

New Biomarker Combination Related to Oxidative Stress and Inflammation in Primary Open-Angle Glaucoma



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Methods
2.2. Biomarker Measurement
2.3. Statistical Analysis of the Data
3. Results
3.1. Population Distribution and Clinical Characteristics
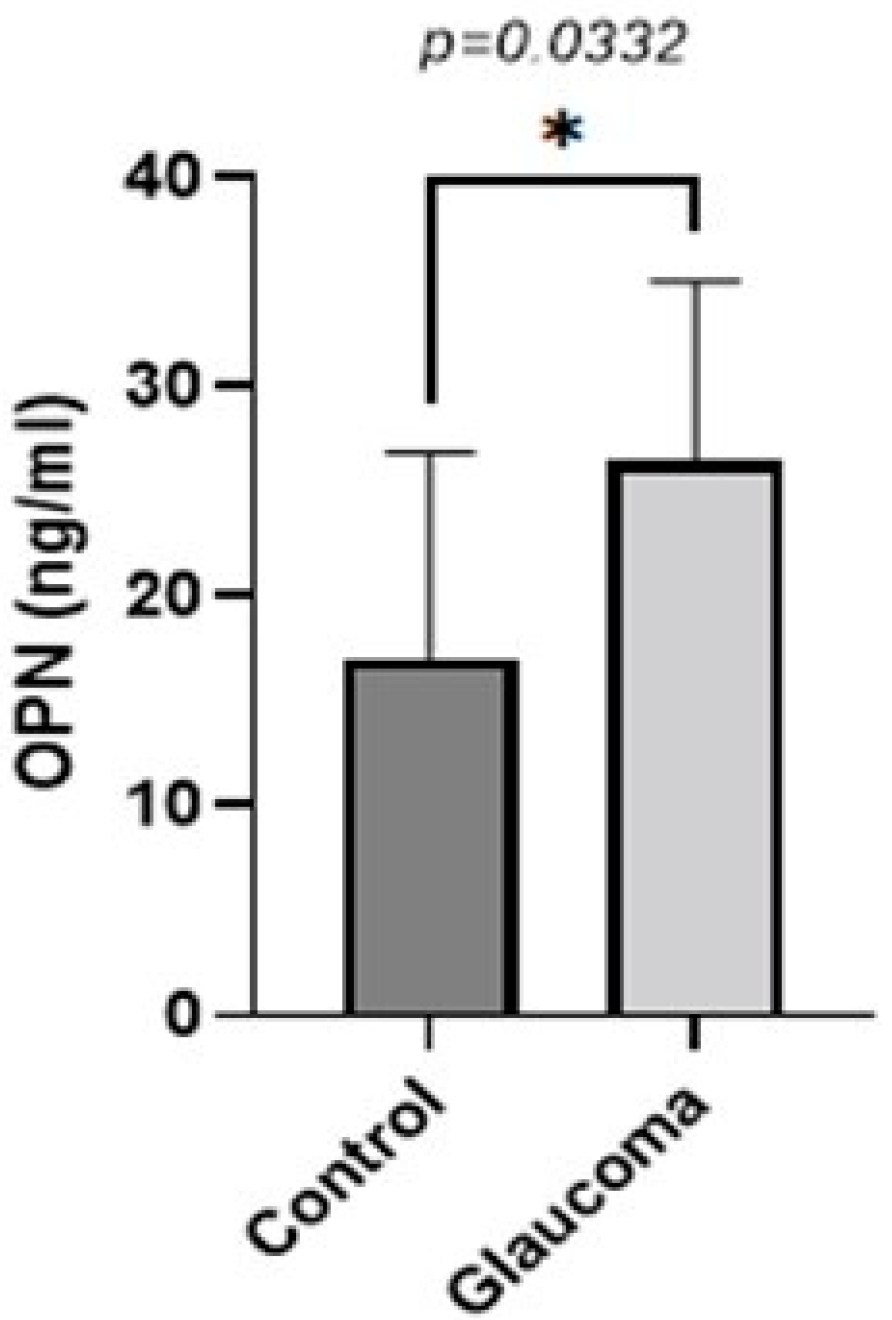
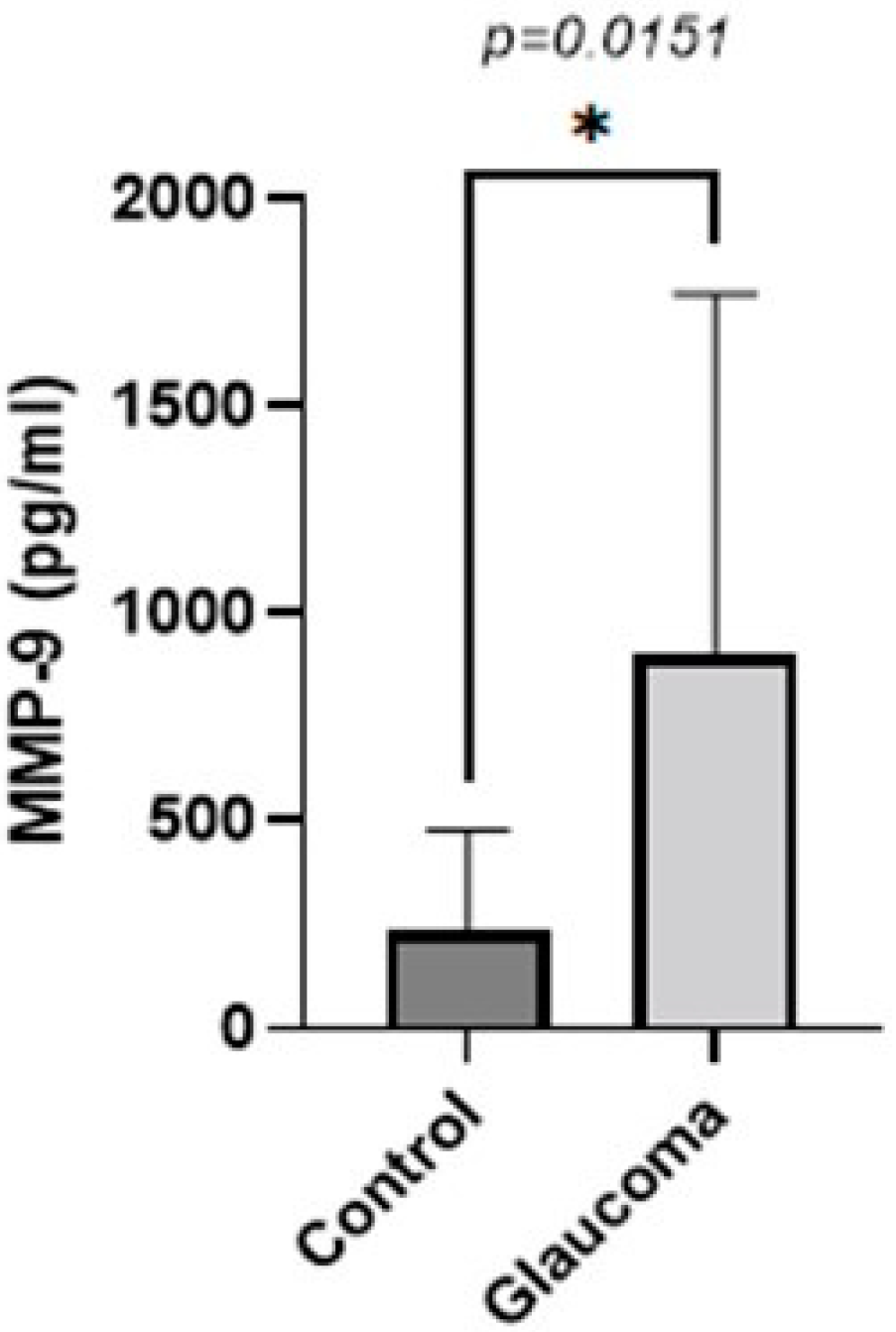
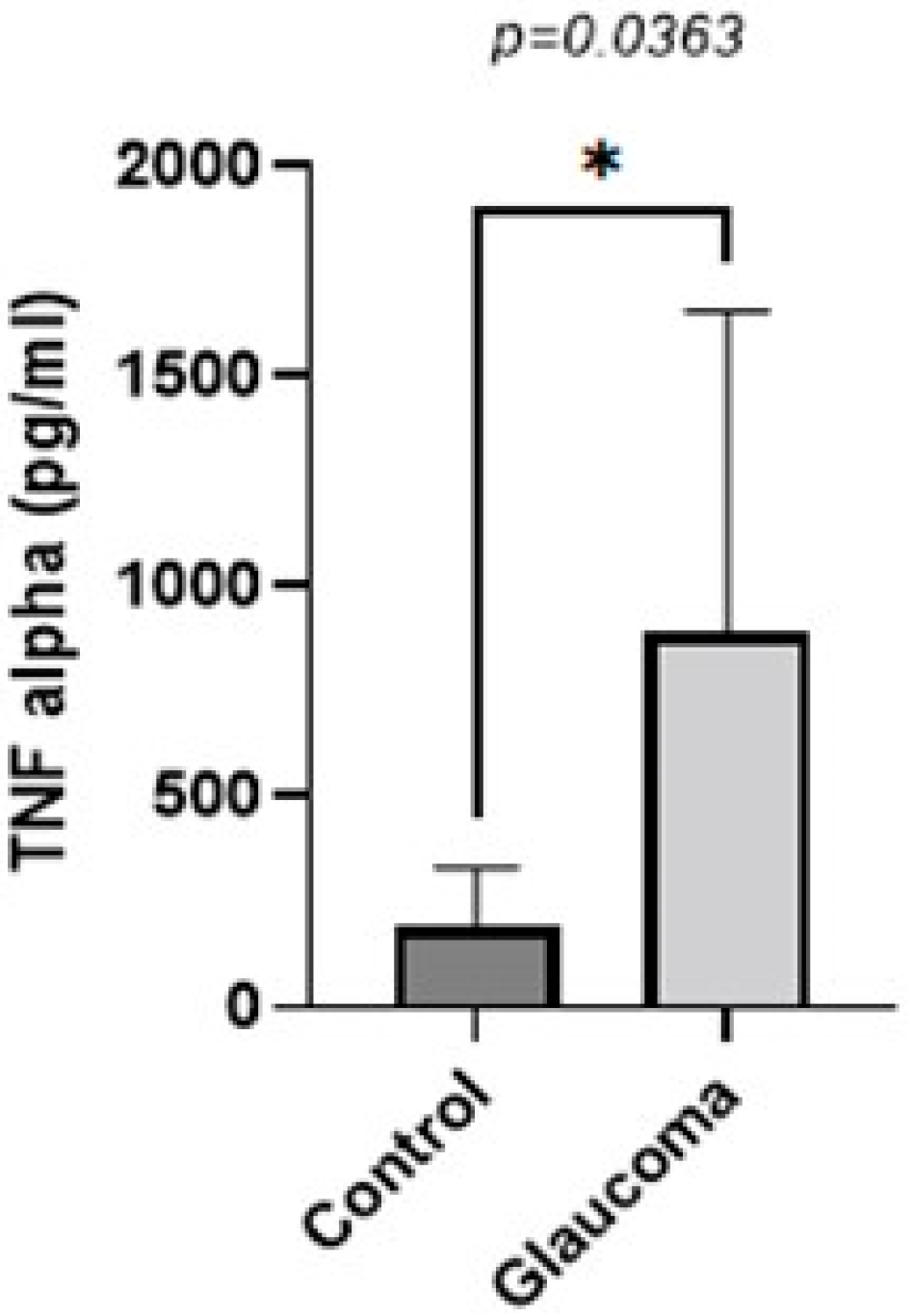
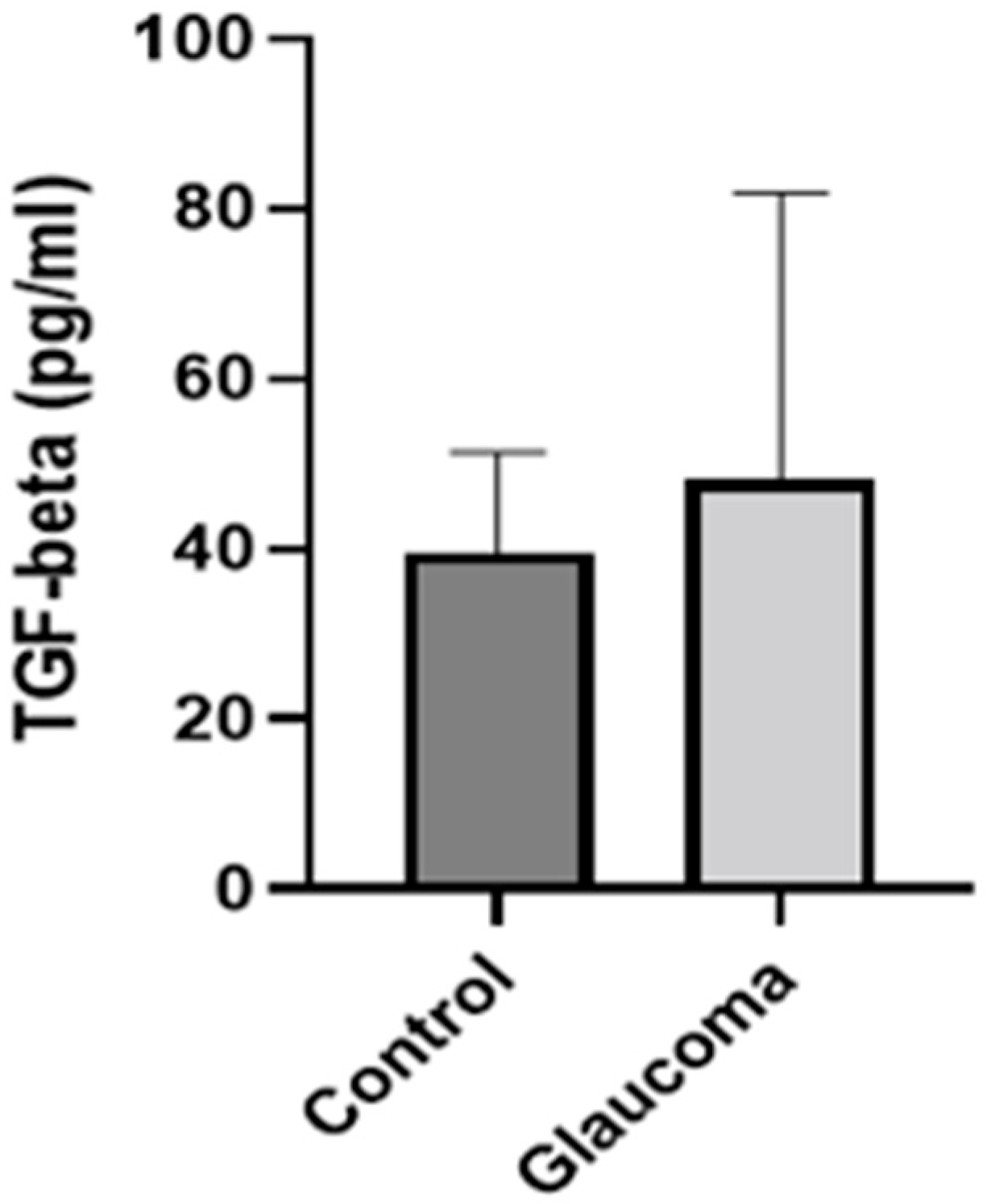
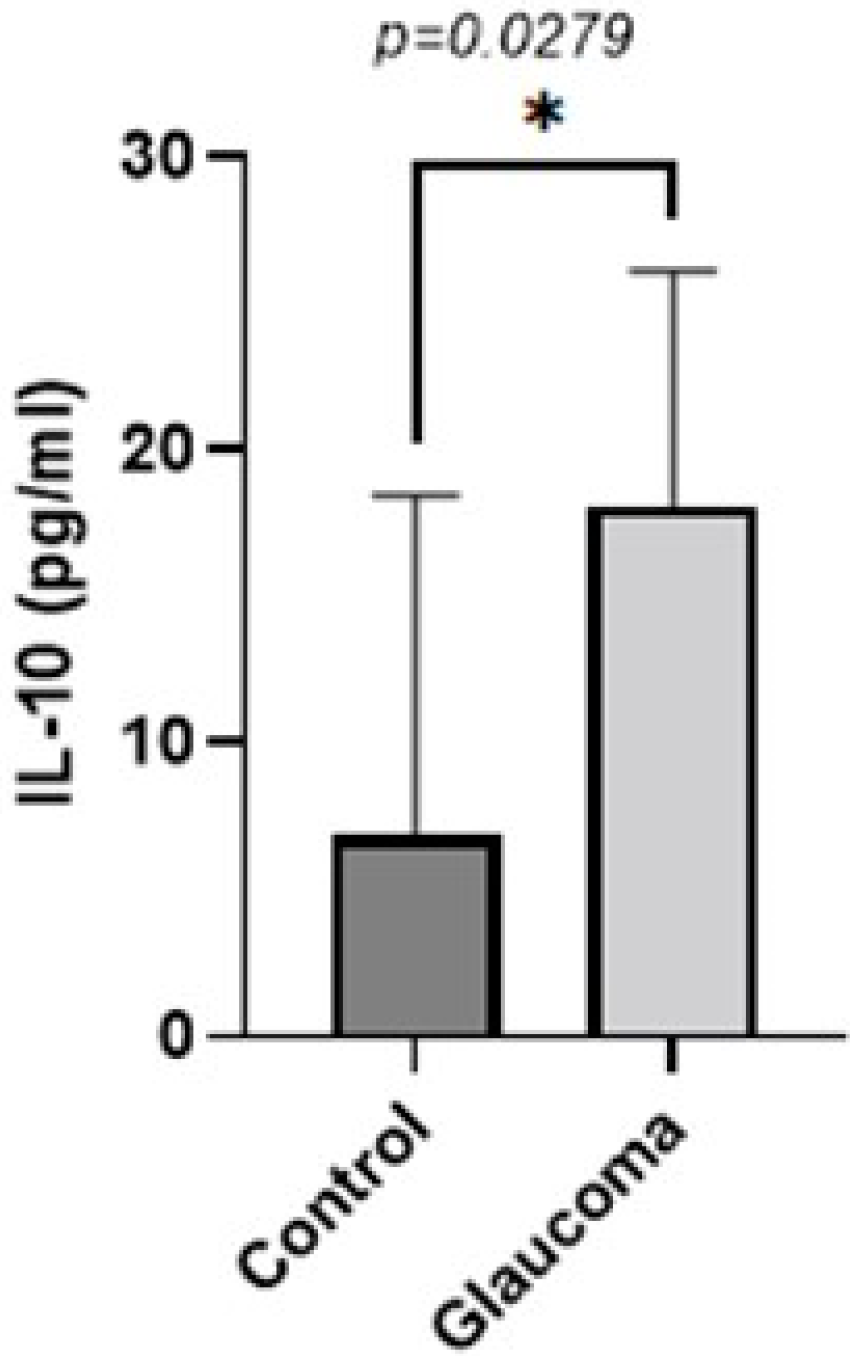
3.2. Biomarker Quantification in the Aqueous Humor of the Study Population
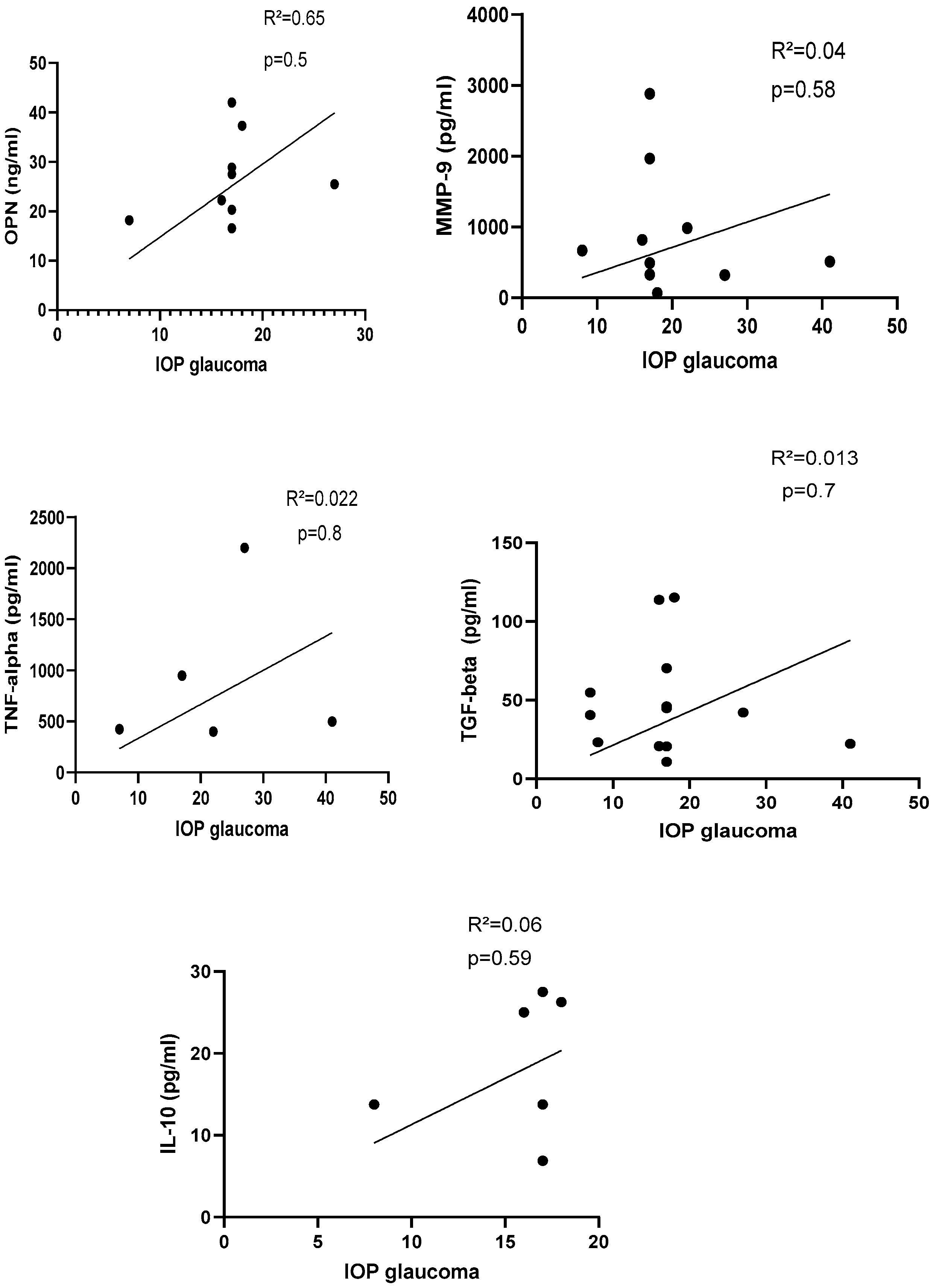
3.3. Correlation Analysis of Biomarker Concentration and Postoperative IOP Values in Glaucoma Patients
3.4. Comparison of Osteopontin Concentration in AH between Males and Females
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Janssen, S.F.; Gorgels, T.G.; Ramdas, W.D.; Klaver, C.C.; van Duijn, C.M.; Jansonius, N.M.; Bergen, A.A. The vast complexity of primary open angle glaucoma: Disease genes, risks, molecular mechanisms and pathobiology. Prog. Retin. Eye Res. 2013, 37, 31–67. [Google Scholar] [CrossRef] [PubMed]
- Foster, P.J.; Buhrmann, R.; Quigley, H.A.; Johnson, G.J. The definition and classification of glaucoma in prevalence surveys. Br. J. Ophthalmol. 2002, 86, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Nikhalashree, S.; George, R.; Shantha, B.; Lingam, V.; Vidya, W.; Panday, M.; Sulochana, K.N.; Coral, K. Detection of Proteins Associated with Extracellular Matrix Regulation in the Aqueous Humour of Patients with Primary Glaucoma. Curr. Eye Res. 2019, 44, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Buffault, J.; Labbé, A.; Hamard, P.; Brignole-Baudouin, F.; Baudouin, C. The trabecular meshwork: Structure, function and clinical implications. A review of the literature. J. Fr. Ophtalmol. 2020, 43, e217–e230. [Google Scholar] [CrossRef]
- To, C.H.; Kong, C.W.; Chan, C.Y.; Shahidullah, M.; Do, C.W. The mechanism of aqueous humour formation. Clin. Exp. Optom. 2002, 85, 335–349. [Google Scholar]
- Dammak, A.; Huete-Toral, F.; Carpena-Torres, C.; Martin-Gil, A.; Pastrana, C.; Carracedo, G. From Oxidative Stress to Inflammation in the Posterior Ocular Diseases: Diagnosis and Treatment. Pharmaceutics 2021, 13, 1376. [Google Scholar] [CrossRef]
- Burgos-Blasco, B.; Vidal-Villegas, B.; Saenz-Frances, F.; Morales-Fernandez, L.; Perucho-Gonzalez, L.; Garcia-Feijoo, J.; Martinez-de-la-Casa, J.M. Tear and aqueous humour cytokine profile in primary open-angle glaucoma. Acta Ophthalmol. 2020, 98, e768–e772. [Google Scholar] [CrossRef]
- Khalef, N.; Labib, H.; Helmy, H.; El Hamid, M.A.; Moemen, L.; Fahmy, I. Levels of cytokines in the aqueous humor of eyes with primary open angle glaucoma, pseudoexfoliation glaucoma and cataract. Electron. Physician 2017, 9, 3833–3837. [Google Scholar] [CrossRef]
- Sawada, H.; Fukuchi, T.; Tanaka, T.; Abe, H. Tumor necrosis factor-alpha concentrations in the aqueous humor of patients with glaucoma. Investig. Ophthalmol. Vis. Sci. 2010, 51, 903–906. [Google Scholar] [CrossRef]
- Balaiya, S.; Edwards, J.; Tillis, T.; Khetpal, V.; Chalam, K.V. Tumor necrosis factor-alpha (TNF-α) levels in aqueous humor of primary open angle glaucoma. Clin. Ophthalmol. 2011, 5, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Markiewicz, L.; Pytel, D.; Mucha, B.; Szymanek, K.; Szaflik, J.; Szaflik, J.P.; Majsterek, I. Altered Expression Levels of MMP1, MMP9, MMP12, TIMP1, and IL-1β as a Risk Factor for the Elevated IOP and Optic Nerve Head Damage in the Primary Open-Angle Glaucoma Patients. Biomed Res. Int. 2015, 2015, 812503. [Google Scholar] [CrossRef] [PubMed]
- Sahay, P.; Rao, A.; Padhy, D.; Sarangi, S.; Das, G.; Reddy, M.M.; Modak, R. Functional Activity of Matrix Metalloproteinases 2 and 9 in Tears of Patients with Glaucoma. Investig. Ophthalmol. Vis. Sci. 2017, 58, Bio106–Bio113. [Google Scholar] [CrossRef]
- Chowdhury, U.R.; Jea, S.Y.; Oh, D.J.; Rhee, D.J.; Fautsch, M.P. Expression profile of the matricellular protein osteopontin in primary open-angle glaucoma and the normal human eye. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6443–6451. [Google Scholar] [CrossRef]
- Kahles, F.; Findeisen, H.M.; Bruemmer, D. Osteopontin: A novel regulator at the cross roads of inflammation, obesity and diabetes. Mol. Metab. 2014, 3, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Birke, M.T.; Neumann, C.; Birke, K.; Kremers, J.; Scholz, M. Changes of osteopontin in the aqueous humor of the DBA2/J glaucoma model correlated with optic nerve and RGC degenerations. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5759–5767. [Google Scholar] [CrossRef]
- Agarwal, P.; Daher, A.M.; Agarwal, R. Aqueous humor TGF-β2 levels in patients with open-angle glaucoma: A meta-analysis. Mol. Vis. 2015, 21, 612–620. [Google Scholar]
- Igarashi, N.; Honjo, M.; Asaoka, R.; Kurano, M.; Yatomi, Y.; Igarashi, K.; Miyata, K.; Kaburaki, T.; Aihara, M. Aqueous autotaxin and TGF-βs are promising diagnostic biomarkers for distinguishing open-angle glaucoma subtypes. Sci. Rep. 2021, 11, 1408. [Google Scholar] [CrossRef]
- Kong, G.Y.; Van Bergen, N.J.; Trounce, I.A.; Crowston, J.G. Mitochondrial dysfunction and glaucoma. J. Glaucoma 2009, 18, 93–100. [Google Scholar] [CrossRef]
- Zhao, J.; Wang, S.; Zhong, W.; Yang, B.; Sun, L.; Zheng, Y. Oxidative stress in the trabecular meshwork (Review). Int. J. Mol. Med. 2016, 38, 995–1002. [Google Scholar] [CrossRef]
- He, Y.; Leung, K.W.; Zhang, Y.H.; Duan, S.; Zhong, X.F.; Jiang, R.Z.; Peng, Z.; Tombran-Tink, J.; Ge, J. Mitochondrial complex I defect induces ROS release and degeneration in trabecular meshwork cells of POAG patients: Protection by antioxidants. Investig. Ophthalmol. Vis. Sci. 2008, 49, 1447–1458. [Google Scholar] [CrossRef]
- Alasil, T.; Wang, K.; Keane, P.A.; Lee, H.; Baniasadi, N.; de Boer, J.F.; Chen, T.C. Analysis of normal retinal nerve fiber layer thickness by age, sex, and race using spectral domain optical coherence tomography. J. Glaucoma 2013, 22, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Cao, W.F.; Wang, Y.X.; Chen, C.X.; Jonas, J.B. Anterior chamber depth and chamber angle and their associations with ocular and general parameters: The Beijing Eye Study. Am. J. Ophthalmol. 2008, 145, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Friedman, D.S.; Zhou, Q.; Yang, X.H.; Sun, L.P.; Guo, L.; Chang, D.S.; Lian, L.; Wang, N.L. Prevalence and characteristics of primary angle-closure diseases in a rural adult Chinese population: The Handan Eye Study. Investig. Ophthalmol. Vis. Sci. 2011, 52, 8672–8679. [Google Scholar] [CrossRef] [PubMed]
- Tehrani, S. Gender difference in the pathophysiology and treatment of glaucoma. Curr. Eye Res. 2015, 40, 191–200. [Google Scholar] [CrossRef]
- Du, Y.; Mao, L.; Wang, Z.; Yan, K.; Zhang, L.; Zou, J. Osteopontin—The stirring multifunctional regulatory factor in multisystem aging. Front. Endocrinol. 2022, 13, 1014853. [Google Scholar] [CrossRef]
- Chowdhury, U.R.; Madden, B.J.; Charlesworth, M.C.; Fautsch, M.P. Proteome analysis of human aqueous humor. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4921–4931. [Google Scholar] [CrossRef]
- Pumphrey, S.A.; Zitek-Morrison, E.; Pizzirani, S.; Meola, D.M. Evaluation of matrix metalloproteinases and tissue inhibitors of metalloproteinases in aqueous humor of dogs with versus without naturally occurring primary angle-closure glaucoma. Am. J. Vet. Res. 2021, 83, 245–255. [Google Scholar] [CrossRef]
- Gao, X.J.; Hou, S.P.; Li, P.H. The association between matrix metalloprotease-9 gene polymorphisms and primary angle-closure glaucoma in a Chinese Han population. Int. J. Ophthalmol. 2014, 7, 397–402. [Google Scholar]
- Micheal, S.; Qamar, R.; Akhtar, F.; Khan, M.I.; Khan, W.A.; Ahmed, A. MTHFR gene C677T and A1298C polymorphisms and homocysteine levels in primary open angle and primary closed angle glaucoma. Mol. Vis. 2009, 15, 2268–2278. [Google Scholar]
- Hosseini, M.; Rose, A.Y.; Song, K.; Bohan, C.; Alexander, J.P.; Kelley, M.J.; Acott, T.S. IL-1 and TNF induction of matrix metalloproteinase-3 by c-Jun N-terminal kinase in trabecular meshwork. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Rönkkö, S.; Rekonen, P.; Kaarniranta, K.; Puustjärvi, T.; Teräsvirta, M.; Uusitalo, H. Matrix metalloproteinases and their inhibitors in the chamber angle of normal eyes and patients with primary open-angle glaucoma and exfoliation glaucoma. Graefes Arch. Clin. Exp. Ophthalmol. 2007, 245, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Zhuravleva, A.N.; Neroev, V.V.; Ndreeva, L.D. Investigation of scleral fibronectin in primary open-angle glaucoma: Immunohistochemical study. Vestn. Oftalmol. 2009, 125, 12–15. [Google Scholar] [PubMed]
- Keller, K.E.; Peters, D.M. Pathogenesis of glaucoma: Extracellular matrix dysfunction in the trabecular meshwork—A review. Clin. Exp. Ophthalmol. 2022, 50, 163–182. [Google Scholar] [CrossRef]
- Kurysheva, N.I.; Sharova, G.A. Primary anterior chamber angle closure: Progression from suspect to glaucoma. Part 1. Frequency and rate of transition from suspected primary angle closure to true angle closure and primary angle closure glaucoma. Vestn. Oftalmol. 2022, 138, 101–107. [Google Scholar] [CrossRef]
- Golubnitschaja, O.; Yeghiazaryan, K.; Liu, R.; Mönkemann, H.; Leppert, D.; Schild, H.; Haefliger, I.O.; Flammer, J. Increased expression of matrix metalloproteinases in mononuclear blood cells of normal-tension glaucoma patients. J. Glaucoma 2004, 13, 66–72. [Google Scholar] [CrossRef]
- Guo, Y.; Zhang, H.; Chen, X.; Yang, X.; Cheng, W.; Zhao, K. Association of TP53 polymorphisms with primary open-angle glaucoma: A meta-analysis. Investig. Ophthalmol. Vis. Sci. 2012, 53, 3756–3763. [Google Scholar] [CrossRef]
- Svinareva, D.I.; Churnosov, M.I. The role of metalloproteinases in the development of primary open-angle glaucoma. Vestn. Oftalmol. 2020, 136, 146–150. [Google Scholar] [CrossRef]
- Chen, X.; Chen, Y.; Wiggs, J.L.; Pasquale, L.R.; Sun, X.; Fan, B.J. Association of Matrix Metalloproteinase-9 (MMP9) Variants with Primary Angle Closure and Primary Angle Closure Glaucoma. PLoS ONE 2016, 11, e0157093. [Google Scholar] [CrossRef]
- Cordeiro, M.F.; Chang, L.; Lim, K.S.; Daniels, J.T.; Pleass, R.D.; Siriwardena, D.; Khaw, P.T. Modulating conjunctival wound healing. Eye 2000, 14 Pt 3B, 536–547. [Google Scholar] [CrossRef]
- Schlötzer-Schrehardt, U.; Zenkel, M.; Küchle, M.; Sakai, L.Y.; Naumann, G.O. Role of transforming growth factor-beta1 and its latent form binding protein in pseudoexfoliation syndrome. Exp. Eye Res. 2001, 73, 765–780. [Google Scholar] [CrossRef]
- Kondkar, A.A.; Sultan, T.; Almobarak, F.A.; Kalantan, H.; Al-Obeidan, S.A.; Abu-Amero, K.K. Association of increased levels of plasma tumor necrosis factor alpha with primary open-angle glaucoma. Clin. Ophthalmol. 2018, 12, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Ten Berge, J.C.; Fazil, Z.; van den Born, I.; Wolfs, R.C.W.; Schreurs, M.W.J.; Dik, W.A.; Rothova, A. Intraocular cytokine profile and autoimmune reactions in retinitis pigmentosa, age-related macular degeneration, glaucoma and cataract. Acta Ophthalmol. 2019, 97, 185–192. [Google Scholar] [CrossRef]
- Jung, Y.; Ohn, K.; Shin, H.; Oh, S.E.; Park, C.K.; Park, H.L. Factors Associated with Elevated Tumor Necrosis Factor-α in Aqueous Humor of Patients with Open-Angle Glaucoma. J. Clin. Med. 2022, 11, 5232. [Google Scholar] [CrossRef]
- Wei, X.; Zhang, B.; Wei, F.; Ding, M.; Luo, Z.; Han, X.; Tan, X. Gegen Qinlian pills alleviate carrageenan-induced thrombosis in mice model by regulating the HMGB1/NF-κB/NLRP3 signaling. Phytomedicine 2022, 100, 154083. [Google Scholar] [CrossRef] [PubMed]
- Rad, F.; Dabbagh, A.; Dorgalaleh, A.; Biswas, A. The Relationship between Inflammatory Cytokines and Coagulopathy in Patients with COVID-19. J. Clin. Med. 2021, 10, 2020. [Google Scholar] [CrossRef] [PubMed]
- Sziksz, E.; Pap, D.; Lippai, R.; Béres, N.J.; Fekete, A.; Szabó, A.J.; Vannay, Á. Fibrosis Related Inflammatory Mediators: Role of the IL-10 Cytokine Family. Mediat. Inflamm. 2015, 2015, 764641. [Google Scholar] [CrossRef]
- Csősz, É.; Deák, E.; Tóth, N.; Traverso, C.E.; Csutak, A.; Tőzsér, J. Comparative analysis of cytokine profiles of glaucomatous tears and aqueous humour reveals potential biomarkers for trabeculectomy complications. FEBS Open Bio 2019, 9, 1020–1028. [Google Scholar] [CrossRef]
- Duvesh, R.; Puthuran, G.; Srinivasan, K.; Rengaraj, V.; Krishnadas, S.R.; Rajendrababu, S.; Balakrishnan, V.; Ramulu, P.; Sundaresan, P. Multiplex Cytokine Analysis of Aqueous Humor from the Patients with Chronic Primary Angle Closure Glaucoma. Curr. Eye Res. 2017, 42, 1608–1613. [Google Scholar] [CrossRef]
- Garweg, J.G.; Zandi, S.; Pfister, I.B.; Skowronska, M.; Gerhardt, C. Comparison of cytokine profiles in the aqueous humor of eyes with pseudoexfoliation syndrome and glaucoma. PLoS ONE 2017, 12, e0182571. [Google Scholar] [CrossRef]
- Martinez-de-la-Casa, J.M.; Perez-Bartolome, F.; Urcelay, E.; Santiago, J.L.; Moreno-Montañes, J.; Arriola-Villalobos, P.; Benitez-Del-Castillo, J.M.; Garcia-Feijoo, J. Tear cytokine profile of glaucoma patients treated with preservative-free or preserved latanoprost. Ocul. Surf. 2017, 15, 723–729. [Google Scholar] [CrossRef]
- Zhang, Y.H.; Xing, Y.Q.; Chen, Z.; Ma, X.C.; Lu, Q. Association between interleukin-10 genetic polymorphisms and risk of primary open angle glaucoma in a Chinese Han population: A case-control study. Int. J. Ophthalmol. 2019, 12, 1605–1611. [Google Scholar] [CrossRef] [PubMed]
- Fakhraie, G.; Parvini, F.; Ghanavi, J.; Saif, S.; Farnia, P. Association of IL-10 gene promoter polymorphisms with susceptibility to pseudoexfoliation syndrome, pseudoexfoliative and primary open-angle glaucoma. BMC Med. Genet. 2020, 21, 32. [Google Scholar] [CrossRef]
- Bell, K.; Und Hohenstein-Blaul, N.V.T.; Teister, J.; Grus, F. Modulation of the Immune System for the Treatment of Glaucoma. Curr. Neuropharmacol. 2018, 16, 942–958. [Google Scholar] [CrossRef]
- Umeno, A.; Yoshida, Y.; Kaidzu, S.; Tanito, M. Positive Association between Aqueous Humor Hydroxylinoleate Levels and Intraocular Pressure. Molecules 2022, 27, 2215. [Google Scholar] [CrossRef] [PubMed]
- Freedman, J.; Iserovich, P. Pro-inflammatory cytokines in glaucomatous aqueous and encysted Molteno implant blebs and their relationship to pressure. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4851–4855. [Google Scholar] [CrossRef]
- Huang, W.; Chen, S.; Gao, X.; Yang, M.; Zhang, J.; Li, X.; Wang, W.; Zhou, M.; Zhang, X.; Zhang, X. Inflammation-related cytokines of aqueous humor in acute primary angle-closure eyes. Investig. Ophthalmol. Vis. Sci. 2014, 55, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Takai, Y.; Tanito, M.; Ohira, A. Multiplex cytokine analysis of aqueous humor in eyes with primary open-angle glaucoma, exfoliation glaucoma, and cataract. Investig. Ophthalmol. Vis. Sci. 2012, 53, 241–247. [Google Scholar] [CrossRef]
- Wang, J.; Fu, M.; Liu, K.; Wang, N.; Zhang, Z.; Zhou, M.; Xu, X. Matricellular Proteins Play a Potential Role in Acute Primary Angle Closure. Curr. Eye Res. 2018, 43, 771–777. [Google Scholar] [CrossRef]
- Tong, Y.; Zhou, Y.L.; Zheng, Y.; Biswal, M.; Zhao, P.Q.; Wang, Z.Y. Analyzing cytokines as biomarkers to evaluate severity of glaucoma. Int. J. Ophthalmol. 2017, 10, 925–930. [Google Scholar]
- Rusmayani, E.; Artini, W.; Sasongko, M.B.; Suhardjo; Viona, V. A Novel Biomarker in Primary Glaucoma: Aqueous Humor and Serum Levels of Ischemia Modified Albumin (IMA). Clin. Ophthalmol. 2022, 16, 4075–4087. [Google Scholar] [CrossRef] [PubMed]
- Mason, L.; Jafri, S.; Dortonne, I.; Sheppard, J.D., Jr. Emerging therapies for dry eye disease. Expert Opin. Emerg. Drugs 2021, 26, 401–413. [Google Scholar] [CrossRef]
- Roda, M.; Corazza, I.; Bacchi Reggiani, M.L.; Pellegrini, M.; Taroni, L.; Giannaccare, G.; Versura, P. Dry Eye Disease and Tear Cytokine Levels—A Meta-Analysis. Int. J. Mol. Sci. 2020, 21, 3111. [Google Scholar] [CrossRef] [PubMed]
- Zaleska-Żmijewska, A.; Strzemecka, E.; Wawrzyniak, Z.M.; Szaflik, J.P. Extracellular MMP-9-Based Assessment of Ocular Surface Inflammation in Patients with Primary Open-Angle Glaucoma. J. Ophthalmol. 2019, 2019, 1240537. [Google Scholar] [CrossRef]
- Lok, Z.S.Y.; Lyle, A.N. Osteopontin in Vascular Disease. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 613–622. [Google Scholar] [CrossRef]
- Abdelaziz Mohamed, I.; Gadeau, A.P.; Hasan, A.; Abdulrahman, N.; Mraiche, F. Osteopontin: A Promising Therapeutic Target in Cardiac Fibrosis. Cells 2019, 8, 1558. [Google Scholar] [CrossRef]
- Lamort, A.S.; Giopanou, I.; Psallidas, I.; Stathopoulos, G.T. Osteopontin as a Link between Inflammation and Cancer: The Thorax in the Spotlight. Cells 2019, 8, 815. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.J.; Cho, H.J.; Kim, H.S. Osteopontin: A multifunctional protein at the crossroads of inflammation, atherosclerosis, and vascular calcification. Curr. Atheroscler. Rep. 2009, 11, 206–213. [Google Scholar] [CrossRef]
- Weber, C.E.; Li, N.Y.; Wai, P.Y.; Kuo, P.C. Epithelial-mesenchymal transition, TGF-β, and osteopontin in wound healing and tissue remodeling after injury. J. Burn Care Res. 2012, 33, 311–318. [Google Scholar] [CrossRef]
- Icer, M.A.; Gezmen-Karadag, M. The multiple functions and mechanisms of osteopontin. Clin. Biochem. 2018, 59, 17–24. [Google Scholar] [CrossRef]
- Niikura, Y.; Ishii, T.; Hosoki, K.; Nagase, T.; Yamashita, N. Ovary-dependent emphysema augmentation and osteopontin induction in adult female mice. Biochem. Biophys. Res. Commun. 2015, 461, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Kariuki, S.N.; Moore, J.G.; Kirou, K.A.; Crow, M.K.; Utset, T.O.; Niewold, T.B. Age- and gender-specific modulation of serum osteopontin and interferon-alpha by osteopontin genotype in systemic lupus erythematosus. Genes Immun. 2009, 10, 487–494. [Google Scholar] [CrossRef]
- Yagisawa, T.; Ito, F.; Osaka, Y.; Amano, H.; Kobayashi, C.; Toma, H. The influence of sex hormones on renal osteopontin expression and urinary constituents in experimental urolithiasis. J. Urol. 2001, 166, 1078–1082. [Google Scholar] [CrossRef] [PubMed]
- El Assar, M.; Álvarez-Bustos, A.; Sosa, P.; Angulo, J.; Rodríguez-Mañas, L. Effect of Physical Activity/Exercise on Oxidative Stress and Inflammation in Muscle and Vascular Aging. Int. J. Mol. Sci. 2022, 23, 8713. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Control (n = 16) Mean ± SD | Glaucoma (n = 16) Mean ± SD |
|---|---|---|
| Age (years) | 54.94 ± 9.23 | 67.37 ± 12.92 |
| Gender | ||
| Male [n (%)] | 8 (50%) | 6 (37.5%) |
| Female [n (%)] | 8 (50%) | 10 (62.5%) |
| Clinical characteristics | ||
| Preoperative IOP (mmHg) | 16.06 ± 2.26 | 16.18 ± 2.9 |
| Postoperative IOP (mmHg) | 20.94 ± 5.64 (p = 0.015) | 17.5 ± 8.09 (p = 0.546) |
| Biomarker | Control Group | Number of Patients | Glaucoma Group | Number of Patients | p- Values |
|---|---|---|---|---|---|
| OPN (ng/mL) | 17.09 ± 10.11 | 16 | 26.50 ± 8.50 | 16 | 0.033 |
| MMP-9 (pg/mL) | 241.10 ± 235.08 | 16 | 904.5 ± 869.21 | 16 | 0.015 |
| TNF-alpha (pg/mL) | 196.41 ± 135 | 8 | 895.04 ± 362.09 | 8 | 0.036 |
| TGF-beta (pg/mL) | 39.62 ± 11.6 | 13 | 48.15 ± 33.73 | 13 | 0.397 |
| Interleukin-10 (pg/mL) | 6.87 ± 11.57 | 8 | 18.13 ± 8.21 | 8 | 0.029 |
| Biomarker | Glaucoma, Female (n = 10) | Glaucoma, Male (n = 6) | p-Values |
|---|---|---|---|
| OPN (ng/mL) | 22.34 ± 10.21 | 24.39 ± 9.41 | 0.74 |
| Biomarker | Control, Female (n = 8) | Control, Male (n = 8) | p-Values |
| OPN (ng/mL) | 25.69 ± 19.02 | 15.74 ± 12.13 | 0.22 |
| Biomarker | Control + Glaucoma Female (n = 18) | Control + Glaucoma Male (n = 14) | p-Values |
| OPN (ng/mL) | 26.60 ± 14.06 | 23.24 ± 7.15 | 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dammak, A.; Sanchez Naves, J.; Huete-Toral, F.; Carracedo, G. New Biomarker Combination Related to Oxidative Stress and Inflammation in Primary Open-Angle Glaucoma. Life 2023, 13, 1455. https://doi.org/10.3390/life13071455
Dammak A, Sanchez Naves J, Huete-Toral F, Carracedo G. New Biomarker Combination Related to Oxidative Stress and Inflammation in Primary Open-Angle Glaucoma. Life. 2023; 13(7):1455. https://doi.org/10.3390/life13071455
Chicago/Turabian StyleDammak, Azza, Juan Sanchez Naves, Fernando Huete-Toral, and Gonzalo Carracedo. 2023. "New Biomarker Combination Related to Oxidative Stress and Inflammation in Primary Open-Angle Glaucoma" Life 13, no. 7: 1455. https://doi.org/10.3390/life13071455
APA StyleDammak, A., Sanchez Naves, J., Huete-Toral, F., & Carracedo, G. (2023). New Biomarker Combination Related to Oxidative Stress and Inflammation in Primary Open-Angle Glaucoma. Life, 13(7), 1455. https://doi.org/10.3390/life13071455