

Primary Hyperhidrosis in Children—A Retrospective Study and a Short Review


 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
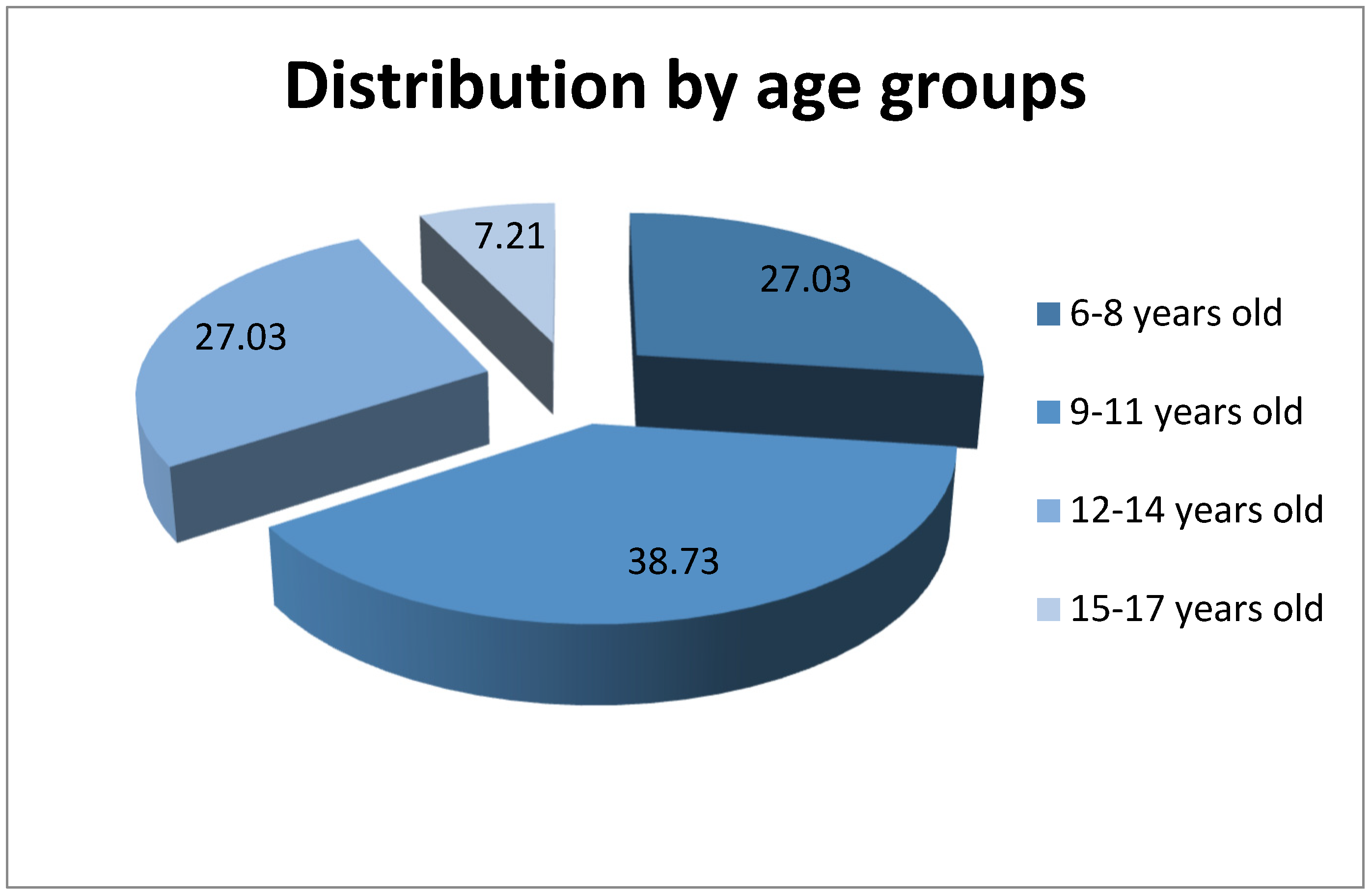
- 6–8 years old—30 children (27.03%), 27 (90%) girls and 3 (10%) boys
- 9–11 years old—43 children (38.73%), 25 (58.14%) girls and 18 (41.86%) boys
- 12–14 years old—30 children (27.03%), 15 (50%) girls and 15 (50%) boys
- 15–17 years old—8 children (7.21%), 0 (0%) girls and 8 (100%) boys
4. Discussion
- Secondary—after medication consumption or from an underlying medical condition, characterized by generalized exaggerated sweating [23]. This usually affects older persons, is asymmetric, may occur at night, during sleep, and is not associated with a familial history [24,25]. The most common triggers are cardiac diseases, endocrinopathies, proliferative diseases, metabolic and psychiatric disorders, nervous system diseases [24,26], or as an adverse reaction to drugs: Cliclooxygenase inhibitors, opioid analgesics, antiviral medication, antibiotics or hypotensive medicaments [24,27].
- 6 or more months of focal, detectable, visible, exaggerated sweating without an explanation.
- 2 or more of the following features:
5. Conclusions
- Hyperhidrosis has a significant impact on the patient. The therapeutic options are varied, each having advantages, disadvantages and adverse effects.
- Hyperhidrosis is underdiagnosed and many cases are not reported and treated, due to the lack of knowledge of therapeutic options for pediatric patients.
- Children are more prone to emotional suffering; their social and psychological development being affected.
- The increased prevalence in girls is false, because they are more likely to report and seek treatment.
- In this study, an increased ratio of girls/boys is observed in the age range between 6 and 11 years, after which the ratio equalizes at 12–14 years, and then reverses in the 15–17 age group.
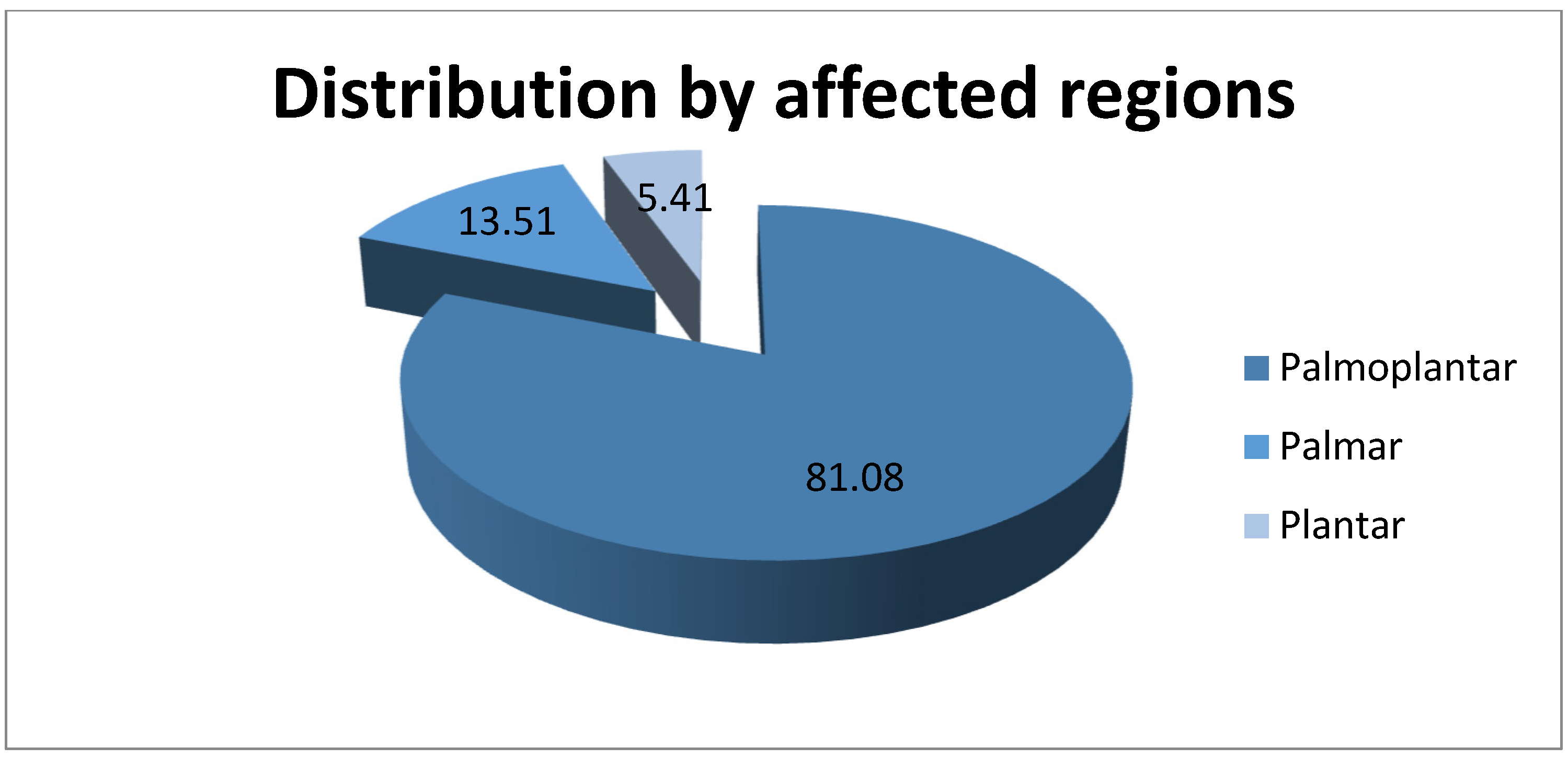
- Palmoplantar combination is the most frequent approach, followed by palmar and then plantar.
- The involvement of the genetic factor is supported in this study by the occurrence of excessive sweating in a family member in 54.10% of cases.
- Due to the approximately equal numbers among the urban and rural populations of Galati County, we can conclude that the significant difference between the number of patients from urban and rural areas, 89 and 22, respectively, is due to the easier access to medical services and therapeutic options for urban patients.
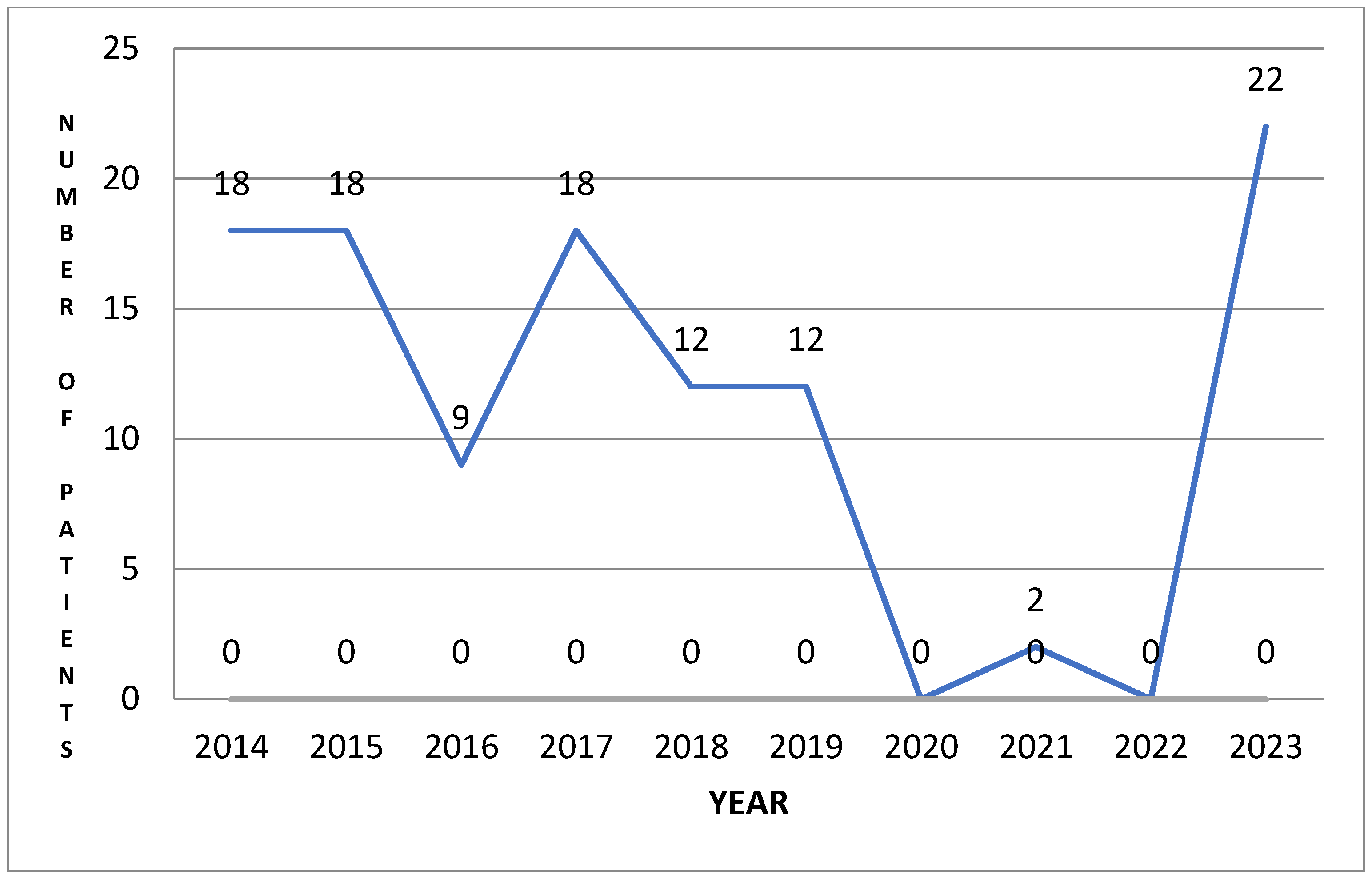
- An aspect that supports lack of knowledge of this disease, of therapeutic possibilities and of the important negative consequences on quality of life and the psyche of children discovered in this study is the drop to 0 in addressability during the COVID-19 pandemic, a period when priorities were different.
- Iontophoresis is effective in improving symptoms, and we will carry out future studies to highlight the improvement in quality of life based on valid questionnaires.
- Effective treatment, whether topical, systemic or invasive, should aim for optimization of patients’ quality of life.
- Before proceeding to permanent and possible irreversible surgical or invasive treatment, conservative therapies should be tried.
- Hyperhidrosis has a profound mental and physical impact on patients, which are under-diagnosed and undertreated, and it deserves as equal consideration as other more well-known skin problems.
- This study aims to raise the alarm about the need for awareness of this frequently underdiagnosed disease, which has serious mental and emotional consequences.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Krishan, P.; Adlar, T.; Potts, G. The impact of hyperhidrosis on quality of life: A review of the literature. Am. J. Clin. Dermatol. 2023, 24, 187–198. [Google Scholar]
- Shiri, N.; Jisun, C. The etiology, diagnosis, and management of hyperhidrosis: A comprehensive review: Therapeutic options. J. Am. Acad. Dermatol. 2019, 81, 657–666. [Google Scholar]
- Le Yan, H.; Fauzi, J.M.; Sotheenathan, K.; Basher, K.; Abdul, A. Diagnosis, impact and management of hyperhidrosis including endoscopic thoracic sympathectomy. J. Med. Malays. 2020, 75, 555–560. [Google Scholar]
- Shiri, N. Diagnosis and quantitative identification of hyperhidrosis. Shanhai Chest 2019, 3, 35. [Google Scholar]
- Lewis, S. Hyperhidrosis: Medical and surgical treatment. Eplasty 2008, 8, e22. [Google Scholar]
- William, L.; Edward, K.; Nowell, S.; Glaser, D.A. An epidemiological study of hyperhidrosis. Dermatol. Surg. 2007, 33, S69–S75. [Google Scholar]
- Ramalho, R.F.; Amante, M.H.; Roncada, R.H.; Cataneo, D.C. Palmar hyperhidrosis: Clinical, pathopsysiological, diagnostic and therapeutic aspects. An. Bras. Dermatol. 2016, 91, 716–725. [Google Scholar]
- Eisenach, J.; Atkinson, J.; Fealey, R. Hyperhidrosis: Evolving therapies for a well-established phenomenon. Mayo Clin. Proc. 2005, 80, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Karimian-Teherani, D.; Panhofer, P.; Ringhofer, C.; Jakesz, R.; Prager, M.; Zacherl, J.; Bischof, G.; Neumayer, C. New epidemiological aspects of patients with severe hyperhidrosis presenting for sympathetic surgery. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Worle, B.; Rapprich, S.; Heckmann, M. Definition and treatment of primary hyperhidrosis. JDDG J. Dtsch. Dermatol. Ges. 2007, 5, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Ro, K.; Cantor, R.; Lange, K.; Ahn, S. Palmar hyperhidrosis: Evidence of genetic transmission. J. Vasc. Surg. 2002, 35, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Hamm, H.; Naumann, M.; Kowalski, J.; Kutt, S.; Kozma, C.; Teale, C. Primary Focal Hyperhidrosis: Disease Characteristics and Functional Impairment. Dermatology 2006, 212, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Higashimoto, I.; Yoshiura, K.; Hirakawa, N.; Higashimoto, K.; Soejima, H.; Totoki, T.; Mukai, T.; Niikawa, N. Primary palmar hyperhidrosis locus maps to 14q11.2-q13. Am. J. Med. Genet. 2006, 140, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Lin, M.; Chen, X.; Cao, Z.; Tan, Z.; Xiong, W.; Tu, Y.; Yang, J. A novel locus for primary focal hyperhidrosis mapped on chromosome 2q31.1. Br. J. Dermatol. 2015, 172, 1150–1153. [Google Scholar] [CrossRef] [PubMed]
- Del Sorbo, F.; Brancati, F.; De Joanna, G.; Valente, E.M.; Lauria, G.; Albanese, A. Primary Focal Hyperhidrosis in a New Family Not Linked to Known Loci. Dermatology 2011, 223, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Solish, N.; Wang, R.; Murray, C. Evaluating the patient presenting with hyperhidrosis. Thorac. Surg. Clin. 2008, 18, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Jacob, C. Examining Hyperhidrosis:An Update on New Treatments. Am. J. Manag. Care 2018, 24, S496–S501. [Google Scholar] [PubMed]
- Solish, N.; Bertucci, V.; Dansereau, A.; Hong, C.H.; Lynde, C.; Lupin, M.; Smith, K.; Storwick, G. Canadian Hyperhidrosis Advisory Committee. A comprehensiveapproach to the recognition, diagnosis, and severity-based treatment of focal hyperhidrosis: Recommendationsof the Canadian Hyperhidrosis Advisory Committee. Dermatol. Surg. 2007, 33, 908–923. [Google Scholar] [PubMed]
- Schereth, T.; Dieterich, M.; Birklein, F. Hyperhidrosis—Causes and Treatmentof Enhanced Sweating. Dtsch. Arztebl. Int. 2009, 106, 32–37. [Google Scholar]
- Benson, R.A.; Palin, R.; Holt, P.J.E.; Loftus, I.M. Diagnosis and management of hyperhidrosis. BMJ 2013, 347, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Birner, P.; Heinzl, H.; Schindl, M.; Pumprla, J.; Schnider, P. Cardiac Autonomic Function in Patients Suffering from Primary Focal Hyperhidrosis. Eur. Neurol. 2000, 44, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Pariser, D.; Ballard, A. Topical therapies in hyperhidrosis care. Dermatol. Clin. 2014, 32, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Walling, H. Clinical differentiation of primary from secondary hyperhidrosis. J. Am. Acad. Dermatol. 2011, 64, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Kisielnicka, A.; Szczerkowska-Dobosz, A.; Purzycka-Bohdan, D.; Nowicki, R. Hyperhidrosis: Disease etiology, classification and management in the light of modern treatment modalities. Adv. Dermat. Allergol. 2022, XXXIX, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Moraites, E.; Vaughn, O.A.; Hill, S. Incidence and prevalence of hyperhidrosis. Dermatol. Clin. 2014, 32, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Rystedt, A.; Brismar, K.; Aquilonius, S.M.; Naver, H.; Swartling, C. Hyperhidrosis—An unknown widespread “silent” disorder. J. Neurol. Neuromedicine 2016, 1, 25–33. [Google Scholar]
- Gordon, J.; Hill, S. Update on pediatric hyperhidrosis. Dermatol. Ther. 2013, 26, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Vary, J. Selected Disorders of Skin Appendages-Acne, Alopecia, Hyperhidrosis. Med. Clin. N. Am. 2015, 99, 1195–1211. [Google Scholar] [CrossRef] [PubMed]
- Hornberge, J.; Grimes, K.; Naumann, M.; Glaser, D.A.; Lowe, N.; Naver, H.; Ahn, S.; Stolman, L. Recognition, diagnosis, and treatment of primary focal hyperhidrosis. J. Am. Acad. Dermatol. 2004, 51, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, A.I.; Mocanu, H.; Moldovan, C.; Soare, I.; Niculet, E.; Tatu, A.L.; Vasile, C.I.; Diculencu, D.; Postolache, P.A.; Nechifor, A. Some Manifestations of Tuberculosis in Otorhinolaryngology—Case Series and a Short Review of Related Data from South-Eastern Europe. Infect. Drug Resist. 2022, 15, 2753–2762. [Google Scholar] [CrossRef]
- Holzle, E. Pathophysiology of sweating. Curr. Probl. Dermatol. 2002, 30, 10–22. [Google Scholar]
- Sato, K.; Kang, W.; Saga, K.; Sato, K.T. Biology of sweat glands and their disorders. I. Normal sweat gland function. J. Am. Acad. Dermatol. 1989, 20, 537–563. [Google Scholar] [CrossRef] [PubMed]
- Heckmann, M.; Baumann-Ceballos, A.; Plewig, G. Botulinim Toxin A for axillary hyperhidrosis (excessive sweating). N. Engl. J. Med. 2001, 344, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Hund, M.; Kinkelin, I.; Naumann, M.; Hamm, H. Definition of axillary hyperhidrosis by gravimetric assessment. Arch. Dermatol. 2002, 138, 539–541. [Google Scholar] [CrossRef] [PubMed]
- Glogau, R. Treatment of palmar hyperhidrosis with botulinum Toxin. Semin. Cutan Med. Surg. 2001, 20, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Callejas, M.A.; Grimalt, R.; Cladellas, E. Hyperhidrosis update. Actas Dermosifiliogr. 2010, 101, 110–118. [Google Scholar] [CrossRef]
- Cohen, J.; Cohen, G.; Solish, N.; Murray, C. Diagnosis, Impact, and Management of Focal Hyperhidrosis: Treatment Review Including Botulinum Toxin Therapy. Facial Plast. Surg. Clin. N. Am. 2007, 15, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Sriraam, L.M.; Sundaram, R.; Ramalingam, R. Minor’s Test: Objective Demonstration of Horner’s Syndrome. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 190–192. [Google Scholar] [CrossRef] [PubMed]
- Hexsel, D.; Rodrigues, T.; Soirefmann, M.; Zechmeister-Prado, D. Recommendations for performing and evaluating the results of the minor test according to a sweating intensity visual scale. Dermatol. Surg. 2010, 36, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Nocivin, I.; Tiplica, G.S. Sinopsis de optiuniterapeutice in hiperhidroza—Synopsis of therapeutic options in hyperhidrosis. Derm. Venerol. 2018, 63, 49–66. [Google Scholar]
- Semkova, K.; Gergovska, M.; Kazandjieva, J.; Tfglassankov, N. Hyperhidrosis, bromhidrosis and chromhidrosis: Fold (intertriginous) dermatoses. Clin. Dermatol. 2015, 33, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Jicman Stan, D.; Sârbu, M.I.; Fotea, S.; Nechifor, A.; Bălan, G.; Anghele, M.; Vasile, C.I.; Niculeț, E.; Sârbu, N.; Rebegea, L.F.; et al. Oral Mucositis Induced by Chemoradiotherapy in Head and Neck Cancer-A Short Review about the Therapeutic Management and the Benefits of Bee Honey. Medicina 2022, 58, 751. [Google Scholar] [CrossRef]
- Atkins, J.; Butler, P. Hyperhidrosis: A review of current management. Plast. Reconst. Surg. 2002, 110, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Holzle, E. Topical pharmacological treatment. Curr. Probl. Dermatol. 2002, 30, 30–43. [Google Scholar]
- Togel, B.; Greve, B.; Raulin, C. Current therapeutic strategies for hyperhidrosis: A review. Eur. J. Dermatol. 2002, 12, 219–223. [Google Scholar] [PubMed]
- Murray, C.; Cohen, J.; Solish, N. Tratment of focal hyperhidrosis. J. Cutan. Med. Surg. 2007, 11, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Bohaty, B.; Hebert, A. Special considerations for children with hyperhidrosis. Dermatol. Clin. 2014, 32, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Glaser, D.A. Oral medications. Dermatol. Clin. 2014, 32, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Walling, H. Systemic therapy for primary hyperhidrosis: A retrospective study of 59 patients treated with glycopyrrolate or clonidine. J. Am. Acad. Dermatol. 2012, 66, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Webber, L. Hyperhidrosis. InnovAiT 2017, 10, 409–416. [Google Scholar] [CrossRef]
- Bobeica, C.; Niculet, E.; Tatu, A.L.; Craescu, M.; Vata, D.; Statescu, L.; Iancu, A.V.; Musat, C.L.; Draganescu, M.L.; Onisor, C.; et al. Old and new therapeutic strategies in systemic sclerosis. Exp. Ther. Med. 2022, 23, 134. [Google Scholar] [CrossRef] [PubMed]
- Nwabudike, L.C.; Tatu, A.L. Reply to Happle, R. et al. Koebner’s sheep in Wolf’s clothing: Does the isotopic response exist as a distinct phenomenon? J. Eur. Acad. Dermatol. Venereol. 2018, 32, e336–e337. [Google Scholar] [CrossRef] [PubMed]
- Brănișteanu, D.E.; Pintilie, A.; Dimitriu, A.; Cerbu, A.; Ciobanu, D.; Oanţă, A.; Tatu, A.L. Clinical, laboratory and therapeutic profile of lichen planus. Med.-Surg. J. 2017, 121, 25–32. [Google Scholar]
- Nwabudike, L.C.; Tatu, A.L. Reply to Gambichler T et al.: Altered epigenetic pathways and cell cycle dysregulation in healthy appearing skin of patients with koebnerized squamous cell carcinomas following skin surgery. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e3–e4. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.; Bachoo, P.; Holmes, J. Botulinum toxin type B: A new therapy for axillary hyperhidrosis. Br. J. Plast. Surg. 2005, 58, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Gregoriou, S.; Sidiropoulou, P.; Kontochristopoulos, G.; Rigopoulos, D. Management strategies of palmar hyperhidrosis: Challenges and solutions. Clin. Cosmet. Investig. Dermatol. 2019, 12, 733–744. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Profile | n = 111 (%) | |
|---|---|---|
| Age | ||
| 6–8 | 30 (27.03%) | |
| 9–11 | 43 (38.73%) | |
| 12–14 | 30 (27.03%) | |
| 15–17 | 8 (7.21%) | |
| Sex | ||
| Girls | 67 (60.36%) | |
| Boys | 44 (39.64%) | |
| Environment | ||
| Urban | 89 (80.18%) | |
| Rural | 22 (19.82%) | |
| Site of involvement | ||
| Palmoplantar | 90 (81.08%) | |
| Palmar | 15 (13.51%) | |
| Plantar | 6 (5.14%) | |
| Family history | ||
| Yes | 60 (54.10%) | |
| No | 51 (45.90%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nastase, F.; Verenca, M.C.; Niculet, E.; Radaschin, D.S.; Busila, C.; Vasile, C.I.; Tatu, A.L. Primary Hyperhidrosis in Children—A Retrospective Study and a Short Review. Life 2024, 14, 645. https://doi.org/10.3390/life14050645
Nastase F, Verenca MC, Niculet E, Radaschin DS, Busila C, Vasile CI, Tatu AL. Primary Hyperhidrosis in Children—A Retrospective Study and a Short Review. Life. 2024; 14(5):645. https://doi.org/10.3390/life14050645
Chicago/Turabian StyleNastase, Florentina, Madalina Codruta Verenca, Elena Niculet, Diana Sabina Radaschin, Camelia Busila, Claudiu Ionut Vasile, and Alin Laurentiu Tatu. 2024. "Primary Hyperhidrosis in Children—A Retrospective Study and a Short Review" Life 14, no. 5: 645. https://doi.org/10.3390/life14050645
APA StyleNastase, F., Verenca, M. C., Niculet, E., Radaschin, D. S., Busila, C., Vasile, C. I., & Tatu, A. L. (2024). Primary Hyperhidrosis in Children—A Retrospective Study and a Short Review. Life, 14(5), 645. https://doi.org/10.3390/life14050645