (33.3) | 0 (0.0) | 1 (12.5) |
| Regression structures | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (8.3) | 0 (0.0) |
| Blue-white veil | 0 (0.0) | 0 (0.0) | 1 (12.5) | 1 (16.7) | 0 (0.0) | 0 (0.0) |
| Irregular streaks | 1 (16.7) | 2 (14.3) | 1 (12.5) | 0 (0.0) | 0 (0.0) | 2 (25.0) |
| Irregular diffuse pigmentation | 1 (16.7) | 0 (0.0) | 0 (0.0) | 1 (16.7) | 1 (8.3) | 0 (0.0) |
| Irregular fibrillar pattern | 1 (16.7) | 1 (7.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (12.5) |
| Parallel furrow pattern | 2 (33.3) | 5 (35.7) | 5 (62.5) | 2 (33.3) | 7 (58.3) | 4 (50.0) |
| Regular fibrillar pattern | 0 (0.0) | 1 (7.1) | 2 (25.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Lattice-like pattern | 2 (33.3) | 5 (35.7) | 1 (12.5) | 1 (16.7) | 2 (16.7) | 3 (37.5) |
| 4 Subareas | Eminence of the Sole * | Heel | Toe ° | Plantar Arch | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N (%)/Mean ± SD | MM | AN | p | MM | AN | p | MM | AN | p | MM | AN | p |
| Dermoscopic patterns | 17 | 50 | 23 | 31 | 19 | 68 | 27 | 165 | ||||
| Asymmetry of structures | 9 (52.9) | 16 (32.0) | 0.211 | 12 (52.2) | 9 (29.0) | 0.149 | 18 (94.7) | 22 (32.4) | <0.001 | 22 (81.5) | 45 (27.3) | <0.001 |
| Asymmetry of colors | 11 (64.7) | 15 (30.0) | 0.025 | 16 (69.6) | 7 (22.6) | 0.002 | 15 (78.9) | 22 (32.4) | 0.001 | 23 (85.2) | 45 (27.3) | 0.001 |
| Parallel ridge pattern | 2 (11.8) | 7 (14.0) | 1.000 | 8 (34.8) | 3 (9.7) | 0.054 | 2 (10.5) | 9 (13.2) | 1.000 | 5 (18.5) | 15 (9.1) | 0.251 |
| Irregular blotches | 6 (35.3) | 13 (26.0) | 0.672 | 6 (26.1) | 3 (9.7) | 0.218 | 12 (63.2) | 14 (20.6) | 0.001 | 9 (33.3) | 24 (14.5) | 0.034 |
| Regression structures | 8 (47.1) | 5 (10.0) | 0.003 | 9 (39.1) | 3 (9.7) | 0.025 | 7 (36.8) | 5 (7.4) | 0.004 | 15 (55.6) | 21 (12.7) | <0.001 |
| Blue-white veil | 8 (47.1) | 4 (8.0) | 0.001 | 6 (26.1) | 2 (6.5) | 0.105 | 6 (31.6) | 8 (11.8) | 0.085 | 10 (37.0) | 12 (7.3) | <0.001 |
| Irregular streaks | 3 (17.6) | 4 (8.0) | 0.506 | 3 (13.0) | 2 (6.5) | 0.725 | 3 (15.8) | 9 (13.2) | 1.000 | 6 (22.2) | 19 (11.5) | 0.221 |
| Irregular diffuse Pigmentation | 4 (23.5) | 3 (6.0) | 0.114 | 3 (13.0) | 3 (13.3) | 1.000 | 5 (26.3) | 1 (1.5) | 0.001 | 7 (25.9) | 16 (9.7) | 0.037 |
| Irregular fibrillar pattern | 3 (17.6) | 4 (8.0) | 0.506 | 1 (4.3) | 4 (12.9) | 0.550 | 2 (10.5) | 8 (11.8) | 1.000 | 3 (11.1) | 21 (12.7) | 1.000 |
| Parallel furrow pattern | 4 (23.5) | 20 (40.0) | 0.352 | 0 (0.0) | 9 (29.0) | 0.014 | 4 (21.1) | 26 (38.2) | 0.263 | 0 (0.0) | 37 (22.4) | 0.013 |
| Regular fibrillar pattern | 0 (0.0) | 9 (18.0) | 0.142 | 1 (4.3) | 7 (22.6) | 0.140 | 2 (10.5) | 5 (7.4) | 1.000 | 0 (0.0) | 17 (10.3) | 0.167 |
| Lattice-like pattern | 1 (5.9) | 9 (18.0) | 0.414 | 0 (0.0) | 13 (41.9) | 0.001 | 1 (5.3) | 13 (19.1) | 0.271 | 1 (3.7) | 47 (28.5) | 0.012 |
| PALMAR AREAS * | Fingers | Palmar Lateral | Palmar Medial | |||
|---|---|---|---|---|---|---|
| N (%)/Mean ± SD | MM | AN | MM | AN | MM | AN |
| Dermoscopic patterns | 3 | 6 | 3 | 12 | 2 | 8 |
| Asymmetry of structures | 2 (66.7) | 1 (16.7) | 2 (66.7) | 4 (33.3) | 1 (50.0) | 1 (12.5) |
| Asymmetry of colours | 3 (100.0) | 1 (16.7) | 2 (66.7) | 5 (41.7) | 1 (50.0) | 2 (25.0) |
| Parallel ridge pattern | 3 (100.0) | 4 (66.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Irregular blotches | 2 (66.7) | 2 (33.3) | 1 (33.3) | 0 (0.0) | 0 (0.0) | 1 (12.5) |
| Regression structures | 2 (66.7) | 0 (0.0) | 2 (66.7) | 1 (8.3) | 0 (0.0) | 0 (0.0) |
| Blue-white veil | 1 (33.3) | 1 (16.7) | 1 (33.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Irregular streaks | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (25.0) |
| Irregular diffuse pigmentation | 1 (33.3) | 1 (16.7) | 1 (33.3) | 1 (8.3) | 0 (0.0) | 0 (0.0) |
| Irregular fibrillar pattern | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (12.5) |
| Parallel furrow pattern | 1 (33.3) | 2 (33.3) | 0 (0.0) | 7 (58.3) | 0 (0.0) | 4 (50.0) |
| Regular fibrillar pattern | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Lattice-like pattern | 0 (0.0) | 1 (16.7) | 1 (33.3) | 2 (16.7) | 0 (0.0) | 3 (37.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tognetti, L.; Cartocci, A.; Moscarella, E.; Lallas, A.; Dika, E.; Fargnoli, M.C.; Longo, C.; Nazzaro, G.; Paoli, J.; Stanganelli, I.; et al. Pattern Analysis of Benign and Malignant Atypical Melanocytic Skin Lesions of Palms and Soles: Variations of Dermoscopic Features According to Anatomic Site and Personal Experience. Life 2024, 14, 659. https://doi.org/10.3390/life14060659
Tognetti L, Cartocci A, Moscarella E, Lallas A, Dika E, Fargnoli MC, Longo C, Nazzaro G, Paoli J, Stanganelli I, et al. Pattern Analysis of Benign and Malignant Atypical Melanocytic Skin Lesions of Palms and Soles: Variations of Dermoscopic Features According to Anatomic Site and Personal Experience. Life. 2024; 14(6):659. https://doi.org/10.3390/life14060659
Chicago/Turabian StyleTognetti, Linda, Alessandra Cartocci, Elvira Moscarella, Aimilios Lallas, Emi Dika, Maria Concetta Fargnoli, Caterina Longo, Gianluca Nazzaro, John Paoli, Ignazio Stanganelli, and et al. 2024. "Pattern Analysis of Benign and Malignant Atypical Melanocytic Skin Lesions of Palms and Soles: Variations of Dermoscopic Features According to Anatomic Site and Personal Experience" Life 14, no. 6: 659. https://doi.org/10.3390/life14060659
APA StyleTognetti, L., Cartocci, A., Moscarella, E., Lallas, A., Dika, E., Fargnoli, M. C., Longo, C., Nazzaro, G., Paoli, J., Stanganelli, I., Magi, S., Lacarrubba, F., Broganelli, P., Perrot, J.-L., Suppa, M., Kittler, H., Giuffrida, R., Cinotti, E., Sofia, L. C., ... Rubegni, P. (2024). Pattern Analysis of Benign and Malignant Atypical Melanocytic Skin Lesions of Palms and Soles: Variations of Dermoscopic Features According to Anatomic Site and Personal Experience. Life, 14(6), 659. https://doi.org/10.3390/life14060659