
Systematic Review and Meta-Analysis: Recurrent Laryngeal Nerve Variants and Their Implication in Surgery and Neck Pathologies, Using the Anatomical Quality Assurance (AQUA) Checklist


Abstract
1. Introduction
2. Methodology
2.1. Search Strategy
2.2. Search Terms
2.3. Eligibility Criteria of Included Studies
2.4. Outcomes
2.5. Data Extraction and Synthesis
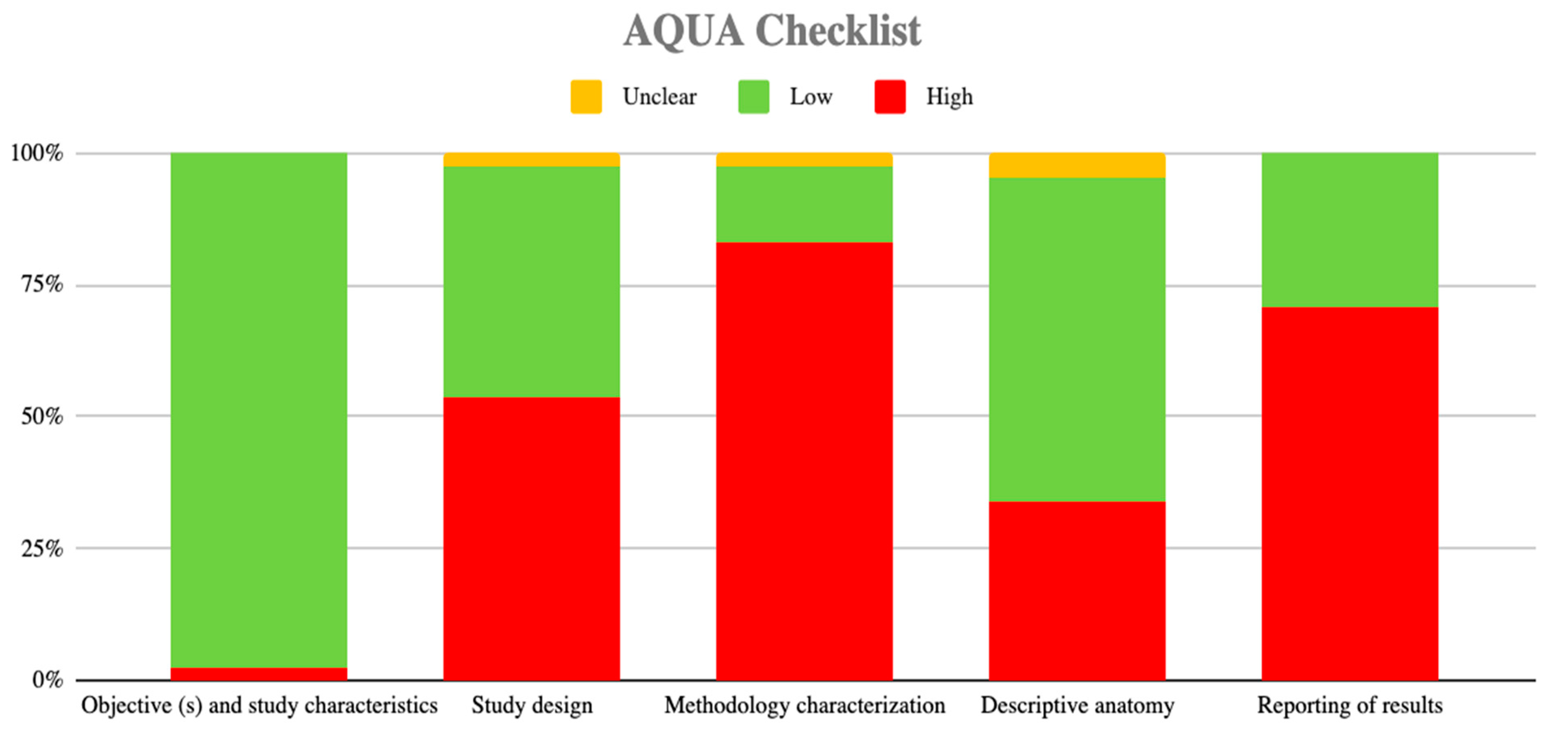
2.6. Assessment of the Methodological Quality of the Included Studies
2.7. Analysis of Data
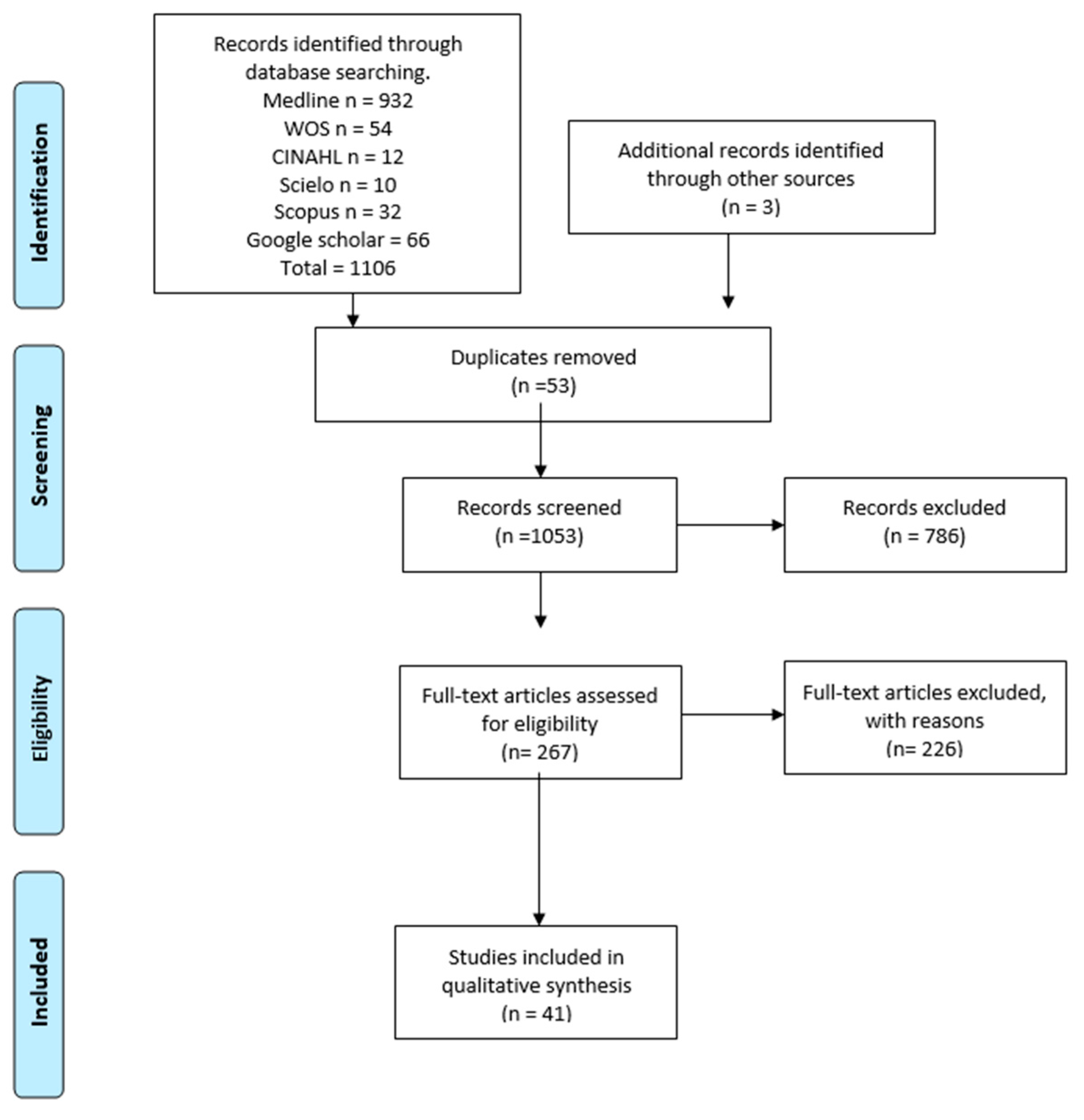
3. Results
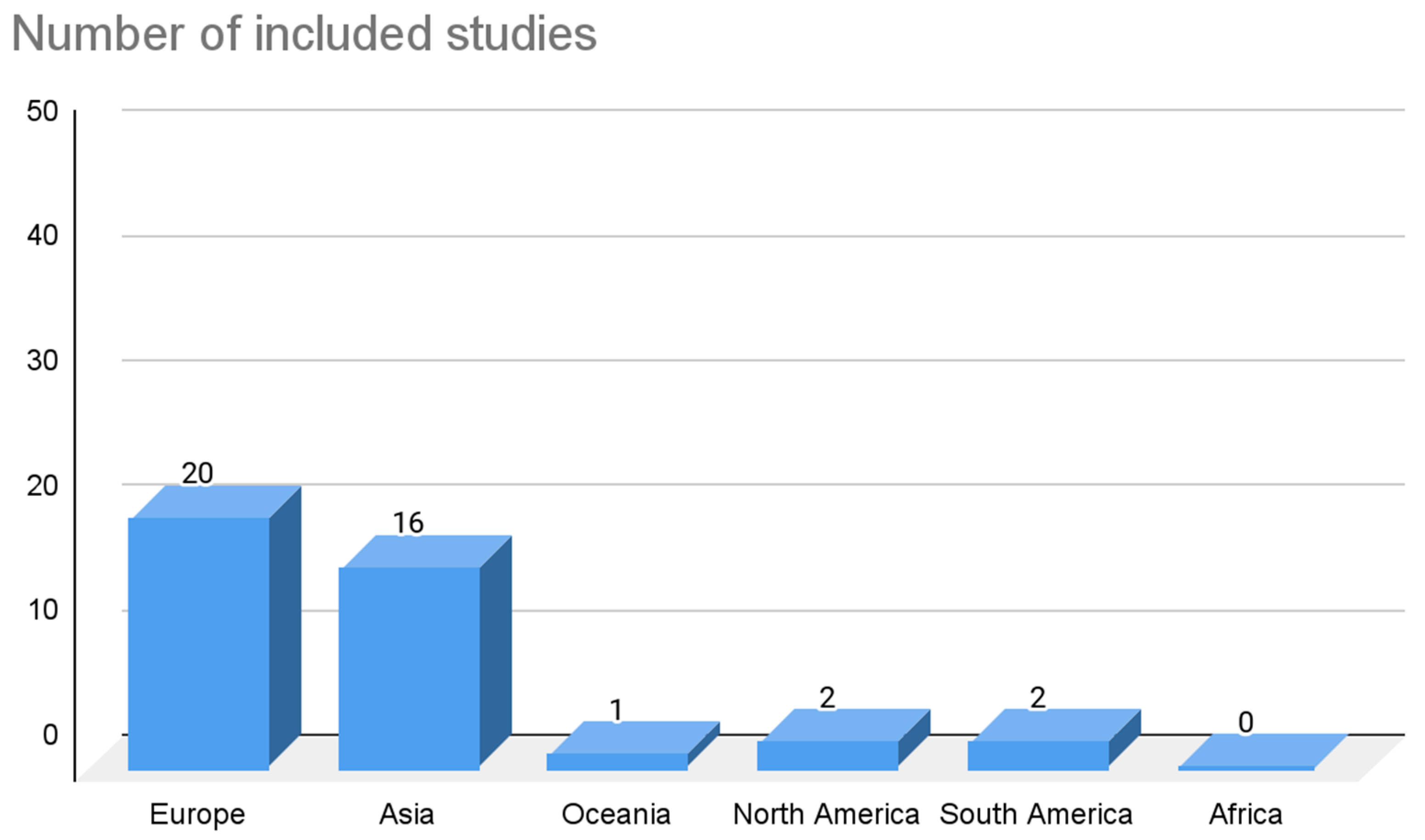
3.1. Included Studies
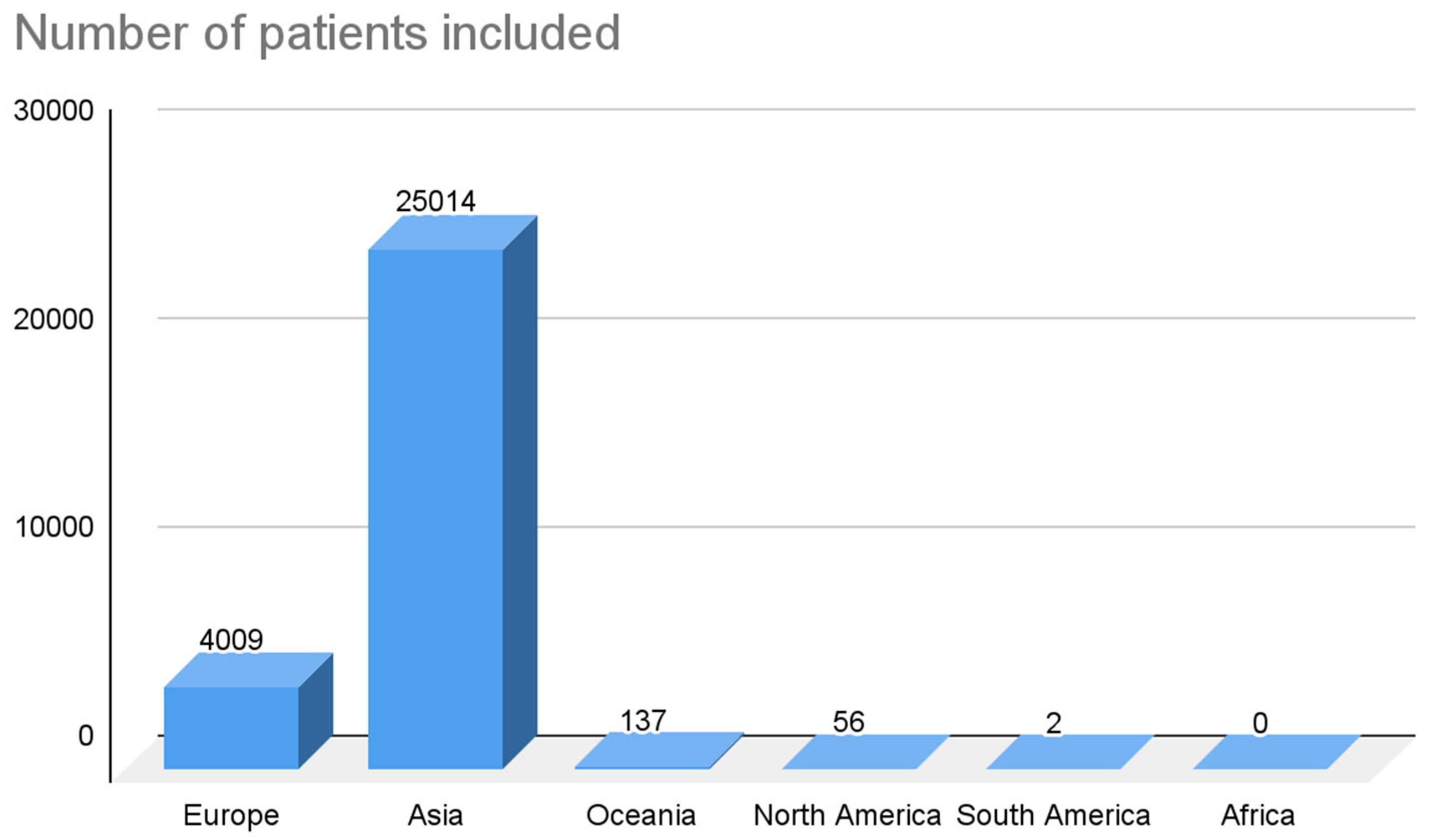
3.2. Characteristics of the Studies and the Population Studied
4. Prevalence
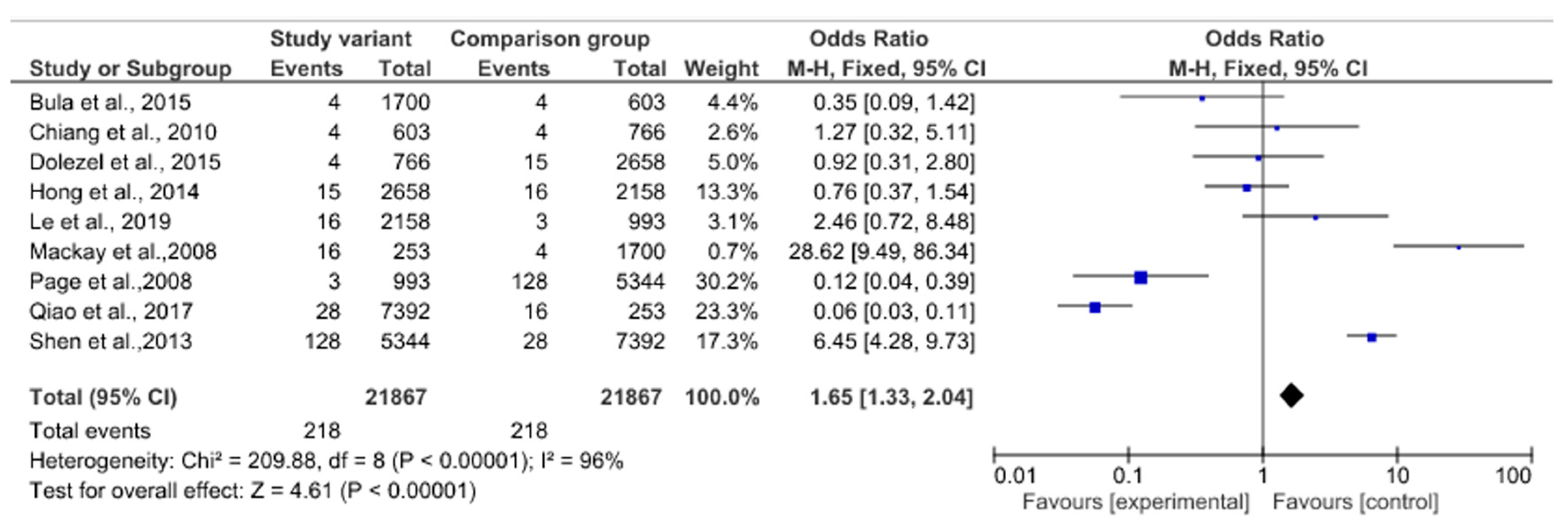
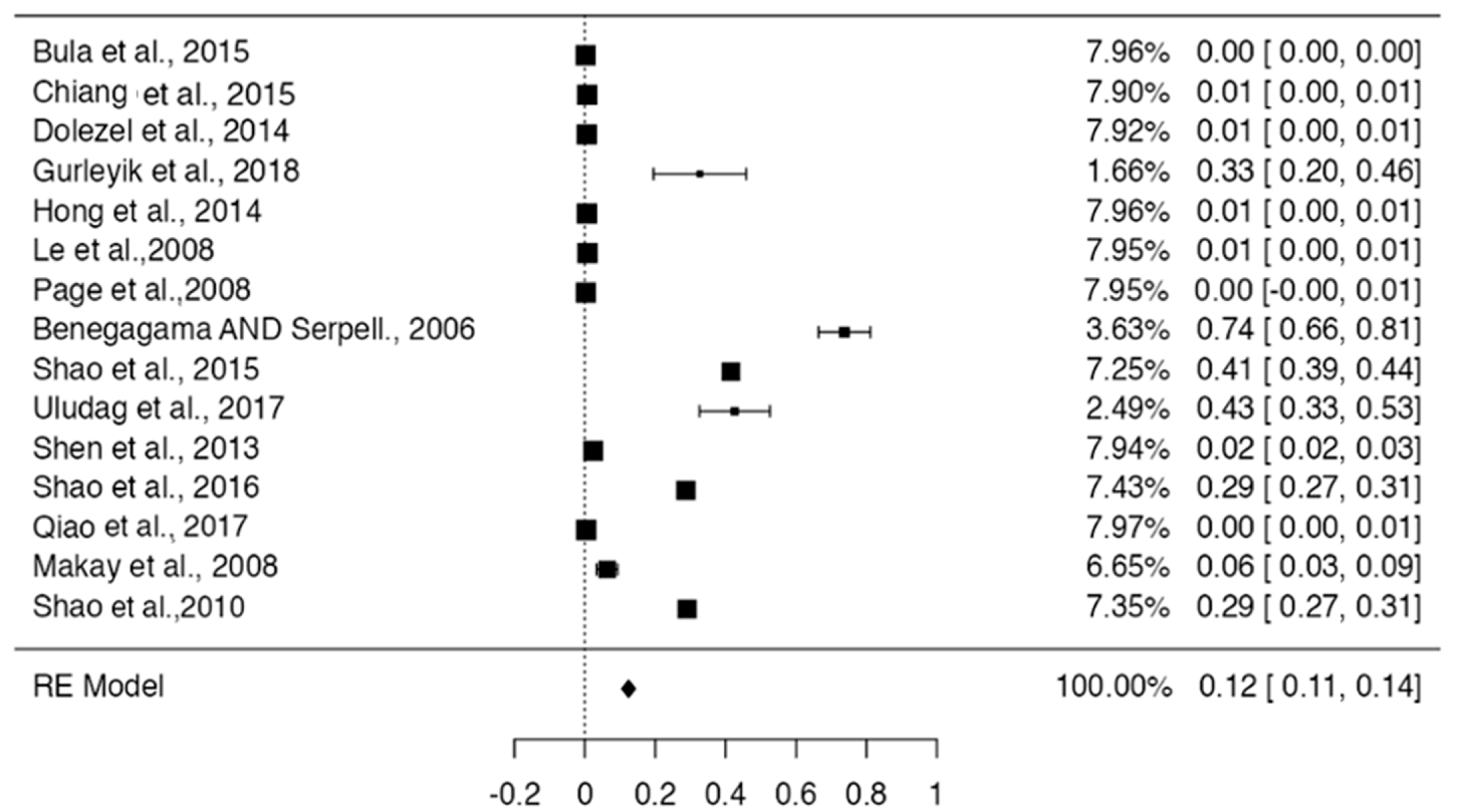
5. Meta-Analysis
6. Clinical Consideration
7. Discussion
8. Limitations
9. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Álvaro, S.; Andrés, C.; Adonis, R.; Andrés, Á. Anatomía quirúrgica cervical de importancia en cirugía tiroidea. Rev. Colomb. 2014, 29, 50–58. [Google Scholar]
- Lee, M.-S.; Lee, U.-Y.; Lee, J.-H.; Han, S.-H. Relative direction and position of recurrent laryngeal nerve for anatomical configuration. Surg. Radiol. Anat. 2009, 31, 649–655. [Google Scholar] [CrossRef]
- Makay, O.; Icoz, G.; Yilmaz, M.; Akyildiz, M.; Yetkin, E. The recurrent laryngeal nerve and the inferior thyroid artery—Anatomical variations during surgery. Langenbeck’s Arch. Surg. 2008, 393, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Uen, Y.-H.; Chen, T.-H.; Shyu, J.-F.; Shyr, Y.-M.; Su, C.-H.; Chen, J.-Y.; Lee, C.-S.; Liu, J.-C. Surgical Anatomy of the Recurrent Laryngeal Nerves and its Clinical Applications in Chinese Adults. Surg. Today 2006, 36, 312–315. [Google Scholar] [CrossRef]
- Coady, M.A.; Adler, F.; Davila, J.J.; Gahtan, V. Nonrecurrent laryngeal nerve during carotid artery surgery: Case report and literature review. J. Vasc. Surg. 2000, 32, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Harness, J.K.; Fung, L.K.; Thompson, N.W.; Burney, R.E.; McLeod, M.K. Total thyroidectomy: Complications and technique. World J. Surg. 1986, 10, 781–785. [Google Scholar] [CrossRef]
- Shao, T.; Qiu, W.; Yang, W. Anatomical variations of the recurrent laryngeal nerve in Chinese patients: A prospective study of 2,404 patients. Sci. Rep. 2016, 6, 25475. [Google Scholar] [CrossRef]
- Casella, C.; Pata, G.; Nascimbeni, R.; Mittempergher, F.; Salerni, B. Does Extralaryngeal Branching Have An Impact on the Rate of Postoperative Transient or Permanent Recurrent Laryngeal Nerve Palsy? World J. Surg. 2008, 33, 261–265. [Google Scholar] [CrossRef]
- Snyder, S.K.; Hendricks, J.C. Intraoperative neurophysiology testing of the recurrent laryngeal nerve: Plaudits and pitfalls. Surgery 2005, 138, 1183–1192. [Google Scholar] [CrossRef]
- Shindo, M.L.; Wu, J.C.; Park, E.E. Surgical Anatomy of the Recurrent Laryngeal Nerve Revisited. Otolaryngol. Neck Surg. 2005, 133, 514–519. [Google Scholar] [CrossRef]
- Yalcxin, B. Anatomic configurations of the recurrent laryngeal nerve and inferior thyroid artery. Surgery 2006, 139, 181–187, Erratum in Surgery 2008, 143, 453. [Google Scholar] [CrossRef]
- Buła, G.; Mucha, R.; Paliga, M.; Koziołek, H.; Niedzielski, Z.; Gawrychowski, J. Non-Recurrent Laryngeal Nerve. Pol. J. Surg. 2015, 87, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Yetisir, F.; Ozkardes, A.B.; Dundar, H.Z.; Birkan, B.; Ciftci, A.B.; Kilic, M. Non-recurrent laryngeal nerve. Turk. J. Surg. 2013, 30, 112–114. [Google Scholar] [CrossRef]
- Henry, B.M.; Vikse, J.; Graves, M.J.; Sanna, S.; Sanna, B.; Tomaszewska, I.M.; Tubbs, R.S.; Tomaszewski, K.A. Extralaryngeal branching of the recurrent laryngeal nerve: A meta-analysis of 28,387 nerves. Langenbeck’s Arch. Surg. 2016, 401, 913–923. [Google Scholar] [CrossRef] [PubMed]
- Chiang, F.-Y.; Lu, I.-C.; Chen, H.-C.; Chen, H.-Y.; Tsai, C.-J.; Hsiao, P.-J.; Lee, K.-W.; Wu, C.-W. Anatomical Variations of Recurrent Laryngeal Nerve During Thyroid Surgery: How to Identify and Handle the Variations With Intraoperative Neuromonitoring. Kaohsiung J. Med Sci. 2010, 26, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Chu, K.-S.; Wu, S.-H.; Lu, I.-C.; Tsai, C.-J.; Wu, C.-W.; Kuo, W.-R.; Lee, K.-W.; Chiang, F.-Y. Feasibility of Intraoperative Neuromonitoring During Thyroid Surgery After Administration of Nondepolarizing Neuromuscular Blocking Agents. World J. Surg. 2009, 33, 1408–1413. [Google Scholar] [CrossRef]
- Pablo, D.J.; Simón, D.C. Monitorización intraoperatoria de los nervios laríngeos superior e inferior en cirugía de tiroides y paratiroides. Rev. Colomb. Cir. 2012, 27, 298–305. Available online: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S2011-75822012000400009&lng=en. (accessed on 2 March 2023).
- Sheahan, P.; Murphy, M.S. Thyroid tubercle of zuckerkandl: Importance in thyroid surgery. Laryngoscope 2011, 121, 2335–2337. [Google Scholar] [CrossRef]
- Bobanga, I.D.; McHenry, C.R. Treatment of patients with Graves’ disease and the appropriate extent of thyroidectomy. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101319. [Google Scholar] [CrossRef] [PubMed]
- Lang, B.H.H.; Wong, C.K.H.; Ma, E.P.-M. A systematic review and meta-analysis on acoustic voice parameters after uncomplicated thyroidectomy. Laryngoscope 2016, 126, 528–537. [Google Scholar] [CrossRef]
- Haney, M.M.; Hamad, A.; Leary, E.; Bunyak, F.; Lever, T.E. Automated Quantification of Vocal Fold Motion in a Recurrent Laryngeal Nerve Injury Mouse Model. Laryngoscope 2019, 129, E247–E254. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Li, Y.; Xu, W.; Cheng, L.; Ren, H. Clinical and Electromyographic Characteristics of Unilateral Vocal Fold Paralysis With Lower Cranial Nerve Injury. J. Voice 2017, 31, 126.e1–126.e6. [Google Scholar] [CrossRef] [PubMed]
- Chiang, F.-Y.; Lu, I.-C.; Kuo, W.-R.; Lee, K.-W.; Chang, N.-C.; Wu, C.-W. The mechanism of recurrent laryngeal nerve injury during thyroid surgery—The application of intraoperative neuromonitoring. Surgery 2008, 143, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Lu, I.-C.; Chu, K.-S.; Tsai, C.-J.; Wu, C.-W.; Kuo, W.-R.; Chen, H.-Y.; Lee, K.-W.; Chiang, F.-Y. Optimal Depth of NIM EMG Endotracheal Tube for Intraoperative Neuromonitoring of the Recurrent Laryngeal Nerve During Thyroidectomy. World J. Surg. 2008, 32, 1935–1939. [Google Scholar] [CrossRef] [PubMed]
- Sancho Fornos, S.; Vaqué Urbaneja, J.; Ponce Marco, J.L.; Palasí Giménez, R.; Herrera Vela, C. Complicaciones de la cirugía tiroidea. Cirugía Española 2001, 69, 198–203. [Google Scholar] [CrossRef]
- Henry, B.M.; Tomaszewski, K.A.; Walocha, J.A. Methods of Evidence-Based Anatomy: A guide to conducting systematic reviews and meta-analysis of anatomical studies. Ann. Anat.-Anat. Anz. 2016, 205, 16–21. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S.; Ben Van Den, A. Cochrane Handbook for Systematic Reviews of Interventions. Int. Coach. Psychol. Rev. 2020, 15, 123–125. [Google Scholar] [CrossRef]
- Chiang, F.-Y.; Lee, K.-W.; Chen, H.-C.; Chen, H.-Y.; Lu, I.-C.; Kuo, W.-R.; Hsieh, M.-C.; Wu, C.-W. Standardization of Intraoperative Neuromonitoring of Recurrent Laryngeal Nerve in Thyroid Operation. World J. Surg. 2010, 34, 223–229. [Google Scholar] [CrossRef]
- Le, V.Q.; Ngo, Q.D.; Ngo, X.Q. Nonrecurrent laryngeal nerve in thyroid surgery: Frequency, anatomical variations according to a new classification and surgery consideration. Head Neck 2019, 41, 2969–2975. [Google Scholar] [CrossRef]
- Le, Q.V.; Ngo, D.Q.; Ngo, Q.X. Non-recurrent laryngeal nerve in thyroid surgery: A report of case series in Vietnam and literature review. Int. J. Surg. Case Rep. 2018, 50, 56–59. [Google Scholar] [CrossRef]
- Prades, J.M.; Dubois, M.D.; Dumollard, J.M.; Tordella, L.; Rigail, J.; Timoshenko, A.P.; Peoc’h, M. Morphological and functional asymmetry of the human recurrent laryngeal nerve. Surg. Radiol. Anat. 2012, 34, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Beneragama, T.; Serpell, J.W. Extralaryngeal bifurcation of the recurrent laryngeal nerve: A common variation. ANZ J. Surg. 2006, 76, 928–931. [Google Scholar] [CrossRef]
- Dolezel, R.; Jarosek, J.; Hana, L.; Ryska, M. Clinical relevance and surgical anatomy of non-recurrent laryngeal nerve: 7 year experience. Surg. Radiol. Anat. 2015, 37, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Gurleyik, E.; Cetin, F.; Dogan, S.; Yekenkurul, E.; Onsal, U.; Gürsoy, F.; Ipor, A. Displacement of the Recurrent Laryngeal Nerve in Patients with Recurrent Goiter Undergoing Redo Thyroid Surgery. J. Thyroid. Res. 2018, 48, 4763712. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.H.; Park, H.T.; Yang, Y.S. Characteristic travelling patterns of non-recurrent laryngeal nerves. J. Laryngol. Otol. 2014, 128, 534–539. [Google Scholar] [CrossRef]
- Hong, Y.T.; Hong, K.H. The Relationship Between the Non-recurrent Laryngeal Nerve and the Inferior Thyroid Artery. Indian J. Surg. 2018, 80, 109–112. [Google Scholar] [CrossRef]
- Ng, C.; Woess, C.; Maier, H.; Schmidt, V.-M.; Lucciarini, P.; Öfner, D.; Rabl, W.; Augustin, F. Nerve at risk: Anatomical variations of the left recurrent laryngeal nerve and implications for thoracic surgeons. Eur. J. Cardio-Thorac. Surg. 2020, 58, 1201–1205. [Google Scholar] [CrossRef]
- Page, C.; Monet, P.; Peltier, J.; Bonnaire, B.; Strunski, V. Non-recurrent laryngeal nerve related to thyroid surgery: Report of three cases. J. Laryngol. Otol. 2008, 122, 757–761. [Google Scholar] [CrossRef]
- Shao, T.; Yang, W.; Zhang, T.; Wang, Y.; Jin, X.; Li, Q.; Kuang, J.; Qiu, W.; Chu, P.G.; Yen, Y. A Newly Identified Variation at the Entry of the Recurrent Laryngeal Nerve into the Larynx. J. Investig. Surg. 2010, 23, 314–320. [Google Scholar] [CrossRef]
- Shao, T.; Qiu, W.; Yang, W. Confirmation of an anatomic variation of the recurrent laryngeal nerve at site of entry into the larynx in Chinese population. Am. J. Otolaryngol. 2015, 37, 351–355. [Google Scholar] [CrossRef]
- Qiao, N.; Wu, L.; Gao, W.; Qu, F.; Duan, P.; Cao, C.; Li, P.; Sun, B.; Wang, G. Anatomic Characteristics, Identification, and Protection of the Nonrecurrent Laryngeal Nerve during Thyroidectomy. Otolaryngol. Neck Surg. 2017, 157, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Xiang, M.; Wu, H.; Ma, Y.; Chen, L.; Cheng, L. Routine exposure of recurrent laryngeal nerve in thyroid surgery can prevent nerve injury. Neural Regen. Res. 2013, 8, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.M.; Fahim, D.K.; Gemechu, J.M. Anatomical Variations of the Recurrent Laryngeal Nerve and Implications for Injury Prevention during Surgical Procedures of the Neck. Diagnostics 2020, 10, 670. [Google Scholar] [CrossRef] [PubMed]
- Yin, C.; Song, B.; Wang, X. Anatomical Variations in Recurrent Laryngeal Nerves in Thyroid Surgery. Ear Nose Throat J. 2021, 100, 930S–936S. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Wang, K. A novel variation of the recurrent laryngeal nerve. BMC Surg. 2017, 17, 66. [Google Scholar] [CrossRef]
- Cetin, F.; Gürleyik, E.; Dogan, S. Morphology and Functional Anatomy of the Recurrent Laryngeal Nerve with Extralaryngeal Terminal Bifurcation. Anat. Res. Int. 2016, 2016, 503170. [Google Scholar] [CrossRef]
- Uludag, M.; Isgor, A.; Yetkin, G.; Citgez, B. Anatomic variations of the non-recurrent inferior laryngeal nerve. BMJ Case Rep. 2009, 2009, bcr1020081107. [Google Scholar] [CrossRef]
- Babademez, M.A.; Günbey, E.; Ozmen, E.; Celik, E. Anomalous Relationship of Coexisting Ipsilateral Recurrent and Nonrecurrent Inferior Laryngeal Nerves during Thyroid Surgery. J. Craniofac. Surg. 2013, 24, e190–e192. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Won, D.-Y.; Oh, S.-H.; Hong, S.-Y.; Woo, R.-S.; Baik, T.-K.; Yoo, H.-I.; Song, D.-Y. Three concurrent variations of the aberrant right subclavian artery, the non-recurrent laryngeal nerve and the right thoracic duct. Folia Morphol. 2016, 75, 560–564. [Google Scholar] [CrossRef]
- Moradi, A.; Hajian, A. The intracranial branch; A rare anatomical variation of the recurrent laryngeal nerve; Case report. Int. J. Surg. Case Rep. 2021, 78, 9–11. [Google Scholar] [CrossRef]
- Obaid, T.; Kulkarni, N.; Pezzi, T.A.; Turkeltaub, A.E.; Pezzi, C.M. Coexisting right nonrecurrent and right recurrent inferior laryngeal nerves: A rare and controversial entity. Surg. Today 2014, 44, 2392–2396. [Google Scholar] [CrossRef] [PubMed]
- Piperos, T.; Kaklamanos, I.; Chrysikos, D.; Zarokosta, M.; Boumpa, E.; Zoulamoglou, M.; Kalles, V.; Gkogka, G.-I.; Mariolis-Sapsakos, T. Abnormal distance of the extralaryngeal bifurcation point of the recurrent laryngeal nerve from the cricothyroid joint. J. Surg. Case Rep. 2018, 2018, rjx257. [Google Scholar] [CrossRef] [PubMed]
- Ayerdi, J.; Gupta, S.K.; Sampson, L.N.; Deshmukh, N. Recognition of a non-recurrent laryngeal nerve during carotid endarterectomy. Cardiovasc. Surg. 2002, 10, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Chrysikos, D.; Sgantzos, M.; Tsiaoussis, J.; Noussios, G.; Troupis, T.; Protogerou, V.; Spartalis, E.; Triantafyllou, T.; Mariolis-Sapsakos, T. Non-Recurrent Right Laryngeal Nerve: A Rare Anatomic Variation Encountered During a Total Thyroidectomy. Acta Medica 2019, 62, 69–71. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Iorgulescu, R.; Bistriceanu, I.; Badanoiu, D.; Calin, C.; Capatana, C.; Iordache, N. Non-recurrent inferior laryngeal nerve: Case report and review of the literature. J. Med. Life 2014, 7, 90–94. [Google Scholar] [PubMed]
- Manoglu, B.; Yılmaz, E.M.; Erdogan, A.; Özkan, M.B.; Ozciftci, V.M. Report of a rare case: Double recurrent laryngeal nerve. Turk. J. Surg. 2015, 32, 298–299. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Kanazawa, J.; Numata, N.; Hitomi, J. The right-sided aortic arch with unusual course of bilateral recurrent laryngeal nerves: A report of rare variations. Surg. Radiol. Anat. 2017, 39, 223–228. [Google Scholar] [CrossRef]
- De Freitas, C.A.F.; Levenhagen, M.M.M.D.; Constantino, I.S.; Paroni, A.F.; Martins, M.R. Relation of Nonrecurrent Laryngeal Nerve with Zuckerkandl’s Tubercle. Case Rep. Surg. 2020, 2020, 2459321. [Google Scholar] [CrossRef]
- Ahumada, N.G.; Hojaij, F.C.; Cunico, C.; Akahane, H.G.K.; Leitão, C.A.; Matias, J.E.F. Left Nonrecurrent Laryngeal Nerve: A Very Unusual Finding during Thyroid Surgery. Case Rep. Surg. 2022, 2022, 4632501. [Google Scholar] [CrossRef]
- Wang, J.J.; Lu, I.-C.; Chang, P.-Y.; Wu, C.-W.; Wang, L.-F.; Huang, T.-Y.; Chiang, F.-Y. Peculiar anatomic variation of recurrent laryngeal nerve and EMG change in a patient with right substernal goiter and pre-operative vocal cord palsy—Case report. Gland. Surg. 2020, 9, 802–805. [Google Scholar] [CrossRef]
- Gurleyik, G.; Torun, M.; Gurleyik, E. Nonrecurrent Laryngeal Nerve: Precise Detection by Electrophysiological Nerve Monitoring. Cureus 2018, 10, e2670. [Google Scholar] [CrossRef] [PubMed]
- Casal, D.; Peças, A.; Sousa, D.; Rosa-Santos, J. A non-recurrent inferior laryngeal nerve in a man undergoing thyroidectomy: A case report. J. Med. Case Rep. 2010, 4, 386. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Uludag, M.; Aygun, N.; Kartal, K.; Besler, E.; Isgor, A. Innervation of the human posterior cricoarytenoid muscle by the external branch of the superior laryngeal nerve. Head Neck 2017, 39, 2200–2207. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. (2021) (Version 4.0) [Computer Software]. Available online: https://cran.r-project.org (accessed on 4 April 2021).
- Henry, B.M.; Tomaszewski, K.; Ramakrishnan, P.K.; Roy, J.; Vikse, J.; Loukas, M.; Tubbs, R.S.; Walocha, J.A. Development of the Anatomical Quality Assessment (AQUA) Tool for the quality assessment of anatomical studies included in meta-analyses and systematic reviews. Clin. Anat. 2017, 30, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Gurleyik, E.; Dogan, S.; Cetin, F. Coexistence of Right Nonrecurrent Nerve and Bifurcated Recurrent Laryngeal Nerve Pointed by Zuckerkandl’s Tubercle. Cureus 2017, 9, e1078. [Google Scholar] [CrossRef]
- Kostek, M.; Caliskan, O.; Yanar, C.; Cakir, Y.; Uludag, M. The most common anatomical variation of recurrent laryngeal nerve: Extralaryngeal branching. Sisli Etfal Hast. Tip Bul. 2021, 55, 294–303. [Google Scholar] [CrossRef]
- Bakalinis, E.; Makris, I.; Demesticha, T.; Tsakotos, G.; Skandalakis, P.; Filippou, D. Non-recurrent Laryngeal Nerve and Concurrent Vascular Variants: A Review. Acta Med. Acad. 2018, 47, 186. [Google Scholar] [CrossRef]
- LeClair, K.; Bell, K.J.L.; Furuya-Kanamori, L.; Doi, S.A.; Francis, D.O.; Davies, L. Evaluation of Gender Inequity in Thyroid Cancer Diagnosis: Differences by Sex in US Thyroid Cancer Incidence Compared With a Meta-analysis of Subclinical Thyroid Cancer Rates at Autopsy. JAMA Intern. Med. 2021, 181, 1351. [Google Scholar] [CrossRef]
- Ling, X.Y.; Smoll, N.R. A systematic review of variations of the recurrent laryngeal nerve. Clin. Anat. 2016, 29, 104–110. [Google Scholar] [CrossRef]
- Polednak, A.P. Relationship of the recurrent laryngeal nerve to the inferior thyroid artery: A comparison of findings from two systematic reviews. Clin. Anat. 2017, 30, 318–321. [Google Scholar] [CrossRef]
- Polednak, A.P. Anatomical variation in the right non-recurrent laryngeal nerve reported from studies using pre-operative arterial imaging. Surg. Radiol. Anat. SRA 2019, 41, 943–949. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Study Design | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | ||
| [3] | Prospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [13] | Retrospective study | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | N | Y | Y | Y | NA | Y |
| [14] | Case report | Y | Y | N | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | NA | N |
| [28] | Retrospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | NA | Y |
| [29] | Multiple-case study | Y | Y | Y | Y | N | Y | Y | N | N | Y | N | N | Y | N | N | Y | Y | N | Y | Y | N | Y | N | NA | Y |
| [30] | Prospective study | Y | N | Y | Y | N | Y | Y | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | NA | Y |
| [31] | Multiple-case study | Y | Y | Y | Y | N | Y | Y | N | Y | Y | N | N | Y | Y | Y | Y | Y | N | Y | Y | N | Y | N | NA | Y |
| [32] | Prospective study | Y | Y | Y | N | Y | Y | N | N | Y | Y | N | Y | N | N | Y | U | Y | Y | U | Y | Y | Y | Y | NA | NY |
| [33] | Retrospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [34] | Retrospective study | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | N | Y | Y | N | NA | Y |
| [35] | Retrospective study | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | U | U | Y | N | Y | Y | Y | N | Y | Y | N | Y | NA | Y |
| [36] | Retrospective study | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | NA | Y |
| [37] | Multiple-case study | Y | Y | Y | Y | N | Y | Y | N | N | Y | Y | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [38] | Retrospective study | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | N | Y | Y | N | NA | Y |
| [39] | Retrospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [40] | Retrospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [41] | Retrospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [42] | Retrospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [43] | Retrospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [44] | Prospective clinical trial | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [45] | Case report | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | N | Y | N | Y | N | Y | Y | Y | NA | N |
| [46] | Prospective study | Y | Y | Y | Y | Y | Y | N | N | Y | Y | Y | N | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | NA | Y |
| [47] | Multiple-case study | Y | Y | Y | Y | N | Y | Y | N | N | Y | N | N | Y | N | N | Y | Y | N | Y | Y | N | Y | N | NA | Y |
| [48] | Case report | Y | N | Y | Y | N | Y | Y | Y | Y | N | Y | N | N | N | Y | Y | N | N | Y | N | Y | N | Y | NA | Y |
| [48] | Case report | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | N | Y | N | Y | N | Y | Y | Y | NA | N |
| [49] | Case report | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | N | Y | N | Y | N | Y | Y | Y | NA | Y |
| [49] | Prospective study | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| [50] | Case report | Y | N | Y | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | N | Y | N | Y | N | Y | Y | Y | NA | N |
| [51] | Case report | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | N | Y | N | Y | N | Y | Y | Y | NA | N |
| [52] | Case report | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | Y | Y | Y | N | Y | N | Y | N | Y | Y | Y | NA | Y |
| [53] | Case report | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | NA | Y |
| [54] | Case report | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | NA | Y |
| [55] | Case report | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | Y | NA | N |
| [56] | Case report | Y | Y | Y | Y | N | Y | N | Y | Y | Y | N | Y | N | N | Y | Y | N | N | N | Y | Y | N | N | NA | Y |
| [7] | Prospective study | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | N | Y | Y | N | Y | N | Y | Y | N | Y | N | Y | NA | Y |
| [57] | Case report | Y | Y | Y | Y | Y | N | Y | Y | Y | N | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | NA | N |
| [58] | Case report | Y | Y | Y | N | Y | Y | N | N | Y | N | N | Y | N | Y | N | Y | N | N | N | Y | N | N | Y | NA | Y |
| [59] | Case report | Y | Y | Y | Y | Y | N | N | Y | Y | Y | N | N | N | Y | Y | U | Y | Y | Y | U | Y | N | Y | NA | Y |
| [60] | Case report | Y | N | N | Y | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | N | Y | N | Y | N | Y | Y | Y | NA | N |
| [61] | Case report | Y | Y | Y | N | Y | Y | N | N | Y | Y | N | Y | N | N | Y | N | Y | Y | N | Y | N | Y | N | NA | N |
| [62] | Case report | Y | Y | Y | N | Y | Y | U | U | N | Y | Y | N | Y | N | N | Y | Y | Y | N | Y | Y | N | N | NA | N |
| [63] | Prospective study | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | N | NA | Y |
| Author & Year | Type of Study & N | Incidence and Characteristics | Statistical Values | Geographic Region | Laterality | Gender |
|---|---|---|---|---|---|---|
| [12] | Retrospective study | 4 patients with NRLN, 1400 patients with RLN bilateral exposition, 300 witch unilateral exposition of RLN | Not presented | Poland | Uni & bilateral | Not mentioned |
| [13] | Case report (1 patient) | 1 case of right NRLN type I | Not presented | Turkey | Right | 1 woman (100%) |
| [3] | Nonrandomized prospective study (253 patients) | 57 RLN with 2 branches 4 RLN with 3 branches Position of RLN respect to inferior thyroid artery (ITA) Posterior: Right: 163 Left: 181 Anterior: Right: 61 Left: 50 Between the inferior thyroid artery branches Right: 19 Left: 13 | The distributions of the three types of relationships between the RLNs and the ITA differ significantly (p < 0.05). There was no statistically significant difference between the sides regarding the relationship of RLNs with ITA (p > 0.05). | Turkey | bilateral | 205 men (81%) & 48 women (19%) |
| [28] | Retrospective study | 603 patients, 1 NRLN type I and 3 NRLN type II | Not presented | Korea | Right | Not mentioned |
| [29] | Case series (4 patients) | 4 NRLN (1 type II A) | Not presented | Vietnam | Right | 4 women (100%) |
| [30] | Prospective study (2158 patients) | 16 patients with NRLN | Not presented | Vietnam | Not mentioned | 14 women (88%) & 2 men (12%) |
| [31] | Case series (6 bodies) | Left RLN average length was 136.6 mm Right RLN average length was 75 mm | A value p < 0.05 was considered statistically significant | France | Bilateral | 6 women (100%) |
| [32] | Prospective study (137 patients) | 1 right NRLN. RLN bifurcation before entering the larynx on the right side, 49 cases (35.77%) RLN bifurcation before entering the larynx on the left side, 28 cases (20.32%) Ramifications on both sides of the RLN, 14 cases (10.22%) | There was a statistically significant difference between the variations due to bifurcation on the right side and the bifurcation on the left side (p ≤ 0.05). | Australia | Bilateral | 114 women (83.21%) & 23 Men (16.79%) |
| [33] | Retrospective study | 766 patients, 1439 RLN (725 right and 714 left) and 4 NRLN type IIA | Not presented | France | Uni & bilateral | 615 women (80.2%) & 151 men (19.8%) |
| [34] | Retrospective study | 49 patients with 61 RLN (38 right and 23 left) | Not presented | Turkey | Uni & bilateral | 47 females (96%) & 2 men (4%) |
| [35] | Retrospective study (2658 patients) | 15 patients with NRLN | Not presented | Korea | Not mentioned | 2179 women (82%) & 479 men (18%) |
| [36] | Retrospective study (16 patients) | 16 cases of NRLN | Not presented | Korea | Right | 14 women (88%) & 2 men (12%) |
| [37] | Case series (100 bodies) | 11 left RLN separates above the aortic arch crossing it with a considerable distance from the vagus nerve 48 left RLN separates at the aortic arch level 41 left RLN emerges from the vagus nerve in perpendicular direction under the aortic arch | There was no association between sex and course of RLN (p = 0.386). | Austria | Left | 72 men (72%) & 28 women (28%) |
| [38] | Retrospective study (993 patients) | 1 patient with right NRLN type I 1 patient with right NRLN type II | Not presented | France | Right | 773 women (77.84%) & 220 men (22.16%) |
| [40] | Retrospective study (2068 pacientes) | Variation in the site of branching to the larynx by a fan-shaped recurrent laryngeal nerve on the right side (155 cases) and left side (46 cases). Variation in the site of branching to the larynx by a recurrent laryngeal nerve with extralaryngeal branches of the two-branch subtype on the right side (129 cases) and left side (181 cases) Variation in the site of branching to the larynx by a recurrent laryngeal nerve with extralaryngeal branches of the two-branch subtype dividing the larynx separately on the right side (111 cases) and 170 cases on the left side. | There was a statistically significant difference when comparing the branching of the recurrent laryngeal nerve with a fan shape on the left and right sides (p < 0.001) There was a statistically significant difference when comparing the branching of the recurrent laryngeal nerve with extralaryngeal branches on the left and right sides (p < 0.001). | China | Bilateral | Not mentioned |
| [41] | Retrospective study (7392 patients) | 28 Right NRLN 5 type I 19 type IIa 4 type IIb | For the enumeration data they applied the I2 test and for the measurement data they applied the 2-independent-sample t-test. The difference was statistically significant with p < 0.05. The appearance of NRNL was not significantly associated with sex, age, nature of the tumor, number of lesions, or monitor use (p > 0.05). | China | Right | 1492 men (20.1%) & 5900 women (79.8%) |
| [41] | Retrospective (2068 patients) | 322 RLN branched extralaryngeally According to number of branches per side: 131 extralaryngeal branching right RLNs (129 RLNs with two branches, 2 RLNs with three branches, 0 RLNs with four branches) 191 extralaryngeal branching left RLNs (181 RLNs with two branches, 7 RLNs with three branches, 3 RLNs with four branches) | Value was significantly lower than that of the variation that occurred in the left side (p < 0.001). The variation occurred more frequently on the right side than on the left (p < 0.0001) | China | Bilateral | 1894 females (91.59%) y 174 males (8.41%) |
| [42] | Retrospective study (5344 patients) | Anatomical variations of the RLN in the cases of the dissection group (23.4%/n = 128)
| There were no significant differences in sex, age, thyroid disease, type of surgery, and number of surgeries between the two groups using chi-square analysis (p > 0.05). | China | Bilateral | 1418 males (26.53%) y 3926 females (73.47%) |
| [43] | Retrospective study (55 cadavers) | Right side: Right RLN presents 2–5 extralaryngeal branches (89.1%). 22 bifurcated RLN, 15 trifurcated RLN, 12 multi-branched RLN, 6 unbranched RLN. Left side: left RLN presents 2–5 extralaryngeal branches (74.6%). 15 bifurcated RLN, 19 trifurcated RLN, 7 multi-branched RLN, 14 unbranched RLN. | Data were quantitatively analyzed with McNemar’s test and Fisher’s exact test. Statistical significance was determined based on a value of p < 0.05. | USA | Bilateral | 28 males (50.9%) y 27 females (49.1%) |
| [44] | Prospective clinical essay (294 patients) | RLN by number of bifurcations per side: Left side: 159 with one bifurcation (type I). 60 with two bifurcations (type II). 15 with three bifurcations (type III). Right side: 170 with one bifurcation (type I). 63 with two bifurcations (type II). 11 with three bifurcations (type III). 2 right NRLN (type IV) | There was no statistically significant difference for sideways comparison (p > 0.05) | China | Uni & bilateral | 49 men (16.7%) & 245 women (83.3%) |
| [45] | Case report (1 patient) | 1 left NLR under Inferior Thyroid artery | Not presented | China | Left | Woman (100%) |
| [46] | Prospective study | 67 RLN in 36 patients. | Not presented | Turkey | Uni & bilateral | 30 Women (83.33%), 6 men (16.67%) |
| [66] | Case report | 1 patient with RLN with an extralaryngeal bifurcation | Not presented | Turkey | Right | Not mentioned |
| [47] | Case series (2 patients) | NRLN originating from the vagus nerve, presenting 2 branches before passing through Berry’s ligament, 1 case (50%) NRLN originating in the vagus nerve, following its normal course below the trunk of the inferior thyroid artery, 1 case (50%) | Not presented | Turkey | Unilateral | Not mentioned |
| [48] | Case study (1 patient) | Coexistence of right RLN with NRLN type II | Not presented | Turkey | Right | 1 Woman (100%) |
| [49] | Case study (1 body) | Coexistence of NRLN type II, aberrant subclavian artery & thoracic duct type I on the right side | Not presented | South korea | Right | 1 Man (100%) |
| [50] | Case report (1 patient) | Left and right RLN | Not presented | Iran | Bilateral | 1 woman (100%) |
| [51] | Case study (1 patient) | Coexistence of right RLN with NRLN | Not presented | Japan | Right | 1 Man (100%) |
| [52] | Case study (1 patient) | Distance of 7 cm between the extralaryngeal bifurcation to the cricothyroid joint, 1 case (100%) | Not presented | Greece | Left | 1 woman (100%) |
| [53] | Case study (1 patient) | 1 patient with right NRLN | Not presented | USA | Right | 1 woman (100%) |
| [54] | Case report | 1 patient with NRLN | Not presented | Greece | Right | Woman (100%) |
| [55] | Case report (1 patient) | Right NRLN emerges from vagus nerve | Not presented | Rumania | Right | 1 Woman (100%) |
| [56] | Case report (1 patient) | Left double RLN | Not presented | Turkey | Left | 1 Woman (100%) |
| [7] | Prospective study (2404 patients) | According to extralaryngeal divergence (type I):
| The laterality of the NLR variations was not statistically significant (p = 0.07) | China | Bilateral | 510 men (21.2%) & 1894 women (78.8%) |
| [57] | Case report (1 patient) | Bilateral RLN | Not presented | Japan | Bilateral | Man (100%) |
| [58] | Case study (1 patient) | Right NRLN with thyroid tissue in zuckerkandl tubercle region | Not presented | Brazil | Right | 1 woman (100%) |
| [59] | Case report (1 case) | 1 (100%) left NRLN | Not presented | Brazil | Left | Woman (100%) |
| [60] | Case report (1 patient) | Right RLN lies over the thyroid tumor and compressed against the clavicle | Not presented | Taiwán | Right | Man (100%) |
| [61] | Case report | 1 Patient with right NRLN | Not presented | Turkey | Right | Woman (100%) |
| [62] | Case report | 1 (100%) of NRLN | Not presented | Portugal | Right | Man (100%) |
| [63] | Prospective study (94 pacientes) | 77 RLNs bifurcate before entering the larynx. 36 right RLN branched. 41 branched left RLN Bilateral examination (n = 67):
| There was no significant difference in branching rates between sides (p = 0.196). There was no significant difference between the sides in terms of branching (p = 0.471). | Turkey | Bilateral and unilateral | 76 females (80.9%) y 18 males (19.2%) |
| Study | N Total | Men and % | Women and % | Does Not Specify and % |
|---|---|---|---|---|
| [3] | 253 | 205/81% | 48/19% | 0/0% |
| [5] | 5344 | 1418/26.53% | 3926/73.47% | 0/0% |
| [8] | 2068 | 174/8.41% | 1894/91.59% | 0/0% |
| [13] | 1700 | 0/0% | 0/0% | 1700/100% |
| [28] | 603 | 0/0% | 0/0% | 603/100% |
| [29] | 4 | 0/0% | 4/100% | 0/0% |
| [30] | 2158 | 0/0% | 0/0% | 2158/100% |
| [31] | 6 | 0/0% | 6/100% | 0/0% |
| [32] | 137 | 23/16.79% | 114/53.21% | 0/0% |
| [33] | 766 | 151/19.8% | 615/80.2% | 0/0% |
| [34] | 49 | 2/4.08% | 47/95.92 | 0/0% |
| [35] | 2658 | 479/18.02% | 2179/81.98% | 0/0% |
| [36] | 16 | 2/12.5% | 14/87.5% | 0/0% |
| [36] | 100 | 72/72% | 28/28% | 0/0% |
| [38] | 993 | 220/22.16% | 763/77.84% | 0/0% |
| [39] | 2068 | 0/0% | 0/0% | 2068/100% |
| [40] | 2404 | 510/21.2% | 1894/78.8% | 0/0% |
| [41] | 7392 | 1492/20.2% | 5900/79.8% | 0/0% |
| [43] | 55 | 28/50.9% | 27/49.1% | 0/0% |
| [44] | 294 | 49/16.7% | 245/53.3% | 0/0% |
| [46] | 36 | 6/16.77% | 30/83.33% | 0/0% |
| [47] | 2 | 0/0% | 0/0% | 2/100% |
| [59] | 94 | 18/19.2% | 76/80.9% | 0/0% |
| Mean Famele and Male | - | 27.88% | 72.12% | - |
| Author | N Patients | Prevalence Number and Percentage |
|---|---|---|
| [3] | 253 | 16/6.32% |
| [8] | 2068 | 601/29.06% |
| [12] | 1700 | 4/0.24% |
| [15] | 603 | 4/0.66% |
| [27] | 2658 | 15/0.56% |
| [64] | 16 | 16/100% |
| [28] | 4 | 4/100% |
| [11] | 2158 | 16/0.74% |
| [30] | 6 | 6/100% |
| [31] | 137 | 101/73.72% |
| [32] | 766 | 4/0.52% |
| [33] | 49 | 16/32.65% |
| [36] | 100 | 100/100% |
| [37] | 993 | 3/0.30% |
| [38] | 2068 | 858/41.49% |
| [40] | 7392 | 28/0.38% |
| [41] | 5344 | 128/2.39% |
| [42] | 55 | 55/100% |
| [43] | 294 | 294/100% |
| [45] | 36 | 36/100% |
| [66] | 2 | 2/100% |
| [68] | 2404 | 690/28.7% |
| [58] | 94 | 40/42.55% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valenzuela-Fuenzalida, J.J.; Baeza-Garrido, V.; Navia-Ramírez, M.F.; Cariseo-Ávila, C.; Bruna-Mejías, A.; Becerra-Farfan, Á.; Lopez, E.; Orellana Donoso, M.; Loyola-Sepulveda, W. Systematic Review and Meta-Analysis: Recurrent Laryngeal Nerve Variants and Their Implication in Surgery and Neck Pathologies, Using the Anatomical Quality Assurance (AQUA) Checklist. Life 2023, 13, 1077. https://doi.org/10.3390/life13051077
Valenzuela-Fuenzalida JJ, Baeza-Garrido V, Navia-Ramírez MF, Cariseo-Ávila C, Bruna-Mejías A, Becerra-Farfan Á, Lopez E, Orellana Donoso M, Loyola-Sepulveda W. Systematic Review and Meta-Analysis: Recurrent Laryngeal Nerve Variants and Their Implication in Surgery and Neck Pathologies, Using the Anatomical Quality Assurance (AQUA) Checklist. Life. 2023; 13(5):1077. https://doi.org/10.3390/life13051077
Chicago/Turabian StyleValenzuela-Fuenzalida, Juan José, Vicente Baeza-Garrido, María Fernanda Navia-Ramírez, Carolina Cariseo-Ávila, Alejandro Bruna-Mejías, Álvaro Becerra-Farfan, Esteban Lopez, Mathias Orellana Donoso, and Walter Loyola-Sepulveda. 2023. "Systematic Review and Meta-Analysis: Recurrent Laryngeal Nerve Variants and Their Implication in Surgery and Neck Pathologies, Using the Anatomical Quality Assurance (AQUA) Checklist" Life 13, no. 5: 1077. https://doi.org/10.3390/life13051077
APA StyleValenzuela-Fuenzalida, J. J., Baeza-Garrido, V., Navia-Ramírez, M. F., Cariseo-Ávila, C., Bruna-Mejías, A., Becerra-Farfan, Á., Lopez, E., Orellana Donoso, M., & Loyola-Sepulveda, W. (2023). Systematic Review and Meta-Analysis: Recurrent Laryngeal Nerve Variants and Their Implication in Surgery and Neck Pathologies, Using the Anatomical Quality Assurance (AQUA) Checklist. Life, 13(5), 1077. https://doi.org/10.3390/life13051077