
Management of Cerebrospinal Fluid Leakage after Microvascular Decompression Surgery: Clinical Strategy


Abstract
1. Introduction
2. Patients and Methods
3. Results
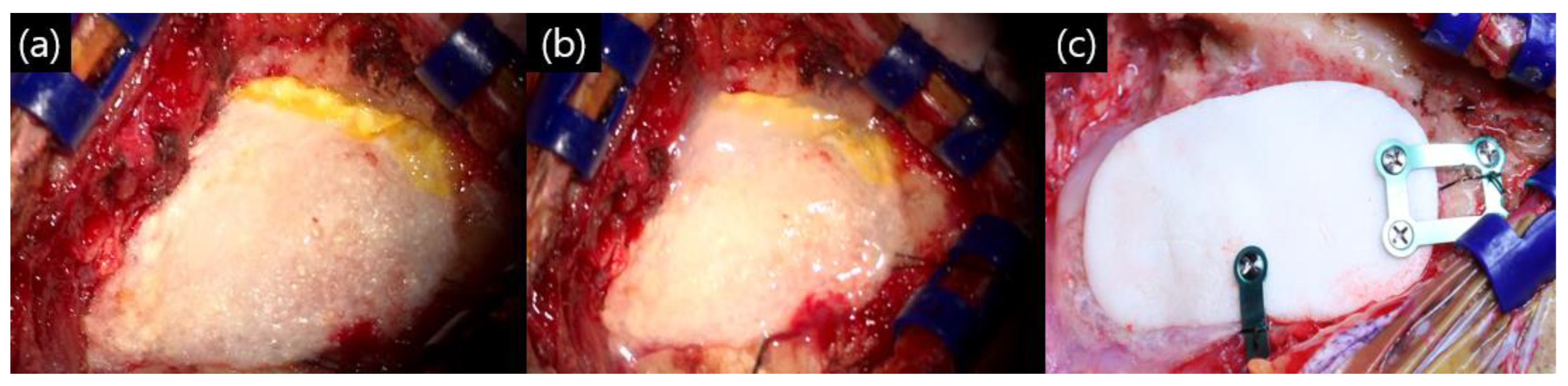
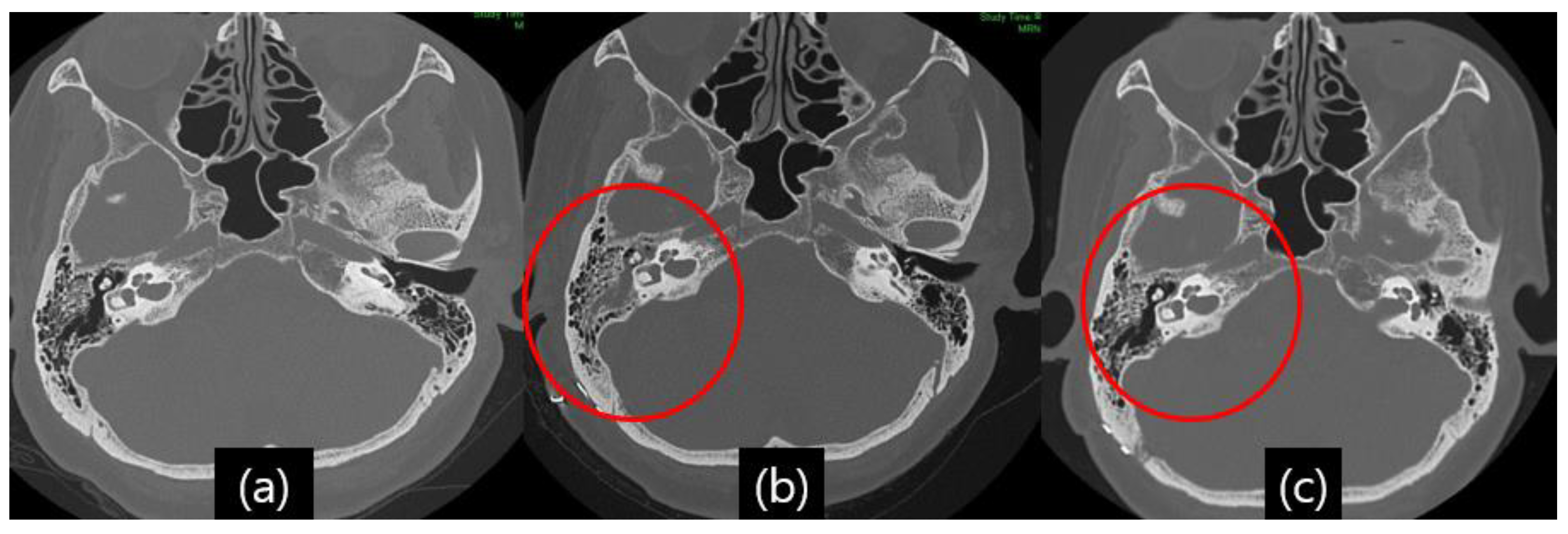
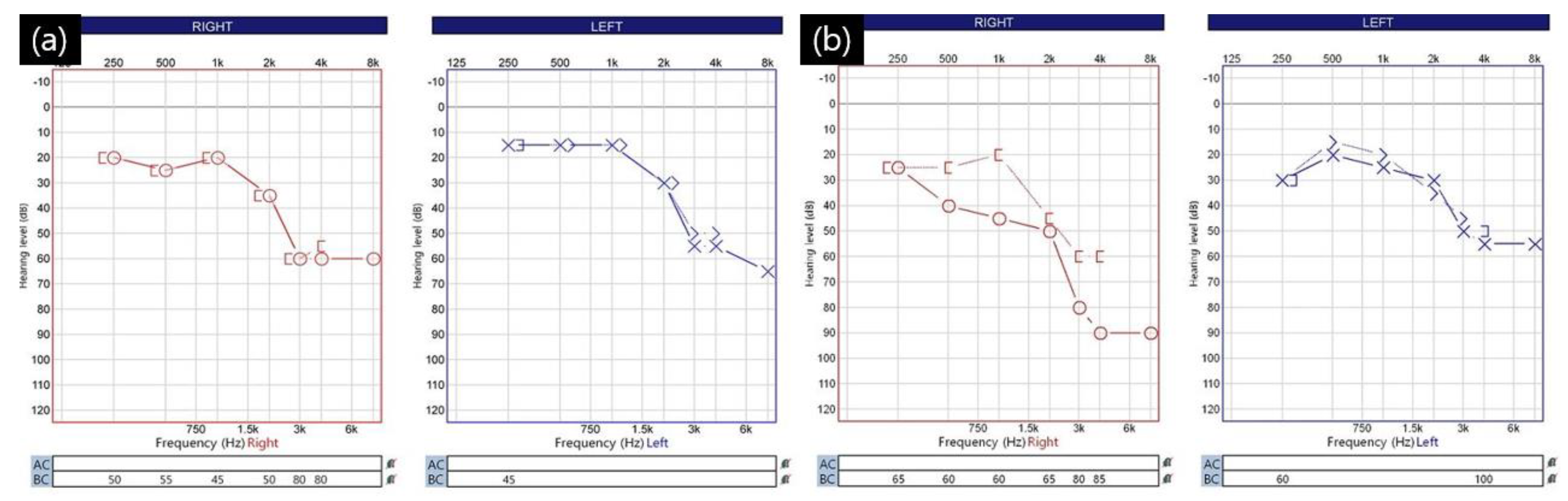
Illustrative Case
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abuzayed, B.; Kafadar, A.M.; Oguzoglu, S.A.; Canbaz, B.; Kaynar, M.Y. Duraplasty using autologous fascia lata reenforced by on-site pedicled muscle flap: Technical note. J. Craniofacial Surg. 2009, 20, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Caltabiano, G.A.; Viglianesi, A.; Bellomia, D.; Chiaramonte, R.; Pero, G.; Chiaramonte, I. Spontaneous temporal cerebrospinal fluid leak. A case report and literature review. Neuroradiol. J. 2010, 23, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Altaf, I.; Vohra, A.H.; Shams, S. Management of Cerebrospinal Fluid Leak following Posterior Cranial Fossa Surgery. Pak. J. Med. Sci. 2016, 32, 1439–1443. [Google Scholar] [CrossRef] [PubMed]
- Grotenhuis, J.A. Costs of postoperative cerebrospinal fluid leakage: 1-year, retrospective analysis of 412 consecutive nontrauma cases. Surg. Neurol. 2005, 64, 490–493, discussion 493–494. [Google Scholar] [CrossRef]
- Khan, S.A.; Laulloo, A.; Vats, A.; Nath, F. Microvascular decompression: Incidence and prevention of postoperative CSF leakage in a consecutive series of 134 patients. Br. J. Neurosurg. 2020, 34, 416–418. [Google Scholar] [CrossRef]
- Venable, G.T.; Roberts, M.L.; Lee, R.P.; Michael, L.M., 2nd. Primary Dural Closure for Retrosigmoid Approaches. J. Neurol. Surg. B Skull Base 2018, 79, 330–334. [Google Scholar] [CrossRef]
- Stoker, M.A.; Forbes, J.A.; Hanif, R.; Cooper, C.; Nian, H.; Konrad, P.E.; Neimat, J.S. Decreased Rate of CSF Leakage Associated with Complete Reconstruction of Suboccipital Cranial Defects. J. Neurol. Surg. B Skull Base 2012, 73, 281–286. [Google Scholar] [CrossRef]
- Arlt, F.; Trantakis, C.; Krupp, W.; Renner, C.; Winkler, D.; Strauss, G.; Meixensberger, J. Cerebrospinal fluid leak after microsurgical surgery in vestibular schwannomas via retrosigmoidal craniotomy. Neurol. Res. 2011, 33, 947–952. [Google Scholar] [CrossRef]
- Sherif, C.; Di Ieva, A.; Gibson, D.; Pakrah-Bodingbauer, B.; Widhalm, G.; Krusche-Mandl, I.; Erdoes, J.; Gilloon, B.; Matula, C. A management algorithm for cerebrospinal fluid leak associated with anterior skull base fractures: Detailed clinical and radiological follow-up. Neurosurg. Rev. 2012, 35, 227–237, discussion 237–228. [Google Scholar] [CrossRef]
- Albu, S.; Florian, I.S.; Bolboaca, S.D. The benefit of early lumbar drain insertion in reducing the length of CSF leak in traumatic rhinorrhea. Clin. Neurol. Neurosurg. 2016, 142, 43–47. [Google Scholar] [CrossRef]
- Barbanti Brodano, G.; Serchi, E.; Babbi, L.; Terzi, S.; Corghi, A.; Gasbarrini, A.; Bandiera, S.; Griffoni, C.; Colangeli, S.; Ghermandi, R.; et al. Is lumbar drainage of postoperative cerebrospinal fluid fistula after spine surgery effective? J. Neurosurg. Sci. 2014, 58, 23–27. [Google Scholar]
- Khan, R.; Sajjad, M.; Khan, A.A.; Ahmad, B.; Ahmad, S.; Mushtaq, M.; Sultan, S.; Iftikhar, O. Comparison of Lumbar Drain Insertion and Conservative Management in the Treatment of Traumatic CSF Rhinorrhoea. J. Ayub Med. Coll. Abbottabad 2019, 31, 441–444. [Google Scholar] [PubMed]
- Mantur, M.; Lukaszewicz-Zajac, M.; Mroczko, B.; Kulakowska, A.; Ganslandt, O.; Kemona, H.; Szmitkowski, M.; Drozdowski, W.; Zimmermann, R.; Kornhuber, J.; et al. Cerebrospinal fluid leakage—Reliable diagnostic methods. Clin. Chim. Acta 2011, 412, 837–840. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.W.; Kim, S.H.; Whang, K. Traumatic Cerebrospinal Fluid Leak: Diagnosis and Management. Korean J. Neurotrauma 2017, 13, 63–67. [Google Scholar] [CrossRef]
- Baker, E.H.; Wood, D.M.; Brennan, A.L.; Baines, D.L.; Philips, B.J. New insights into the glucose oxidase stick test for cerebrospinal fluid rhinorrhoea. Emerg. Med. J. 2005, 22, 556–557. [Google Scholar] [CrossRef]
- Phang, S.Y.; Whitehouse, K.; Lee, L.; Khalil, H.; McArdle, P.; Whitfield, P.C. Management of CSF leak in base of skull fractures in adults. Br. J. Neurosurg. 2016, 30, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Risch, L.; Lisec, I.; Jutzi, M.; Podvinec, M.; Landolt, H.; Huber, A.R. Rapid, accurate and non-invasive detection of cerebrospinal fluid leakage using combined determination of beta-trace protein in secretion and serum. Clin. Chim. Acta 2005, 351, 169–176. [Google Scholar] [CrossRef]
- Eseonu, C.I.; Goodwin, C.R.; Zhou, X.; Theodros, D.; Bender, M.T.; Mathios, D.; Bettegowda, C.; Lim, M. Reduced CSF leak in complete calvarial reconstructions of microvascular decompression craniectomies using calcium phosphate cement. J. Neurosurg. 2015, 123, 1476–1479. [Google Scholar] [CrossRef]
- Park, J.S.; Kong, D.S.; Lee, J.A.; Park, K. Intraoperative management to prevent cerebrospinal fluid leakage after microvascular decompression: Dural closure with a “plugging muscle” method. Neurosurg. Rev. 2007, 30, 139–142, discussion 142. [Google Scholar] [CrossRef]
- Allen, K.P.; Isaacson, B.; Purcell, P.; Kutz, J.W., Jr.; Roland, P.S. Lumbar subarachnoid drainage in cerebrospinal fluid leaks after lateral skull base surgery. Otol. Neurotol. 2011, 32, 1522–1524. [Google Scholar] [CrossRef]
- Mangus, B.D.; Rivas, A.; Yoo, M.J.; Alvarez, J.; Wanna, G.B.; Haynes, D.S.; Bennett, M.L. Management of cerebrospinal fluid leaks after vestibular schwannoma surgery. Otol. Neurotol. 2011, 32, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Hussein, M.; Abdellatif, M. Continuous Lumbar Drainage for the Prevention and Management of Perioperative Cerebrospinal Fluid Leakage. Asian J. Neurosurg. 2019, 14, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, S.K.; Suhail, N.; Mitha, R.; Moazzam, M.; Zahid, N.; Shamim, M.S. Lumbar Drain for Temporary Cerebrospinal Fluid Diversion: Factors Related to the Risks of Complications at a University Hospital. World Neurosurg. 2020, 143, e193–e198. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, A.M.; Shah, A.; Eichberg, D.G.; Komotar, R.J.; Ivan, M. Conservative Management of Post-Operative Cerebrospinal Fluid Leak following Skull Base Surgery: A Pilot Study. Brain Sci. 2022, 12, 152. [Google Scholar] [CrossRef] [PubMed]
- Graf, C.J.; Gross, C.E.; Beck, D.W. Complications of spinal drainage in the management of cerebrospinal fluid fistula. J. Neurosurg. 1981, 54, 392–395. [Google Scholar] [CrossRef]
- Ransom, E.R.; Palmer, J.N.; Kennedy, D.W.; Chiu, A.G. Assessing risk/benefit of lumbar drain use for endoscopic skull-base surgery. Int. Forum Allergy Rhinol. 2011, 1, 173–177. [Google Scholar] [CrossRef]
- Liang, H.; Zhang, L.; Gao, A.; Li, Y.; Jiang, Z.; Hu, F.; Shao, B.; Liu, Y.; Zhang, X. Risk Factors for Infections Related to Lumbar Drainage in Spontaneous Subarachnoid Hemorrhage. Neurocritical Care 2016, 25, 243–249. [Google Scholar] [CrossRef]
- Abuabara, A. Cerebrospinal fluid rhinorrhoea: Diagnosis and management. Med. Oral. Patol. Oral. Cir. Bucal 2007, 12, E397–E400. [Google Scholar]
- Daele, J.J.; Goffart, Y.; Machiels, S. Traumatic, iatrogenic, and spontaneous cerebrospinal fluid (CSF) leak: Endoscopic repair. B-ENT 2011, 7 (Suppl. S17), 47–60. [Google Scholar]
- Coplin, W.M.; Avellino, A.M.; Kim, D.K.; Winn, H.R.; Grady, M.S. Bacterial meningitis associated with lumbar drains: A retrospective cohort study. J. Neurol. Neurosurg. Psychiatry 1999, 67, 468–473. [Google Scholar] [CrossRef]
- Greenberg, B.M.; Williams, M.A. Infectious complications of temporary spinal catheter insertion for diagnosis of adult hydrocephalus and idiopathic intracranial hypertension. Neurosurgery 2008, 62, 431–435, discussion 435–436. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total patients | |
| Median age, years (range) | 58 (19–82) |
| Male:Female | 131:344 |
| Left:Right | 223:252 |
| Suspected CSF leakage | 18 (3.8%) |
| Lumbar drainage catheter insertion | 5 (1.1%) |
| Disease | |
| Trigeminal neuralgia | 47 (9.9%) |
| Hemifacial spasm | 427 (89.9%) |
| * Glossopharyngeal neuralgia | 1 (0.0%) |
| Trigeminal neuralgia | |
| Median age, years (range) | 63.5 (28–80) |
| Male:Female | 16:31 |
| Left:Right | 17:30 |
| Suspected CSF leakage | 1 |
| Lumbar drainage catheter insertion | 0 |
| Hemifacial spasm | |
| Median age, years (range) | 58 (19–82) |
| Male:Female | 115:312 |
| Left:Right | 227:200 |
| Suspected CSF leakage | 17 |
| Lumbar drainage catheter insertion | 5 |
| Patient No | Sex | Age | Disease | Side | Offending Vessel | Mastoid Air Cell Exposure | Symptom from POD | LD from POD | LD Maintained | Hospital Stay | Symptom Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2021-95 | F | 36 | HFS | R | PICA | + | 2 | - | - | 9 | - |
| 2021-97 | F | 39 | HFS | R | AICA | + | 2 | 3 | 5 | 13 | - |
| 2021-106 | M | 69 | HFS | L | AICA-PICA | + | 3 | - | - | 7 | - |
| 2022-6 | M | 63 | HFS | L | AICA-PICA-VA | + | 5 | 6 | 6 | 15 | - |
| 2022-22 | F | 30 | HFS | L | AICA-PICA | + | 2 | 3 | 6 | 13 | - |
| 2022-59 | M | 63 | HFS | L | PICA | + | 3 | - | - | 9 | - |
| 2022-78 | M | 38 | HFS | R | AICA | + | 6 | 8 | 5 | 19 | - |
| 2022-91 | F | 77 | TN | R | Vein | + | 3 | - | - | 13 | - |
| 2022-99 | M | 39 | HFS | L | AICA | + | 3 | - | - | 8 | - |
| 2022-107 | F | 55 | HFS | R | AICA | + | 4 | - | - | 7 | - |
| 2022-117 | F | 56 | HFS | L | AICA | + | 4 | - | - | 8 | - |
| 2022-140 | F | 59 | HFS | R | AICA-VA | + | 5 | 6 | 4 | 14 | - |
| 2022-144 | M | 47 | HFS | L | AICA-PICA-VA | + | 2 | - | - | 8 | - |
| 2022-145 | F | 59 | HFS | R | AICA | + | 3 | - | - | 8 | - |
| 2023-4 | M | 53 | HFS | L | AICA-PICA | + | 3 | - | - | 7 | - |
| 2023-19 | F | 53 | HFS | R | AICA | + | 3 | - | - | 7 | - |
| 2023-30 | F | 69 | HFS | L | VA | + | 3 | - | - | 8 | - |
| 2023-33 | F | 55 | HFS | L | AICA | + | 3 | - | - | 8 | - |
| Suspected CSF leakage (N = 18) | |
| Median age, years (range) | 55 (30–77) |
| Male:Female | 7:11 |
| Left:Right | 10:8 |
| Symptom from POD | 3.3 (2–6) |
| Mastoid air cell opened | 18 (100%) |
| Definite CSF leakage (N = 5) | |
| Male:Female | 2:3 |
| Left:Right | 2:3 |
| LD catheter insertion | 5 (100%) |
| LD insertion from POD | 5.2 (3–8) |
| Maintenance period of LD catheter | 5.2 (4–6) |
| Average hospital stay | 14.8 (13–19) |
| CSF leakage symptom recurrence | 0 (0.0%) |
| Revision operation | 0 (0.0%) |
| Intracranial infection | 0 (0.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-S.; Cho, K.-R.; Park, K.; Jeon, C. Management of Cerebrospinal Fluid Leakage after Microvascular Decompression Surgery: Clinical Strategy. Life 2023, 13, 1771. https://doi.org/10.3390/life13081771
Lee H-S, Cho K-R, Park K, Jeon C. Management of Cerebrospinal Fluid Leakage after Microvascular Decompression Surgery: Clinical Strategy. Life. 2023; 13(8):1771. https://doi.org/10.3390/life13081771
Chicago/Turabian StyleLee, Hyun-Seok, Kyung-Rae Cho, Kwan Park, and Chiman Jeon. 2023. "Management of Cerebrospinal Fluid Leakage after Microvascular Decompression Surgery: Clinical Strategy" Life 13, no. 8: 1771. https://doi.org/10.3390/life13081771
APA StyleLee, H.-S., Cho, K.-R., Park, K., & Jeon, C. (2023). Management of Cerebrospinal Fluid Leakage after Microvascular Decompression Surgery: Clinical Strategy. Life, 13(8), 1771. https://doi.org/10.3390/life13081771