
Evidence-Based Approaches to Anticoagulation in Reconstructive Microsurgery—A Systematic Literature Review

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
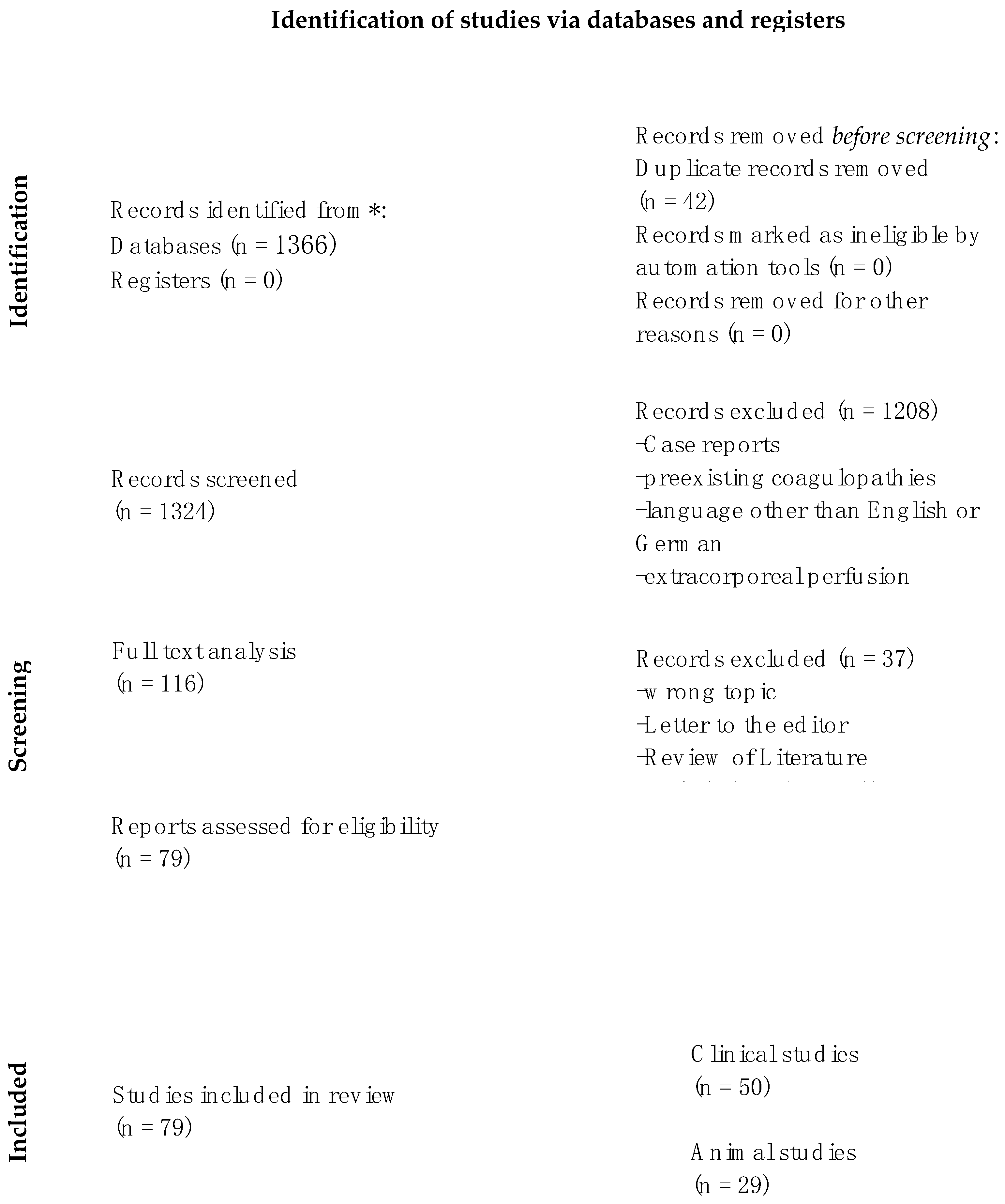
3.1. Article Screening
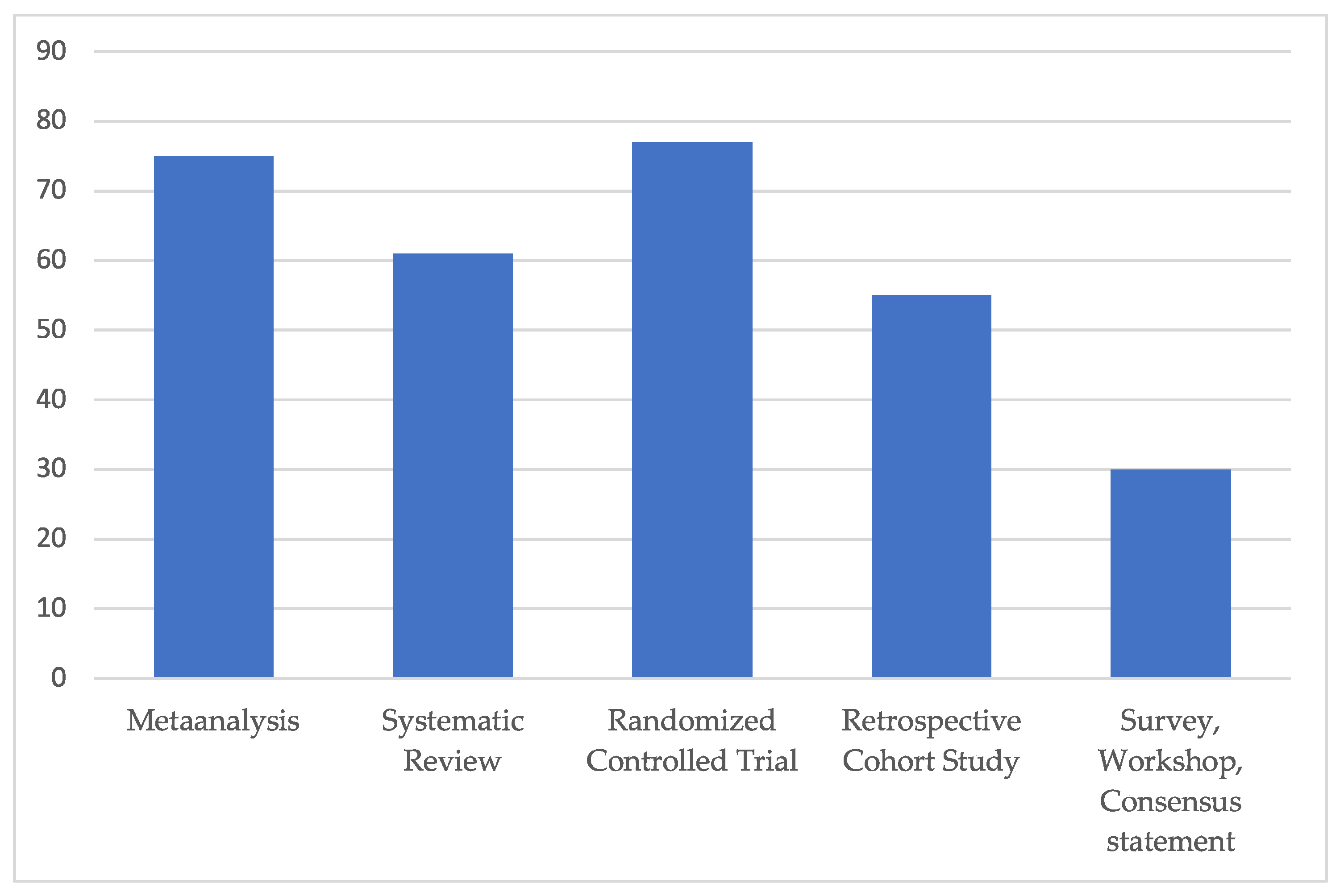
3.2. Study Types
3.2.1. Clinical Studies (Table S1)
Systematic Reviews
Metaanalyses
Prospective Randomized Clinical Trials (RCT)
Prospective Cohort Study or Case Series
Retrospective Cohort Study
Others
3.2.2. Animal Studies (Table S2)
Prospective Cohort Studies/Randomized-Controlled Trials
- (1)
- Systemic administration
- (2)
- Irrigation/intraluminal and topical administration
- (3)
- Other routes of administration
4. Discussion
4.1. Clinical Studies
4.2. Animal Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sigaux, N.; Philouze, P.; Boucher, F.; Jacquemart, M.; Frobert, P.; Breton, P. Efficacy of the Postoperative Management after Microsurgical Free Tissue Transfer. J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 173–177. [Google Scholar] [CrossRef]
- Ahmad, F.I.; Gerecci, D.; Gonzalez, J.D.; Peck, J.J.; Wax, M.K. The Role of Postoperative Hematoma on Free Flap Compromise. Laryngoscope 2015, 125, 1811–1815. [Google Scholar] [CrossRef]
- Durnig, P.; Meier, M.; Reichert, B. Monitoring of Free Flaps and Replantations. Status Quo in German-Speaking Microsurgery Units. Handchir. Mikrochir. Plast. Chir. 2008, 40, 392–399. [Google Scholar] [CrossRef]
- Xipoleas, G.; Levine, E.; Silver, L.; Koch, R.M.; Taub, P.J. A Survey of Microvascular Protocols for Lower-Extremity Free Tissue Transfer I: Perioperative Anticoagulation. Ann. Plast. Surg. 2007, 59, 311–315. [Google Scholar] [CrossRef]
- Motakef, S.; Mountziaris, P.M.; Ismail, I.K.; Agag, R.L.; Patel, A. Emerging Paradigms in Perioperative Management for Microsurgical Free Tissue Transfer: Review of the Literature and Evidence-Based Guidelines. Plast. Reconstr. Surg. 2015, 135, 290–299. [Google Scholar] [CrossRef]
- Keith, J.N.; Chong, T.W.; Davar, D.; Moore, A.G.; Morris, A.; Gimbel, M.L. The Timing of Preoperative Prophylactic Low-Molecular-Weight Heparin Administration in Breast Reconstruction. Plast. Reconstr. Surg. 2013, 132, 279–284. [Google Scholar] [CrossRef]
- Lighthall, J.G.; Cain, R.; Ghanem, T.A.; Wax, M.K. Effect of Postoperative Aspirin on Outcomes in Microvascular Free Tissue Transfer Surgery. Otolaryngol.-Head. Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head. Neck Surg. 2013, 148, 40–46. [Google Scholar] [CrossRef]
- Chien, W.; Varvares, M.A.; Hadlock, T.; Cheney, M.; Deschler, D.G. Effects of Aspirin and Low-Dose Heparin in Head and Neck Reconstruction Using Microvascular Free Flaps. Laryngoscope 2005, 115, 973–976. [Google Scholar] [CrossRef]
- Karimi, E.; Ardestani, S.H.; Jafari, M.; Hagh, A.B. Testing a New Anticoagulation Method for Free Flap Reconstruction of Head and Neck Cancers. Clin. Exp. Otorhinolaryngol. 2016, 9, 370–373. [Google Scholar] [CrossRef]
- Disa, J.J.; Polvora, V.P.; Pusic, A.L.; Singh, B.; Cordeiro, P.G. Dextran-Related Complications in Head and Neck Microsurgery: Do the Benefits Outweigh the Risks? A Prospective Randomized Analysis. Plast. Reconstr. Surg. 2003, 112, 1534–1539. [Google Scholar] [CrossRef]
- Chen, C.M.; Ashjian, P.; Disa, J.J.; Cordeiro, P.G.; Pusic, A.L.; Mehrara, B.J. Is the Use of Intraoperative Heparin Safe? Plast. Reconstr. Surg. 2008, 121, 49e–53e. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Cevik, J.; Middleton, R.; Ramakrishnan, A.; Cabalag, M. Rationalizing Post-Operative Prophylactic Anticoagulation in Reconstructive Head and Neck Cancer Patients: A Review. ANZ J. Surg. 2021, 91, 2610–2616. [Google Scholar] [CrossRef]
- Couteau, C.; Rem, K.; Guillier, D.; Moris, V.; Revol, M.; Cristofari, S. Improving Free-Flap Survival Using Intra-Operative Heparin: Ritualistic Practice or Evidence-Base Medicine? A Systematic Review. Ann. Chir. Plast. Esthet. 2018, 63, e1–e5. [Google Scholar] [CrossRef]
- Lin, P.-T.; Wang, S.-H.; Chi, C.-C. Low Molecular Weight Heparin for Prevention of Microvascular Occlusion in Digital Replantation. Cochrane Database Syst. Rev. 2020, 4, CD009894. [Google Scholar] [CrossRef]
- Liu, J.; Shi, Q.; Yang, S.; Liu, B.; Guo, B.; Xu, J. Does Postoperative Anticoagulation Therapy Lead to a Higher Success Rate for Microvascular Free-Tissue Transfer in the Head and Neck? A Systematic Review and Meta-Analysis. J. Reconstr. Microsurg. 2018, 34, 087–094. [Google Scholar] [CrossRef]
- Pršić, A.; Kiwanuka, E.; Caterson, S.A.; Caterson, E.J. Anticoagulants and Statins As Pharmacological Agents in Free Flap Surgery: Current Rationale. Eplasty 2015, 15, e51. [Google Scholar]
- Trull, B.; Zhang, Z.; Boyd, K.; Allen, M.; Zhang, J. Canadian Postoperative Dependency Protocols Following Lower Limb Microvascular Reconstruction: A National Survey and Literature Review. Plast. Surg. 2021, 29, 122–127. [Google Scholar] [CrossRef]
- Abraham, M.; Badhey, A.; Hu, S.; Kadakia, S.; Rasamny, J.K.; Moscatello, A.; Ducic, Y. Thromboprophylaxis in Head and Neck Microvascular Reconstruction. Craniomaxillofacial Trauma Reconstr. 2018, 11, 85–95. [Google Scholar] [CrossRef]
- Spiegel, J.H.; Polat, J.K. Microvascular Flap Reconstruction by Otolaryngologists: Prevalence, Postoperative Care, and Monitoring Techniques. Laryngoscope 2007, 117, 485–490. [Google Scholar] [CrossRef]
- Pan, X.; Chen, G.; Shao, H.; Han, C.; Zhang, L.; Zhi, L. Effect of Heparin on Prevention of Flap Loss in Microsurgical Free Flap Transfer: A Meta-Analysis. PLoS ONE 2014, 9, e95111. [Google Scholar] [CrossRef] [PubMed]
- Swartz, J.E.; Aarts, M.C.J.; Swart, K.M.A.; Disa, J.J.; Gerressen, M.; Kuo, Y.-R.; Wax, M.K.; Grolman, W.; Braunius, W.W. The Value of Postoperative Anticoagulants to Improve Flap Survival in the Free Radial Forearm Flap: A Systematic Review and Retrospective Multicentre Analysis. Clin. Otolaryngol. 2015, 40, 600–609. [Google Scholar] [CrossRef]
- Jones, S.J.; Scott, D.A.; Watson, R.; Morrison, W.A. Milrinone Does Not Improve Free Flap Survival in Microvascular Surgery. Anaesth. Intensive Care 2007, 35, 720–725. [Google Scholar] [CrossRef]
- Khouri, R.K.; Sherman, R.; Buncke, H.J.; Feller, A.M.; Hovius, S.; Benes, C.O.; Ingram, D.M.; Natarajan, N.N.; Sherman, J.W.; Yeramian, P.D.; et al. A Phase II Trial of Intraluminal Irrigation with Recombinant Human Tissue Factor Pathway Inhibitor to Prevent Thrombosis in Free Flap Surgery. Plast. Reconstr. Surg. 2001, 107, 408–415; discussion 416–418. [Google Scholar] [CrossRef]
- Furnas, H.J.; Lineaweaver, W.; Buncke, H.J. Blood Loss Associated with Anticoagulation in Patients with Replanted Digits. J. Hand Surg. 1992, 17, 226–229. [Google Scholar] [CrossRef]
- Fukui, A.; Maeda, M.; Sempuku, T.; Tamai, S.; Mizumoto, S.; Inada, Y. Continuous Local Intra-Arterial Infusion of Anticoagulants for Digit Replantation and Treatment of Damaged Arteries. J. Reconstr. Microsurg. 1989, 5, 127–136. [Google Scholar] [CrossRef]
- Saito, A.; Sawaizumi, M.; Imai, T.; Matsumoto, S. Continuous Local Intraarterial Infusion of Anticoagulants for Microvascular Free Tissue Transfer in Primary Reconstruction of the Lower Limb Following Resection of Sarcoma. Microsurgery 2010, 30, 376–379. [Google Scholar] [CrossRef]
- Başaran, B.; Ünsaler, S.; Kesimli, M.C.; Aslan, İ. Free Flap Reconstruction of the Head and Neck Region: A Series of 127 Flaps Performed by Otolaryngologists. Turk. Arch. Otorhinolaryngol. 2021, 59, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Efanov, J.I.; Khriguian, J.; Cassier, S.; Boghossian, E.; Harris, P.G.; Bou-Merhi, J.; Danino, M.A. Duration and Cessation Characteristics of Heparinization after Finger Replantation: A Retrospective Analysis of Outcomes. Microsurgery 2018, 38, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Eley, K.A.; Parker, R.J.; Watt-Smith, S.R. Low Molecular Weight Heparin in Patients Undergoing Free Tissue Transfer Following Head and Neck Ablative Surgery: Review of Efficacy and Associated Complications. Br. J. Oral Maxillofac. Surg. 2013, 51, 610–614. [Google Scholar] [CrossRef]
- Enajat, M.; Aziz Mohammadi, M.; Debeij, J.; van der Hulst, R.; Mureau, M. Effect of Acetylsalicylic Acid on Microvascular Thrombosis in Autologous Breast Reconstruction. J. Reconstr. Microsurg. 2013, 30, 065–070. [Google Scholar] [CrossRef] [PubMed]
- Jayaprasad, K.; Mathew, J.; Thankappan, K.; Sharma, M.; Duraisamy, S.; Rajan, S.; Paul, J.; Iyer, S. Safety and Efficacy of Low Molecular Weight Dextran (Dextran 40) in Head and Neck Free Flap Reconstruction. J. Reconstr. Microsurg. 2013, 29, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Pugh, C.M.; Dennis, R.H.; Massac, E.A. Evaluation of Intraoperative Anticoagulants in Microvascular Free-Flap Surgery. J. Natl. Med. Assoc. 1996, 88, 655–657. [Google Scholar] [PubMed]
- Senchenkov, A.; Lemaine, V.; Tran, N.V. Management of Perioperative Microvascular Thrombotic Complications—The Use of Multiagent Anticoagulation Algorithm in 395 Consecutive Free Flaps. J. Plast. Reconstr. Aesthet. Surg. 2015, 68, 1293–1303. [Google Scholar] [CrossRef]
- Yii, N.W.; Evans, G.R.D.; Miller, M.J.; Reece, G.P.; Langstein, H.; Chang, D.; Kroll, S.S.; Wang, B.; Robb, G.L. Thrombolytic Therapy:: What Is Its Role in Free Flap Salvage? Ann. Plast. Surg. 2001, 46, 601–604. [Google Scholar] [CrossRef]
- Bassiri-Tehrani, B.; Karanetz, I.; Bernik, S.F.; Dec, W.; Lehman, J.C.; Lerman, O.Z. The Timing of Chemoprophylaxis in Autologous Microsurgical Breast Reconstruction: Plast. Reconstr. Surg. 2018, 142, 1116–1123. [Google Scholar] [CrossRef]
- Filipan, D.; Dediol, E.; Blivajs, I.; Milic, M. The Effects of Dextran on Postoperative Thrombosis and Hemodilution in Microvascular Head and Neck Reconstruction. Ann. Plast. Surg. 2020, 85, 38–42. [Google Scholar] [CrossRef]
- Numajiri, T.; Sowa, Y.; Nishino, K.; Arai, A.; Tsujikawa, T.; Ikebuchi, K.; Nakano, H.; Sakaguchi, H. Use of Systemic Low-Dose Unfractionated Heparin in Microvascular Head and Neck Reconstruction: Influence in Free-Flap Outcomes. J. Plast. Surg. Hand Surg. 2016, 50, 135–141. [Google Scholar] [CrossRef]
- Okochi, M.; Komuro, Y.; Ueda, K. Selective and Continuous Transarterial Heparin Infusion: Postmicrosurgical Therapy of Lower Leg Reconstruction for Cases with Recipient Artery Damage. World J. Plast. Surg. 2019, 8, 298–304. [Google Scholar]
- Riva, F.M.G.; Chen, Y.-C.; Tan, N.-C.; Lin, P.-Y.; Tsai, Y.-T.; Chang, H.-W.; Kuo, Y.-R. The Outcome of Prostaglandin-E1 and Dextran-40 Compared to No Antithrombotic Therapy in Head and Neck Free Tissue Transfer: Analysis of 1,351 Cases in a Single Center. Microsurgery 2012, 32, 339–343. [Google Scholar] [CrossRef]
- Labosky, D.A. Selective Heparinization of Venous Anastomosis in Latissimus Dorsi Free Flaps to Cover Lower-Extremity Soft-Tissue Defects. Microsurgery 1991, 12, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.T.; Jeon, B.-J.; Lim, S.-Y.; Pyon, J.-K.; Bang, S.-I.; Oh, K.-S.; Mun, G.-H. The Effects of Ketorolac on Microvascular Thrombosis in Lower Extremity Reconstruction: Plast. Reconstr. Surg. 2012, 129, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Mirzabeigi, M.N.; Wang, T.; Kovach, S.J.; Taylor, J.A.; Serletti, J.M.; Wu, L.C. Free Flap Take-Back Following Postoperative Microvascular Compromise: Predicting Salvage versus Failure. Plast. Reconstr. Surg. 2012, 130, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Tamai, S.; Tatsumi, Y.; Shimizu, T.; Hori, Y.; Okuda, H.; Takita, T.; Sakamoto, H.; Fukui, A. Traumatic Amputation of Digits: The Fate of Remaining Blood. An Experimental and Clinical Study. J. Hand Surg. 1977, 2, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.L.; Eadie, P.A.; Orr, D.; Al-Rawi, M.; O’Donnell, M.; Lawlor, D. Prospective Evaluation of Outcome Measures in Free-Flap Surgery. J. Reconstr. Microsurg. 2004, 20, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Davies, D.M. A World Survey of Anticoagulation Practice in Clinical Microvascular Surgery. Br. J. Plast. Surg. 1982, 35, 96–99. [Google Scholar] [CrossRef]
- Kremer, T.; Bauer, M.; Zahn, P.; Wallner, C.; Fuchs, P.; Horch, R.E.; Schaefer, D.J.; Bader, R.D.; Lehnhardt, M.; Reichert, B.; et al. Perioperatives Management in der Mikrochirurgie–Konsensus-Statement der Deutschsprachigen Arbeitsgemeinschaft für Mikrochirurgie der peripheren Nerven und Gefäße. Handchir. Mikrochir. Plast. Chir. 2016, 48, 205–211. [Google Scholar] [CrossRef]
- Boyko, T.; Fontenot, A.; Manisundaram, A.; Burke, M. Current Practices in Peri-Operative Free Flap Anticoagulation and Post-Operative Monitoring of Microsurgeons in USA. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2019, 72, 2064–2094. [Google Scholar] [CrossRef]
- Rendenbach, C.; Hölterhoff, N.; Hischke, S.; Kreutzer, K.; Smeets, R.; Assaf, A.T.; Heiland, M.; Wikner, J. Free Flap Surgery in Europe: An Interdisciplinary Survey. Int. J. Oral Maxillofac. Surg. 2018, 47, 676–682. [Google Scholar] [CrossRef]
- Schmitz, M.; Riss, R.; Kneser, U.; Jokuszies, A.; Harder, Y.; Beier, J.P.; Schäfer, D.J.; Vogt, P.M.; Fansa, H.; Andree, C.; et al. Perioperative coagulation management in microsurgery: Report of the consensus workshops in the course of the 31st and 32nd Annual Meeting of the German-language Working Group for microsurgery of the peripheral nerves and vessels (DAM) November 2009 in Erlangen and November 2010 in Basel. Handchir. Mikrochir. Plast. Chir. 2011, 43, 376–383. [Google Scholar] [CrossRef]
- Ridha, H.; Jallali, N.; Butler, P.E. The Use of Dextran Post Free Tissue Transfer. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2006, 59, 951–954. [Google Scholar] [CrossRef] [PubMed]
- Siegel, D.B. Use of Anticoagulants in Replantation and Elective Microsurgery. Microsurgery 1991, 12, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Pederson, W.C. Clinical Use of Anticoagulants Following Free Tissue Transfer Surgery. J. Hand Surg. 2008, 33, 1435–1436. [Google Scholar] [CrossRef] [PubMed]
- Abdelfattah, U.; Elbanoby, T.; Kim, E.N.; Park, E.J.; Suh, H.P.; Hong, J.P.J. Effect of Simvastatin Use in Free Tissue Transfer: An Experimental Study in a Rat Epigastric Free Flap Model. J. Reconstr. Microsurg. 2020, 36, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Chung, T.L.; Pumplin, D.W.; Holton, L.H., 3rd; Taylor, J.A.; Rodriguez, E.D.; Silverman, R.P. Prevention of Microsurgical Anastomotic Thrombosis Using Aspirin, Heparin, and the Glycoprotein IIb/IIIa Inhibitor Tirofiban. Plast. Reconstr. Surg. 2007, 120, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Cox, G.W.; Runnels, S.; Hsu, H.S.; Das, S.K. A Comparison of Heparinised Saline Irrigation Solutions in a Model of Microvascular Thrombosis. Br. J. Plast. Surg. 1992, 45, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Engrav, L.H.; Benjamin, C.I.; Crandall, H.; Perry, J.F. Experimental Effects of Heparin or Magnesium Sulfate on the Patency of Microvascular Anastomoses. Plast. Reconstr. Surg. 1975, 55, 618–619. [Google Scholar] [CrossRef]
- Ezzat, W.H.; Dahl, J.P.; Luginbuhl, A.; Gordin, E.; Krein, H.; Heffelfinger, R.N. Recombinant Human Tissue Factor Pathway Inhibitor Prevents Thrombosis in a Venous Tuck Model. Laryngoscope 2010, 120, 2172–2176. [Google Scholar] [CrossRef]
- Greenberg, B.M.; Masem, M.; Wang, Y.X.; Rubin, P.; May, J.W.J. Efficacy of Intraarterial Heparin in Maintaining Microvascular Patency: An Experimental Model. Plast. Reconstr. Surg. 1991, 87, 933–940. [Google Scholar] [CrossRef]
- Lan, M.; lu Li, X.; Cooley, B.; Gould, J. Microvascular Salvage Procedures with Adjuvant Antithrombotic Therapy for Restitution of Patency in a Rat Model. J. Reconstr. Microsurg. 1992, 8, 201–205. [Google Scholar] [CrossRef]
- Murthy, P.; Riesberg, M.V.; Hart, S.; Bustillo, A.; Duque, C.S.; Said, S.; Civantos, F.J. Efficacy of Perioperative Thromboprophylactic Agents in the Maintenance of Anastamotic Patency and Survival of Rat Microvascular Free Groin Flaps. Otolaryngol.-Head. Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head. Neck Surg. 2003, 129, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Ozbeck, M.R.; Brown, D.M.; Deune, E.G.; Lantieri, L.A.; Kania, N.M.; Pasia, E.N.; Cooley, B.C.; Wun, T.C.; Khouri, R.K. Topical Tissue Factor Pathway Inhibitor Improves Free-Flap Survival in a Model Simulating Free-Flap Errors. J. Reconstr. Microsurg. 1995, 11, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Ritter, E.F.; Cronan, J.C.; Rudner, A.M.; Serafin, D.; Klitzman, B. Improved Microsurgical Anastomotic Patency with Low Molecular Weight Heparin. J. Reconstr. Microsurg. 1998, 14, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Rumbolo, P.M.; Cooley, B.C.; Hanel, D.P.; Gould, J.S. Comparison of the Influence of Intralumenal Irrigation Solutions on Free Flap Survival. Microsurgery 1992, 13, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Vlastou, C.; Earle, A.S. Intraoperative Heparin in Replantation Surgery—An Experimental Study. Ann. Plast. Surg. 1983, 10, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Wallmichrath, J.; Knab, R.; Baumeister, R.G.H.; Volkmer, E.; Giunta, R.E.; Frick, A. Protective Effects of Antithrombin on Free Groin Flaps after Secondary Venous Stasis in the Rat Model. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 707–711. [Google Scholar] [CrossRef]
- Yates, Y.J.; Farias, C.L.; Kazmier, F.R.; Puckett, C.L.; Concannon, M.J. The Effect of Tirofiban on Microvascular Thrombosis: Crush Model. Plast. Reconstr. Surg. 2005, 116, 205–208. [Google Scholar] [CrossRef]
- Greenberg, B.M.; Masem, M.; May, J.W.J. Therapeutic Value of Intravenous Heparin in Microvascular Surgery: An Experimental Vascular Thrombosis Study. Plast. Reconstr. Surg. 1988, 82, 463–472. [Google Scholar] [CrossRef]
- Kirschner, R.E.; Xu, J.; Fyfe, B.; Chang, B.; Bucky, L.P. Salvage of Free Flaps after Secondary Venous Ischemia by Local Delivery of Heparin. Ann. Plast. Surg. 1999, 42, 521–527; discussion 527–528. [Google Scholar] [CrossRef]
- Korompilias, A.V.; Chen, L.E.; Seaber, A.V.; Urbaniak, J.R. Antithrombotic Potencies of Enoxaparin in Microvascular Surgery: Influence of Dose and Administration Methods on Patency Rate of Crushed Arterial Anastomoses. J. Hand Surg. 1997, 22, 540–546. [Google Scholar] [CrossRef]
- Li, X.; Cooley, B.C.; Fowler, J.D.; Gould, J.S. Intravascular Heparin Protects Muscle Flaps from Ischemia/Reperfusion Injury. Microsurgery 1995, 16, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Ramelli, E.; Durry, A.; Ruffenach, L.; Bruant-Rodier, C.; Bodin, F. Decrease of Thrombosis in Microsurgical Anastomoses: The Use of Intraoperative Pure Intraluminal Unfractionated Heparin. J. Reconstr. Microsurg. 2020, 36, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Hudson, D.A.; Engelbrecht, G.; Duminy, F.J. Another Method to Prevent Venous Thrombosis in Microsurgery: An in Situ Venous Catheter: Plast. Reconstr. Surg. 2000, 105, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, K.; Walenga, J.M.; Liang, M.D.; Fareed, J. Recombinant Hirudin--Initial Observations in Reconstructive Microsurgery. Haemostasis 1991, 21 (Suppl. S1), 168–171. [Google Scholar] [CrossRef] [PubMed]
- Reichel, C.A.; Croll, G.H.; Puckett, C.L. A Comparison of Irrigation Solutions for Microanastomoses. J. Hand Surg. 1988, 13, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, S. The Importance of Topical Heparin in Microvascular Anastomoses: A Study in the Rat. Br. J. Plast. Surg. 1980, 33, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Wolfort, S.F.; Angel, M.F.; Knight, K.R.; Amiss, L.R.; Morgan, R.F. The Beneficial Effect of Dextran on Anastomotic Patency and Flap Survival in a Strongly Thrombogenic Model. J. Reconstr. Microsurg. 1992, 8, 375–378. [Google Scholar] [CrossRef]
- Lepore, D.A.; Knight, K.R.; Bhattacharya, S.; Ritz, M.; Robbins, S.P.; Sieg, P.; Morrison, W.A.; O’Brien, B.M. Drug Mixture Which Improves Survival of Ischemic Rabbit Epigastric Skin Flaps. Microsurgery 1994, 15, 685–692. [Google Scholar] [CrossRef]
- Maeda, M.; Fukui, A.; Tamai, S. Combined Therapy with Antithrombotic Agents and Radical Scavengers for Reperfusion Injury of Flaps. J. Reconstr. Microsurg. 1991, 7, 233–243. [Google Scholar] [CrossRef]
- Farina, J.A.J.; Piccinato, C.E.; Campos, A.D.; Rossi, M.A. Comparative Study of Isovolemic Hemodilution with 3% Albumin, Dextran-40, and Prophylactic Enoxaparin (LMWH) on Thrombus Formation at Venous Microanastomosis in Rats. Microsurgery 2006, 26, 456–464. [Google Scholar] [CrossRef]
- Mayer, B.; Kretschmer, R.; Gunzenhäusser, E. Interposition connectors with heparin coating for vascular anastomosis of microsurgical tissue flaps. Laryngorhinootologie 1992, 71, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Ashjian, P.; Chen, C.M.; Pusic, A.; Disa, J.J.; Cordeiro, P.G.; Mehrara, B.J. The Effect of Postoperative Anticoagulation on Microvascular Thrombosis. Ann. Plast. Surg. 2007, 59, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Bashir, M.M.; Yousaf, N.; Khan, F.A. The Outcome of Microvascular Free Flap Surgery with or without the Use of Postoperative Heparin. J. Coll. Physicians Surg.-Pak. JCPSP 2014, 24, 412–415. [Google Scholar] [PubMed]
- Fagin, A.P.; Petrisor, D. Controversies in Microvascular Maxillofacial Reconstruction. Oral Maxillofac. Surg. Clin. N. Am. 2017, 29, 415–424. [Google Scholar] [CrossRef]
- Jallali, N. Dextrans in Microsurgery: A Review. Microsurgery 2003, 23, 78–80. [Google Scholar] [CrossRef]
- Salgado, C.J.; Chim, H.; Schoenoff, S.; Mardini, S. Postoperative Care and Monitoring of the Reconstructed Head and Neck Patient. Semin. Plast. Surg. 2010, 24, 281–287. [Google Scholar] [CrossRef]
- Strebel, N.; Prins, M.; Agnelli, G.; Büller, H.R. Preoperative or Postoperative Start of Prophylaxis for Venous Thromboembolism with Low-Molecular-Weight Heparin in Elective Hip Surgery? Arch. Intern. Med. 2002, 162, 1451–1456. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Characteristics |
|
|
| Intervention |
|
|
| Outcomes |
| |
| Study design |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biermann, N.; Chak, J.C.; Wiesmeier, A.; Klein, S.M.; Ruewe, M.; Spoerl, S.; Kruppa, P.; Prantl, L.; Anker, A.M. Evidence-Based Approaches to Anticoagulation in Reconstructive Microsurgery—A Systematic Literature Review. Life 2024, 14, 82. https://doi.org/10.3390/life14010082
Biermann N, Chak JC, Wiesmeier A, Klein SM, Ruewe M, Spoerl S, Kruppa P, Prantl L, Anker AM. Evidence-Based Approaches to Anticoagulation in Reconstructive Microsurgery—A Systematic Literature Review. Life. 2024; 14(1):82. https://doi.org/10.3390/life14010082
Chicago/Turabian StyleBiermann, Niklas, Juy Chi Chak, Anna Wiesmeier, Silvan M. Klein, Marc Ruewe, Steffen Spoerl, Philipp Kruppa, Lukas Prantl, and Alexandra M. Anker. 2024. "Evidence-Based Approaches to Anticoagulation in Reconstructive Microsurgery—A Systematic Literature Review" Life 14, no. 1: 82. https://doi.org/10.3390/life14010082
APA StyleBiermann, N., Chak, J. C., Wiesmeier, A., Klein, S. M., Ruewe, M., Spoerl, S., Kruppa, P., Prantl, L., & Anker, A. M. (2024). Evidence-Based Approaches to Anticoagulation in Reconstructive Microsurgery—A Systematic Literature Review. Life, 14(1), 82. https://doi.org/10.3390/life14010082