


Association of Circulating Neutrophils with Relative Volume of Lipid-Rich Necrotic Core of Coronary Plaques in Stable Patients: A Substudy of SMARTool European Project

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. CTCA and Quantitative Image Analysis
2.3. Biochemical and Hematological Analyses
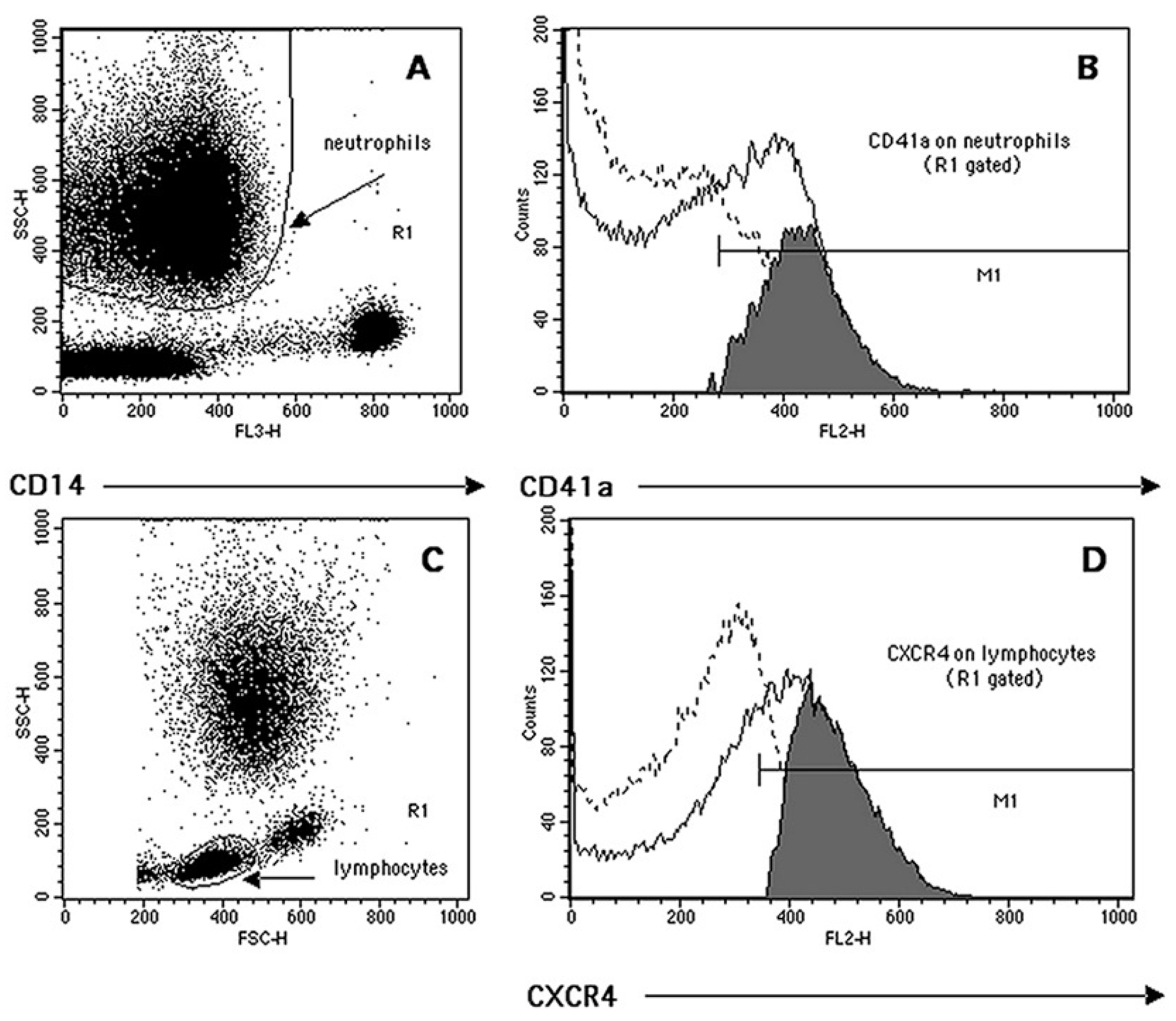
2.4. Flow Cytometry Analysis
2.5. Statistical Analysis
3. Results
3.1. Patients Clinical Characteristics and Plasma Biochemistry
3.2. Relationships between Leukocyte Subsets Count, Leukocyte Subsets Count Ratios, Neutrophil/PLT Ratio and LRNCV Values
3.3. Relationships between Leukocyte Phenotypic Features and LRNCV Values
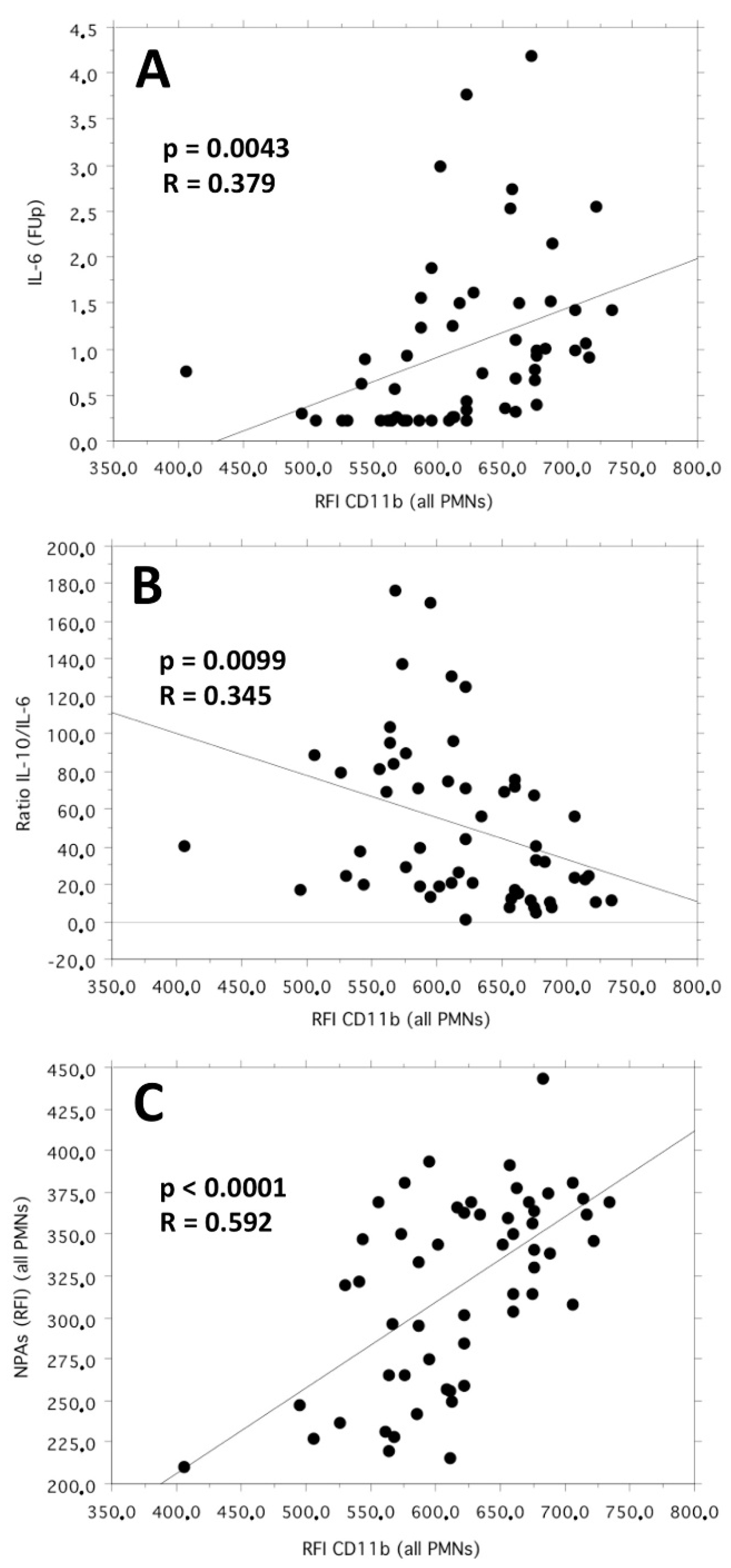
3.4. Relationships between Leukocyte-Platelet Adhesion Index and LRNCV Values
3.5. Relationships between Leukocyte Receptor Ratios and LRNCV Values
4. Discussions
4.1. Study Results
4.2. Comparison with Similar Studies
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sbrana, S.; Campolo, J.; Clemente, A.; Bastiani, L.; Cecchettini, A.; Ceccherini, E.; Caselli, C.; Neglia, D.; Parodi, O.; Chiappino, D.; et al. Blood monocyte phenotype fingerprint of stable coronary artery disease: A cross-sectional substudy of SMARTool clinical Trial. BioMed Res. Int. 2020, 2020, 8748934. [Google Scholar] [CrossRef] [PubMed]
- Sbrana, S.; Cecchettini, A.; Bastiani, L.; Di Giorgi, N.; Mazzone, A.; Ceccherini, E.; Vozzi, F.; Caselli, C.; Neglia, D.; Clemente, A.; et al. Bood M2-like monocyte polarization is associated with calcific plaque phenotype in stable coronary artery disease: A sub-study of SMARTool clinical trial. Biomedicines 2022, 10, 565. [Google Scholar] [CrossRef] [PubMed]
- Silvestre-Roig, C.; Braster, Q.; Ortega-Gomez, A.; Soehnlein, O. Neutrophils as regulators of cardiovascular inflammation. Nat. Rev. Cardiol. 2020, 17, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Soehnlein, O. Multiple roles for neutrophils in atherosclerosis. Circ. Res. 2012, 110, 875–888. [Google Scholar] [CrossRef]
- Baetta, R.; Corsini, A. Role of polymorphonuclear neutrophils in atherosclerosis: Current state and future perspectives. Atherosclerosis 2010, 210, 1–13. [Google Scholar] [CrossRef]
- Carbone, F.; Mach, F.; Montecucco, F. Update on the role of neutrophils in atherosclerotic plaque vulnerability. Curr. Drug Targets 2015, 16, 321–333. [Google Scholar] [CrossRef]
- Ionita, M.G.; van den Borne, P.; Catanzariti, L.M.; Moll, F.L.; de Vries, J.P.P.; Pasterkamp, G.; Vink, A.; de Kleijn, D.P.V. High neutrophil numbers in human carotid atherosclerotic plaques are associated with characteristics of rupture-prone lesions. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1842–1848. [Google Scholar] [CrossRef]
- Roth Flach, R.J.; Su, C.; Bollinger, E.; Cortes, C.; Robertson, A.W.; Opsahi, A.C.; Coskran, T.M.; Maresca, K.P.; Keliher, E.J.; Yates, P.D.; et al. Myeloperoxidase inhibition in mice alters atherosclerotic lesion composition. PLoS ONE 2019, 14, e0214150. [Google Scholar] [CrossRef]
- Balta, S.; Celik, T.; Mikhailidis, D.P.; Ozturk, C.; Demirkol, S.; Aparci, M.; Iyisoy, A. The relation between atherosclerosis and the neutrophil-lymphocyte ratio. Clin. Appl. Thromb. Hemost. 2016, 22, 405–411. [Google Scholar] [CrossRef]
- Choi, Y.H.; Hong, Y.J.; Ahn, Y.; Park, I.H.; Jeong, M.H. Relationship between neutrophil-to lymphocyte ratio and plaque components in patients with coronary artery disease: Virtual histology intravascular ultrasound analysis. J. Korean Med. Sci. 2014, 29, 950–956. [Google Scholar] [CrossRef]
- Smit, J.M.; van Rosendael, A.R.; El Mahdiui, M.; Neglia, D.; Knuuti, J.; Saraste, A.; Buechel, R.R.; Teresinska, A.; Pizzi, M.N.; Roque, A.; et al. Impact of clinical characteristics and statins on coronary plaque progression by serial computed tomography angiography. Circ. Cardiovasc. Imaging 2020, 13, e009750. [Google Scholar] [CrossRef]
- Van Rosendael, A.R.; Shaw, L.J.; Xie, J.X.; Dimitriu-Leen, A.C.; Smit, J.M.; Scholte, A.J.; van Werkhoven, J.M.; Callister, T.Q.; De Lago, A.; Berman, D.S.; et al. Superior risk stratification with coronary computed tomography angiography using a comprehensive atherosclerotic risk score. JACC Cardiovasc. Imaging 2019, 12, 1987–1997. [Google Scholar] [CrossRef]
- Greenland, P.; Blaha, M.J.; Budoff, M.J.; Erbel, R.; Watson, K.E. Coronary calcium score and cardiovascular risk. J. Am. Coll. Cardiol. 2018, 72, 434–447. [Google Scholar] [CrossRef]
- Sbrana, S.; Bevilacqua, S.; Buffa, M.; Spiller, D.; Parri, M.S.; Gianetti, J.; De Filippis, R.; Clerico, A. Post-reperfusion changes of monocyte function in coronary blood after extracorporeal circulation. Cytom. Part B Clin. Cytom. 2005, 65, 14–21. [Google Scholar] [CrossRef]
- Mastej, K.; Adamiec, R. Neutrophil surface expression of CD11b and CD62L in diabetic microangiopathy. Acta Diabetol. 2008, 45, 183–190. [Google Scholar] [CrossRef]
- Siddiqi, M.; Garcia, Z.C.; Stein, D.S.; Denny, T.N.; Spolarics, Z. Relationship between oxidative burst activity and CD11b expression in neutrophils and monocytes from healthy individuals: Effects of race and gender. Cytom. Commun. Clin. Cytom. 2001, 46, 243–246. [Google Scholar] [CrossRef]
- Weyrich, A.S.; Zimmerman, G.A. Platelets: Signaling cells in the immune continuum. Trends Immunol. 2004, 25, 489–495. [Google Scholar] [CrossRef]
- Németh, T.; Mócsai, A. Feedback amplification of neutrophil function. Trends Immunol. 2016, 37, 412–424. [Google Scholar] [CrossRef]
- Särndahl, E.; Bergström, I.; Brodin, V.P.; Nijm, J.; Lundqvist Setterud, H.; Jonasson, L. Neutrophil activation status in stable coronary artery disease. PLoS ONE 2007, 2, e1056. [Google Scholar] [CrossRef]
- Gaul, D.S.; Stein, S.; Matter, C.M. Neutrophils in cardiovascular disease. Eur. Heart J. 2017, 38, 1702–1704. [Google Scholar] [CrossRef]
- Maréchal, P.; Tridetti, J.; Nguyen, M.L.; Wéra, O.; Jiang, Z.; Gustin, M.; Donneau, A.F.; Oury, C.; Lancellotti, P. Neutrophil phenotypes in coronary artery disease. J. Clin. Med. 2020, 9, 1602. [Google Scholar] [CrossRef] [PubMed]
- Caselli, C.; Di Giorgi, N.; Ragusa, R.; Lorenzoni, V.; Smit, J.; el Mahdiui, M.; Buechel, R.R.; Teresinska, A.; Pizzi, M.N.; Roque, A.; et al. Association of MMP9 with adverse features of plaque progression and residual inflammatory risk in patients with chronic coronary syndrome (CCS). Vascul. Pharmacol. 2022, 146, 107098. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, S.M.; Corriden, R.; Nizet, V. How neutrophils meet their end. Trends Immunol. 2020, 41, 531–544. [Google Scholar] [CrossRef] [PubMed]
- De Vries, J.J.; Autar, A.S.A.; van Dam-Nolen, D.H.K.; Donkel, S.J.; Kassem, M.; van der Kolk, A.G.; van Velzen, T.J.; Kooi, M.E.; Hendrikse, J.; Nederkoom, P.J.; et al. Association between plaque vulnerability and neutrophil extracellular traps (NETs) levels: The Plaque at Risk study. PLoS ONE 2022, 17, e0269805. [Google Scholar] [CrossRef]
- Singhal, A.; Kumar, S. Neutrophil and remnant clearance in immunity and inflammation. Immunology 2022, 165, 22–43. [Google Scholar] [CrossRef]
- Soehnlein, O. Neutrophil research, quo vadis? Trends Immunol. 2019, 40, 561–564. [Google Scholar] [CrossRef]
- Nijhuis, J.; Rensen, S.S.; Slaats, Y.; van Dielen, F.M.H.; Buurman, W.A.; Greve, J.W.M. Neutrophil activation in morbid obesity, chronic activation of acute inflammation. Obesity 2009, 17, 2014–2018. [Google Scholar] [CrossRef]
- Bai, M.; Grieshaber-Bouyer, R.; Wang, J.; Schmider, A.B.; Wilson, Z.S.; Zeng, L.; Halyabar, O.; Godin, M.D.; Nguyen, H.N.; Levescot, A.; et al. CD177 modulates human neutrophil migration through activation-mediated integrin and chemoreceptor regulation. Blood 2017, 130, 2092–2100. [Google Scholar] [CrossRef]
- Dhayni, K.; Zibara, K.; Issa, H.; Kamel, S.; Bennis, Y. Targeting CXCR1 and CXCR2 receptors in cardiovascular diseases. Pharmacol. Ther. 2022, 237, 108257. [Google Scholar] [CrossRef]
- Pircher, J.; Engelmann, B.; Massberg, S.; Schulz, C. Platelet-neutrophil crosstalk in atherothrombosis. Thromb. Haemost. 2019, 119, 1274–1282. [Google Scholar] [CrossRef]
- Frydman, G.H.; Le, A.; Ellett, F.; Jorgensen, J.; Fox, J.G.; Tompkins, R.G.; Irimia, D. Technical advance: Changes in neutrophil migration patterns upon contact with platelets in a microfluidic assay. J. Leucoc. Biol. 2017, 101, 797–806. [Google Scholar] [CrossRef]
- Kaiser, R.; Escaig, R.; Erber, J.; Nicolai, L. Neutrophil-platelet interactions as novel treatment targets in cardiovascular disease. Front. Cardiovasc. Med. 2022, 8, 824112. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Patients (n° = 55) | CAD1 (n° = 16) | CAD2 (n° = 21) | CAD3 (n° = 18) | ANOVA p Value | |
|---|---|---|---|---|---|
| Age (years) | 68.53 ± 1.07 | 65.18 ± 2.25 | 70.28 ± 1.72 | 69.50 ± 1.50 | Ns |
| Gender (M/F, n°) | 39/16 | 12/4 | 12/9 | 15/3 | Ns |
| Framingham Risk Score (a.u.) (FRS) | 15.40 ± 0.46 | 14.43 ± 1.09 | 16.09 ± 0.56 | 15.44 ± 0.75 | Ns |
| Diabetes, n° (%) | 17 (30.91) | 2 (3.64) | 6 (10.91) | 9 (16.37) | 0.059 * |
| Oral antidiabetics, n° (%) | 15 (27.28) | 2 (3.64) | 5 (9.09) | 8 (14.54) | Ns |
| Statin use, n° (%) | 41 (74.54) | 10 (18.19) | 14 (25.45) | 17 (30.91) | 0.059 * ^ |
| Statin dosage, (mg/die) | 13.27 ± 1.49 | 8.75 ± 2.01 | 13.09 ± 2.72 | 17.50 ± 2.43 | Ns |
| Creatinine (mg/dL) | 0.85 ± 0.03 | 0.89 ± 0.05 | 0.78 ± 0.04 | 0.90 ± 0.05 | Ns |
| Hs-CRP (mg/dL) | 0.44 ± 0.10 | 0.53 ± 0.18 | 0.33 ± 0.07 | 0.50 ± 0.24 | Ns |
| ICAM-1 (ng/mL) | 225.53 ± 13.62 | 241.77 ± 24.83 | 222.04 ± 21.22 | 215.15 ± 26.03 | Ns |
| VCAM-1 (ng/mL) | 635.15 ± 22.39 | 719.15 ± 59.19 | 547.93 ± 17.10 | 662.24 ± 27.97 | 0.004 § ^ |
| IL-6 (pg/mL) | 1.01 ± 0.13 | 1.30 ± 0.28 | 0.66 ± 0.10 | 1.16 ± 0.24 | Ns |
| IFN-γ (pg/mL) | 32.04 ± 1.69 | 34.10 ± 4.52 | 30.52 ± 1.97 | 31.97 ± 2.44 | Ns |
| IL-10 (pg/mL) | 27.26 ± 1.76 | 40.02 ± 2.91 | 23.70 ± 2.51 | 20.07 ± 1.51 | <0.0001 § * |
| TNF-α (pg/mL) | 69.74 ± 3.11 | 73.33 ± 8.71 | 67.46 ± 4.03 | 69.21 ± 3.29 | Ns |
| MCP-1 (pg/mL) | 173.14 ± 8.79 | 184.20 ± 11.66 | 177.58 ± 13.98 | 158.14 ± 18.82 | Ns |
| IL-8 (pg/mL) | 1.97 ± 0.23 | 1.93 ± 0.46 | 1.56 ± 0.35 | 2.48 ± 0.41 | Ns |
| RANTES (pg/mL) | 141.25 ± 14.26 | 141.27 ± 24.66 | 144.77 ± 26.87 | 137.18 ± 22.47 | Ns |
| Fractalkine (pg/mL) | 0.96 ± 0.20 | 1.10 ± 0.35 | 1.32 ± 0.40 | 0.42 ± 0.24 | Ns |
| MMP9 (ng/mL) | 90.98 ± 11.44 | 130.65 ± 31.63 | 78.19 ± 12.57 | 70.63 ± 12.30 | 0.038 * |
| LDL cholesterol (mg/dL) | 105.04 ± 4.61 | 110.19 ± 8.66 | 110.43 ± 8.33 | 94.17 ± 6.47 | Ns |
| Triglycerides (mg/dL) | 133.47 ± 6.59 | 128.00 ± 13.62 | 140.38 ± 11.99 | 130.28 ± 8.57 | Ns |
| HDL/LDL Ratio | 0.57 ± 0.03 | 0.53 ± 0.05 | 0.56 ± 0.04 | 0.61 ± 0.06 | Ns |
| BMI (Body Mass Index) | 27.26 ± 0.49 | 28.09 ± 0.85 | 26.79 ± 0.71 | 27.05 ± 1.00 | Ns |
| LRNCV (a.u.) | 0.25 ± 0.01 | 0.26 ± 0.02 | 0.25 ± 0.01 | 0.23 ± 0.01 | Ns |
| LRNCV (a.u.) (n° = 55) | ||
|---|---|---|
| Regression Coefficient | p-Value | |
| Framingham risk score (a.u.) | −0.003 | 0.479 |
| Diabetes | −0.015 | 0.811 |
| Oral antidiabetics therapy | 0.026 | 0.690 |
| Statin therapy use | −0.001 | 0.982 |
| Statin therapy dosage (mg/die) | −1.284 × 10−5 | 0.992 |
| Creatinine (mg/dL) | −0.012 | 0.855 |
| Hs-CRP (mg/dL) | 0.001 | 0.970 |
| IL-6 (pg/mL) | 0.001 | 0.942 |
| ICAM-1 (ng/mL) | −2.265 × 10−4 | 0.089 |
| VCAM-1 (ng/mL) | −7.039 × 10−5 | 0.401 |
| IFN-γ (pg/mL) | 0.003 | 0.066 |
| IL-10 (pg/mL) | −3.992 × 10−4 | 0.689 |
| TNF-α (pg/mL) | −0.001 | 0.327 |
| MCP-1 (pg/mL) | −1.718 × 10−4 | 0.418 |
| IL-8 (pg/mL) | 0.001 | 0.842 |
| RANTES (pg/mL) | −3.252 × 10−5 | 0.768 |
| Fractalkine (pg/mL) | 0.011 | 0.217 |
| MMP9 (ng/mL) | 2.220 × 10−4 | 0.185 |
| LDL cholesterol (mg/dL) | 0.001 | 0.110 |
| Triglycerides (mg/dL) | −1.697 × 10−4 | 0.619 |
| HDL/LDL ratio | 0.040 | 0.638 |
| BMI | 0.004 | 0.269 |
| LRNCV (a.u.) (n° = 55) | ||
|---|---|---|
| Regression Coefficient | p-Value | |
| WBC (n°/µL) | 1.225 × 10−5 | 0.053 |
| Neutrophil (n°/µL) | 1.750 × 10−5 | 0.021 |
| Neutrophil (n°/µL)/WBC (n°/µL) Ratio | 0.254 | 0.054 |
| Neutrophil (n°/µL)/Lymphocyte (n°/µL) Ratio (NLR) | 0.026 | 0.007 |
| Neutrophil (n°/µL)/PLT (n°/µL) Ratio | 4.234 | 0.014 |
| LRNCV (a.u.) (n° = 55) | ||
|---|---|---|
| Regression Coefficient | p-Value | |
| Neutrophils (N) vs. Lymphocytes (L) Phenotypic Ratios (RFI) | ||
| CD11b (N)/CD11b (L) | 0.074 | 0.009 |
| CD11b (N)/CD18 (L) | 0.133 | 0.001 |
| CD11b (N)/CCR5 (L) | 0.090 | 0.017 |
| CD11b (N)/CCR2 (L) | 0.071 | 0.011 |
| CD11b (N)/CXCR4 (L) | 0.069 | 0.053 |
| Neutrophils (N) vs. Monocytes (M) Phenotypic Ratios (RFI) | ||
| CD11b (N)/CCR5 (M) | 0.038 | 0.031 |
| CD11b (N)/CCR2 (M) | 0.136 | 0.001 |
| CD11b (N)/HLA-DR (M) | 0.193 | 0.009 |
| CD11b (N)/CD16 (M) | 0.030 | 0.035 |
| CD11b (N)/CD163 (M) | 0.165 | 0.0002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sbrana, S.; Cecchettini, A.; Bastiani, L.; Mazzone, A.; Vozzi, F.; Caselli, C.; Neglia, D.; Clemente, A.; Scholte, A.J.H.A.; Parodi, O.; et al. Association of Circulating Neutrophils with Relative Volume of Lipid-Rich Necrotic Core of Coronary Plaques in Stable Patients: A Substudy of SMARTool European Project. Life 2023, 13, 428. https://doi.org/10.3390/life13020428
Sbrana S, Cecchettini A, Bastiani L, Mazzone A, Vozzi F, Caselli C, Neglia D, Clemente A, Scholte AJHA, Parodi O, et al. Association of Circulating Neutrophils with Relative Volume of Lipid-Rich Necrotic Core of Coronary Plaques in Stable Patients: A Substudy of SMARTool European Project. Life. 2023; 13(2):428. https://doi.org/10.3390/life13020428
Chicago/Turabian StyleSbrana, Silverio, Antonella Cecchettini, Luca Bastiani, Annamaria Mazzone, Federico Vozzi, Chiara Caselli, Danilo Neglia, Alberto Clemente, Arthur J. H. A. Scholte, Oberdan Parodi, and et al. 2023. "Association of Circulating Neutrophils with Relative Volume of Lipid-Rich Necrotic Core of Coronary Plaques in Stable Patients: A Substudy of SMARTool European Project" Life 13, no. 2: 428. https://doi.org/10.3390/life13020428
APA StyleSbrana, S., Cecchettini, A., Bastiani, L., Mazzone, A., Vozzi, F., Caselli, C., Neglia, D., Clemente, A., Scholte, A. J. H. A., Parodi, O., Pelosi, G., & Rocchiccioli, S. (2023). Association of Circulating Neutrophils with Relative Volume of Lipid-Rich Necrotic Core of Coronary Plaques in Stable Patients: A Substudy of SMARTool European Project. Life, 13(2), 428. https://doi.org/10.3390/life13020428