

Risk of Atrial Fibrillation in Patients with Different Cancer Types in Taiwan

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Ethics Statement
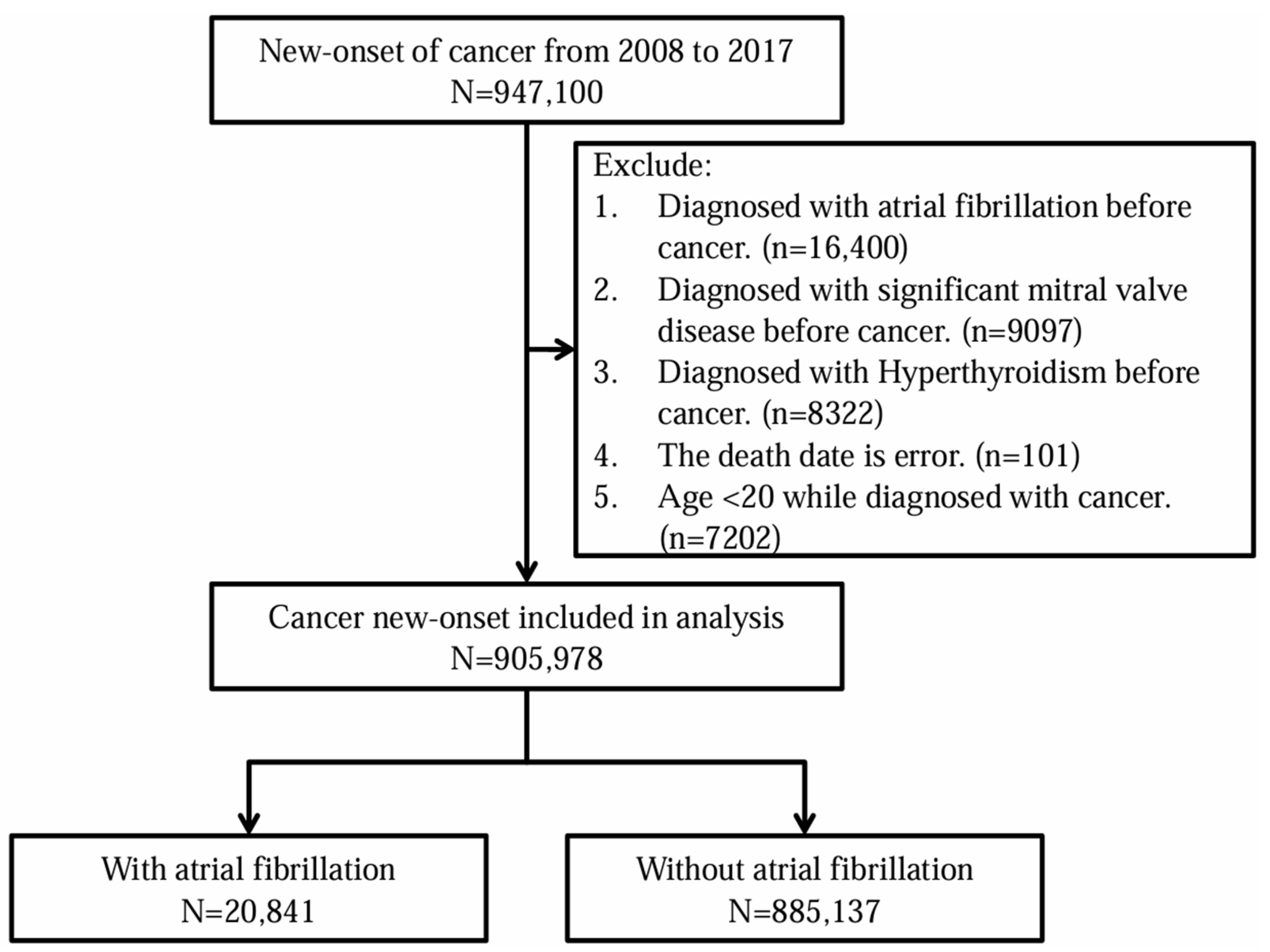
2.3. Study Participants and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Risk of AF in Cancer Patients
3.3. Incidence of AF in Different Types of Cancer
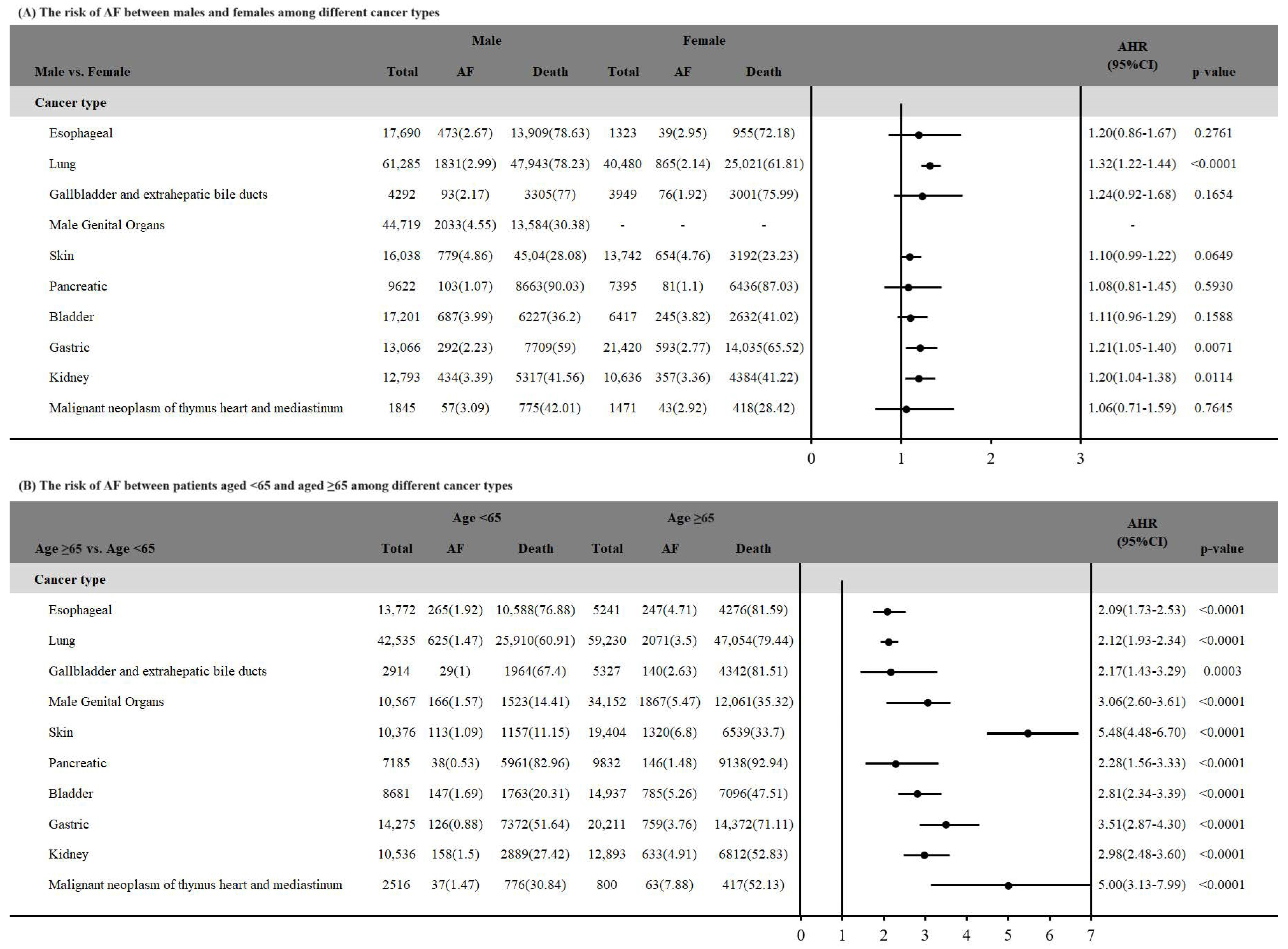
3.4. Incidence of AF in Different Types of Cancer Stratified by Sex
3.5. Incidence of AF in Patients with Different Types of Cancer Stratified by Age
4. Discussion
4.1. Limitations
4.2. Strengths
4.3. Prospective Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chu, G.; Versteeg, H.H.; Verschoor, A.J.; Trines, S.A.; Hemels, M.E.W.; Ay, C.; Huisman, M.V.; Klok, F.A. Atrial fibrillation and cancer—An unexplored field in cardiovascular oncology. Blood Rev. 2019, 35, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Ording, A.G.; Horváth-Puhó, E.; Adelborg, K.; Pedersen, L.; Prandoni, P.; Sørensen, H.T. Thromboembolic and bleeding complications during oral anticoagulation therapy in cancer patients with atrial fibrillation: A Danish nationwide population-based cohort study. Cancer Med. 2017, 6, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Vedovati, M.C.; Giustozzi, M.; Verdecchia, P.; Pierpaoli, L.; Conti, S.; Verso, M.; Di Filippo, F.; Marchesini, E.; Bogliari, G.; Agnelli, G.; et al. Patients with cancer and atrial fibrillation treated with doacs: A prospective cohort study. Int. J. Cardiol. 2018, 269, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, L.A.; Fonseca, S.M.R.; Machado, T.I.V. Atrial fibrillation and cancer. Front. Cardiovasc. Med. 2021, 8, 590768. [Google Scholar] [CrossRef]
- Ostenfeld, E.B.; Erichsen, R.; Pedersen, L.; Farkas, D.K.; Weiss, N.S.; Sørensen, H.T. Atrial fibrillation as a marker of occult cancer. PLoS ONE 2014, 9, e102861. [Google Scholar] [CrossRef] [PubMed]
- Erichsen, R.; Christiansen, C.F.; Mehnert, F.; Weiss, N.S.; Baron, J.A.; Sørensen, H.T. Colorectal cancer and risk of atrial fibrillation and flutter: A population-based case-control study. Intern. Emerg. Med. 2012, 7, 431–438. [Google Scholar] [CrossRef]
- Guzzetti, S.; Costantino, G.; Vernocchi, A.; Sada, S.; Fundarò, C. First diagnosis of colorectal or breast cancer and prevalence of atrial fibrillation. Intern. Emerg. Med. 2008, 3, 227–231. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, M.; Smedegaard, L.; Madelaire, C.; Nielsen, D.; Torp-Pedersen, C.; Gislason, G.; Schou, M.; Fosbøl, E. Incidence of atrial fibrillation in conjunction with breast cancer. Heart Rhythm. 2019, 16, 343–348. [Google Scholar] [CrossRef]
- Jakobsen, C.B.; Lamberts, M.; Carlson, N.; Lock-Hansen, M.; Torp-Pedersen, C.; Gislason, G.H.; Schou, M. Incidence of atrial fibrillation in different major cancer subtypes: A Nationwide population-based 12 year follow up study. BMC Cancer 2019, 19, 1105. [Google Scholar] [CrossRef]
- Guha, A.; Fradley, M.G.; Dent, S.F.; Weintraub, N.L.; Lustberg, M.B.; Alonso, A.; Addison, D. Incidence, risk factors, and mortality of atrial fibrillation in breast cancer: A SEER-Medicare analysis. Eur. Heart J. 2022, 43, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Zhang, Z.; Tse, G.; Feng, X.; Korantzopoulos, P.; Letsas, K.P.; Yan, B.P.; Wu, W.K.K.; Zhang, H.; Li, G.; et al. Association of Cancer and the Risk of Developing Atrial Fibrillation: A Systematic Review and Meta-Analysis. Cardiol. Res. Pract. 2019, 2019, 8985273. [Google Scholar] [CrossRef]
- Menichelli, D.; Vicario, T.; Ameri, P.; Toma, M.; Violi, F.; Pignatelli, P.; Pastori, D. Cancer and atrial fibrillation: Epidemiology, mechanisms, and anticoagulation treatment. Prog. Cardiovasc. Dis. 2021, 66, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.P.; Choi, E.K.; Han, K.D.; Park, S.H.; Jung, J.H.; Park, S.H.; Ahn, H.J.; Lim, J.H.; Lee, S.R.; Oh, S. Risk of Atrial Fibrillation According to Cancer Type: A Nationwide Population-Based Study. JACC CardioOncology 2021, 3, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.-J.; Wang, Y.-W.; Lee, W.-C. Taiwan’s nationwide cancer registry system of 40 years: Past, present, and future. J. Formos. Med. Assoc. 2019, 118, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.-Y.; Su, C.-C.; Shao, S.-C.; Sung, S.-F.; Lin, S.-J.; Kao Yang, Y.-H.; Lai, E.C.-C. Taiwan’s national health insurance research database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Farmakis, D.; Parissis, J.; Filippatos, G. Insights into onco-cardiology: Atrial fibrillation in cancer. J. Am. Coll. Cardiol. 2014, 63, 945–953. [Google Scholar] [CrossRef]
- Hu, Y.-F.; Chen, Y.-J.; Lin, Y.-J.; Chen, S.-A. Inflammation and the pathogenesis of atrial fibrillation. Nat. Rev. Cardiol. 2015, 12, 230–243. [Google Scholar] [CrossRef]
- Carlisle, M.A.; Fudim, M.; DeVore, A.D.; Piccini, J.P. Heart failure and atrial fibrillation, like fire and fury. JACC Heart Fail. 2019, 7, 447–456. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, W.T.; Lakoski, S.G.; Qureshi, W.; Judd, S.E.; Howard, G.; Howard, V.J.; Cushman, M.; Soliman, E.Z. Relation between cancer and atrial fibrillation (from the REasons for Geographic And Racial Differences in Stroke Study). Am. J. Cardiol. 2015, 115, 1090–1094. [Google Scholar] [CrossRef]
- Ay, C.; Grilz, E.; Nopp, S.; Moik, F.; Königsbrügge, O.; Klimek, P.; Thurner, S.; Posch, F.; Pabinger, I. Atrial fibrillation and cancer: Prevalence and relative risk from a nationwide study. Res. Pract. Thromb. Haemost. 2023, 7, 100026. [Google Scholar] [CrossRef]
- Zubair Khan, M.; Gupta, A.; Patel, K.; Abraham, A.; Franklin, S.; Kim, D.Y.; Patel, K.; Hussian, I.; Zarak, M.S.; Figueredo, V.; et al. Association of atrial fibrillation and various cancer subtypes. J. Arrhythm. 2021, 37, 1205–1214. [Google Scholar] [CrossRef]
- Lopez-Fernandez, T.; Martin-Garcia, A.; Rabadán, I.R.; Mitroi, C.; Ramos, P.M.; Diez-Villanueva, P.; Cervantes, C.E.; Martín, C.A.; Salinas, G.L.A.; Arenas, M. Atrial fibrillation in active cancer patients: Expert position paper and recommendations. Rev. Española Cardiol. 2019, 72, 749–759. [Google Scholar] [CrossRef]
- Tsai, Y.-W.; Tsai, T.-I.; Yang, C.-L.; Kuo, K.N. Gender differences in smoking behaviors in an Asian population. J. Women’s Health 2008, 17, 971–978. [Google Scholar] [CrossRef]
- Wang, L.-J.; Lin, C.-L.; Chen, Y.-C.; Lin, C.; Shyu, Y.-C.; Chen, C.-K. Sex Differences in the Relationship between Excessive Alcohol Consumption and Metabolic Abnormalities: A Community-Based Study in Taiwan. Nutrients 2022, 14, 2957. [Google Scholar] [CrossRef]
- Jeong, S.-M.; Jeon, K.H.; Shin, D.W.; Han, K.; Kim, D.; Park, S.H.; Cho, M.H.; Lee, C.M.; Nam, K.-W.; Lee, S.P. Smoking cessation, but not reduction, reduces cardiovascular disease incidence. Eur. Heart J. 2021, 42, 4141–4153. [Google Scholar] [CrossRef]
- Giannopoulos, G.; Anagnostopoulos, I.; Kousta, M.; Vergopoulos, S.; Deftereos, S.; Vassilikos, V. Alcohol consumption and the risk of incident atrial fibrillation: A meta-analysis. Diagnostics 2022, 12, 479. [Google Scholar] [CrossRef]
- Chang, Y.-T.; Chen, Y.-L.; Kang, H.-Y. Revealing the influences of sex hormones and sex differences in atrial fibrillation and vascular cognitive impairment. Int. J. Mol. Sci. 2021, 22, 8776. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Sun, L.; Burstein, D.S.; Getz, K.D. Considerations of Competing Risks Analysis in Cardio-Oncology Studies: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncology 2022, 4, 287–301. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Koulaouzidis, A.; Marlicz, W.; Lok, V.; Chu, C.; Ngai, C.H.; Zhang, L.; Chen, P.; Wang, S.; Yuan, J. Global burden, risk factors, and trends of esophageal cancer: An analysis of cancer registries from 48 countries. Cancers 2021, 13, 141. [Google Scholar] [CrossRef]
- Tsai, M.-C.; Chou, Y.-C.; Lee, Y.-K.; Hsu, W.-L.; Tang, C.-S.; Chen, S.-Y.; Huang, S.-P.; Chen, Y.-C.; Lee, J.-M. Secular Trends in Incidence of Esophageal Cancer in Taiwan from 1985 to 2019: An Age-Period-Cohort Analysis. Cancers 2022, 14, 5844. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Lee, J.M.; Wu, D.C.; Hsu, H.K.; Kao, E.L.; Huang, H.L.; Wang, T.N.; Huang, M.C.; Wu, M.T. Independent and combined effects of alcohol intake, tobacco smoking and betel quid chewing on the risk of esophageal cancer in Taiwan. Int. J. Cancer 2005, 113, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, A.; Obi, K.O.; Rubenstein, J.H. The synergistic effects of alcohol and tobacco consumption on the risk of esophageal squamous cell carcinoma: A meta-analysis. Off. J. Am. Coll. Gastroenterol. ACG 2014, 109, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; van Rein, N.; van der Hulle, T.; Heemelaar, J.C.; Trines, S.A.; Versteeg, H.H.; Klok, F.A.; Cannegieter, S.C. Coexisting atrial fibrillation and cancer: Time trends and associations with mortality in a nationwide Dutch study. Eur. Heart J. 2024, ehae222. [Google Scholar] [CrossRef] [PubMed]
- Conen, D.; Wong, J.A.; Sandhu, R.K.; Cook, N.R.; Lee, I.-M.; Buring, J.E.; Albert, C.M. Risk of malignant cancer among women with new-onset atrial fibrillation. JAMA Cardiol. 2016, 1, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Aliot, E.; Botto, G.L.; Crijns, H.J.; Kirchhof, P. Quality of life in patients with atrial fibrillation: How to assess it and how to improve it. Europace 2014, 16, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Thrall, G.; Lane, D.; Carroll, D.; Lip, G.Y. Quality of life in patients with atrial fibrillation: A systematic review. Am. J. Med. 2006, 119, 448.e1–448.e19. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.-J.; You, S.-L.; Chen, C.-J.; Yang, Y.-W.; Lo, W.-C.; Lai, M.-S. Quality assessment and improvement of nationwide cancer registration system in Taiwan: A review. Jpn. J. Clin. Oncol. 2015, 45, 291–296. [Google Scholar] [CrossRef]
- Lin, L.J.; Cheng, M.H.; Lee, C.H.; Wung, D.C.; Cheng, C.L.; Kao Yang, Y.H. Compliance with antithrombotic prescribing guidelines for patients with atrial fibrillation--a nationwide descriptive study in Taiwan. Clin. Ther. 2008, 30, 1726–1736. [Google Scholar] [CrossRef]
- Chang, C.H.; Lee, Y.C.; Tsai, C.T.; Chang, S.N.; Chung, Y.H.; Lin, M.S.; Lin, J.W.; Lai, M.S. Continuation of statin therapy and a decreased risk of atrial fibrillation/flutter in patients with and without chronic kidney disease. Atherosclerosis 2014, 232, 224–230. [Google Scholar] [CrossRef]
- Chao, T.F.; Liu, C.J.; Chen, S.J.; Wang, K.L.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Chen, T.J.; et al. Does digoxin increase the risk of ischemic stroke and mortality in atrial fibrillation? A nationwide population-based cohort study. Can. J. Cardiol. 2014, 30, 1190–1195. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Overall (N = 905,978) | With Atrial Fibrillation (N = 20,841) | Without Atrial Fibrillation (N = 885,137) | p Value | |
|---|---|---|---|---|
| Age, years (mean ± SD) | 61.46 ± 14.90 | 72.54 ± 10.89 | 61.20 ± 14.89 | <0.0001 |
| Age stratification (%) | ||||
| <65 | 520,914 (57.50) | 4786 (22.96) | 516,128 (58.31) | <0.0001 |
| ≥65 | 385,064 (42.50) | 16,055 (77.04) | 369,009 (41.69) | |
| Sex (%) | ||||
| Male | 473,855 (52.30) | 13,051 (62.62) | 460,804 (52.06) | <0.0001 |
| Female | 432,123 (47.70) | 7790 (37.38) | 424,333 (47.94) | |
| Comorbidities (%) | ||||
| Hypertension | 327,009 (36.09) | 12,326 (59.14) | 314,683 (35.55) | <0.0001 |
| Diabetes mellitus | 172,174 (19.00) | 5366 (25.75) | 166,808 (18.85) | <0.0001 |
| Stroke | 65,119 (7.19) | 2694 (12.93) | 62,425 (7.05) | <0.0001 |
| PAOD | 15,785 (1.74) | 687 (3.30) | 15,098 (1.71) | <0.0001 |
| Heart failure | 33,594 (3.71) | 2335 (11.20) | 31,259 (3.53) | <0.0001 |
| Myocardial infarction | 7486 (0.83) | 348 (1.67) | 7138 (0.81) | <0.0001 |
| ESRD | 3176 (0.35) | 81 (0.39) | 3095 (0.35) | 0.3465 |
| Death | 405,115 (44.72) | 11,727 (56.27) | 393,388 (44.44) | <0.0001 |
| Characteristics | Patients | Event of AF | PYs | Incidence Rate | Crude HR (95% C.I.) | p | Adjusted HR (95% C.I.) | p |
|---|---|---|---|---|---|---|---|---|
| Overall | 905,978 | 20,841 (2.3) | 3,241,527 | 64.29 | - | - | ||
| Age | ||||||||
| <65 | 520,914 | 4786 (22.96) | 2,169,483.20 | 22.06 | Ref. | Ref. | ||
| ≥65 | 385,064 | 16,055 (77.04) | 1,072,043.80 | 149.76 | 6.33 (6.13–6.54) | <0.0001 | 4.67 (4.51–4.84) | <0.0001 |
| Sex | ||||||||
| Male | 473,855 | 13,051 (2.75) | 1,467,721.58 | 88.92 | 1.90 (1.85–1.96) | <0.0001 | 1.50 (1.46–1.54) | <0.0001 |
| Female | 432,123 | 7790 (1.80) | 1,773,805.42 | 43.92 | Ref. | Ref. | ||
| Comorbidities | ||||||||
| Hypertension | ||||||||
| Yes | 327,009 | 12,326 (3.77) | 1,017,778.61 | 121.11 | 3.03 (2.94–3.11) | <0.0001 | 1.57 (1.52–1.62) | <0.0001 |
| No | 578,969 | 8515 (1.47) | 2,223,748.39 | 38.29 | Ref. | Ref. | ||
| Diabetes mellitus | 9 | |||||||
| Yes | 172,174 | 5366 (3.12) | 502,778.54 | 106.73 | 1.78 (1.73–1.84) | <0.0001 | 1.02 (0.99–1.06) | 0.1423 |
| No | 733,804 | 15,475 (2.11) | 2,738,748.47 | 56.5 | Ref. | Ref. | ||
| Myocardial infarction | ||||||||
| Yes | 7486 | 348 (4.65) | 17,420.19 | 199.77 | 2.83 (2.55–3.15) | <0.0001 | 1.26 (1.13–1.40) | <0.0001 |
| No | 898,492 | 20,493 (2.28) | 3,224,106.81 | 63.56 | Ref. | Ref. | ||
| Stroke | ||||||||
| Yes | 65,119 | 2694 (4.14) | 158,914.73 | 169.52 | 2.62 (2.52–2.73) | <0.0001 | 1.19 (1.14–1.24) | <0.0001 |
| No | 840,859 | 18,147 (2.16) | 3,082,612.27 | 58.87 | Ref. | Ref. | ||
| PAOD | ||||||||
| Yes | 15,785 | 687 (4.35) | 43,905.58 | 156.47 | 2.34 (2.17–2.52) | <0.0001 | 1.22 (1.13–1.31) | <0.0001 |
| No | 890,193 | 20,154 (2.26) | 3,197,621.42 | 63.03 | Ref. | Ref. | ||
| Heart failure | ||||||||
| Yes | 33,594 | 2335 (6.95) | 77,674.41 | 300.61 | 4.65 (4.45–4.85) | <0.0001 | 2.31 (2.21–2.42) | <0.0001 |
| No | 872,384 | 18,506 (2.12) | 3,163,852.59 | 58.49 | Ref. | Ref. | ||
| ESRD | ||||||||
| Yes | 3176 | 81 (2.55) | 4084.2 | 198.33 | 2.13 (1.71–2.65) | <0.0001 | 1.31 (1.05–1.63) | 0.0159 |
| No | 902,802 | 20,760 (2.30) | 3,237,442.8 | 64.12 | Ref. | Ref. |
| Cancer Type | Patients | With AF | Without AF | PYs | Incidence Rate |
|---|---|---|---|---|---|
| Esophageal | 19,013 | 512 (2.69) | 18,501 (97.31) | 32,833.31 | 155.94 |
| Lung | 101,765 | 2696 (2.65) | 99,069 (97.35) | 196,536.87 | 137.18 |
| Gallbladder and extrahepatic bile ducts | 8241 | 169 (2.05) | 8072 (97.95) | 15,632.73 | 108.11 |
| Male genital organs | 44,720 | 2033 (4.55) | 42,687 (95.45) | 190,265.33 | 106.85 |
| Skin | 29,780 | 1433 (4.81) | 28,347 (95.19) | 134,729.49 | 106.36 |
| Pancreatic | 17,017 | 184 (1.08) | 16,833 (98.92) | 17,428.05 | 105.58 |
| Bladder | 23,618 | 932 (3.95) | 22,686 (96.05) | 95,376.87 | 97.72 |
| Gastric | 34,486 | 885 (2.57) | 33,601 (97.43) | 94,212.39 | 93.94 |
| Kidney | 23,429 | 791 (3.38) | 22,638 (96.62) | 87,304.02 | 90.6 |
| Malignant neoplasm of thymus heart and mediastinum | 3316 | 100 (3.02) | 3216 (96.98) | 12,096.85 | 82.67 |
| Liver | 101,273 | 1920 (1.9) | 99,353 (98.1) | 236,491.44 | 81.19 |
| Colorectal | 137,841 | 3976 (2.88) | 133,865 (97.12) | 526,792.81 | 75.48 |
| Malignant neoplasm of connective and other soft tissue | 4594 | 122 (2.66) | 4472 (97.34) | 17,665.49 | 69.06 |
| Small intestine | 3566 | 82 (2.3) | 3484 (97.7) | 12,087.33 | 67.84 |
| Peritoneum | 1634 | 25 (1.53) | 1609 (98.47) | 4651.76 | 53.74 |
| Eye | 771 | 19 (2.46) | 752 (97.54) | 3730.35 | 50.93 |
| CNS cancer | 6916 | 94 (1.36) | 6822 (98.64) | 18,637.03 | 50.44 |
| Head and neck | 84,313 | 1381 (1.64) | 82,932 (98.36) | 333,474.91 | 41.41 |
| Bone | 1116 | 18 (1.61) | 1098 (98.39) | 4490.1 | 40.09 |
| Breast | 115,996 | 1269 (1.09) | 114,727 (98.91) | 581,233.59 | 21.83 |
| Gynecologic | 74,669 | 820 (1.1) | 73,849 (98.9) | 383,875 | 21.36 |
| Thyroid | 25,160 | 263 (1.05) | 24,897 (98.95) | 128,149.54 | 20.52 |
| Others | 42,745 | 1117 (2.61) | 41,628 (97.39) | 113,838 | 98.12 |
| Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|
| Cancer Type | Patients | With AF | PYs | Incidence Rate | Patients | With AF | PYs | Incidence Rate |
| Lung | 61,285 | 1831 (2.99) | 98,963.86 | 185.02 | 40,480 | 865 (2.14) | 97,573.01 | 88.65 |
| Esophageal | 17,690 | 473 (2.67) | 30,238.53 | 156.42 | 1323 | 39 (2.95) | 2594.78 | 150.3 |
| Gallbladder and extrahepatic bile ducts | 4292 | 93 (2.17) | 7956.93 | 116.88 | 3949 | 76 (1.92) | 7675.8 | 99.01 |
| Pancreatic | 9622 | 103 (1.07) | 9300.22 | 110.75 | 7395 | 81 (1.1) | 8127.83 | 99.66 |
| Skin | 16,038 | 779 (4.86) | 70,761.82 | 110.09 | 13,742 | 654 (4.76) | 63,967.66 | 102.24 |
| Breast | 443 | 21 (4.74) | 1936.13 | 108.46 | 115,553 | 1248 (1.08) | 579,297.45 | 21.54 |
| Male genital organs | 44,719 | 2033 (4.55) | 190,259.08 | 106.85 | - | - | - | - |
| Gastric | 21,420 | 593 (2.77) | 55,531.75 | 106.79 | 13,066 | 292 (2.23) | 38,680.64 | 75.49 |
| Bladder | 17,201 | 687 (3.99) | 70,660.26 | 97.23 | 6417 | 245 (3.82) | 24,716.61 | 99.12 |
| Peritoneum | 672 | 17 (2.53) | 1843.59 | 92.21 | 962 | 8 (0.83) | 2808.18 | 28.49 |
| Malignant neoplasm of thymus heart and mediastinum | 1845 | 57 (3.09) | 6190.35 | 92.08 | 1471 | 43 (2.92) | 5906.5 | 72.8 |
| Kidney | 12,793 | 434 (3.39) | 47,401.71 | 91.56 | 10,636 | 357 (3.36) | 39,902.31 | 89.47 |
| Connective and other soft tissue | 2679 | 83 (3.1) | 10,055.64 | 82.54 | 1915 | 39 (2.04) | 7609.85 | 51.25 |
| Colorectal | 80,750 | 2507 (3.1) | 304,351.01 | 82.37 | 57,091 | 1469 (2.57) | 222,441.81 | 66.04 |
| Small intestine | 2116 | 54 (2.55) | 6901.49 | 78.24 | 1450 | 28 (1.93) | 5185.83 | 53.99 |
| Liver | 71,332 | 1251 (1.75) | 164,903.71 | 75.86 | 29,941 | 669 (2.23) | 71,587.74 | 93.45 |
| Eye | 403 | 12 (2.98) | 1920.63 | 62.48 | 368 | 7 (1.9) | 1809.71 | 38.68 |
| CNS cancer | 3862 | 46 (1.19) | 9904.06 | 46.45 | 3054 | 48 (1.57) | 8732.98 | 54.96 |
| Head and neck | 73,100 | 1192 (1.63) | 284,135.66 | 41.95 | 11,213 | 189 (1.69) | 49,339.26 | 38.31 |
| Bone | 633 | 9 (1.42) | 2513.75 | 35.8 | 483 | 9 (1.86) | 1976.35 | 45.54 |
| Thyroid | 6055 | 92 (1.52) | 29,120.33 | 31.59 | 19,105 | 171 (0.9) | 99,029.21 | 17.27 |
| Gynecologic | 0 | 0 (0) | 0 | 0 | 74,669 | 820 (1.1) | 383,875 | 21.36 |
| Others | 24,905 | 684 (2.75) | 62,871.08 | 108.79 | 17,840 | 433 (2.43) | 50,966.92 | 84.96 |
| <65 | ≥65 | |||||||
|---|---|---|---|---|---|---|---|---|
| Cancer Type | Patients | With AF | PYs | Incidence Rate | Patients | With AF | PYs | Incidence Rate |
| Esophageal | 13,772 | 265 (1.92) | 25,392.91 | 104.36 | 5241 | 247 (4.71) | 7440.41 | 331.97 |
| Lung | 42,535 | 625 (1.47) | 107,103.09 | 58.35 | 59,230 | 2071 (3.5) | 89,433.78 | 231.57 |
| Gallbladder and extrahepatic bile ducts | 2914 | 29 (1.00) | 7363.95 | 39.38 | 5327 | 140 (2.63) | 8268.78 | 169.31 |
| Pancreatic | 7185 | 38 (0.53) | 10,066.16 | 37.75 | 9832 | 146 (1.48) | 7361.89 | 198.32 |
| Malignant neoplasm of thymus heart and mediastinum | 2516 | 37 (1.47) | 10,048.92 | 36.82 | 800 | 63 (7.88) | 2047.93 | 307.63 |
| Bladder | 8681 | 147 (1.69) | 42,650.85 | 34.47 | 14,937 | 785 (5.26) | 52,726.03 | 148.88 |
| Kidney | 10,536 | 158 (1.50) | 46,672.57 | 33.85 | 12,893 | 633 (4.91) | 40,631.45 | 155.79 |
| Liver | 50,358 | 444 (0.88) | 133,665.53 | 33.22 | 50,915 | 1476 (2.90) | 102,825.92 | 143.54 |
| Male genital organs | 10,567 | 166 (1.57) | 51,015.16 | 32.54 | 34,152 | 1867 (5.47) | 139,243.91 | 134.08 |
| Bone | 862.00 | 11 (1.28) | 3821.1 | 28.79 | 254 | 7 (2.76) | 669.00 | 104.63 |
| Gastric | 14,275 | 126 (0.88) | 48,919.06 | 25.76 | 20,211 | 759 (3.76) | 45,293.33 | 167.57 |
| Small intestine | 1907 | 20 (1.05) | 7846.47 | 25.49 | 1659 | 62 (3.74) | 4240.86 | 146.20 |
| Connective and other soft tissue | 2959 | 33 (1.12) | 12,990.8 | 25.4 | 1635 | 89 (5.44) | 4674.69 | 190.39 |
| Colorectal | 68,253 | 740 (1.08) | 293,692.62 | 25.2 | 69,588 | 3236 (4.65) | 233,100.19 | 138.82 |
| Head and neck | 66,490 | 658 (0.99) | 277,514.73 | 23.71 | 17,823 | 723 (4.06) | 55,960.18 | 129.20 |
| CNS cancer | 4649 | 33 (0.71) | 15,282.01 | 21.59 | 2267 | 61 (2.69) | 3355.03 | 181.82 |
| Skin | 10,376 | 113 (1.09) | 54,561.16 | 20.71 | 19,404 | 1320 (6.8) | 80,168.33 | 164.65 |
| Peritoneum | 1040 | 6 (0.58) | 3521.02 | 17.04 | 594 | 19 (3.20) | 1130.75 | 168.03 |
| Eye | 468 | 3 (0.64) | 2376.56 | 12.62 | 303 | 16 (5.28) | 1353.79 | 118.19 |
| Thyroid | 22,002 | 114 (0.52) | 115,765.6 | 9.85 | 3158 | 149 (4.72) | 12,383.93 | 120.32 |
| Breast | 95,018 | 473 (0.50) | 490,987.65 | 9.63 | 20,978 | 796 (3.79) | 90,245.93 | 88.20 |
| Gynecologic | 61,535 | 272 (0.44) | 330,285.3 | 8.24 | 13,134 | 548 (4.17) | 53,589.7 | 102.26 |
| Others | 22,016 | 275 (1.25) | 77,940.01 | 35.28 | 20,729 | 842 (4.06) | 35,898 | 234.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, K.-M.; Yu, C.-H.; Wu, Y.-C.; Wang, J.-J.; Liang, F.-W.; Ho, C.-H. Risk of Atrial Fibrillation in Patients with Different Cancer Types in Taiwan. Life 2024, 14, 621. https://doi.org/10.3390/life14050621
Liao K-M, Yu C-H, Wu Y-C, Wang J-J, Liang F-W, Ho C-H. Risk of Atrial Fibrillation in Patients with Different Cancer Types in Taiwan. Life. 2024; 14(5):621. https://doi.org/10.3390/life14050621
Chicago/Turabian StyleLiao, Kuang-Ming, Chia-Hung Yu, Yu-Cih Wu, Jhi-Joung Wang, Fu-Wen Liang, and Chung-Han Ho. 2024. "Risk of Atrial Fibrillation in Patients with Different Cancer Types in Taiwan" Life 14, no. 5: 621. https://doi.org/10.3390/life14050621
APA StyleLiao, K.-M., Yu, C.-H., Wu, Y.-C., Wang, J.-J., Liang, F.-W., & Ho, C.-H. (2024). Risk of Atrial Fibrillation in Patients with Different Cancer Types in Taiwan. Life, 14(5), 621. https://doi.org/10.3390/life14050621