
Transcutaneous Neuromodulation for Constipation and Fecal Incontinence in Children: A Systematic Review and Meta-Analysis
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Patients and Methods
2.1. Eligibility Criteria
2.2. Data Sources and Searches
2.3. Study Selection and Data Extraction
2.4. Statistical Analysis and Risk of Bias
2.5. Quality of Evidence and Level of Recommendation
2.6. Declaration and Registration
3. Results
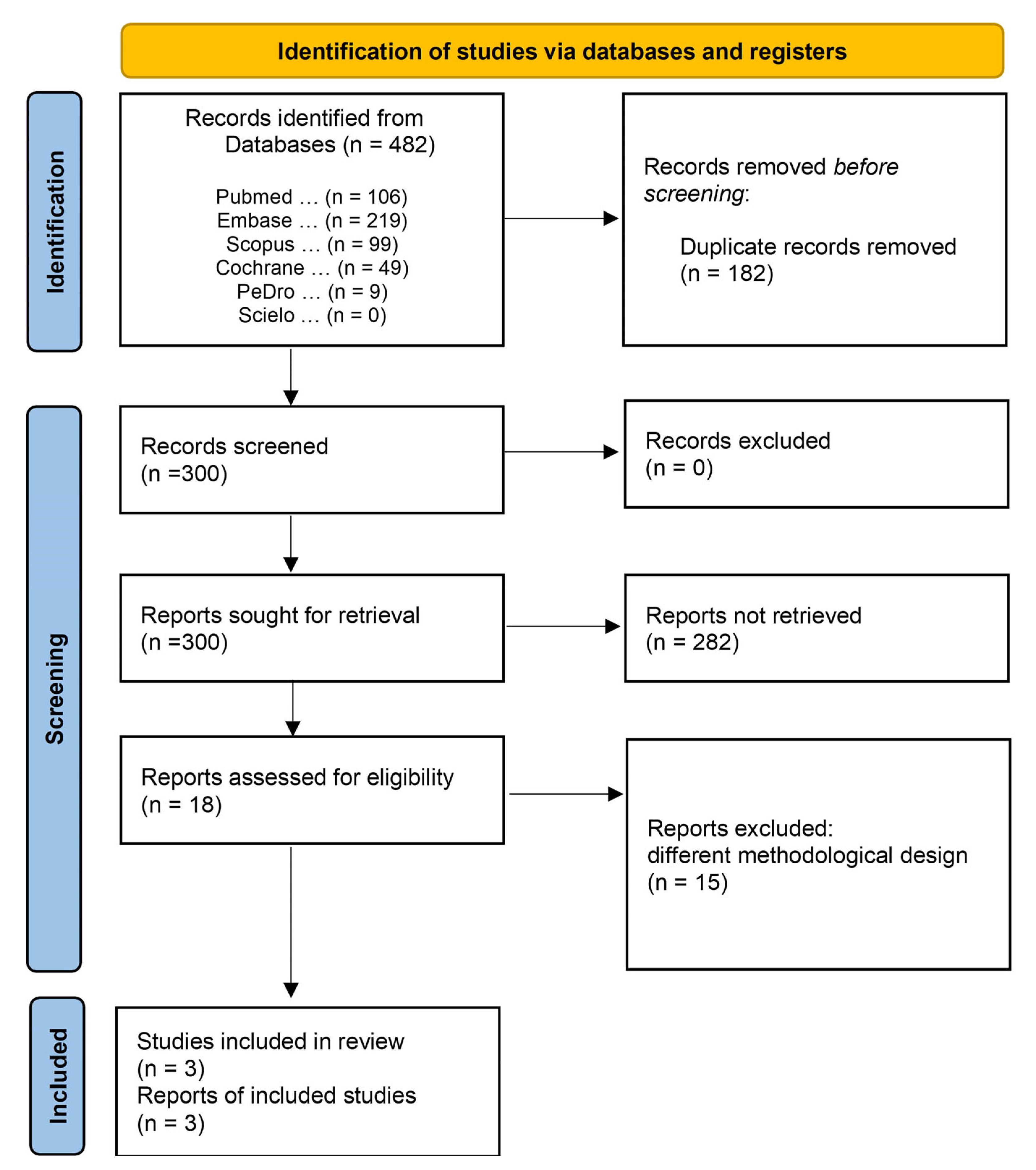
3.1. Study Selection
3.2. Characteristics of the Included Studies
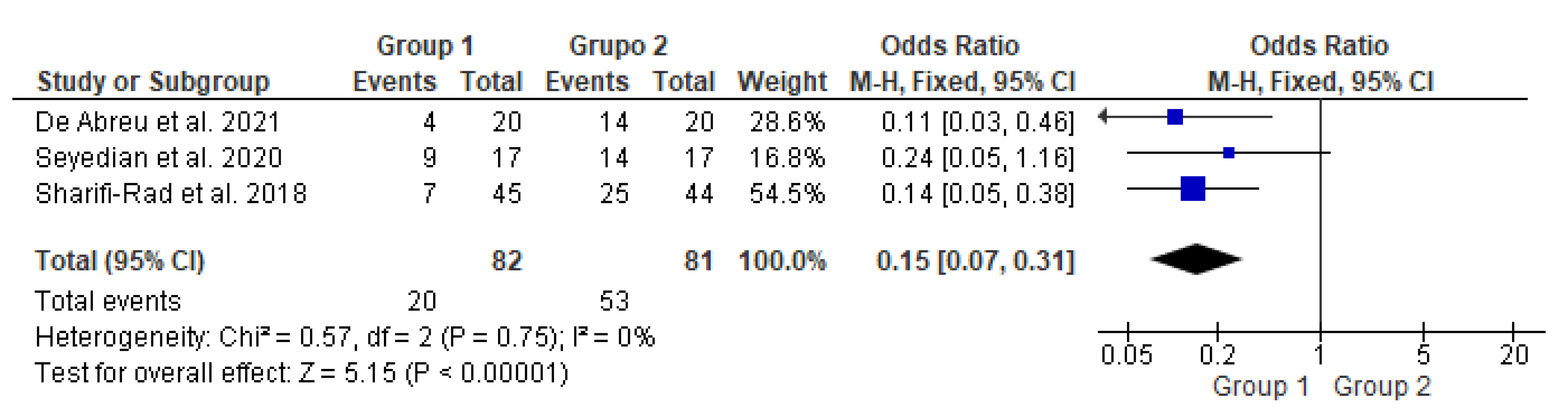
3.3. Meta-Analysis on Constipation Improvement
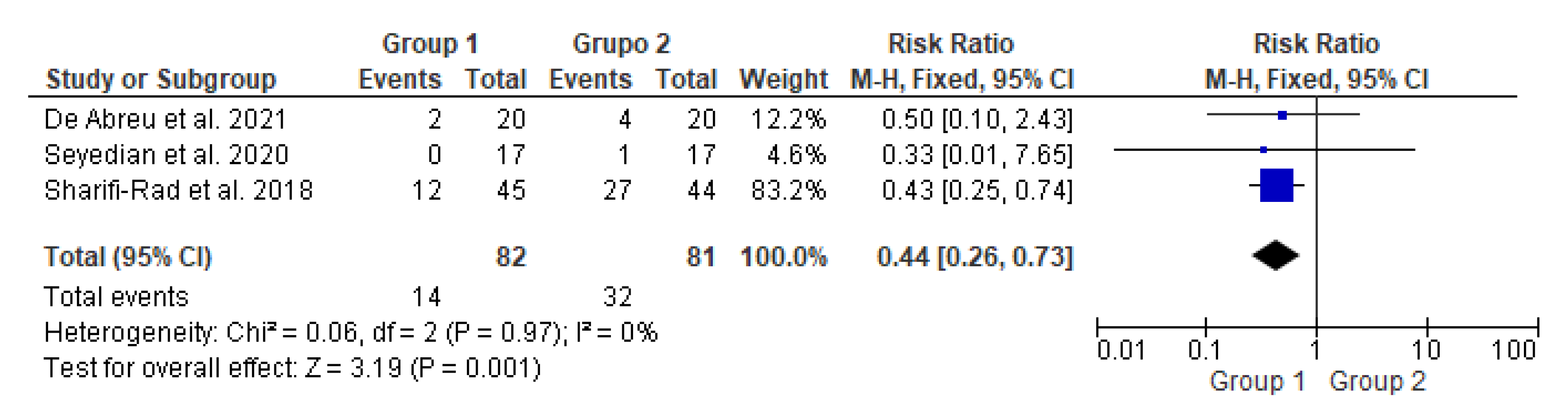
3.4. Meta-Analysis on Fecal Incontinence Improvement
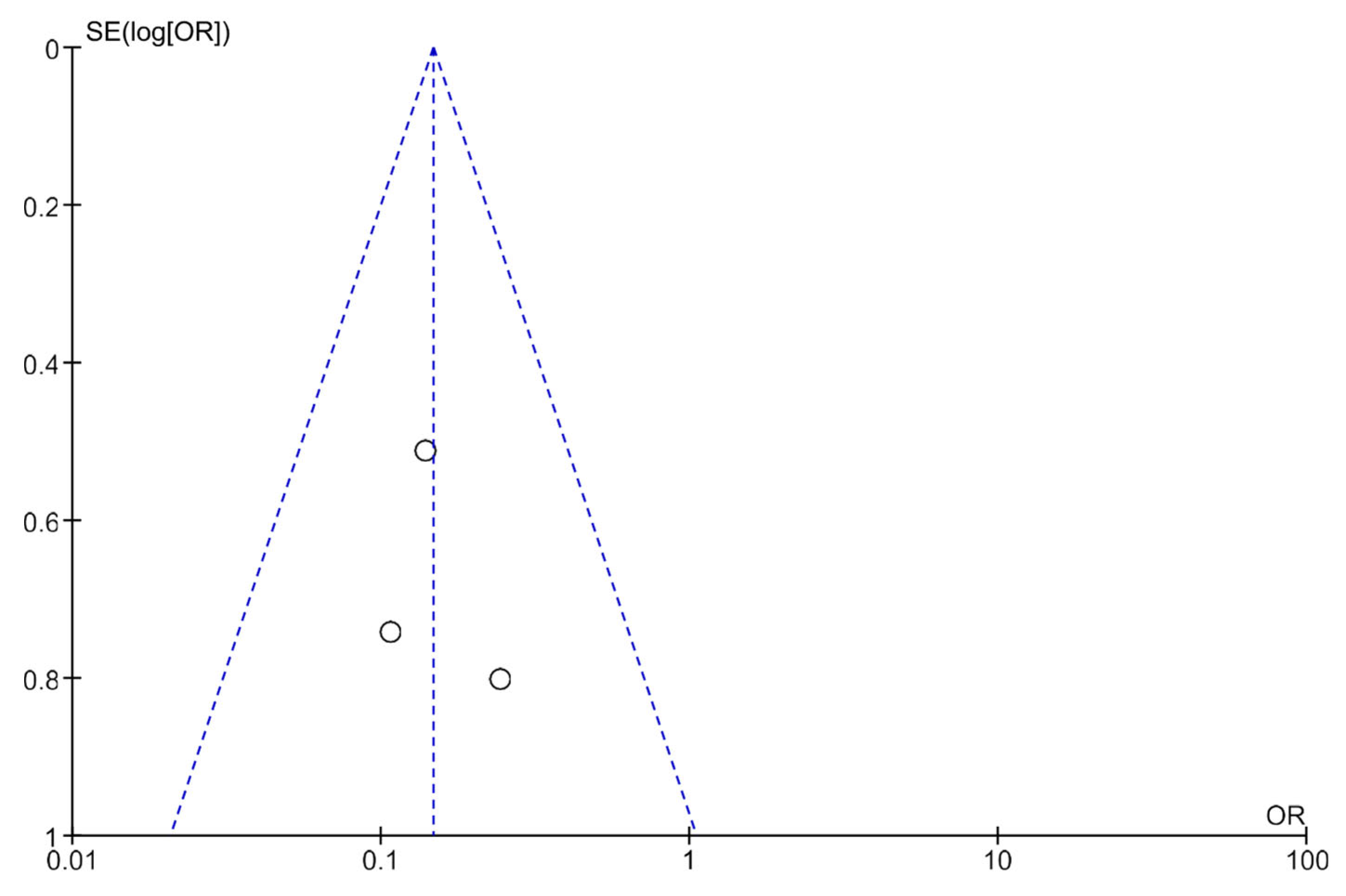
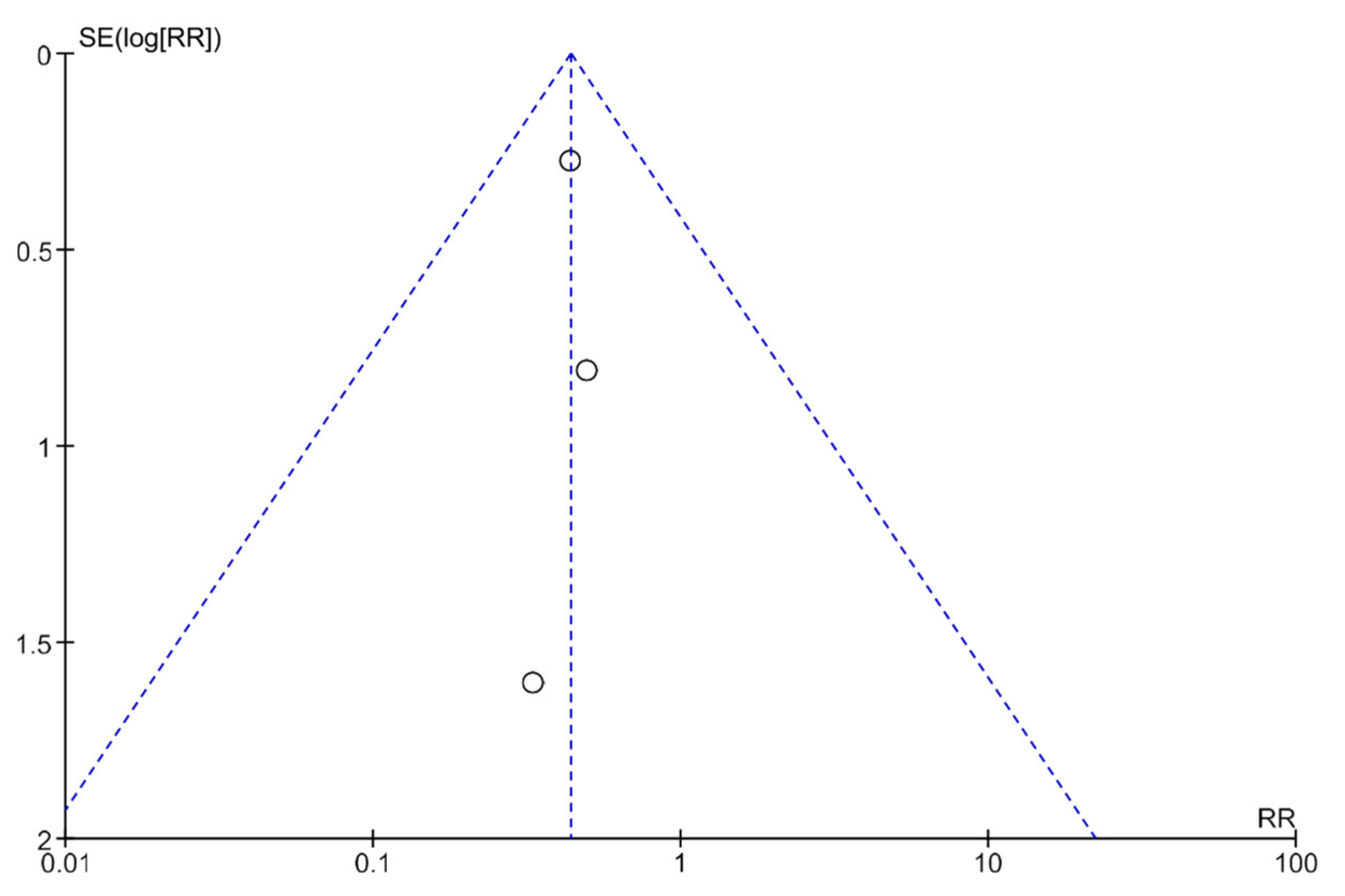
3.5. Publication Bias Analysis Using Funnel Plots
3.6. Risk of Bias and Methodological Quality Analysis
3.7. Quality of Evidence and Level of Recommendation
4. Discussion
5. Conclusions
Implications for Clinical Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mousa, H.M.; Barsamian, J.M.; Benitez, A.J.; Webster, J.M.; Fiorino, K.N. Pediatric Constipation: An Epidemiologic and Physiologic Approach to Guide a Stepwise Approach to its Management. Curr. Treat. Options Pediatr. 2020, 6, 155–169. [Google Scholar] [CrossRef]
- Tabbers, M.; DiLorenzo, C.; Berger, M.; Faure, C.; Langendam, M.; Nurko, S.; Staiano, A.; Vandenplas, Y.; Benninga, M.; European Society for Pediatric Gastroenterology; et al. Evaluation and treatment of functional constipation in infants and children: Evidence-based recommendations from ESPGHAN and NASPGHAN. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 258–274. [Google Scholar] [CrossRef] [PubMed]
- Vriesman, M.H.; Koppen, I.J.N.; Camilleri, M.; Di Lorenzo, C.; Benninga, M.A. Management of functional constipation in children and adults. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 21–39. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.L.; Di Lorenzo, C. Neurostimulation of the gastrointestinal tract in children: Is it time to shock the gut? Curr. Opin. Pediatr. 2016, 28, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.T.; Lee, W.S.; Ang, H.L.; Teo, K.M.; Yik, Y.I.; Lai, N.M. Transcutaneous electrical stimulation (TES) for treatment of constipation in children. Cochrane Database Syst. Rev. 2016, 2016, CD010873. [Google Scholar] [CrossRef]
- Iacona, R.; Ramage, L.; Malakounides, G. Current State of Neuromodulation for Constipation and Fecal Incontinence in Children: A Systematic Review. Eur. J. Pediatr. Surg. 2019, 29, 495–503. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.; Chandler, J.; Welch, V.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Rasquin, A.; Di Lorenzo, C.; Forbes, D.; Guiraldes, E.; Hyams, J.S.; Staiano, A.; Walker, L.S. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2006, 130, 1527–1537. [Google Scholar] [CrossRef]
- Benninga, M.A.; Nurko, S.; Faure, C.; Hyman, P.E.; Roberts, I.S.J.; Schechter, N.L. Childhood Functional Gastrointestinal Disorders: Neonate/Toddler. Gastroenterology 2016, 150, 1443–1455.e2. [Google Scholar] [CrossRef] [PubMed]
- Játiva-Mariño, E.; Rivera-Valenzuela, M.G.; Velasco-Benitez, C.A.; Saps, M. The prevalence of functional constipation in children was unchanged after the Rome IV criteria halved the diagnosis period in Rome III. Acta Paediatr. 2019, 108, 2274–2277. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Brozek, J.L.; Canelo-Aybar, C.; Akl, E.A.; Bowen, J.M.; Bucher, J.; Chiu, W.A.; Cronin, M.; Djulbegovic, B.; Falavigna, M.; Guyatt, G.H.; et al. GRADE Guidelines 30: The GRADE approach to assessing the certainty of modeled evidence—An overview in the context of health decision-making. J. Clin. Epidemiol. 2021, 129, 138–150. [Google Scholar] [CrossRef] [PubMed]
- de Abreu, G.E.; de Souza, L.A.; da Fonseca, M.L.V.; Barbosa, T.B.C.; de Mello, E.R.D.; Nunes, A.N.B.; Barroso, U.D.O., Jr. Parasacral Transcutaneous Electrical Nerve Stimulation for the Treatment of Children and Adolescents with Bladder and Bowel Dysfunction: A Randomized Clinical Trial. J. Urol. 2021, 205, 1785–1791. [Google Scholar] [CrossRef] [PubMed]
- Ladi-Seyedian, S.-S.; Sharifi-Rad, L.; Kajbafzadeh, A.-M. Management of Bladder Bowel Dysfunction in Children by Pelvic Floor Interferential Electrical Stimulation and Muscle Exercises: A Randomized Clinical Trial. Urology 2020, 144, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Rad, L.; Seyedian, S.L.; Manouchehri, N.; Alimadadi, H.; Allahverdi, B.; Motamed, F.; Fallahi, G.-H. Effects of Interferential Electrical Stimulation Plus Pelvic Floor Muscles Exercises on Functional Constipation in Children: A Randomized Clinical Trial. Am. J. Gastroenterol. 2018, 113, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Kumsar, Ş.; Keskin, U.; Akay, A.; Bilgilisoy, U.T.; Erdem, R.; Peşkircioğlu, L.; Özkardeş, H. Effects of Sacral Neuromodulation on Isolated Urinary Bladder Function in a Rat Model of Spinal Cord Injury. Neuromodulation 2015, 18, 67–74; discussion 74–75. [Google Scholar] [CrossRef]
- Lundby, L.; Møller, A.; Buntzen, S.; Krogh, K.; Vang, K.; Gjedde, A.; Laurberg, S. Relief of Fecal Incontinence by Sacral Nerve Stimulation Linked to Focal Brain Activation. Dis. Colon Rectum 2011, 54, 318–323. [Google Scholar] [CrossRef]
- Michelsen, H.B.; Buntzen, S.; Krogh, K.; Laurberg, S. Rectal Volume Tolerability and Anal Pressures in Patients with Fecal Incontinence Treated with Sacral Nerve Stimulation. Dis. Colon Rectum 2006, 49, 1039–1044. [Google Scholar] [CrossRef]
- Kenefick, N.J.; Emmanuel, A.; Nicholls, R.J.; Kamm, M.A. Effect of sacral nerve stimulation on autonomic nerve function. Br. J. Surg. 2003, 90, 1256–1260. [Google Scholar] [CrossRef]
- Dos Santos, J.; Lopes, R.I.; Koyle, M.A. Bladder and bowel dysfunction in children: An update on the diagnosis and treatment of a common, but underdiagnosed pediatric problem. Can. Urol. Assoc. J. 2017, 11, S64–S72. [Google Scholar] [CrossRef] [PubMed]
- Halachmi, S.; Farhat, W.A. Interactions of Constipation, Dysfunctional Elimination Syndrome, and Vesicoureteral Reflux. Adv. Urol. 2008, 2008, 828275. [Google Scholar] [CrossRef] [PubMed]
- Kegel, A.H. Physiologic therapy for urinary stress incontinence. J. Am. Med. Assoc. 1951, 146, 915–917. [Google Scholar] [CrossRef] [PubMed]
- van Engelenburg-van Lonkhuyzen, M.L.; Bols, E.M.; Benninga, M.A.; Verwijs, W.A.; de Bie, R.A. Effectiveness of Pelvic Physiotherapy in Children with Functional Constipation Compared with Standard Medical Care. Gastroenterology 2017, 152, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Joensson, I.M.; Hagstroem, S.; Siggaard, C.; Bower, W.; Djurhuus, J.C.; Krogh, K. Transcutaneous Electrical Nerve Stimulation Increases Rectal Activity in Children. J. Craniofacial Surg. 2015, 61, 80–84. [Google Scholar] [CrossRef]
- Chase, J.; Robertson, V.J.; Southwell, B.; Hutson, J.; Gibb, S. Pilot study using transcutaneous electrical stimulation (interferential current) to treat chronic treatment-resistant constipation and soiling in children. J. Gastroenterol. Hepatol. 2005, 20, 1054–1061. [Google Scholar] [CrossRef]
- Ismail, K.A.; Chase, J.; Gibb, S.; Clarke, M.; Catto-Smith, A.G.; Robertson, V.J.; Hutson, J.M.; Southwell, B.R. Daily transabdominal electrical stimulation at home increased defecation in children with slow-transit constipation: A pilot study. J. Pediatr. Surg. 2009, 44, 2388–2392. [Google Scholar] [CrossRef]
- Clarke, M.C.C.; Catto-Smith, A.G.; King, S.K.; Dinning, P.G.; Cook, I.J.; Chase, J.W.; Gibb, S.M.; Robertson, V.J.; Simpson, D.; Hutson, J.M.; et al. Transabdominal electrical stimulation increases colonic propagating pressure waves in paediatric slow transit constipation. J. Pediatr. Surg. 2012, 47, 2279–2284. [Google Scholar] [CrossRef]
- Dwyer, M.E.; Vandersteen, D.R.; Hollatz, P.; Reinberg, Y.E. Sacral Neuromodulation for the Dysfunctional Elimination Syndrome: A 10-Year Single-center Experience With 105 Consecutive Children. Urology 2014, 84, 911–918. [Google Scholar] [CrossRef]
- Thomas, G.P.; Dudding, T.C.; Rahbour, G.; Nicholls, R.J.; Vaizey, C.J. Sacral nerve stimulation for constipation. Br. J. Surg. 2012, 100, 174–181. [Google Scholar] [CrossRef]
- Yik, Y.I.; Ismail, K.A.; Hutson, J.M.; Southwell, B.R. Home transcutaneous electrical stimulation to treat children with slow-transit constipation. J. Pediatr. Surg. 2012, 47, 1285–1290. [Google Scholar] [CrossRef]
- Yik, Y.I.; Leong, L.; Hutson, J.M.; Southwell, B.R. The impact of transcutaneous electrical stimulation therapy on appendicostomy operation rates for children with chronic constipation—A single-institution experience. J. Pediatr. Surg. 2012, 47, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Yik, Y.I.; Ismail, K.A.; Hutson, J.M.; Southwell, B.R. Tu1366 Daily Transabdominal Electrical Stimulation Reduces Soiling in Children With Slow-Transit Constipation. Gastroenterology 2012, 142, S-812–S-813. [Google Scholar] [CrossRef]
- Yik, Y.I.; Ismail, K.; Hutson, J.; Southwell, B. Home-based transabdominal electrical stimulation slowly improves treatment-resistant chronic constipation in children. Neuromodulation 2013, 16, e102. [Google Scholar]
- Yik, Y.I.; Ismail, K.A.; Hutson, J.M.; Southwell, B.R. Transabdominal electrical stimulation using interferential current is able to treat chronic constipation in children. Neuromodulation 2013, 16, e13. [Google Scholar]
- Southwell, B. Transabdominal electrical stimulation to treat slow transit constipation in children. Neuromodulation 2012, 15, 63. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia, R.R.; Gameiro, L.F.O.; Trevisane, N.G.; Bertanha, M.; Ortolan, E.V.P.; Lourenção, P.L.T.d.A. Transcutaneous Neuromodulation for Constipation and Fecal Incontinence in Children: A Systematic Review and Meta-Analysis. Life 2023, 13, 430. https://doi.org/10.3390/life13020430
Correia RR, Gameiro LFO, Trevisane NG, Bertanha M, Ortolan EVP, Lourenção PLTdA. Transcutaneous Neuromodulation for Constipation and Fecal Incontinence in Children: A Systematic Review and Meta-Analysis. Life. 2023; 13(2):430. https://doi.org/10.3390/life13020430
Chicago/Turabian StyleCorreia, Ronny Rodrigues, Luis Felipe Orsi Gameiro, Nathalia Grion Trevisane, Matheus Bertanha, Erika Veruska Paiva Ortolan, and Pedro Luiz Toledo de Arruda Lourenção. 2023. "Transcutaneous Neuromodulation for Constipation and Fecal Incontinence in Children: A Systematic Review and Meta-Analysis" Life 13, no. 2: 430. https://doi.org/10.3390/life13020430
APA StyleCorreia, R. R., Gameiro, L. F. O., Trevisane, N. G., Bertanha, M., Ortolan, E. V. P., & Lourenção, P. L. T. d. A. (2023). Transcutaneous Neuromodulation for Constipation and Fecal Incontinence in Children: A Systematic Review and Meta-Analysis. Life, 13(2), 430. https://doi.org/10.3390/life13020430