
Micropulse Laser Trabeculoplasty with 577 nm Wavelength at 1500 or 1000 mW for Primary Open-Angle Glaucoma: A Pilot Study

 , , , ,
, , , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
MLT Technique
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, P.J.B.; Keeffe, P.J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef] [PubMed]
- Janz, N.K.; Wren, P.A.; Lichter, P.R.; Musch, D.C.; Gillespie, B.W.; Guire, K.E.; Mills, R.P.; CIGTS Study Group. The Collaborative Initial Glaucoma Treatment Study: Interim quality of life findings after initial medical or surgical treatment of glaucoma. Ophthalmology 2001, 108, 1954–1965. [Google Scholar] [CrossRef] [PubMed]
- Lichter, P.R.; Musch, D.C.; Gillespie, B.W.; Guire, K.E.; Janz, N.K.; Wren, P.A.; Mills, R.P.; CIGTS Study Group. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology 2001, 108, 1943–1953. [Google Scholar] [CrossRef] [PubMed]
- Samples, J.R.; Singh, K.; Lin, S.C.; Francis, B.A.; Hodapp, E.; Jampel, H.D.; Smith, S.D. Laser trabeculoplasty for open-angle glaucoma: A report by the american academy of ophthalmology. Ophthalmology 2011, 118, 2296–2302. [Google Scholar] [CrossRef]
- Gazzard, G.; Konstantakopoulou, E.; Garway-Heath, D.; Garg, A.; Vickerstaff, V.; Hunter, R.; Ambler, G.; Bunce, C.; Wormald, R.; Nathwani, N.; et al. Selective laser trabeculoplasty versus drops for newly diagnosed ocular hypertension and glaucoma: The LiGHT RCT. Health Technol. Assess. 2019, 23, 1–102. [Google Scholar] [CrossRef]
- Gazzard, G.; Konstantakopoulou, E.; Garway-Heath, D.; Garg, A.; Vickerstaff, V.; Hunter, R.; Ambler, G.; Bunce, C.; Wormald, R.; Nathwani, N.; et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): A multicentre randomised controlled trial. Lancet 2019, 393, 1505–1516. [Google Scholar] [CrossRef]
- Wang, H.; Cheng, J.-W.; Wei, R.-L.; Cai, J.-P.; Li, Y.; Ma, X.-Y. Meta-analysis of selective laser trabeculoplasty with argon laser trabeculoplasty in the treatment of open-angle glaucoma. Can. J. Ophthalmol. 2013, 48, 186–192. [Google Scholar] [CrossRef]
- Wise, J.B.; Witter, S.L. Argon laser therapy for open-angle glaucoma. A pilot study. Arch. Ophthalmol. 1979, 97, 319–322. [Google Scholar] [CrossRef]
- Worthen, D.M.; Wickham, M.G. Argon laser trabeculotomy. Trans. Am. Acad. Ophthalmol. Otolaryngol. 1974, 78, OP371–OP375. [Google Scholar]
- Brooks, A.M.; West, R.H.; Gillies, W.E. Argon laser trabeculoplasty five years on. J. Ophthalmol. 1988, 16, 343–351. [Google Scholar] [CrossRef]
- Hong, C.; Kitazawa, Y.; Tanishima, T. Influence of argon laser treatment of glaucoma on corneal endothelium. Jpn. J. Ophthalmol. 1983, 27, 567–574. [Google Scholar]
- Latina, M.A.; Park, C. Selective targeting of trabecular meshwork cells: In Vitro studies of pulsed and CW laser interactions. Exp. Eye Res. 1995, 60, 359–371. [Google Scholar] [CrossRef]
- Leahy, K.E.; White, A.J. Selective laser trabeculoplasty: Current perspectives. Clin. Ophthalmol. 2015, 9, 833–841. [Google Scholar]
- Kramer, T.R.; Noecker, R.J. Comparison of the morphologic changes after selective laser trabeculoplasty and argon laser trabeculoplasty in human eye bank eyes. Ophthalmology 2001, 108, 773–779. [Google Scholar] [CrossRef]
- Koenig, L.R.; Kovacs, K.D.; Gupta, M.P.; Van Tassel, S.H. Hypopyon following selective laser trabeculoplasty. Am. J. Ophthalmol. Case Rep. 2020, 18, 100675. [Google Scholar] [CrossRef]
- Zhou, Y.; Aref, A.A. A review of selective laser trabeculoplasty: Recent findings and current perspectives. Ophthalmol. Ther. 2017, 6, 19–32. [Google Scholar] [CrossRef]
- Songm, J. Complications of selective laser trabeculoplasty: A review. Clin. Ophthalmol. 2016, 10, 137–143. [Google Scholar] [CrossRef]
- Zhang, H.Y.; Qin, Y.J.; Yang, Y.F.; Xu, J.G.; Bin Yu, M. Intraocular Pressure-Lowering Potential of Subthreshold Selective Laser Trabeculoplasty in Patients with Primary Open-Angle Glaucoma. J. Ophthalmol. 2016, 2016, 2153723. [Google Scholar] [CrossRef]
- Kennedy, J.B.; SooHoo, J.R.; Kahook, M.Y.; Seibold, L.K. Selective Laser Trabeculoplasty: An Update. Asia Pac. J. Ophthalmol. 2016, 5, 63–69. [Google Scholar] [CrossRef]
- Abouhussein, M.A. Micropulse laser trabeculoplasty for open-angle glaucoma. Delta J. Ophthalmol. 2016, 17, 80–84. [Google Scholar] [CrossRef]
- Ingvoldstad, D.D.; Krishna, R.; Willoughby, L. MicroPulse Diode Laser Trabeculoplasty versus Argon Laser Trabeculoplasty in the Treatment of Open Angle Glaucoma. Investig. Ophthalmol. Vis. Sci. 2005, 46, 123. [Google Scholar]
- Tsang, S.; Cheng, J.; Lee, J.W. Developments in laser trabeculoplasty. Br. J. Ophthalmol. 2016, 100, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Ma, A.; Yu, S.W.Y.; Wong, J.K.W. Micropulse laser for the treatment of glaucoma: A literature review. Surv. Ophthalmol. 2019, 64, 486–497. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.Q.; Chen, T.A.; Deiner, M.S.; Ou, Y. Clinical Outcomes of Micropulse Laser Trabeculoplasty Compared to Selective Laser Trabeculoplasty at One Year in Open-Angle Glaucoma. Clin. Ophthalmol. 2021, 15, 243–251. [Google Scholar] [CrossRef]
- Abramowitz, B.; Chadha, N.; Kouchouk, A.; Alhabshan, R.; Belyea, D.A.; Lamba, T. Selective laser trabeculoplasty vs. micropulse laser trabeculoplasty in open-angle glaucoma. Clin. Ophthalmol. 2018, 12, 1599–1604. [Google Scholar] [CrossRef]
- Fudemberg, S.J.; Myers, J.S.; Katz, L.J. Trabecular meshwork tissue examination with scanning electron microscopy: A comparison of micropulse diode laser (MLT), selective laser (SLT), and argon laser (ALT) trabeculoplasty in human cadaver tissue. Investig. Ophthalmol. Vis. Sci. 2008, 49, 1236. [Google Scholar]
- Detry-Morel, M.; Muschart, F.; Pourjavan, S. Micropulse diode laser (810 nm) versus argon laser trabeculoplasty in the treatment of open-angle glaucoma: Comparative short-term safety and efficacy profile. Bull Soc. Belge. Ophtalmol. 2008, 308, 21–28. [Google Scholar]
- Valera-Cornejo, D.A.; Loayza-Gamboa, W.; Herrera-Quiroz, J.; Alvarado-Vlllacorta, R.; Cordova-Crisanto, L.; Valderrama-Albino, V.; Davalos, N.P. Micropulse Trabeculoplasty in Open Angle Glaucoma. Adv. Biomed. Res. 2018, 7, 156. [Google Scholar] [CrossRef]
- Tai, T.Y.T. Micropulse Laser Trabeculoplasty after Previous Laser Trabeculoplasty. Arch. Ophthalmol. 2011, 129, 1011–1017. [Google Scholar]
- Babalola, O.E. Micropulse diode laser trabeculoplasty in Nigerian patients. Clin. Ophthalmol. 2015, 9, 1347–1351. [Google Scholar] [CrossRef]
- Fea, A.M.; Bosone, A.; Rolle, T.; Brogliatti, B.; Grignolo, F.M. Micropulse diode laser trabeculoplasty (MDLT): A phase II clinical study with 12 months follow-up. Clin. Ophthalmol. 2008, 2, 247–252. [Google Scholar] [CrossRef]
- Kakihara, S.; Hirano, T.; Imai, A.; Kurenuma, T.; Chiku, Y.; Murata, T. Micropulse laser trabeculoplasty under maximal tolerable glaucoma eyedrops: Treatment effectiveness and impact of surgical expertise. Int. J. Ophthalmol. 2021, 14, 388–392. [Google Scholar] [CrossRef]
- Rantala, E.; Valimaki, J. Micropulse diode laser trabeculoplasty—180-degree treatment. Acta Ophthalmol. 2012, 90, 441–444. [Google Scholar] [CrossRef]
- Gambini, G.; Carlà, M.M.; Caporossi, T.; De Vico, U.; Savastano, A.; Baldascino, A.; Rizzo, C.; Kilian, R.; Rizzo, S. Spotlight on MicroPulse Laser Trabeculoplasty in Open-Angle Glaucoma: What’s on? A Review of the Literature. Vision 2022, 6, 8. [Google Scholar] [CrossRef]
- De Leon, M.I.; Santana, J.F.O.; Lopex, A.G. Selective Laser Trabeculoplasty vs. Micropulse Laser Trabeculoplasty for the Treatment of Open Angle Glaucoma and Ocular Hypertension. Int. J. Res. Med. Health Sci. 2017, 14, 1. [Google Scholar]
- Makri, O.E.; Plotas, P.; Christopoulou, E.; Georgakopoulos, C. Effect of a single session of micropulse laser trabeculoplasty on corneal endothelial parameters. Clin. Exp. Optom. 2020, 103, 479–483. [Google Scholar] [CrossRef]
- Lee, J.W.Y.; Yau, G.S.K.; Yick, D.W.F.; Yuen, C.Y.F. MicroPulse Laser Trabeculoplasty for the Treatment of Open-Angle Glaucoma. Medicine 2015, 94, e2075. [Google Scholar] [CrossRef]
- Gossage, D. Two-year data on MicroPulse laser trabeculoplasty. Eye World 2015, 4, 58. [Google Scholar]
- Makri, O.E.; Pagoulatos, D.; Kagkelaris, K.; Plotas, P.; Georgakopoulos, C. Evaluation of intraocular pressure in the first 24 hours after micropulse laser trabeculoplasty in eyes with pseudoexfoliation glaucoma. J. Fr. Ophtalmol. 2019, 42, 983–986. [Google Scholar] [CrossRef]
- Hirabayashi, M.T.; Rosenlof, T.L.; An, J.A. Comparison of successful outcome predictors for MicroPulse® laser trabeculoplasty and selective laser trabeculoplasty at 6 months. Clin. Ophthalmol. 2019, 13, 1001. [Google Scholar] [CrossRef]
- Hoskins, H.D., Jr.; Hetherington, J., Jr.; Minckler, D.S.; Lieberman, M.F.; Shaffer, R.N. Complications of laser trabeculoplasty. Ophthalmology 1983, 90, 796–799. [Google Scholar] [CrossRef] [PubMed]
- Traverso, C.; Cohen, E.J.; Groden, L.R.; Cassel, G.H.; Laibson, P.R.; Spaeth, G.L. Central corneal endothelial cell density after argon laser trabeculoplasty. Arch. Ophthalmol. 1984, 102, 1322–1324. [Google Scholar] [CrossRef] [PubMed]
- Bettis, D.I.; Whitehead, J.J.; Farhi, P.; Zabriskie, N.A. Intraocular pressure spike and corneal decompensation following selective laser trabeculoplasty in patients with exfoliation glaucoma. J. Glaucoma 2016, 25, e433–e437. [Google Scholar] [CrossRef] [PubMed]
- Regin39, M.; Bunya, V.Y.; Orlin, S.E.; Ansari, H. Corneal edema and haze after selective laser trabeculoplasty. J. Glaucoma 2011, 20, 327–329. [Google Scholar] [CrossRef]
- Knickelbein, J.E.; Singh, A.; Flowers, B.E.; Nair, U.K.; Eisenberg, M.; Davis, R.; Raju, L.V.; Schuman, J.S.; Conner, I.P. Acute corneal edema with subsequent thinning and hyperopic shift following selective laser trabeculoplasty. J. Cataract. Refract. Surg. 2014, 40, 1731–17354. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| MLT 1500 | MLT 1000 | p-Value | |
|---|---|---|---|
| Eyes, n | 9 | 9 | |
| BCVA, letters (±SD) | 42.9 (±17.2) | 49.3 (±5.1) | 0.297 |
| ECC, cell/mm2(±SD) | 2271 (±461) | 2143.6 (±445.2) | 0.559 |
| CCT, μm (±SD) | 525.7 (±24.2) | 533.3 (±31.4) | 0.575 |
| IOP, mmHg (±SD) | 15.7 (±4.8) | 14.9 (±3.4) | 0.724 |
| N. of glaucoma topical medications | 2.5 (±1.1) | 2.4 (±1.0) | 0.829 |
| MLT 1500 | MLT 1000 | p-Value | ||
|---|---|---|---|---|
| ECC, cell/mm2 (±SD) | T0 | 2271 ± 461 | 2143 ± 445 | 0.559 |
| T1 | 2218 ± 474 | 2121 ± 446 | 0.660 | |
| T4 | 2157 ± 463 | 2003 ± 470 | 0.494 | |
| T5 | 2179 ± 424 | 2071 ± 506 | 0.460 | |
| CCT, μm (±SD) | T0 | 525 ± 24 | 533 ± 31 | 0.575 |
| T1 | 531 ± 28 | 538 ± 29 | 0.601 | |
| T4 | 529 ± 27 | 536 ± 32 | 0.488 | |
| T5 | 528 ± 28 | 539 ± 31 | 0.087 | |
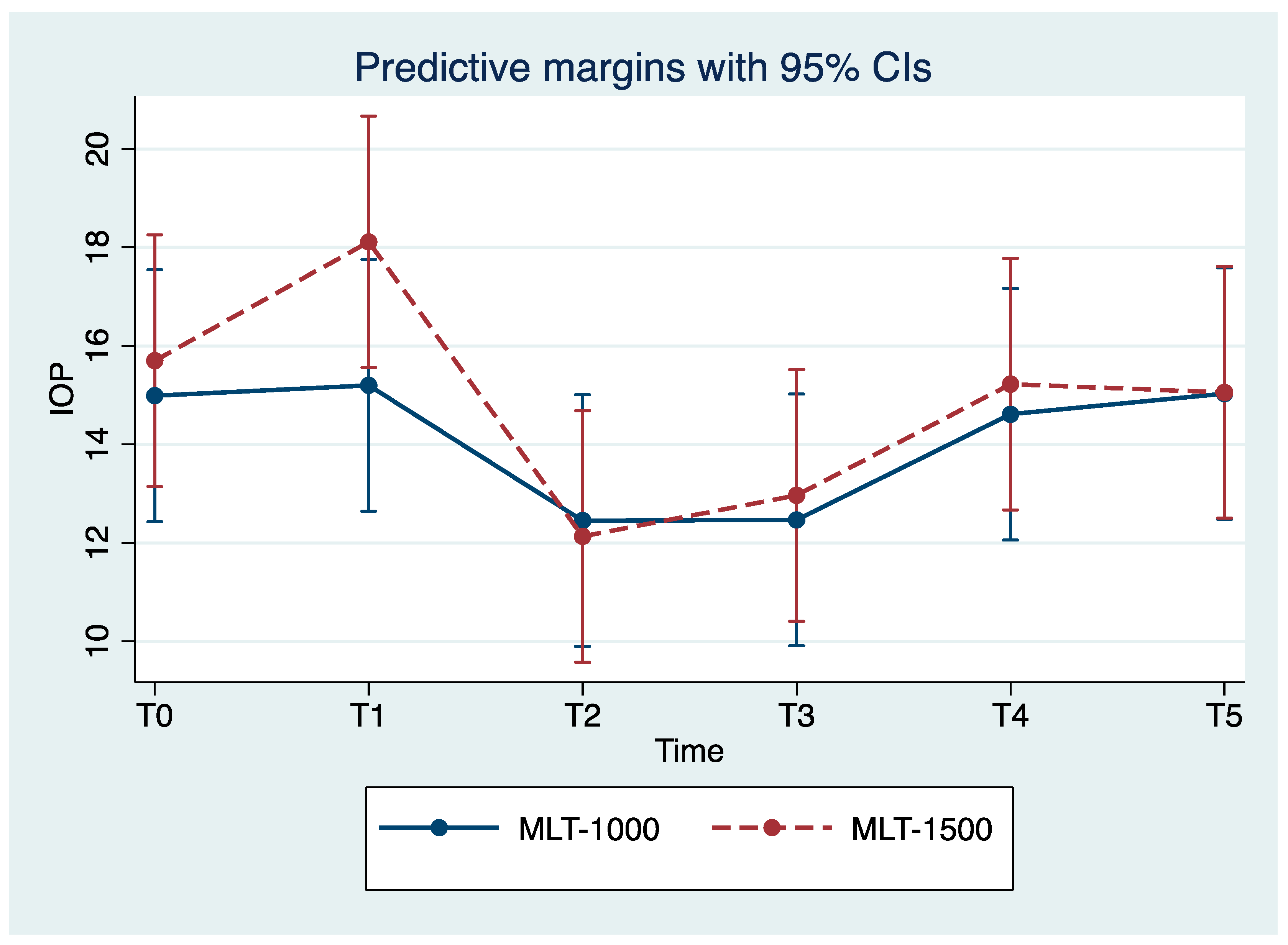
| IOP, (mm Hg) | T0 | 15.7 ± 4.8 | 14.9 ± 3.4 | 0.724 |
| T1 | 18.1 ± 7 | 15.2 ± 3.5 | 0.282 | |
| T2 | 12.1 ± 3.8 | 12.4 ± 2.6 | 0.837 | |
| T3 | 12.9 ± 2.9 | 12.4 ± 2.9 | 0.725 | |
| T4 | 15.2 ± 3.3 | 14.6 ± 3.6 | 0.691 | |
| T5 | 15.0 ± 2.9 | 15.0 ± 3.1 | 0.987 | |
| BCVA, (ETDRS chart letters) | T0 | 42.9 ± 17.2 | 49.3 ± 5.1 | 0.297 |
| T5 | 42.1 ± 16.9 | 49.6 ± 4.9 | 0.132 | |
| Medications, n (±SD) | T0 | 2.5 ± 1.1 | 2.4 ± 1.0 | 0.829 |
| T3/T5 | 2.0 ± 1.2 | 1.9 ± 1.0 | 0.839 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verdina, T.; Gironi, M.; Battaglia, B.; Gentile, M.; Chester, J.; Kaleci, S.; Scatigna, G.; Mastropasqua, R.; Cavallini, G.M. Micropulse Laser Trabeculoplasty with 577 nm Wavelength at 1500 or 1000 mW for Primary Open-Angle Glaucoma: A Pilot Study. Life 2023, 13, 982. https://doi.org/10.3390/life13040982
Verdina T, Gironi M, Battaglia B, Gentile M, Chester J, Kaleci S, Scatigna G, Mastropasqua R, Cavallini GM. Micropulse Laser Trabeculoplasty with 577 nm Wavelength at 1500 or 1000 mW for Primary Open-Angle Glaucoma: A Pilot Study. Life. 2023; 13(4):982. https://doi.org/10.3390/life13040982
Chicago/Turabian StyleVerdina, Tommaso, Matteo Gironi, Bruno Battaglia, Michele Gentile, Johanna Chester, Shaniko Kaleci, Gianluca Scatigna, Rodolfo Mastropasqua, and Gian Maria Cavallini. 2023. "Micropulse Laser Trabeculoplasty with 577 nm Wavelength at 1500 or 1000 mW for Primary Open-Angle Glaucoma: A Pilot Study" Life 13, no. 4: 982. https://doi.org/10.3390/life13040982
APA StyleVerdina, T., Gironi, M., Battaglia, B., Gentile, M., Chester, J., Kaleci, S., Scatigna, G., Mastropasqua, R., & Cavallini, G. M. (2023). Micropulse Laser Trabeculoplasty with 577 nm Wavelength at 1500 or 1000 mW for Primary Open-Angle Glaucoma: A Pilot Study. Life, 13(4), 982. https://doi.org/10.3390/life13040982