
The Use of Pre-Endoscopic Metoclopramide Does Not Prevent the Need for Repeat Endoscopy: A U.S. Based Retrospective Cohort Study

 ,
, 
Abstract
1. Introduction
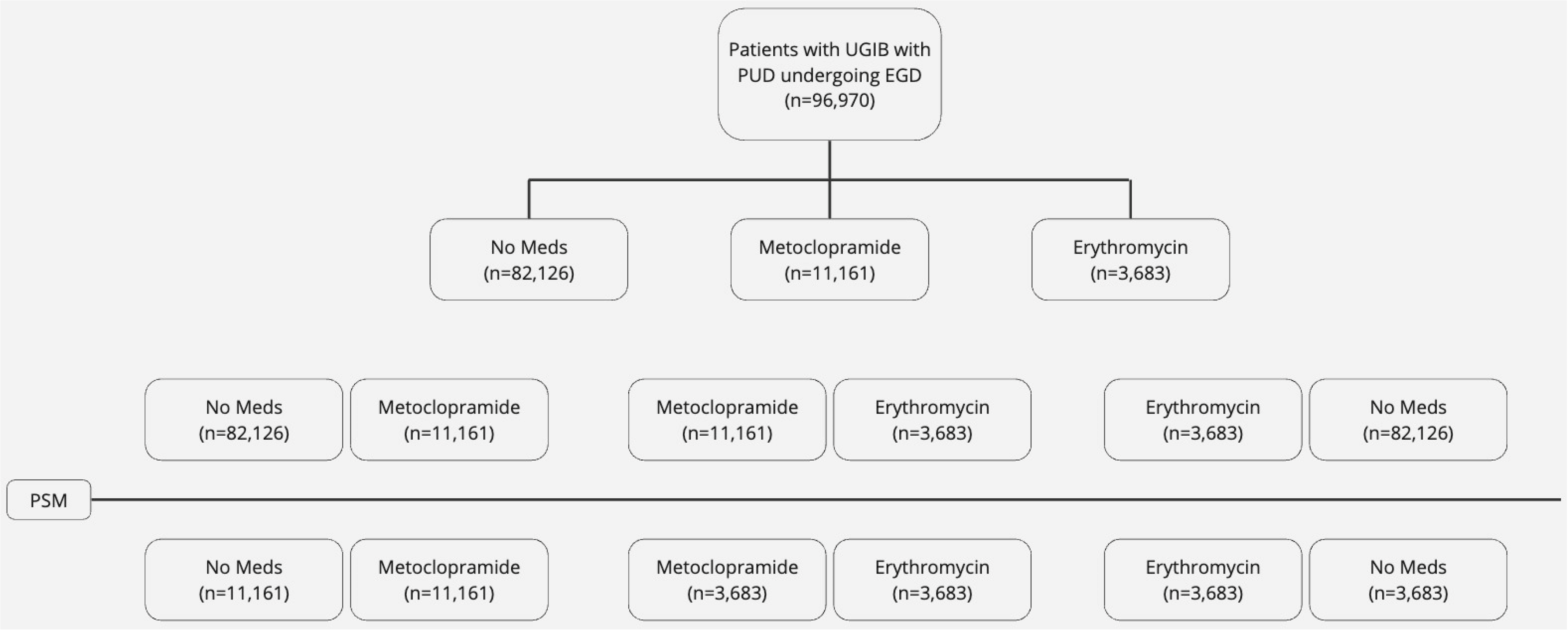
2. Materials and Methods
2.1. Statistical Analysis
2.2. Inclusion and Exclusion Criteria
3. Results
3.1. Baseline Characteristics
3.2. Outcomes
4. Discussion
4.1. Concept
4.2. Normal Gastric Physiology and Dynamics
4.3. Background
4.4. Medication under Study: Erythromycin
4.5. Medication under Study: Metoclopramide
4.6. Other Agents
4.7. Recommendations
4.8. Clinical Application
4.9. Our Study and Available Data
4.10. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bechtold, M.; Theivanayagam, S.; Lim, R.; Cobell, W.; Gowda, J.; Matteson, M.; Choudhary, A. Administration of erythromycin before endoscopy in upper gastrointestinal bleeding: A meta-analysis of randomized controlled trials. Saudi J. Gastroenterol. 2013, 19, 205. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3793471/ (accessed on 3 March 2024). [CrossRef] [PubMed]
- Hwang, J.H.; Fisher, D.A.; Ben-Menachem, T.; Chandrasekhara, V.; Chathadi, K.; Decker, G.A.; Early, D.S.; Evans, J.A.; Fanelli, R.D.; Foley, K.; et al. The role of endoscopy in the management of acute non-variceal upper GI bleeding. Gastrointest. Endosc. 2012, 75, 1132–1138. Available online: https://pubmed.ncbi.nlm.nih.gov/22624808/ (accessed on 3 March 2024). [CrossRef] [PubMed]
- Laine, L.; Jensen, D.M. Management of Patients With Ulcer Bleeding. Am. J. Gastroenterol. 2012, 107, 345–360. Available online: https://pubmed.ncbi.nlm.nih.gov/22310222/ (accessed on 3 March 2024). [CrossRef] [PubMed]
- Gralnek, I.M.; Dumonceau, J.-M.; Kuipers, E.J.; Lanas, A.; Sanders, D.S.; Kurien, M.; Rotondano, G.; Hucl, T.; Dinis-Ribeiro, M.; Marmo, R.; et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015, 47, a1–a46. Available online: https://pubmed.ncbi.nlm.nih.gov/26417980/ (accessed on 3 March 2024). [CrossRef]
- Goyal, R.K.; Hirano, I. The enteric nervous system. N. Engl. J. Med. 1996, 334, 1106–1115. Available online: https://pubmed.ncbi.nlm.nih.gov/8598871/ (accessed on 3 March 2024). [CrossRef] [PubMed]
- Furness, J.B.; Callaghan, B.P.; Rivera, L.R.; Cho, H.J. The enteric nervous system and gastrointestinal innervation: Integrated local and central control. Adv. Exp. Med. Biol. 2014, 817, 39–71. Available online: https://pubmed.ncbi.nlm.nih.gov/24997029/ (accessed on 3 March 2024).
- Browning, K.N.; Travagli, R.A. Central nervous system control of gastrointestinal motility and secretion and modulation of gastrointestinal functions. Compr. Physiol. 2014, 4, 1339–1368. Available online: https://pubmed.ncbi.nlm.nih.gov/25428846/ (accessed on 3 March 2024). [PubMed]
- van Leerdam, M.E. Epidemiology of acute upper gastrointestinal bleeding. Best Pract. Res. Clin. Gastroenterol. 2008, 22, 209–224. Available online: https://pubmed.ncbi.nlm.nih.gov/18346679/ (accessed on 3 March 2024). [CrossRef]
- Zhou, S.-Y.; Lu, Y.-X.; Yao, H.; Owyang, C.; Zhou, H.; Gao, J.; Zhang, G.; Babic, T.; Browning, K.N.; Travagli, R.A.; et al. Spatial organization of neurons in the dorsal motor nucleus of the vagus synapsing with intragastric cholinergic and nitric oxide/VIP neurons in the rat. Am. J. Physiol. Gastrointest. Liver Physiol. 2008, 294, G1201–G1209. Available online: https://pubmed.ncbi.nlm.nih.gov/18460697/ (accessed on 3 March 2024). [CrossRef]
- Chang, H.Y.; Mashimo, H.; Goyal, R.K. Musings on the wanderer: What’s new in our understanding of vago-vagal reflex? IV. Current concepts of vagal efferent projections to the gut. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 284, G357–G366. Available online: https://pubmed.ncbi.nlm.nih.gov/12576302/ (accessed on 3 March 2024). [CrossRef]
- Travagli, R.A.; Hermann, G.E.; Browning, K.N.; Rogers, R.C. Brainstem circuits regulating gastric function. Annu. Rev. Physiol. 2006, 68, 279–305. Available online: https://pubmed.ncbi.nlm.nih.gov/16460274/ (accessed on 3 March 2024). [CrossRef] [PubMed]
- Goyal, R.K.; Guo, Y.; Mashimo, H. Advances in the physiology of gastric emptying. Neurogastroenterol. Motil. 2019, 31, e13546. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6850045/ (accessed on 3 March 2024). [CrossRef] [PubMed]
- Sanger, G.J.; Broad, J.; Callaghan, B.; Furness, J.B. Ghrelin and Motilin Control Systems in GI Physiology and Therapeutics. Handb. Exp. Pharmacol. 2017, 239, 379–416. Available online: https://pubmed.ncbi.nlm.nih.gov/28035532/ (accessed on 3 March 2024). [PubMed]
- Miyano, Y.; Sakata, I.; Kuroda, K.; Aizawa, S.; Tanaka, T.; Jogahara, T.; Kurotani, R.; Sakai, T. The Role of the Vagus Nerve in the Migrating Motor Complex and Ghrelin- and Motilin-Induced Gastric Contraction in Suncus. PLoS ONE 2013, 8, e64777. Available online: https://pubmed.ncbi.nlm.nih.gov/23724093/ (accessed on 3 March 2024). [CrossRef] [PubMed]
- Treacy, P.J.; Jamieson, G.G.; Dent, J.; Devitt, P.G.; Heddle, R. Duodenal intramural nerves in control of pyloric motility and gastric emptying. Am. J. Physiol. Liver Physiol. 1992, 263 Pt 1, G1–G5. Available online: https://pubmed.ncbi.nlm.nih.gov/1636704/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- He, J.; Irwin, D.M.; Chen, R.; Zhang, Y.-P. Stepwise loss of motilin and its specific receptor genes in rodents. J. Mol. Endocrinol. 2010, 44, 37–44. Available online: https://pubmed.ncbi.nlm.nih.gov/19696113/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Anselmi, L.; Toti, L.; Bove, C.; Travagli, R.A. Neurogastroenterology and Motility: Vagally mediated effects of brain stem dopamine on gastric tone and phasic contractions of the rat. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 313, G434. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5792220/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Abrahamsson, H. Treatment options for patients with severe gastroparesis. Gut 2007, 56, 877–883. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1954884/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Moran, T.H.; Ladenheim, E.E.; Schwartz, G.J. Within-meal gut feedback signaling. Int. J. Obes. Relat. Metab. Disord. 2001, 25 (Suppl. S5), S39–S41. Available online: https://pubmed.ncbi.nlm.nih.gov/11840213/ (accessed on 4 March 2024). [CrossRef]
- Appleyard, S.M.; Bailey, T.W.; Doyle, M.W.; Jin, Y.-H.; Smart, J.L.; Low, M.J.; Andresen, M.C. Proopiomelanocortin Neurons in Nucleus Tractus Solitarius Are Activated by Visceral Afferents: Regulation by Cholecystokinin and Opioids. J. Neurosci. 2005, 25, 3578–3585. Available online: https://pubmed.ncbi.nlm.nih.gov/15814788/ (accessed on 4 March 2024). [CrossRef]
- Cammisotto, P.; Bendayan, M. A review on gastric leptin: The exocrine secretion of a gastric hormone. Anat. Cell Biol. 2012, 45, 1. Available online: https://pubmed.ncbi.nlm.nih.gov/22536547/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Holmes, G.M.; Browning, K.N.; Tong, M.; Qualls-Creekmore, E.; Travagli, R.A. Vagally mediated effects of glucagon-like peptide 1: In vitro and in vivo gastric actions. J. Physiol. 2009, 587 Pt 19, 4749. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2768027/ (accessed on 4 March 2024). [CrossRef]
- Hisadome, K.; Reimann, F.; Gribble, F.M.; Trapp, S. CCK Stimulation of GLP-1 Neurons Involves α1-Adrenoceptor–Mediated Increase in Glutamatergic Synaptic Inputs. Diabetes 2011, 60, 2701–2709. Available online: https://pubmed.ncbi.nlm.nih.gov/21885869/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Anvari, M.; Paterson, C.A.; Daniel, E.E.; Mcdonald, T.J. Effects of GLP-1 on gastric emptying, antropyloric motility, and transpyloric flow in response to a nonnutrient liquid. Dig. Dis. Sci. 1998, 43, 1133–1140. Available online: https://pubmed.ncbi.nlm.nih.gov/9635598/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Verschueren, S.; Janssen, P.; Van Oudenhove, L.; Hultin, L.; Tack, J. Effect of pancreatic polypeptide on gastric accommodation and gastric emptying in conscious rats. Am. J. Physiol. Liver Physiol. 2014, 307, G122–G128. Available online: https://pubmed.ncbi.nlm.nih.gov/24742985/ (accessed on 4 March 2024). [CrossRef]
- Müller, T.D.; Nogueiras, R.; Andermann, M.L.; Andrews, Z.B.; Anker, S.D.; Argente, J.; Batterham, R.L.; Benoit, S.C.; Bowers, C.Y.; Broglio, F.; et al. Ghrelin. Mol. Metab. 2015, 4, 437. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4443295/ (accessed on 4 March 2024). [CrossRef]
- Cabral, A.; Cornejo, M.P.; Fernandez, G.; De Francesco, P.N.; Garcia-Romero, G.; Uriarte, M.; Zigman, J.M.; Portiansky, E.; Reynaldo, M.; Perello, M. Circulating Ghrelin Acts on GABA Neurons of the Area Postrema and Mediates Gastric Emptying in Male Mice. Endocrinology 2017, 158, 1436–1449. Available online: https://pubmed.ncbi.nlm.nih.gov/28204197/ (accessed on 4 March 2024). [CrossRef]
- Price, C.J.; Hoyda, T.D.; Ferguson, A.V. The Area Postrema: A Brain Monitor and Integrator of Systemic Autonomic State. Neuroscientist 2008, 14, 182–194. Available online: https://pubmed.ncbi.nlm.nih.gov/18079557/ (accessed on 4 March 2024). [CrossRef]
- Swartz, E.M.; Browning, K.N.; Travagli, R.A.; Holmes, G.M. Ghrelin increases vagally mediated gastric activity by central sites of action. Neurogastroenterol. Motil. 2014, 26, 272–282. Available online: https://pubmed.ncbi.nlm.nih.gov/24261332/ (accessed on 4 March 2024). [CrossRef]
- Kitazawa, T.; De Smet, B.; Verbeke, K.; Depoortere, I.; Peeters, T.L. Gastric motor effects of peptide and non-peptide ghrelin agonists in mice in vivo and in vitro. Gut 2005, 54, 1078–1084. Available online: https://pubmed.ncbi.nlm.nih.gov/15843418/ (accessed on 4 March 2024). [CrossRef]
- Tümer, C.; Oflazoğlu, H.D.; Obay, B.D.; Kelle, M.; Taşdemir, E. Effect of ghrelin on gastric myoelectric activity and gastric emptying in rats. Regul. Pept. 2008, 146, 26–32. Available online: https://pubmed.ncbi.nlm.nih.gov/17825442/ (accessed on 4 March 2024). [CrossRef]
- Chung, K.T.; Shelat, V.G. Perforated peptic ulcer—An update. World J. Gastrointest. Surg. 2017, 9, 1–12. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5237817/ (accessed on 5 January 2024). [CrossRef]
- Kamal, F.; Khan, M.A.; Lee-Smith, W.; Sharma, S.; Imam, Z.; Henry, C.; Jowhar, D.; Khan, Z.; Petryna, E.; Iqbal, U.; et al. Role of routine second-look endoscopy in patients with acute peptic ulcer bleeding: Meta-analysis of randomized controlled trials. Gastrointest. Endosc. 2021, 93, 1228–1237.e5. Available online: https://pubmed.ncbi.nlm.nih.gov/33417896/ (accessed on 5 January 2024). [CrossRef]
- Schwarzberg, M.N. Pro-kinetic medications as aids in imaging the small bowel by video-capsule. Med. Hypotheses 2005, 64, 602–607. Available online: https://pubmed.ncbi.nlm.nih.gov/15617876/ (accessed on 5 January 2024). [CrossRef]
- Song, Z.Q.; Gu, F.; Yao, W.; Li, J.; Zhou, L.Y.; Lin, S.R. Evaluation of capsule endoscopy on the diagnosis of gastrointestinal diseases. Beijing Da Xue Xue Bao Yi Xue Ban J. Peking Univ. Health Sci. 2010, 42, 539–542. [Google Scholar]
- Chapman, M.J.; Fraser, R.J.; Kluger, M.T.; Buist, M.D.; De Nichilo, D.J. Erythromycin improves gastric emptying in critically ill patients intolerant of nasogastric feeding. Crit. Care Med. 2000, 28, 2334–2337. Available online: https://pubmed.ncbi.nlm.nih.gov/10921561/ (accessed on 5 January 2024). [CrossRef] [PubMed]
- Parkman, H.P. Chapter 24—Prokinetic agents for gastroparesis. In Gastroparesis: Pathophysiology, Clinical Presentation, Diagnosis and Treatment; Academic Press: Cambridge, MA, USA, 2021; pp. 323–339. [Google Scholar] [CrossRef]
- Macrolide Antibiotics. Meyler’s Side Effects of Drugs. 2016, pp. 710–725. Available online: https://linkinghub.elsevier.com/retrieve/pii/B978044453717101009X (accessed on 28 February 2024).
- Sakai, T. Motilin. In Handbook of Hormones: Comparative Endocrinology for Basic and Clinical Research; Academic Press: Cambridge, MA, USA, 2015; Volume 186, pp. 186–188, e21B-2. [Google Scholar]
- Westaway, S.M.; Sanger, G.J. The identification of and rationale for drugs which act at the motilin receptor. Prog. Med. Chem. 2009, 48, 31–80. [Google Scholar] [PubMed]
- Alam, U.; Asghar, O.; Malik, R.A. Diabetic gastroparesis: Therapeutic options. Diabetes Ther. 2010, 1, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Javid, F.A.; Bulmer, D.C.; Broad, J.; Aziz, Q.; Dukes, G.E.; Sanger, G.J. Anti-emetic and emetic effects of erythromycin in Suncus murinus: Role of vagal nerve activation, gastric motility stimulation and motilin receptors. Eur. J. Pharmacol. 2013, 699, 48–54. Available online: https://pubmed.ncbi.nlm.nih.gov/23201066/ (accessed on 26 February 2024). [CrossRef]
- Janssens, J.; Peeters, T.; Vantrappen, G.; Tack, J.; Urbain, J.; De Roo, M.; Muls, E.; Bouillon, R. Improvement of Gastric Emptying in Diabetic Gastroparesis by Erythromycin. N. Engl. J. Med. 1990, 322, 1028–1031. Available online: https://pubmed.ncbi.nlm.nih.gov/2320062/ (accessed on 28 February 2024). [CrossRef]
- Ardakani, M.J.E.; Zare, E.; Basiri, M.; Shalmani, H.M. Erythromycin decreases the time and improves the quality of EGD in patients with acute upper GI bleeding. Gastroenterol. Hepatol. Bed Bench 2013, 6, 195–201. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017518/ (accessed on 26 February 2024).
- Shah, S.A.A.; Nadeem, M.; Jameel, M.; Yasmin, R.; Afsar, A.; Riaz, F. Oral Erythromycin Improves the Quality of Endoscopy in Upper Gastrointestinal Bleeding Patients. Cureus 2020, 12, e10204. Available online: https://pubmed.ncbi.nlm.nih.gov/33042657/ (accessed on 5 January 2024).
- Lee, A.; Kuo, B. Metoclopramide in the treatment of diabetic gastroparesis. Expert Rev. Endocrinol. Metab. 2010, 5, 653. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3027056/ (accessed on 28 February 2024). [CrossRef]
- Clarke, D.E.; Craig, D.A.; Fozard, J.R. The 5-HT4 receptor: Naughty, but nice. Trends Pharmacol. Sci. 1989, 10, 385–386. Available online: https://pubmed.ncbi.nlm.nih.gov/2694534/ (accessed on 26 February 2024). [CrossRef] [PubMed]
- Valenzuela, J.E.; Dooley, C.P. Dopamine antagonists in the upper gastrointestinal tract. Scand J. Gastroenterol. Suppl. 1984, 96, 127–136. [Google Scholar]
- Tonini, M.; Cipollina, L.; Poluzzi, E.; Crema, F.; Corazza, G.R.; De Ponti, F. Review article: Clinical implications of enteric and central D2 receptor blockade by antidopaminergic gastrointestinal prokinetics. Aliment. Pharmacol. Ther. 2004, 19, 379–390. Available online: https://pubmed.ncbi.nlm.nih.gov/14871277/ (accessed on 26 February 2024). [CrossRef]
- Albibi, R.; McCallum, R.W. Metoclopramide: Pharmacology and clinical application. Ann. Intern. Med. 1983, 98, 86–95. Available online: https://pubmed.ncbi.nlm.nih.gov/6336644/ (accessed on 26 February 2024). [CrossRef] [PubMed]
- Fernández, A.G.; Massingham, R. Peripheral receptor populations involved in the regulation of gastrointestinal motility and the pharmacological actions of metoclopramide-like drugs. Life Sci. 1985, 36, 1–14. Available online: https://pubmed.ncbi.nlm.nih.gov/2981378/ (accessed on 28 February 2024). [CrossRef]
- Kishibayashi, N.; Karasawa, A. Stimulating Effects of KW-5092, a Novel Gastroprokinetic Agent, on the Gastric Emptying, Small Intestinal Propulsion and Colonic Propulsion in Rats. Jpn. J. Pharmacol. 1995, 67, 45–50. Available online: https://pubmed.ncbi.nlm.nih.gov/7745844/ (accessed on 26 February 2024). [CrossRef]
- Camilleri, M.; Atieh, J. New Developments in Prokinetic Therapy for Gastric Motility Disorders. Front. Pharmacol. 2021, 12, 711500. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8421525/ (accessed on 4 March 2024). [CrossRef]
- How to Request Domperidone for Expanded Access Use|FDA. Available online: https://www.fda.gov/drugs/investigational-new-drug-ind-application/how-request-domperidone-expanded-access-use (accessed on 4 March 2024).
- Information about Domperidone|FDA. Available online: https://www.fda.gov/drugs/information-drug-class/information-about-domperidone (accessed on 4 March 2024).
- Lucey, M.; Patil, V.; Girling, K.; Jacques, T.; O’leary, M. Does Neostigmine Increase Gastric Emptying in the Critically Ill?—Results of a Pilot Study. Crit. Care Resusc. 2003, 5, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Manini, M.L.; Camilleri, M.; Grothe, R.; Di Lorenzo, C. Application of Pyridostigmine in Pediatric Gastrointestinal Motility Disorders: A Case Series. Pediatr. Drugs 2018, 20, 173–180. Available online: https://pubmed.ncbi.nlm.nih.gov/29243034/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Abell, T.L.; Camilleri, M.; DiMagno, E.P.; Hench, V.S.; Zinsmeister, A.R.; Malagelada, J.-R. Long-term efficacy of oral cisapride in symptomatic upper gut dysmotility. Dig. Dis. Sci. 1991, 36, 616–620. Available online: https://pubmed.ncbi.nlm.nih.gov/2022163/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Richards, R.D.; Valenzuela, G.A.; Davenport, K.G.; Fisher, K.L.K.; McCallum, R.W. Objective and subjective results of a randomized, double-blind, placebo-controlled trial using cisapride to treat gastroparesis. Dig. Dis. Sci. 1993, 38, 811–816. Available online: https://pubmed.ncbi.nlm.nih.gov/8482178/ (accessed on 4 March 2024). [CrossRef]
- Bavestrello, L.; Caimi, L.; Barbera, A. A double-blind comparison of clebopride and placebo in dyspepsia secondary to delayed gastric emptying. Clin. Ther. 1985, 7, 468–473. [Google Scholar] [PubMed]
- Kawamura, E.; Enomoto, M.; Kotani, K.; Hagihara, A.; Fujii, H.; Kobayashi, S.; Iwai, S.; Morikawa, H.; Kawabe, J.; Tominaga, K.; et al. Effect of Mosapride Citrate on Gastric Emptying in Interferon-Induced Gastroparesis. Dig. Dis. Sci. 2012, 57, 1510–1516. Available online: https://pubmed.ncbi.nlm.nih.gov/22399248/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Portincasa, P.; Mearin, F.; Robert, M.; Plazas, M.J.; Mas, M.; Heras, J. Efficacy and tolerability of cinitapride in the treatment of functional dyspepsia and delayed gastric emptying. Gastroenterol. Hepatol. 2009, 32, 669–676. Available online: https://pubmed.ncbi.nlm.nih.gov/19819042/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Carbone, F.; Houte, K.V.D.; Clevers, E.; Andrews, C.N.; Papathanasopoulos, A.; Holvoet, L.; Van Oudenhove, L.; Caenepeel, P.; Arts, J.; Vanuytsel, T.; et al. Prucalopride in Gastroparesis: A Randomized Placebo-Controlled Crossover Study. Am. J. Gastroenterol. 2019, 114, 1265–1274. Available online: https://pubmed.ncbi.nlm.nih.gov/31295161/ (accessed on 4 March 2024). [CrossRef]
- Kuo, B.; Barnes, C.N.; Nguyen, D.D.; Shaywitz, D.; Grimaldi, M.; Renzulli, C.; Canafax, D.; Parkman, H.P. Velusetrag accelerates gastric emptying in subjects with gastroparesis: A multicentre, double-blind, randomised, placebo-controlled, phase 2 study. Aliment. Pharmacol. Ther. 2021, 53, 1090–1097. Available online: https://pubmed.ncbi.nlm.nih.gov/33811761/ (accessed on 4 March 2024). [CrossRef]
- Chedid, V.; Brandler, J.; Arndt, K.; Vijayvargiya, P.; Wang, X.J.; Burton, D.; Harmsen, W.S.; Siegelman, J.; Chen, C.; Chen, Y.; et al. Randomised study: Effects of the 5-HT4 receptor agonist felcisetrag vs placebo on gut transit in patients with gastroparesis. Aliment. Pharmacol. Ther. 2021, 53, 1010–1020. Available online: https://pubmed.ncbi.nlm.nih.gov/33711180/ (accessed on 4 March 2024). [CrossRef]
- Chapman, M.J.; Jones, K.L.; Almansa, C.; Barnes, C.N.; Nguyen, D.; Deane, A.M. Blinded, Double-Dummy, Parallel-Group, Phase 2a Randomized Clinical Trial to Evaluate the Efficacy and Safety of a Highly Selective 5-Hydroxytryptamine Type 4 Receptor Agonist in Critically Ill Patients With Enteral Feeding Intolerance. JPEN J. Parenter Enteral. Nutr. 2021, 45, 115–124. Available online: https://pubmed.ncbi.nlm.nih.gov/31990087/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Beattie, D.T.; Higgins, D.L.; Ero, M.P.; Amagasu, S.M.; Vickery, R.G.; Kersey, K.; Hopkins, A.; Smith, J.A.M. An in vitro investigation of the cardiovascular effects of the 5-HT4 receptor selective agonists, velusetrag and TD-8954. Vascul. Pharmacol. 2013, 58, 150–156. Available online: https://pubmed.ncbi.nlm.nih.gov/23201772/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Beattie, D.T.; Armstrong, S.R.; Vickery, R.G.; Tsuruda, P.R.; Campbell, C.B.; Richardson, C.; McCullough, J.L.; Daniels, O.; Kersey, K.; Li, Y.P.; et al. The pharmacology of TD-8954, a potent and selective 5-HT4 receptor agonist with gastrointestinal prokinetic properties. Front. Pharmacol. 2011, 2, 25. Available online: https://pubmed.ncbi.nlm.nih.gov/21687517/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Pasricha, P.J.; Yates, K.P.; Sarosiek, I.; McCallum, R.W.; Abell, T.L.; Koch, K.L.; Nguyen, L.A.B.; Snape, W.J.; Hasler, W.L.; Clarke, J.O.; et al. Aprepitant Has Mixed Effects on Nausea and Reduces Other Symptoms in Patients with Gastroparesis and Related Disorders. Gastroenterology 2018, 154, 65–76.e11. Available online: https://pubmed.ncbi.nlm.nih.gov/29111115/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Carlin, J.L.; Lieberman, V.R.; Dahal, A.; Keefe, M.S.; Xiao, C.; Birznieks, G.; Abell, T.L.; Lembo, A.; Parkman, H.P.; Polymeropoulos, M.H. Efficacy and Safety of Tradipitant in Patients With Diabetic and Idiopathic Gastroparesis in a Randomized, Placebo-Controlled Trial. Gastroenterology 2021, 160, 76–87.e4. Available online: https://pubmed.ncbi.nlm.nih.gov/32693185/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Shin, A.; Camilleri, M.; Busciglio, I.; Burton, D.; Stoner, E.; Noonan, P.; Gottesdiener, K.; Smith, S.A.; Vella, A.; Zinsmeister, A.R. Randomized controlled phase Ib study of ghrelin agonist, RM-131, in type 2 diabetic women with delayed gastric emptying: Pharmacokinetics and pharmacodynamics. Diabetes Care 2013, 36, 41–48. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3526234/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Camilleri, M.; Lembo, A.; McCallum, R.; Tourkodimitris, S.; Kemps, L.; Miller, M.B.; Bertelsen, K.; Iacob, A. Overall safety of relamorelin in adults with diabetic gastroparesis: Analysis of phase 2a and 2b trial data. Aliment. Pharmacol. Ther. 2020, 51, 1139–1148. Available online: https://pubmed.ncbi.nlm.nih.gov/32301137/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Larson, J.M.; Tavakkoli, A.; E Drane, W.; Toskes, P.P.; Moshiree, B. Advantages of Azithromycin over erythromycin in improving the gastric emptying half-time in adult patients with gastroparesis. J. Neurogastroenterol. Motil. 2010, 16, 407–413. Available online: https://pubmed.ncbi.nlm.nih.gov/21103422/ (accessed on 4 March 2024). [CrossRef] [PubMed]
- Bortolotti, M.; Mari, C.; Brunelli, F.; Sarti, P.; Miglioli, M. Effect of intravenous clarithromycin on interdigestive gastroduodenal motility of patients with functional dyspepsia and Helicobacter pylori gastritis. Dig. Dis. Sci. 1999, 44, 2439–2442. Available online: https://pubmed.ncbi.nlm.nih.gov/10630494/ (accessed on 4 March 2024). [CrossRef]
- Barkun, A.N.; Bardou, M.; Martel, M.; Gralnek, I.M.; Sung, J.J. Prokinetics in acute upper GI bleeding: A meta-analysis. Gastrointest. Endosc. 2010, 72, 1138–1145. Available online: https://pubmed.ncbi.nlm.nih.gov/20970794/ (accessed on 5 January 2024). [CrossRef]
- Muthusamy, V.R.; Kim, S. Prophylactic erythromycin in acute upper gastrointestinal bleeding: Moving forward in improving endoscopic efficacy. Saudi J. Gastroenterol. 2013, 19, 193. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3793469/ (accessed on 5 January 2024). [CrossRef] [PubMed]
- Pateron, D.; Vicaut, E.; Debuc, E.; Sahraoui, K.; Carbonell, N.; Bobbia, X.; Thabut, D.; Adnet, F.; Nahon, P.; Amathieu, R.; et al. Erythromycin Infusion or Gastric Lavage for Upper Gastrointestinal Bleeding: A Multicenter Randomized Controlled Trial. Ann. Emerg. Med. 2011, 57, 582–589. Available online: https://pubmed.ncbi.nlm.nih.gov/21333385/ (accessed on 5 January 2024). [CrossRef] [PubMed]
- Winstead, N.S.; Wilcox, C.M. Erythromycin prior to endoscopy for acute upper gastrointestinal haemorrhage: A cost-effectiveness analysis. Aliment. Pharmacol. Ther. 2007, 26, 1371–1377. Available online: https://pubmed.ncbi.nlm.nih.gov/17848180/ (accessed on 5 January 2024). [CrossRef] [PubMed]
- Estes, D.J.; Berera, S.; Deshpande, A.R.; Sussman, D.A. Re-Visiting Metoclopramide to Optimize Visualization with Gastrointestinal Bleeding—Mobilizing Existing Data. Clin. Endosc. 2019, 52, 516. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6785415/ (accessed on 5 January 2024). [CrossRef] [PubMed]
- Tarasconi, A.; Coccolini, F.; Biffl, W.L.; Tomasoni, M.; Ansaloni, L.; Picetti, E.; Molfino, S.; Shelat, V.; Cimbanassi, S.; Weber, D.G.; et al. Perforated and bleeding peptic ulcer: WSES guidelines. World J. Emerg. Surg. 2020, 15, 3. Available online: https://researchportal.helsinki.fi/en/publications/perforated-and-bleeding-peptic-ulcer-wses-guidelines (accessed on 5 January 2024). [CrossRef] [PubMed]
- Vimonsuntirungsri, T.; Thungsuk, R.; Nopjaroonsri, P.; Faknak, N.; Pittayanon, R. The Efficacy of Metoclopramide for Gastric Visualization by Endoscopy in Patients With Active Upper Gastrointestinal Bleeding: Double-Blind Randomized Controlled Trial. Am. J. Gastroenterol. 2024. Available online: https://journals.lww.com/ajg/fulltext/9900/the_efficacy_of_metoclopramide_for_gastric.951.aspx (accessed on 5 January 2024).
- Bai, Y.; Guo, J.-F.; Li, Z.-S. Meta-analysis: Erythromycin before endoscopy for acute upper gastrointestinal bleeding. Aliment. Pharmacol. Ther. 2011, 34, 166–171. Available online: https://pubmed.ncbi.nlm.nih.gov/21615438/ (accessed on 5 January 2024). [CrossRef] [PubMed]
- Aziz, M.; Haghbin, H.; Gangwani, M.K.; Weissman, S.; Patel, A.R.; Randhawa, M.K.; Samikanu, L.B.; Alyousif, Z.A.; Lee-Smith, W.; Kamal, F.; et al. Erythromycin Improves the Quality of Esophagogastroduodenoscopy in Upper Gastrointestinal Bleeding: A Network Meta-Analysis. Dig. Dis. Sci. 2023, 68, 1435–1446. Available online: https://pubmed.ncbi.nlm.nih.gov/36112271/ (accessed on 5 January 2024). [CrossRef]
- Farooq, U.; Tarar, Z.; Ashraf, M.; Tahan, V.; Daglilar, E. No Difference in Mortality From Nonvariceal Upper Gastrointestinal Hemorrhage Between Racial Groups: A Nationwide Time Trend Analysis, 2008–2018. Mayo Clin. Proc. 2023, 98, 203–205. Available online: http://www.mayoclinicproceedings.org/article/S002561962200653X/fulltext (accessed on 6 March 2024). [CrossRef]
- Manupeeraphant, P.; Wanichagool, D.; Songlin, T.; Thanathanee, P.; Chalermsuksant, N.; Techathuvanan, K.; Sethasine, S. Intravenous metoclopramide for increasing endoscopic mucosal visualization in patients with acute upper gastrointestinal bleeding: A multicenter, randomized, double-blind, controlled trial. Sci. Rep. 2024, 14, 7598. Available online: https://www.nature.com/articles/s41598-024-57913-2 (accessed on 7 April 2024). [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before PSM | |||
|---|---|---|---|
| Metoclopramide (n = 11,161) | Erythromycin (n = 3683) | No Meds (n = 82,126) | |
| Age ± SD | 56.7 ± 16 | 64.9 ± 16.5 | 65.7 ± 15.1 |
| BMI | 28.8 ± 6.6 | 28.7 ± 6.2 | 28.7 ± 6.1 |
| Female | 46.6% | 43.4% | 39.1% |
| Not Hispanic or Latino | 19.1% | 20.3% | 15.5% |
| Hispanic or Latino | 2.2% | 1.7% | 1.5% |
| White | 15.2% | 17.4% | 13.1% |
| Asian | 0.09% | 0.3% | 0.2% |
| Black or African American | 4% | 3% | 2.5% |
| Arm 1 after PSM | Arm 2 after PSM | Arm 3 after PSM | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Metoclopramide (n = 11,161) | No Meds (n = 11,161) | p-Value | Metoclopramide (n = 3683) | Erythromycin (n = 3683) | p-Value | Erythromycin (n = 3683) | No Meds (n = 3683) | p-Value | |
| Age ± SD | 56.7 ± 16 | 56.7 ± 16 | 0.98 | 64.4 ± 16.3 | 64.4 ± 16.4 | 0.94 | 64.9 ± 16.5 | 65 ± 16.5 | 0.75 |
| BMI | 28.8 ± 6.6 | 29.1 ± 6.4 | 0.92 | 28.3 ± 6.3 | 28.8 ± 6.3 | 0.42 | 28.7 ± 6.2 | 28.7 ± 6 | 0.97 |
| Female | 46.6% | 46.6% | 0.99 | 43.4% | 43.7% | 0.76 | 43.4% | 43.4% | 0.98 |
| Not Hispanic or Latino | 19.1% | 19.2% | 0.93 | 20% | 20.2% | 0.86 | 20.5% | 20.3% | 0.89 |
| Hispanic or Latino | 2.2% | 2.2% | 0.92 | 1.5% | 1.8% | 0.31 | 1.7% | 1.7% | 1 |
| White | 15.2% | 15.3% | 0.91 | 16.8% | 17% | 0.73 | 17.5% | 17.5% | 0.98 |
| Asian | 0.09% | 0.1% | 0.82 | 0.3% | 0.3% | 1 | 0.3% | 0.3% | 1 |
| Black or African American | 4% | 3.8% | 0.53 | 3% | 3% | 0.94 | 3% | 2.9% | 0.73 |
|
Metoclopramide
(n = 11,161) |
No Meds
(n = 11,161) | p -Value |
Metoclopramide
(n = 3683) |
Erythromycin
(n = 3683) | p -Value |
Erythromycin
(n = 3683) |
No Meds
(n = 3683) | p -Value | |
|---|---|---|---|---|---|---|---|---|---|
| Repeat EGD | 10.1% | 9.7% | 0.34 | 9.4% | 7.5% | 0.003 | 7.5% | 9.5% | 0.003 |
| Mortality | 1.08% | 1.08% | 0.95 | 1.4% | 0.9% | 0.1 | 1% | 1.6% | 0.02 |
| Post EGD Transfusion | 0.78% | 0.86% | 0.5 | 0.8% | 0.5% | 0.19 | 0.5% | 1% | 0.02 |
| Receptor | Antiemetic | Gastric Emptying | Comments | |
|---|---|---|---|---|
| Metoclopramide |
D2 Antagonist
5HT4 Agonist | Yes | Improve |
Extrapyramidal symptoms
QT prolongation |
| Domperidone | D2 Antagonist | Yes | Improve | Investigational |
| Neostigmine | acetyl cholinesterase Inhibitors | Unknown | Yes |
Bradycardia
Studies limited to critically ill-patient |
| Cisapride, cinitapride, and mosapride |
5HT4 Agonist
5HT3 Antagonist | Unknown | Improve | QT prolongation |
| Prucalopride, velusetrag, naronapride, and felcisetrag. | 5HT4 Agonist | Unknown | Improve | Being studied |
| Clebopride |
5HT4 Agonist
D2 Antagonist | Unknown | Unknown | Not being studied |
| Tradipitant |
D2/D3 Antagonist
NK1 Agonist | Unknown | Unknown | |
| Aprepitant |
D2/D3 Antagonist
NK1 Agonist | Unknown | No | |
| Relamorelin | Ghrelin Agonist | Yes | Yes | Being studied |
| Erythromycin | Motilin Agonist | Unknown | Yes |
Risk for tachyphylaxis
Risk of arrythmia |
| Azithromycin | Motilin Agonist | Unknown | Yes | Risk of antimicrobial resistance |
| Clarithromycin | Motilin Agonist | Unknown | Yes | Risk of antimicrobial resistance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayoub, M.; Faris, C.; Tomanguillo, J.; Anwar, N.; Chela, H.; Daglilar, E. The Use of Pre-Endoscopic Metoclopramide Does Not Prevent the Need for Repeat Endoscopy: A U.S. Based Retrospective Cohort Study. Life 2024, 14, 526. https://doi.org/10.3390/life14040526
Ayoub M, Faris C, Tomanguillo J, Anwar N, Chela H, Daglilar E. The Use of Pre-Endoscopic Metoclopramide Does Not Prevent the Need for Repeat Endoscopy: A U.S. Based Retrospective Cohort Study. Life. 2024; 14(4):526. https://doi.org/10.3390/life14040526
Chicago/Turabian StyleAyoub, Mark, Carol Faris, Julton Tomanguillo, Nadeem Anwar, Harleen Chela, and Ebubekir Daglilar. 2024. "The Use of Pre-Endoscopic Metoclopramide Does Not Prevent the Need for Repeat Endoscopy: A U.S. Based Retrospective Cohort Study" Life 14, no. 4: 526. https://doi.org/10.3390/life14040526
APA StyleAyoub, M., Faris, C., Tomanguillo, J., Anwar, N., Chela, H., & Daglilar, E. (2024). The Use of Pre-Endoscopic Metoclopramide Does Not Prevent the Need for Repeat Endoscopy: A U.S. Based Retrospective Cohort Study. Life, 14(4), 526. https://doi.org/10.3390/life14040526