
COVID-19 Crisis in Brazil: Post-Vaccination Seroprevalence and Infection in More and Less Vaccinated Municipalities in a Northeastern State
 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Target Public Selection
2.2. Data Collection
2.3. Antigenic and RT-qPCR Detection Process
2.4. Antibodies Detection Process
2.5. Statistical Analysis and Data Visualization
3. Results
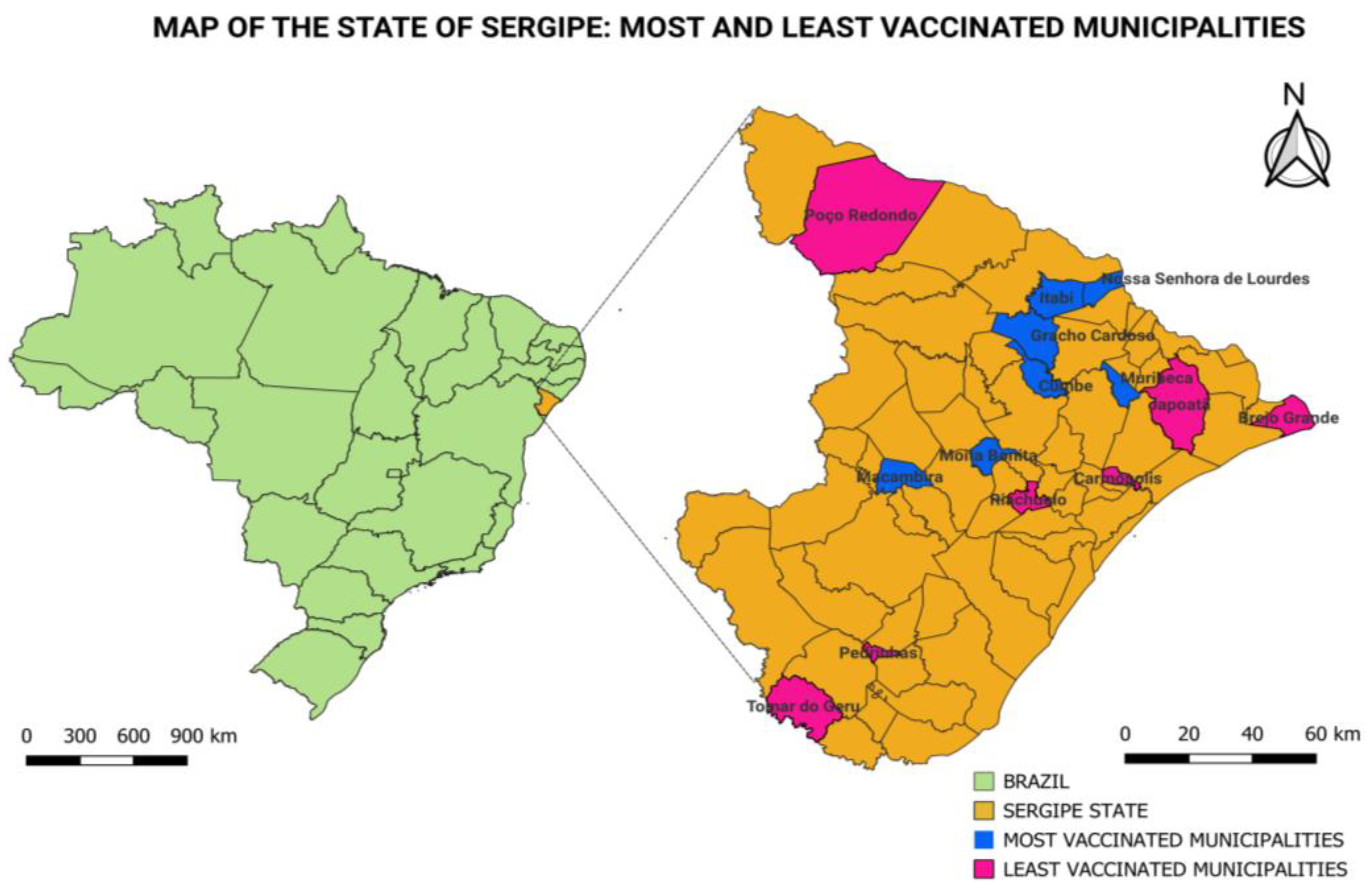
3.1. Data Analysis in the Tested Municipalities
3.2. Association between Antigen/RT-qPCR and IgM Antibodies in the Tested Municipalities
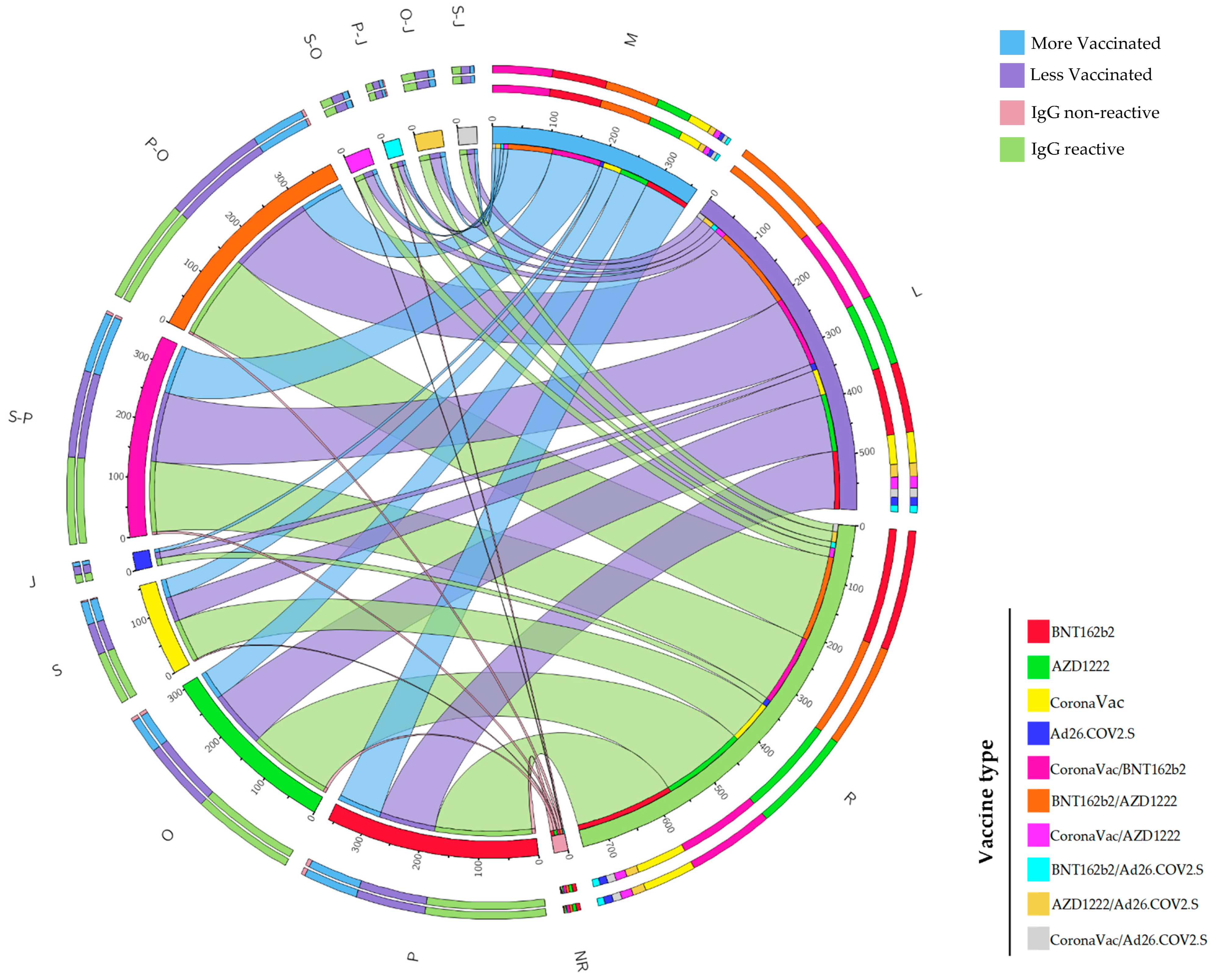
3.3. Distribution and Combinations of Vaccines, Together with the Production of IgG Antibodies, in the Most and Least Vaccinated Municipalities
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alquraan, L.; Alzoubi, K.H.; Rababa’h, S.Y. Mutations of SARS-CoV-2 and Their Impact on Disease Diagnosis and Severity. Inf. Med. Unlocked 2023, 39, 101256. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Update on Omicron. Available online: https://www.who.int/news/item/28-11-2021-update-on-omicron (accessed on 7 August 2023).
- Ren, S.-Y.; Wang, W.-B.; Gao, R.-D.; Zhou, A.-M. Omicron Variant (B.1.1.529) of SARS-CoV-2: Mutation, Infectivity, Transmission, and Vaccine Resistance. World J. Clin. Cases 2022, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Variante Ômicron: Brasil dá Resposta Rápida em Vigilância e Monitoramento da COVID-19. Available online: https://www.gov.br/saude/pt-br/assuntos/noticias/2021/dezembro/variante-omicron-brasil-da-resposta-rapida-em-vigilancia-e-monitoramento-da-covid-19 (accessed on 7 August 2023).
- Moura, E.C.; Cortez-Escalante, J.; Cavalcante, F.V.; Barreto, I.C.d.H.C.; Sanchez, M.N.; Santos, L.M.P. COVID-19: Evolução Temporal e Imunização Nas Três Ondas Epidemiológicas, Brasil, 2020–2022. Rev. Saúde Pública 2022, 56, 105. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). COVID-19 Weekly Epidemiological Update. 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---1-february-2022 (accessed on 19 May 2023).
- Governo de Sergipe. Boletim Vacina COVID-19—29.01.2022—Todos Contra o Corona. Available online: https://todoscontraocorona.net.br/vacina-covid-19-29-01-2022/ (accessed on 16 May 2023).
- de Bruin, Y.B.; Lequarre, A.-S.; McCourt, J.; Clevestig, P.; Pigazzani, F.; Jeddi, M.Z.; Colosio, C.; Goulart, M. Initial Impacts of Global Risk Mitigation Measures Taken during the Combatting of the COVID-19 Pandemic. Saf. Sci. 2020, 128, 104773. [Google Scholar] [CrossRef]
- Schmitz, A.J.; Turner, J.S.; Liu, Z.; Zhou, J.Q.; Aziati, I.D.; Chen, R.E.; Joshi, A.; Bricker, T.L.; Darling, T.L.; Adelsberg, D.C.; et al. A Vaccine-Induced Public Antibody Protects against SARS-CoV-2 and Emerging Variants. Immunity 2021, 54, 2159–2166.e6. [Google Scholar] [CrossRef] [PubMed]
- Jing, S.; Milne, R.; Wang, H.; Xue, L. Vaccine Hesitancy Promotes Emergence of New SARS-CoV-2 Variants. J. Theor. Biol. 2023, 570, 111522. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Strategy to Achieve Global COVID-19 Vaccination by Mid-2022. 2021. Available online: https://www.who.int/publications/m/item/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022 (accessed on 16 May 2023).
- dos Santos, C.V.B.; Valiati, N.C.M.; de Noronha, T.G.; Porto, V.B.G.; Pacheco, A.G.; Freitas, L.P.; Coelho, F.C.; Gomes, M.F.d.C.; Bastos, L.S.; Cruz, O.G.; et al. The Effectiveness of COVID-19 Vaccines against Severe Cases and Deaths in Brazil from 2021 to 2022: A Registry-Based Study. Lancet Reg. Health—Am. 2023, 20, 100465. [Google Scholar] [CrossRef]
- Ministério da Saúde. Vacinômetro COVID-19. Available online: https://infoms.saude.gov.br/extensions/SEIDIGI_DEMAS_Vacina_C19/SEIDIGI_DEMAS_Vacina_C19.html (accessed on 7 August 2023).
- Brasil. Ministério da Saúde. Ministério da Saúde Antecipa de Cinco Para Quatro Meses a Aplicação da Dose de Reforço. Available online: https://www.gov.br/saude/pt-br/assuntos/noticias/2021-1/dezembro/ministerio-da-saude-antecipa-de-cinco-para-quatro-meses-a-aplicacao-da-dose-de-reforco (accessed on 11 February 2023).
- Ministério da Saúde. VACINÔMETRO. Available online: https://conselho.saude.gov.br/vacinometro (accessed on 7 January 2022).
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global Impact of the First Year of COVID-19 Vaccination: A Mathematical Modelling Study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef]
- McLaughlin, J.M.; Khan, F.; Pugh, S.; Swerdlow, D.L.; Jodar, L. County-Level Vaccination Coverage and Rates of COVID-19 Cases and Deaths in the United States: An Ecological Analysis. Lancet Reg. Health—Am. 2022, 9, 100191. [Google Scholar] [CrossRef]
- QGIS. Software. Available online: https://www.qgis.org/pt_BR/site/forusers/download.html (accessed on 7 August 2023).
- Governo Federal. IBGE. Available online: https://cidades.ibge.gov.br/ (accessed on 7 August 2023).
- Governo de Sergipe. Boletins Covid—Todos contra o Corona. Available online: https://todoscontraocorona.net.br/boletins-covid/ (accessed on 16 May 2023).
- Borges, L.P.; Martins, A.F.; de Melo, M.S.; de Oliveira, M.G.B.; Neto, J.M.d.R.; Dósea, M.B.; Cabral, B.C.M.; Menezes, R.F.; Santos, A.A.; Matos, I.L.S.; et al. Seroprevalence of SARS-CoV-2 IgM and IgG Antibodies in an Asymptomatic Population in Sergipe, Brazil. Rev. Panam. Salud Pública 2020, 44, 1. [Google Scholar] [CrossRef]
- Borges, L.P.; Guimarães, A.G.; Fonseca, D.L.M.; Freire, P.P.; Barreto, D.; Souza, D.R.; Gurgel, R.Q.; Lopes, A.S.; Neto, J.M.d.R.; dos Santos, K.A.; et al. Cross-Sectional Analysis of Students and School Workers Reveals a High Number of Asymptomatic SARS-CoV-2 Infections during School Reopening in Brazilian Cities. Heliyon 2022, 8, e11368. [Google Scholar] [CrossRef] [PubMed]
- Gurgel, R.Q.; de Sá, L.C.; Souza, D.R.V.; Martins, A.F.; Matos, I.L.S.; Lima, A.G.A.; Vieira, S.C.F.; Neto, J.M.d.R.; Cuevas, L.E.; Borges, L.P. SARS-CoV-2 Has Been Circulating in Northeastern Brazil since February 2020: Evidence for Antibody Detection in Asymptomatic Patients. J. Infect. 2021, 82, 186–230. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.P.; da Silva, H.S.; Silva, J.R.S.; Guimarães, A.G. Perfil de Mortalidade Por COVID-19 Durante Os Primeiros 15 Meses Da Pandemia. Res. Soc. Dev. 2021, 10, e377101623924. [Google Scholar] [CrossRef]
- Melo, M.A.; Borges, L.P.; Salvatori, R.; Souza, D.R.V.; Santos-Júnior, H.T.; Neto, J.M.d.R.; Campos, V.C.; Santos, A.A.; Oliveira, C.R.P.; da Invenção, G.B.; et al. Individuals with Isolated Congenital GH Deficiency Due to a GHRH Receptor Gene Mutation Appear to Cope Better with SARS-CoV-2 Infection than Controls. Endocrine 2021, 72, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.P.; Nascimento, L.C.; Heimfarth, L.; Souza, D.R.V.; Martins, A.F.; de Rezende Neto, J.M.; dos Santos, K.A.; Matos, I.L.S.; da Invenção, G.B.; Oliveira, B.M.; et al. Estimated SARS-CoV-2 Infection and Seroprevalence in Firefighters from a Northeastern Brazilian State: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 8148. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.P.; Martins, A.F.; de Souza, D.R.V.; de Rezende Neto, J.M.; Santos, A.A.; Oliveira, B.M.; Matos, I.L.S.; da Invenção, G.B.; dos Santos, K.A.; Souza, N.A.A.; et al. Does In-Person Visiting Affect the Number of COVID-19 Cases in Prisons? Life 2021, 11, 1184. [Google Scholar] [CrossRef] [PubMed]
- Eco Diagnóstica. COVID-19 Ag ECO Teste. Available online: https://ecodiagnostica.com.br/diagnostico-rapido/covid-19-ag-eco-teste/ (accessed on 27 December 2023).
- TaqPathTM COVID-19 CE-IVD RT-PCR Kit. Available online: https://www.thermofisher.com/order/catalog/product/A48067?SID=srch-srp-A48067 (accessed on 24 August 2023).
- Clinical Evaluation of the TaqPath COVID-19 CE-IVD RT-PCR Kit for the Detection of SARS-CoV-2. Available online: https://assets.thermofisher.com/TFS-Assets/GSD/Reference-Materials/taqpath-ceivd-rt-pcr-kit-technical-bulletin.pdf (accessed on 24 August 2023).
- Boditech Med Incorporated. ichromaTM COVID-19 Ab. Available online: https://biovalent.com.br/wp-content/uploads/2021/10/BL3686-REV02-08-2020-ICHROMA-COVID-19-AB-Boditech.pdf (accessed on 7 August 2023).
- GRUPO BIOSYS KOVALENT. REAGENTE ICHROMA COVID-19 AB. Available online: https://grupokovalent.com.br/reagente/ichroma-covid-19-ab/ (accessed on 7 August 2023).
- IBM SPSS Software. SPSS. Available online: https://www.ibm.com/br-pt/spss. (accessed on 19 February 2023).
- Zhou, Y.; Zhu, Y.; Wong, W.K. Statistical Tests for Homogeneity of Variance for Clinical Trials and Recommendations. Contemp. Clin. Trials Commun. 2023, 33, 101119. [Google Scholar] [CrossRef]
- McHugh, M.L. The Chi-Square Test of Independence. Biochem. Med. 2013, 23, 143–149. [Google Scholar] [CrossRef]
- Upton, G.J.G. Fisher’s Exact Test. J. R. Stat. Soc. Ser. A Stat. Soc. 1992, 155, 395. [Google Scholar] [CrossRef]
- Santos, C.A.S.; Fiaccone, R.L.; Oliveira, N.F.; Cunha, S.; Barreto, M.L.; do Carmo, M.B.B.; Moncayo, A.-L.; Rodrigues, L.C.; Cooper, P.J.; Amorim, L.D. Estimating Adjusted Prevalence Ratio in Clustered Cross-Sectional Epidemiological Data. BMC Med. Res. Methodol. 2008, 8, 80. [Google Scholar] [CrossRef]
- Persoskie, A.; Ferrer, R.A. A Most Odd Ratio. Am. J. Prev. Med. 2017, 52, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Tseng, T.; Flechner, L. Understanding Results: P-Values, Confidence Intervals, and Number Need to Treat. Indian J. Urol. 2011, 27, 532. [Google Scholar] [CrossRef] [PubMed]
- Krzywinski, M.; Schein, J.; Birol, İ.; Connors, J.; Gascoyne, R.; Horsman, D.; Jones, S.J.; Marra, M.A. Circos: An Information Aesthetic for Comparative Genomics. Genome Res. 2009, 19, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Governo de Sergipe. Boletim COVID-19—Semana Epidemiológica—4—Todos Contra o Corona. Available online: https://todoscontraocorona.net.br/boletim-covid-19-semana-epidemiologica-4/ (accessed on 16 May 2023).
- Ministério da Saúde. COVID-19 NO BRASIL. Available online: https://infoms.saude.gov.br/extensions/covid-19_html/covid-19_html.html (accessed on 29 May 2023).
- Rotshild, V.; Hirsh-Raccah, B.; Miskin, I.; Muszkat, M.; Matok, I. Comparing the Clinical Efficacy of COVID-19 Vaccines: A Systematic Review and Network Meta-Analysis. Sci. Rep. 2021, 11, 22777. [Google Scholar] [CrossRef] [PubMed]
- Marklund, E.; Leach, S.; Axelsson, H.; Nystrom, K.; Norder, H.; Bemark, M.; Angeletti, D.; Lundgren, A.; Nilsson, S.; Andersson, L.M.; et al. Serum-IgG Responses to SARS-CoV-2 after Mild and Severe COVID-19 Infection and Analysis of IgG Non-Responders. PLoS ONE 2020, 15, e0241104. [Google Scholar] [CrossRef] [PubMed]
- Kingstad-Bakke, B.; Lee, W.; Chandrasekar, S.S.; Gasper, D.J.; Salas-Quinchucua, C.; Cleven, T.; Sullivan, J.A.; Talaat, A.; Osorio, J.E.; Suresh, M. Vaccine-Induced Systemic and Mucosal T Cell Immunity to SARS-CoV-2 Viral Variants. Proc. Natl. Acad. Sci. USA 2022, 119, e2118312119. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.K.P.; Zhu, A.; Zhao, J.; Lau, E.H.Y.; Wang, J.; Chen, Z.; Zhuang, Z.; Wang, Y.; Alshukairi, A.N.; Baharoon, S.A.; et al. T-Cell Responses to MERS Coronavirus Infection in People with Occupational Exposure to Dromedary Camels in Nigeria: An Observational Cohort Study. Lancet Infect. Dis. 2021, 21, 385–395. [Google Scholar] [CrossRef]
- Ho, J.Q.; Sepand, M.R.; Bigdelou, B.; Shekarian, T.; Esfandyarpour, R.; Chauhan, P.; Serpooshan, V.; Beura, L.K.; Hutter, G.; Zanganeh, S. The Immune Response to COVID-19: Does Sex Matter? Immunology 2022, 166, 429–443. [Google Scholar] [CrossRef]
- Orner, E.P.; Rodgers, M.A.; Hock, K.; Tang, M.S.; Taylor, R.; Gardiner, M.; Olivo, A.; Fox, A.; Prostko, J.; Cloherty, G.; et al. Comparison of SARS-CoV-2 IgM and IgG Seroconversion Profiles among Hospitalized Patients in Two US Cities. Diagn. Microbiol. Infect. Dis. 2021, 99, 115300. [Google Scholar] [CrossRef]
- Santarpia, J.L.; Rivera, D.N.; Herrera, V.L.; Morwitzer, M.J.; Creager, H.M.; Santarpia, G.W.; Crown, K.K.; Brett-Major, D.M.; Schnaubelt, E.R.; Broadhurst, M.J.; et al. Aerosol and Surface Contamination of SARS-CoV-2 Observed in Quarantine and Isolation Care. Sci. Rep. 2020, 10, 12732. [Google Scholar] [CrossRef]
- Borges, L.P.; Barreto, M.D.S.; Santos, R.S.; DE Souza, J.B.; DA Silva, B.S.; DE Jesus, P.C.; Silva, D.M.; Moura, P.H.; DOS Santos, L.M.; Silva, E.E.; et al. Why Are Measles and Rubella Returning in Brazil? Acad. Bras. Cienc. 2023, 95 (Suppl. S2), e20230832. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.C.B.C.; Nehab, M.F.; Camacho, K.G.; Reis, A.T.; Junqueira-Marinho, M.d.F.; Abramov, D.M.; de Azevedo, Z.M.A.; de Menezes, L.A.; Salú, M.d.S.; Figueiredo, C.E.d.S.; et al. Low COVID-19 Vaccine Hesitancy in Brazil. Vaccine 2021, 39, 6262–6268. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.-Y.; Xu, Y.; Gu, Y.; Zeng, D.; Wheeler, B.; Young, H.; Sunny, S.K.; Moore, Z. Effectiveness of Bivalent Boosters against Severe Omicron Infection. N. Engl. J. Med. 2023, 388, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Ministério da Saúde Amplia Vacinação com Dose de Reforço Bivalente Contra COVID-19 Para Toda População Acima de 18 Anos. Available online: https://www.gov.br/saude/pt-br/assuntos/noticias/2023/abril/ministerio-da-saude-amplia-vacinacao-com-dose-de-reforco-bivalente-contra-covid-19-para-toda-populacao-acima-de-18-anos (accessed on 7 August 2023).


{kind=link}
{kind=link}
{kind=link}
| Population Estimation n * | Vaccinated n (%) ** | Tested Residents n (%) *** | |
|---|---|---|---|
| Group A | |||
| Gracho Cardoso | 5.818 | 4.538 (78) | 50 (12.32) |
| Cumbe | 3.987 | 3.070 (77) | 61 (10.76) |
| Moita Bonita | 11.335 | 8.728 (77) | 39 (14.39) |
| Muribeca | 7.625 | 5.719 (75) | 43 (13.54) |
| Macambira | 6.919 | 5.189 (75) | 65 (10.36) |
| Itabi | 4.903 | 3.677 (75) | 57 (11.29) |
| Nossa Senhora de Lourdes | 6.483 | 4.862 (75) | 47 (12.81) |
| Group B | |||
| Japoatã | 13.434 | 8.060 (60) | 54 (11.76) |
| Pedrinhas | 9.602 | 5.665 (59) | 34 (15.58) |
| Brejo Grande | 8.309 | 4.902 (59) | 71 (9.74) |
| Riachuelo | 10.213 | 5.923 (58) | 51 (12.18) |
| Tomar do Geru | 13.536 | 7.715 (57) | 66 (10.28) |
| Poço Redondo | 34.775 | 19.822 (57) | 51 (12.22) |
| Carmópolis | 16.634 | 9.315 (56) | 77 (9.22) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, R.S.; Barreto, M.d.S.; Silva, E.E.D.; Silva, B.S.d.; Jesus, P.C.d.; Silva, D.M.R.R.; Moura, P.H.M.; Souza, J.B.d.; Santos, L.M.M.d.; Guimarães, A.G.; et al. COVID-19 Crisis in Brazil: Post-Vaccination Seroprevalence and Infection in More and Less Vaccinated Municipalities in a Northeastern State. Life 2024, 14, 94. https://doi.org/10.3390/life14010094
Santos RS, Barreto MdS, Silva EED, Silva BSd, Jesus PCd, Silva DMRR, Moura PHM, Souza JBd, Santos LMMd, Guimarães AG, et al. COVID-19 Crisis in Brazil: Post-Vaccination Seroprevalence and Infection in More and Less Vaccinated Municipalities in a Northeastern State. Life. 2024; 14(1):94. https://doi.org/10.3390/life14010094
Chicago/Turabian StyleSantos, Ronaldy Santana, Marina dos Santos Barreto, Eloia Emanuelly Dias Silva, Beatriz Soares da Silva, Pamela Chaves de Jesus, Deise Maria Rego Rodrigues Silva, Pedro Henrique Macedo Moura, Jessiane Bispo de Souza, Leticia Milena Machado dos Santos, Adriana Gibara Guimarães, and et al. 2024. "COVID-19 Crisis in Brazil: Post-Vaccination Seroprevalence and Infection in More and Less Vaccinated Municipalities in a Northeastern State" Life 14, no. 1: 94. https://doi.org/10.3390/life14010094
APA StyleSantos, R. S., Barreto, M. d. S., Silva, E. E. D., Silva, B. S. d., Jesus, P. C. d., Silva, D. M. R. R., Moura, P. H. M., Souza, J. B. d., Santos, L. M. M. d., Guimarães, A. G., Santana, L. A. d. M., & Borges, L. P. (2024). COVID-19 Crisis in Brazil: Post-Vaccination Seroprevalence and Infection in More and Less Vaccinated Municipalities in a Northeastern State. Life, 14(1), 94. https://doi.org/10.3390/life14010094