
Pityriasis Versicolor—A Narrative Review on the Diagnosis and Management


 , , and
, , and 
Abstract
:1. Introduction
2. Aetiology
3. Epidemiology
4. Pathophysiology
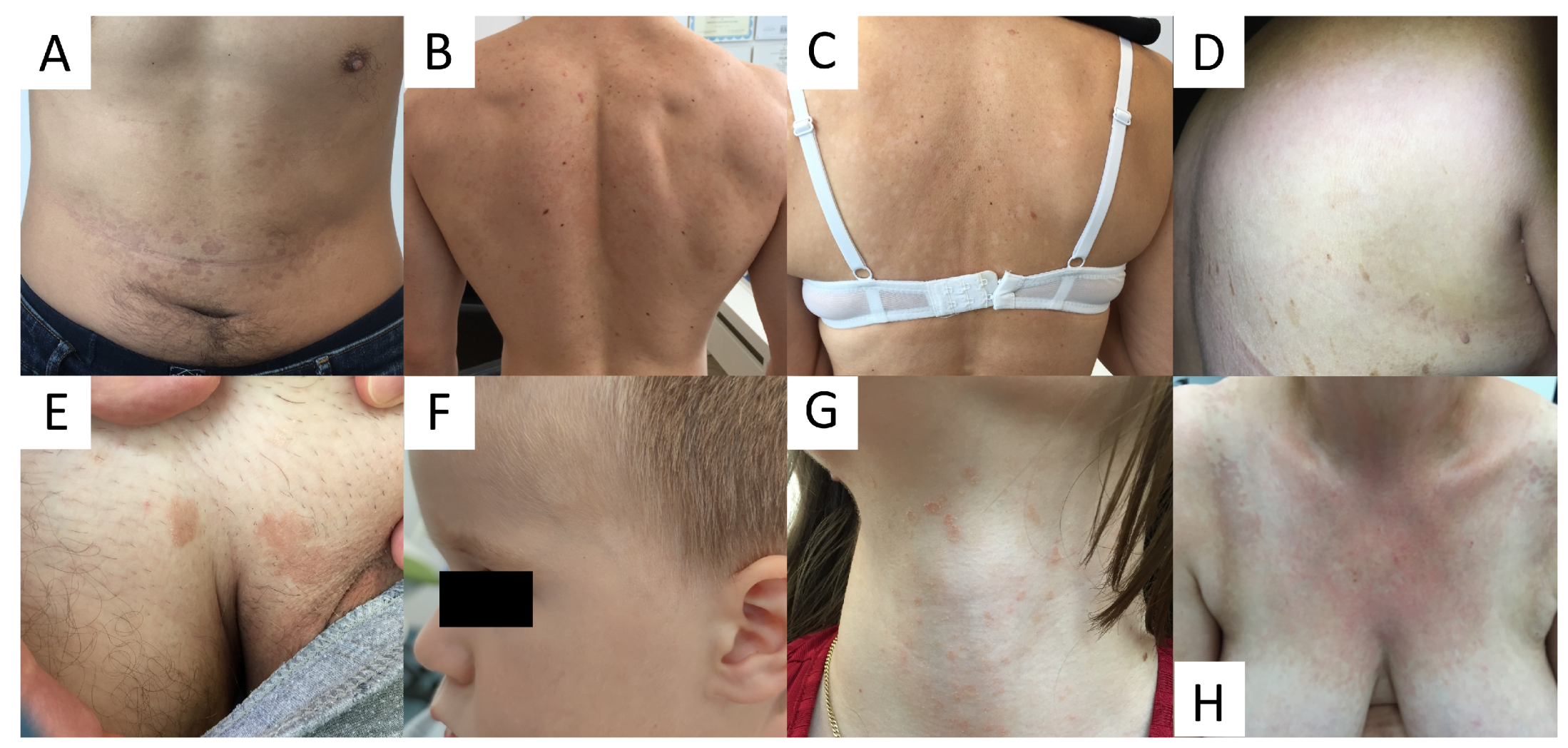
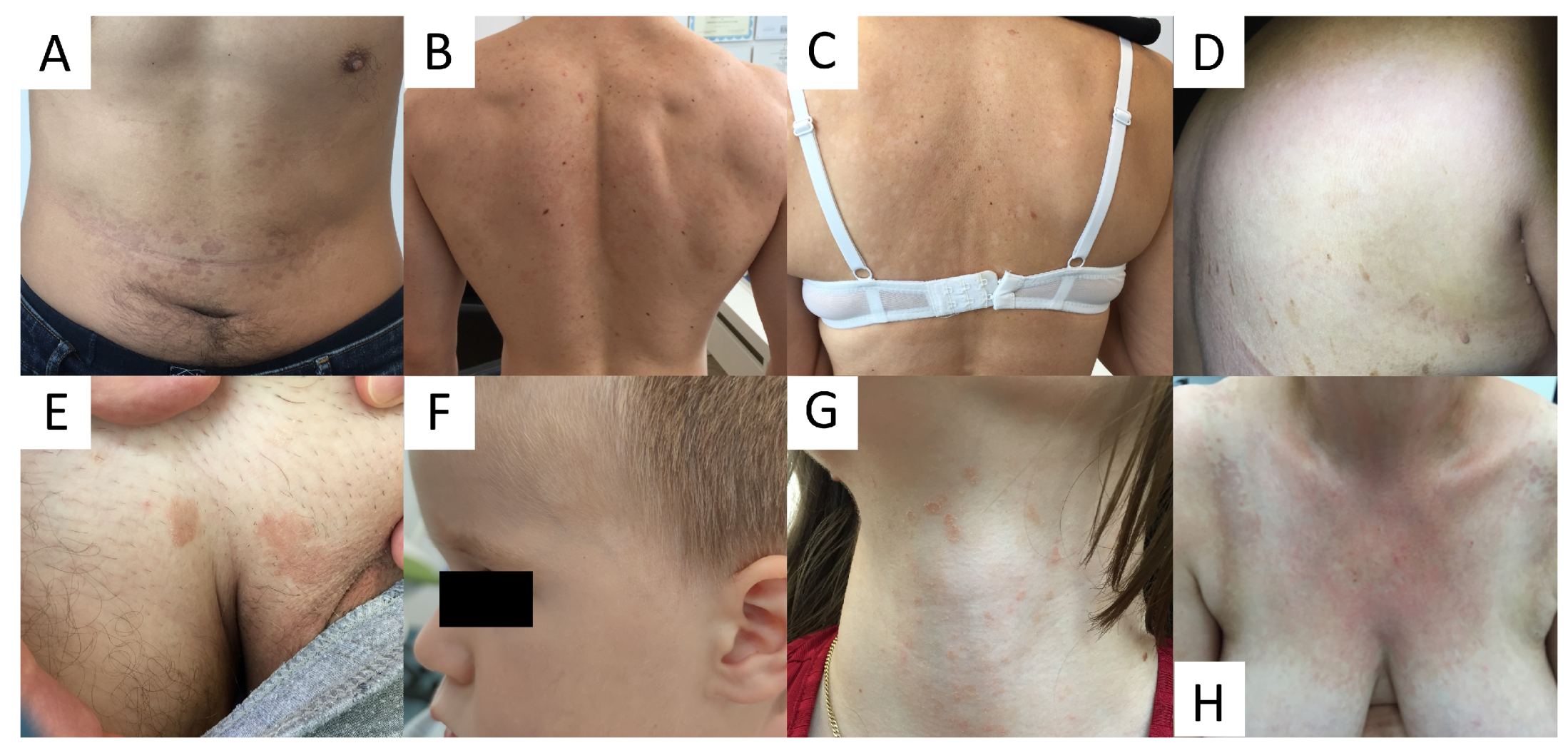
5. Clinical Presentation
6. Diagnosis
6.1. Culture
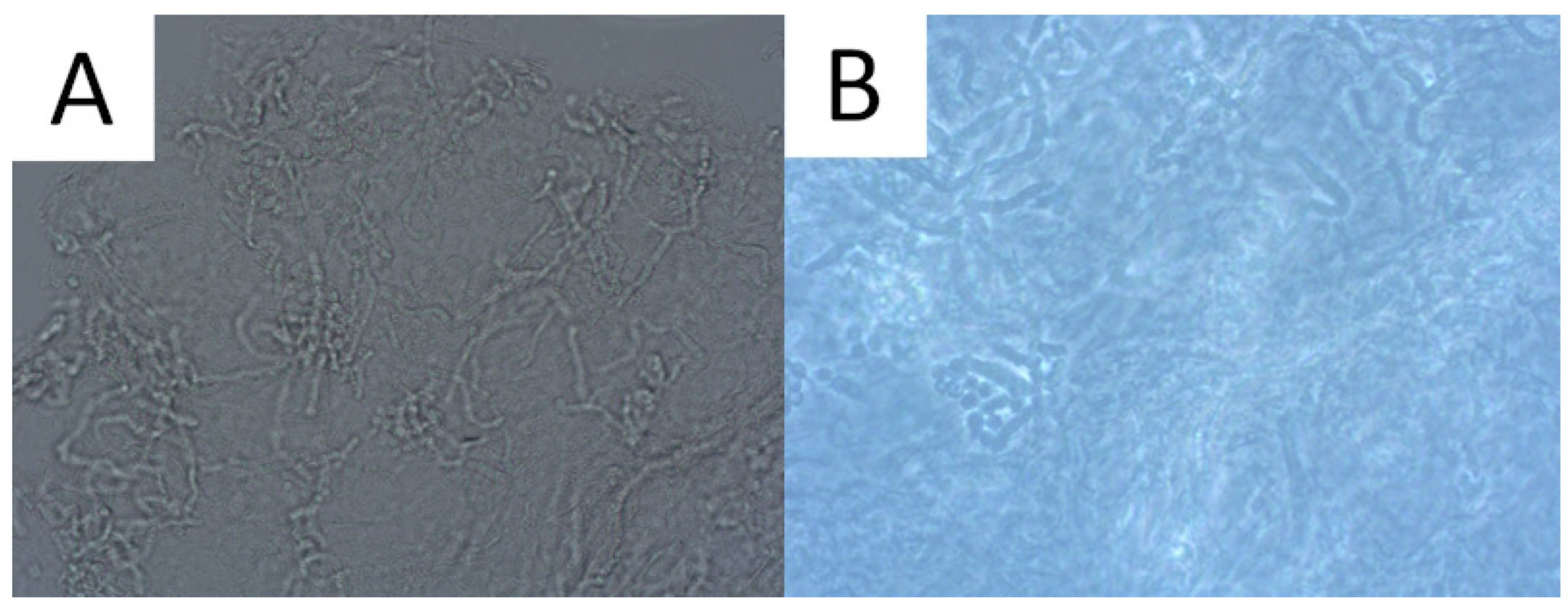
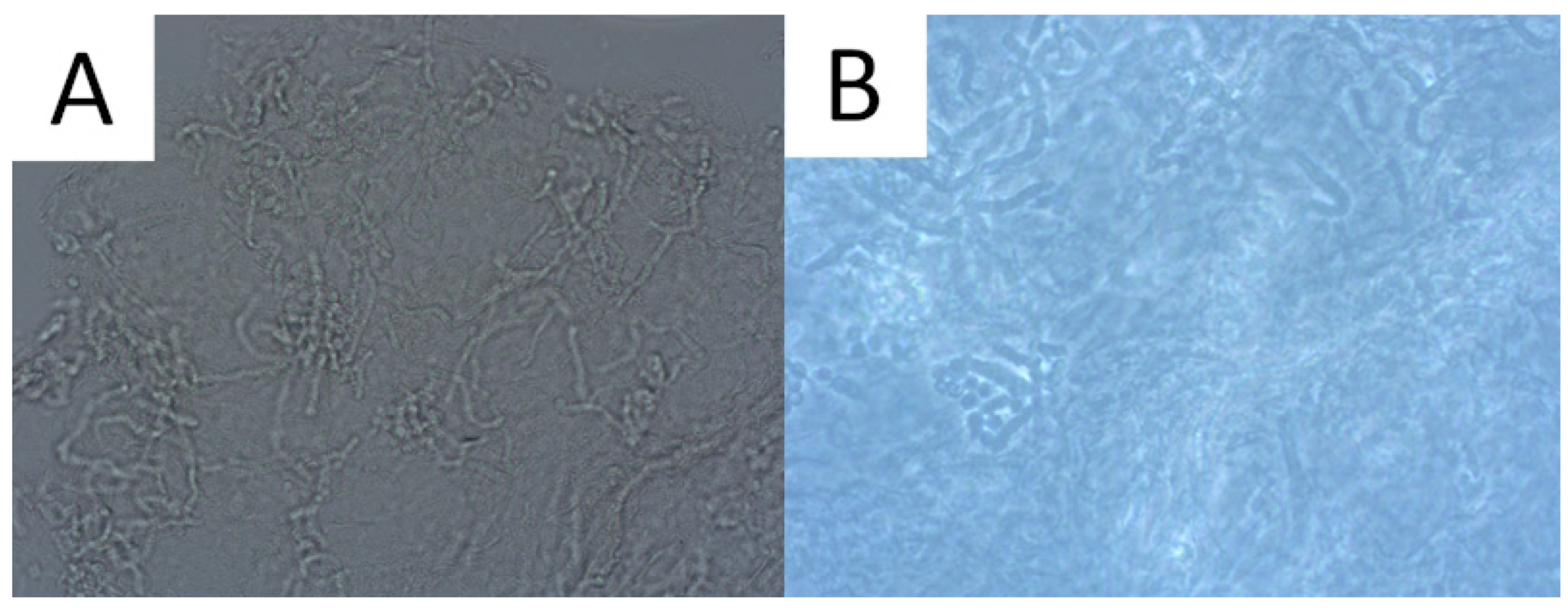
6.2. Direct Microscopic Examination
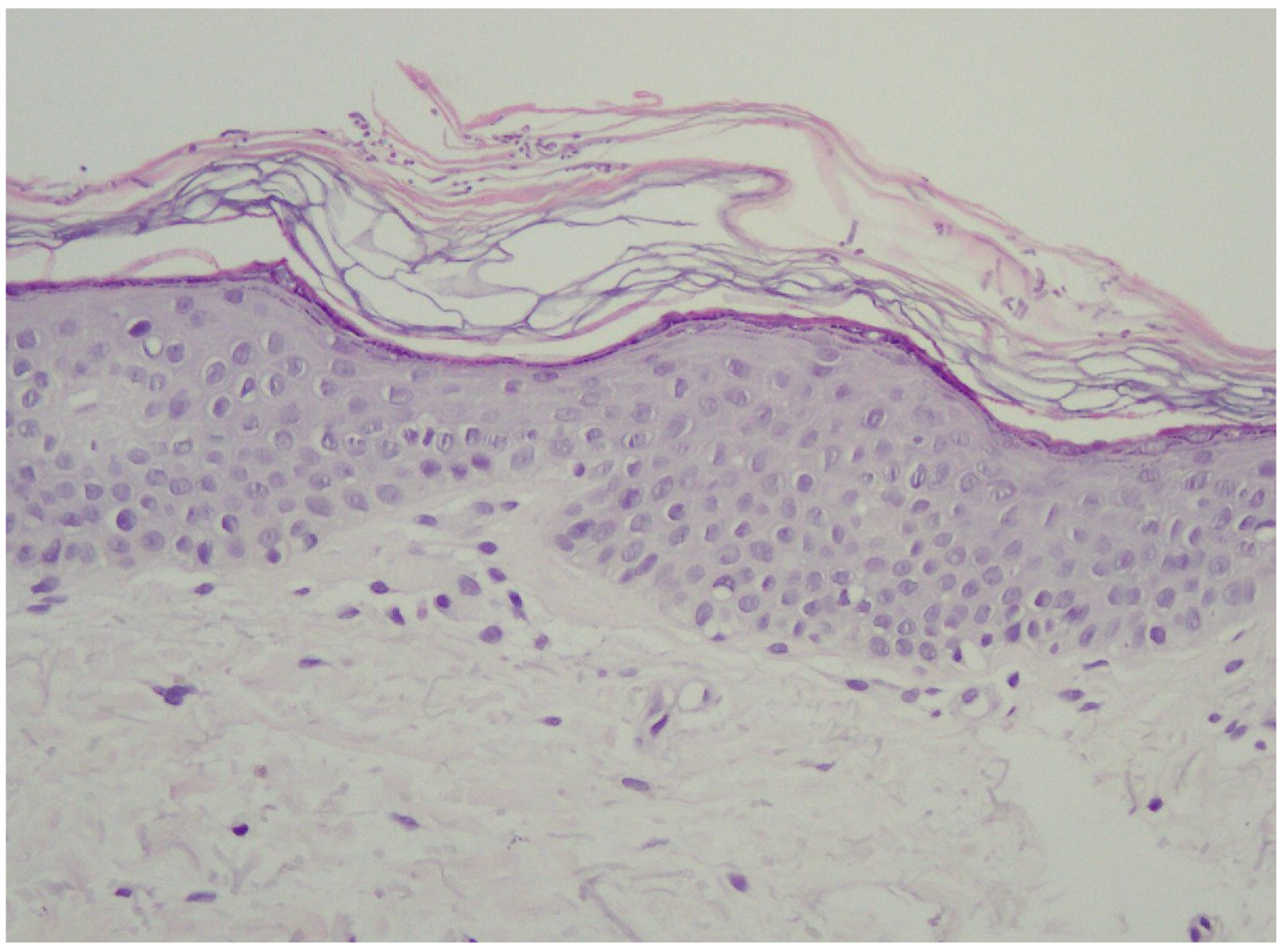
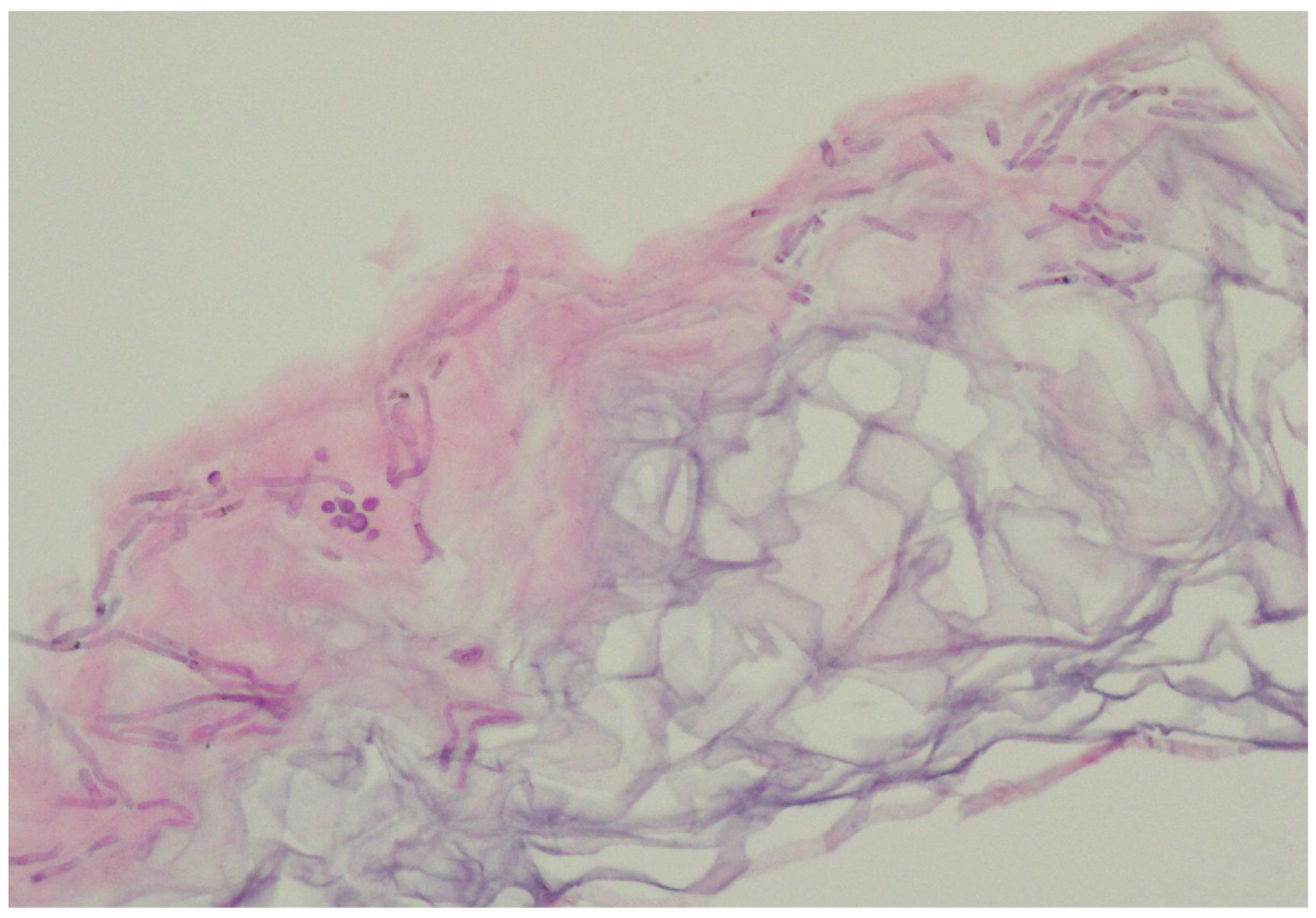
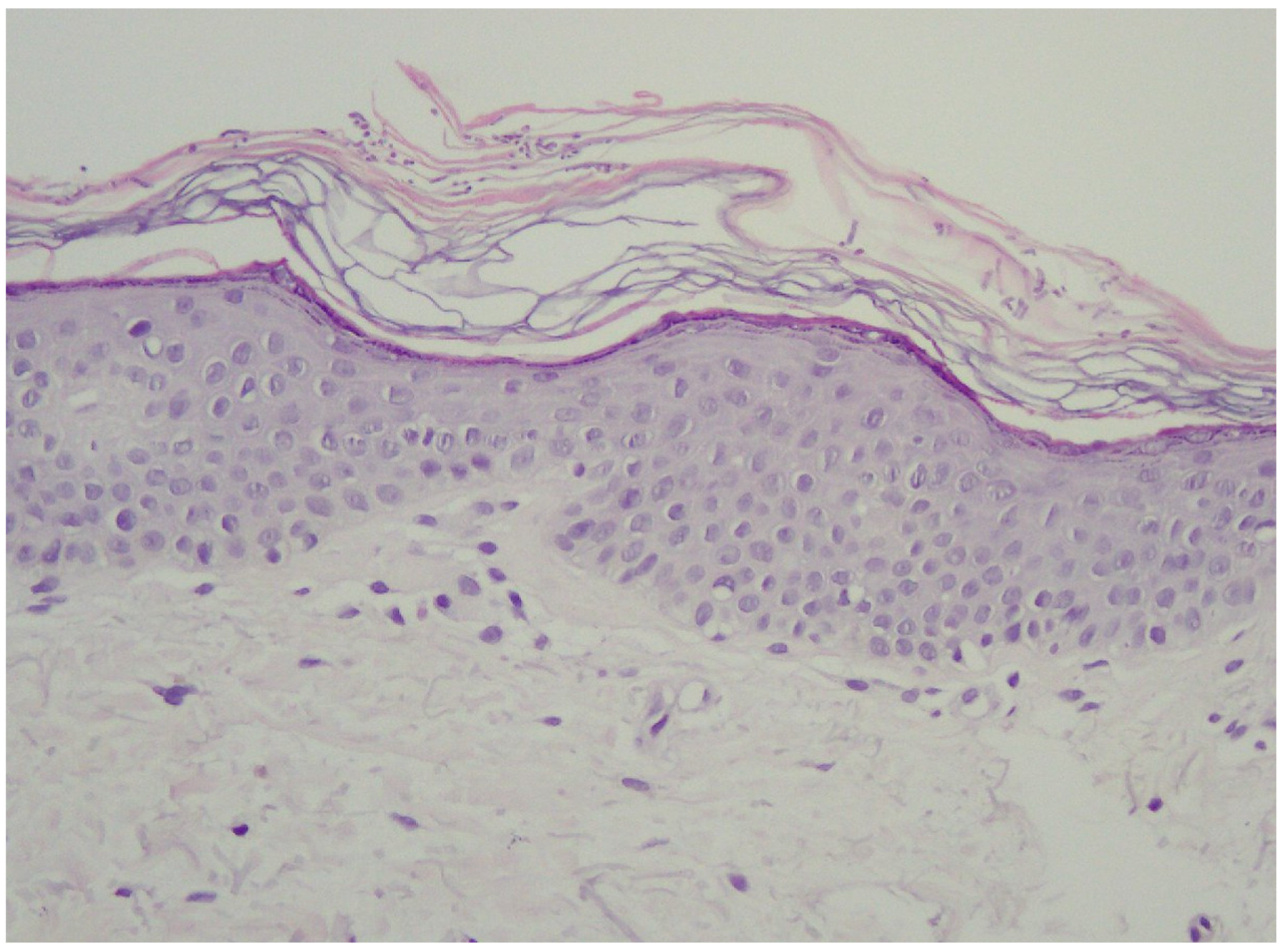
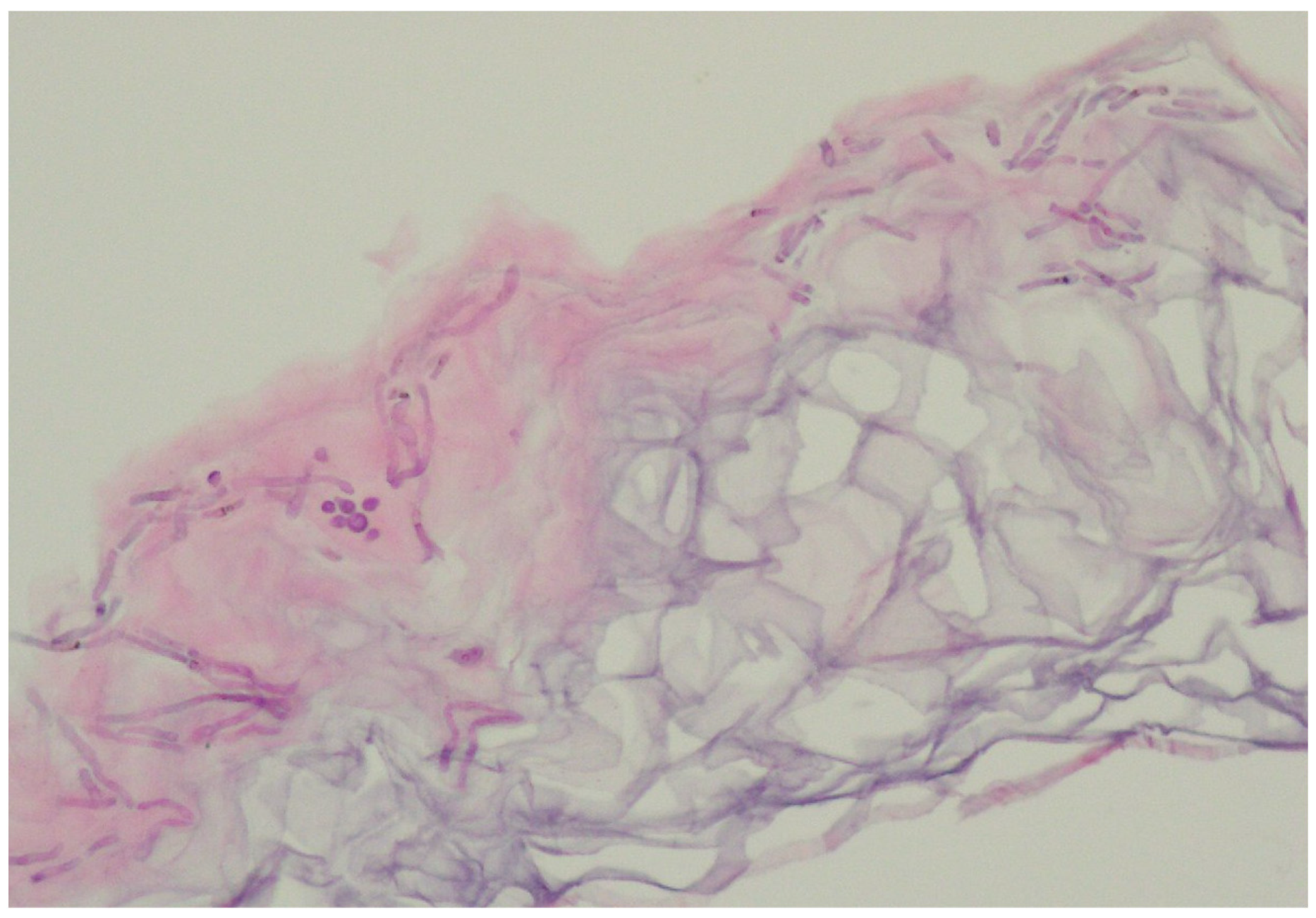
6.3. Histopathology
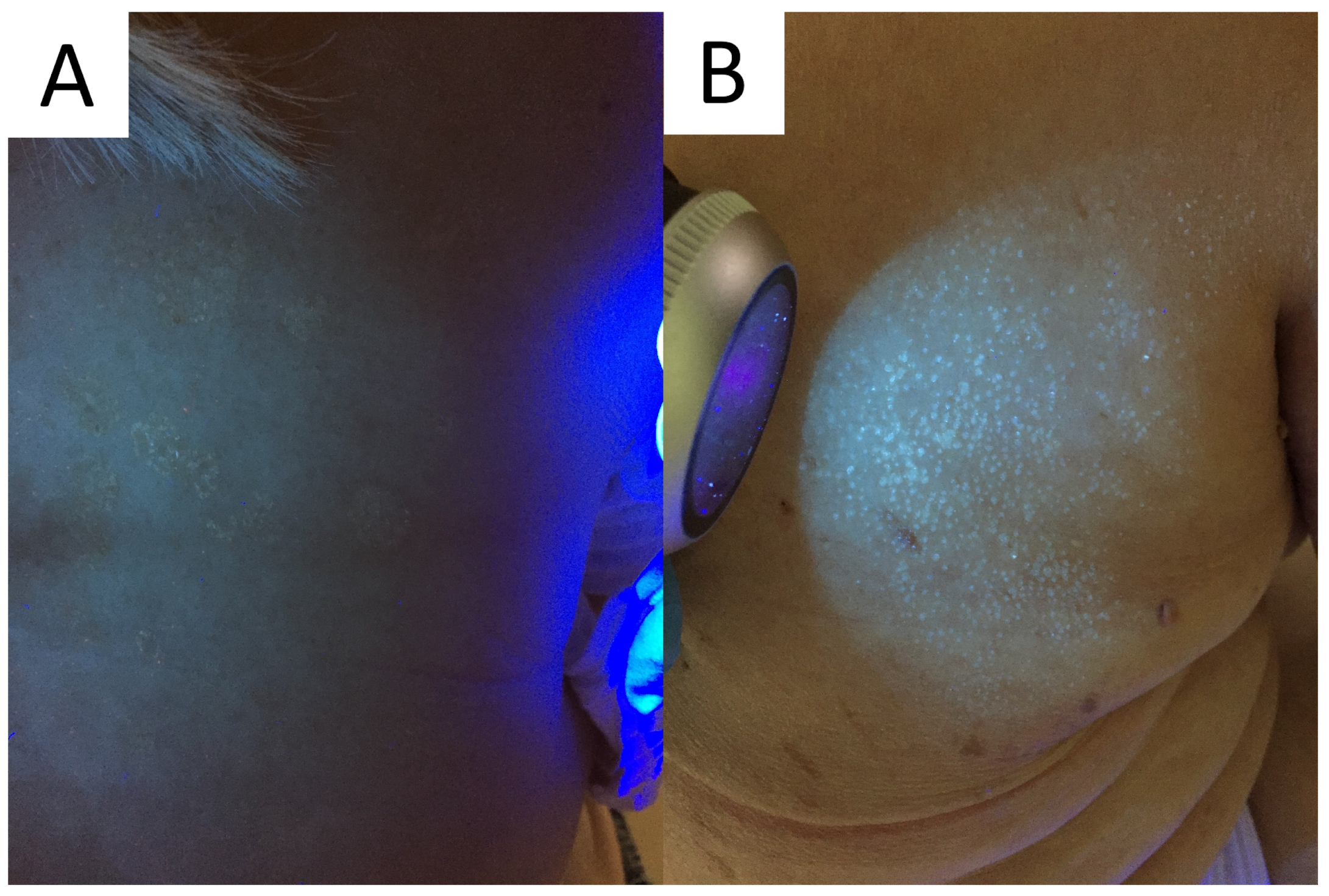
6.4. Wood’s Light
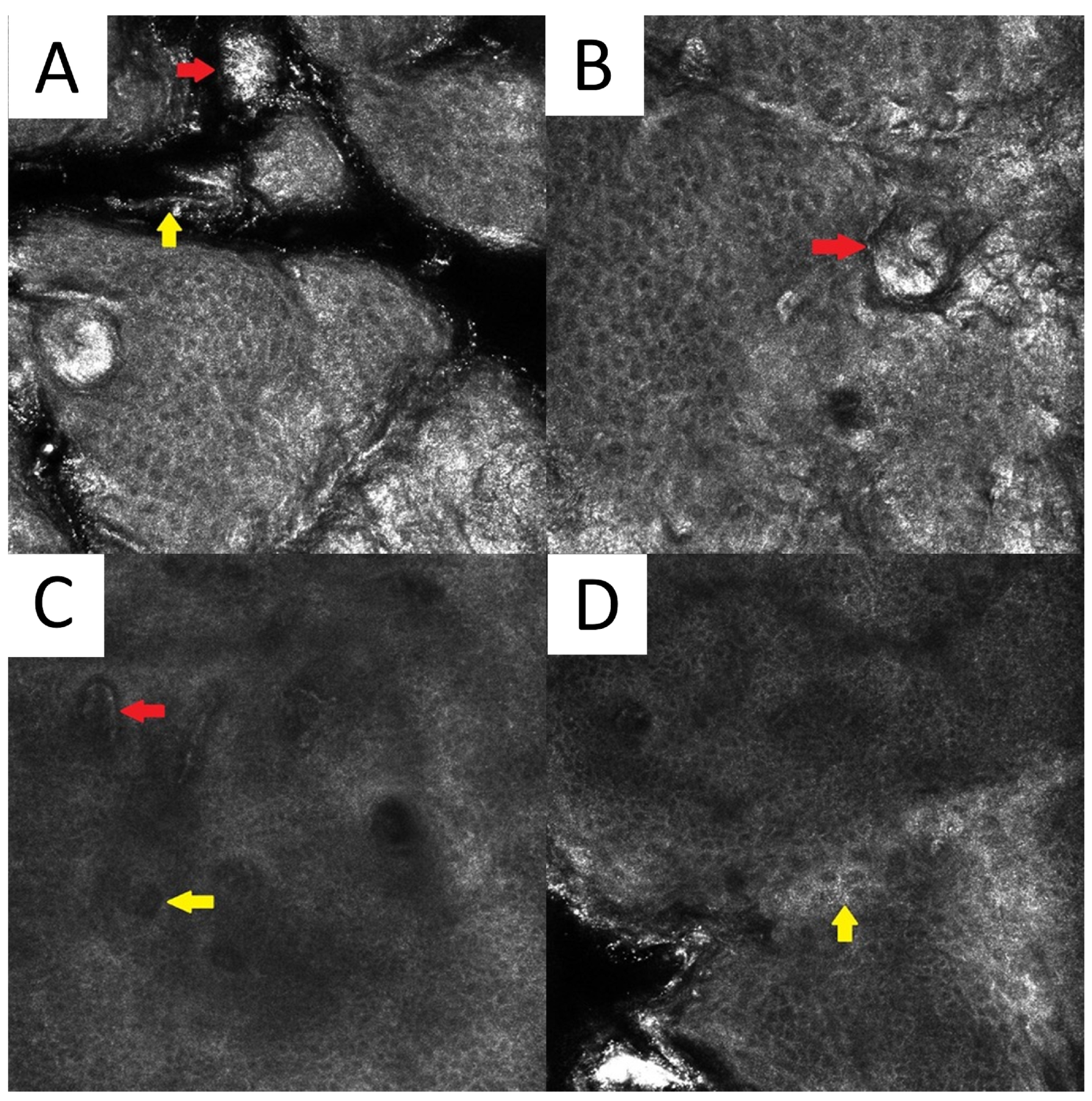
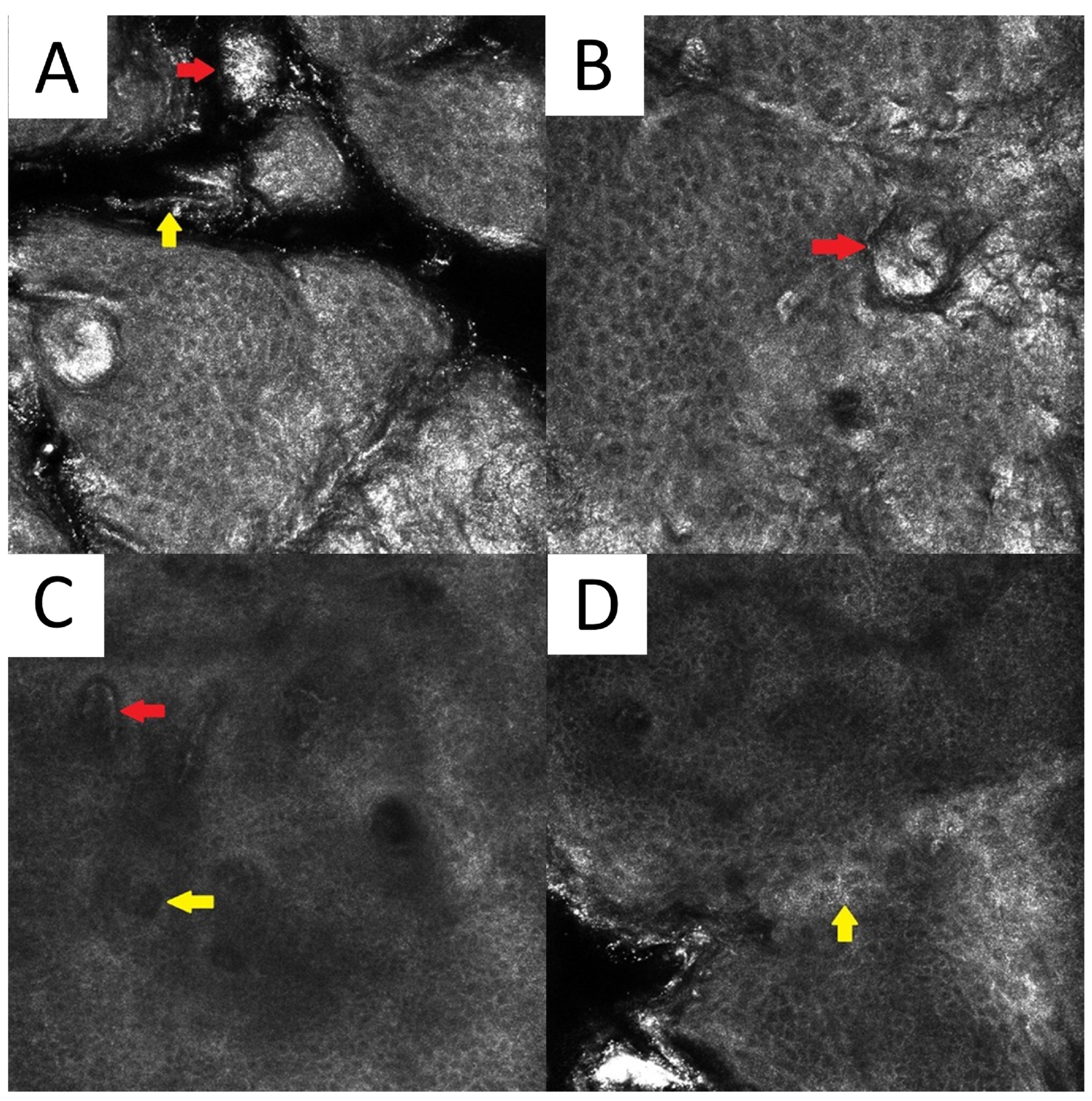
6.5. Reflectance Confocal Microscopy
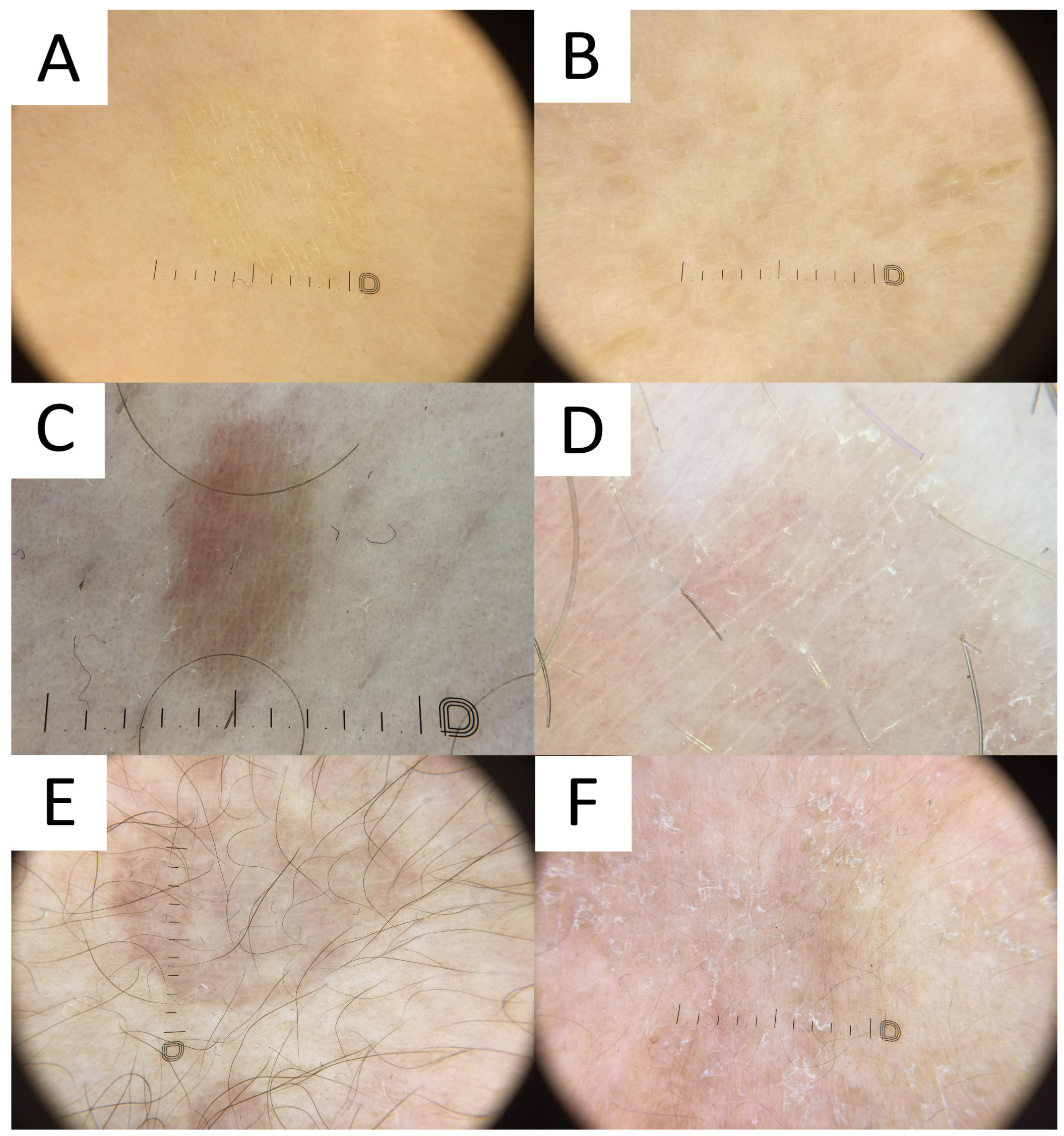
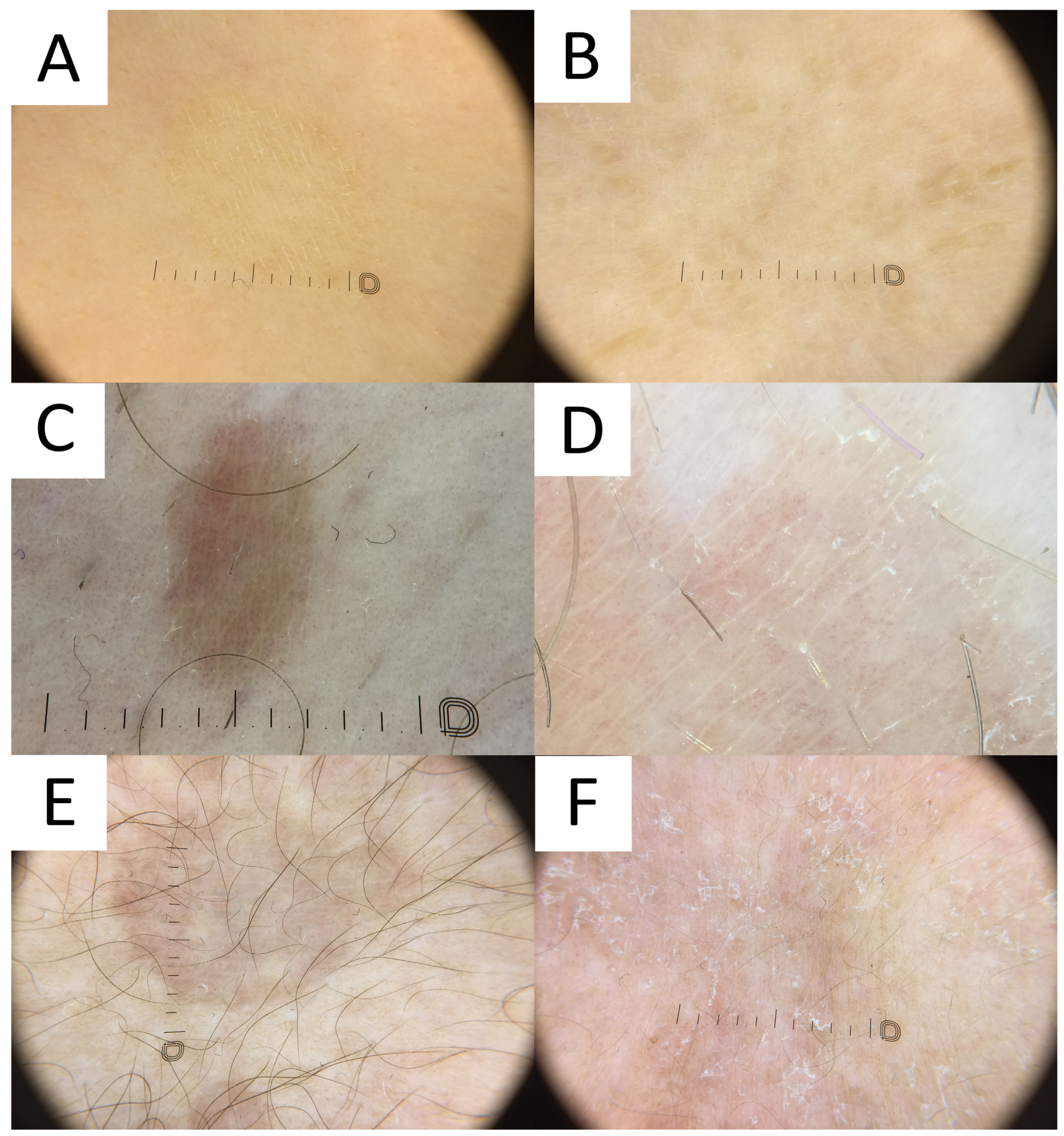
6.6. Dermatoscopy
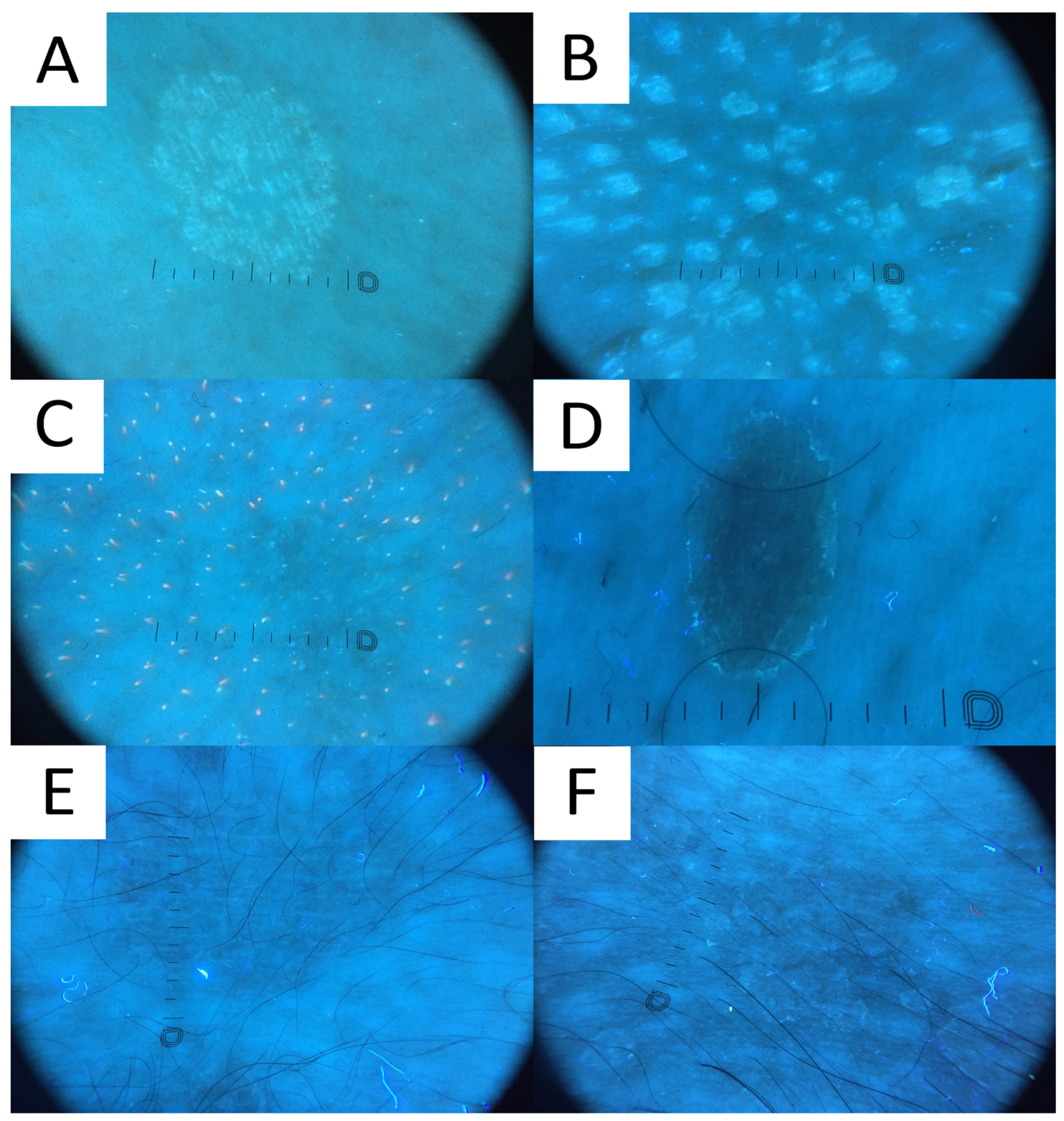
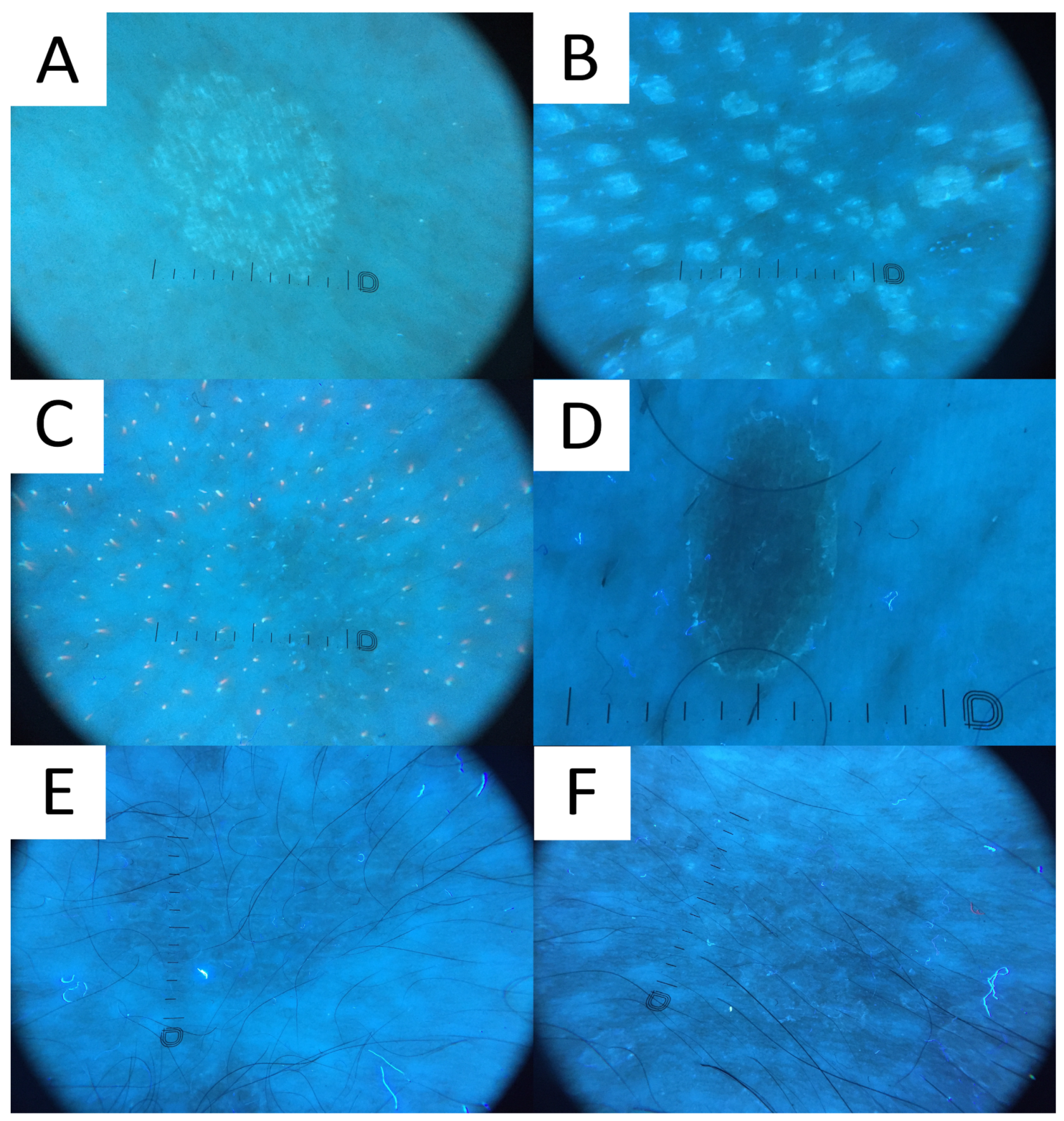
6.7. Ultraviolet-Induced Fluorescence Dermatoscopy
7. Treatment
8. General Recommendations to Limit the Risk of Recurrence
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karray, M.; McKinney, W.P. Tinea Versicolor; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Mathur, M.; Acharya, P.; Karki, A.; Kc, N.; Shah, J. Dermoscopic pattern of pityriasis versicolor. Clin. Cosmet. Investig. Dermatol. 2019, 12, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Krueger, L.; Saizan, A.; Stein, J.A.; Elbuluk, N. Dermoscopy of acquired pigmentary disorders: A comprehensive review. Int. J. Dermatol. 2022, 61, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.; Barankin, B.; Lam, J.M.; Leong, K.F.; Hon, K.L. Tinea versicolor: An updated review. Drugs Context 2022, 11. [Google Scholar] [CrossRef]
- Kaymak, Y.; Taner, E. Anxiety and depression in patients with pityriasis rosea compared to patients with tinea versicolor. Dermatol. Nurs. 2008, 20, 367–370+377. [Google Scholar] [PubMed]
- Gupta, A.K.; Foley, K.A. Antifungal Treatment for Pityriasis Versicolor. J. Fungi 2015, 1, 13–29. [Google Scholar] [CrossRef]
- Gupta, A.K.; Lyons, D.C. Pityriasis versicolor: An update on pharmacological treatment options. Expert Opin. Pharmacother. 2014, 15, 1707–1713. [Google Scholar] [CrossRef]
- Theelen, B.; Cafarchia, C.; Gaitanis, G.; Bassukas, I.D.; Boekhout, T.; Dawson, T.L., Jr. Malassezia ecology, pathophysiology, and treatment. Med. Mycol. 2018, 56, S10–S25. [Google Scholar] [CrossRef]
- Vijaya Chandra, S.H.; Srinivas, R.; Dawson, T.L., Jr.; Common, J.E. Cutaneous Malassezia: Commensal, Pathogen, or Protector? Front. Cell. Infect. Microbiol. 2020, 10, 614446. [Google Scholar] [CrossRef]
- Wang, Q.M.; Theelen, B.; Groenewald, M.; Bai, F.Y.; Boekhout, T. Moniliellomycetes and Malasseziomycetes, two new classes in Ustilaginomycotina. Persoonia 2014, 33, 41–47. [Google Scholar] [CrossRef]
- Ianiri, G.; Heitman, J. Approaches for Genetic Discoveries in the Skin Commensal and Pathogenic Malassezia Yeasts. Front. Cell. Infect. Microbiol. 2020, 10, 393. [Google Scholar] [CrossRef]
- Saunte, D.M.L.; Gaitanis, G.; Hay, R.J. Malassezia-Associated Skin Diseases, the Use of Diagnostics and Treatment. Front. Cell. Infect. Microbiol. 2020, 10, 112. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.A. Superficial fungal infections. Lancet 2004, 364, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Findley, K.; Oh, J.; Yang, J.; Conlan, S.; Deming, C.; Meyer, J.A.; Schoenfeld, D.; Nomicos, E.; Park, M.; Kong, H.H.; et al. Topographic diversity of fungal and bacterial communities in human skin. Nature 2013, 498, 367–370. [Google Scholar] [CrossRef]
- Dyląg, M.; Leniak, E.; Gnat, S.; Szepietowski, J.C.; Kozubowski, L. A case of anti-pityriasis versicolor therapy that preserves healthy mycobiome. BMC Dermatol. 2020, 20, 9. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.; Celis, A.M.; Guevara-Suarez, M.I.; Molina, J.; Carazzone, C. Yeast Smell Like What They Eat: Analysis of Volatile Organic Compounds of Malassezia furfur in Growth Media Supplemented with Different Lipids. Molecules 2019, 24, 419. [Google Scholar] [CrossRef] [PubMed]
- Jo, J.H.; Kennedy, E.A.; Kong, H.H. Topographical and physiological differences of the skin mycobiome in health and disease. Virulence 2017, 8, 324–333. [Google Scholar] [CrossRef]
- Alvarado, Z.; Pereira, C. Fungal diseases in children and adolescents in a referral centre in Bogota, Colombia. Mycoses 2018, 61, 543–548. [Google Scholar] [CrossRef]
- De Luca, D.A.; Maianski, Z.; Averbukh, M. A study of skin disease spectrum occurring in Angola phototype V–VI population in Luanda. Int. J. Dermatol. 2018, 57, 849–855. [Google Scholar] [CrossRef]
- Musicante, M.; Bembry, R.; Wright, T.S. Tinea versicolor in a premature infant. Pediatr. Dermatol. 2023, 40, 578–579. [Google Scholar] [CrossRef]
- Renati, S.; Cukras, A.; Bigby, M. Pityriasis versicolor. BMJ 2015, 350, h1394. [Google Scholar] [CrossRef] [PubMed]
- Maleszka, R.; Adamski, Z.; Szepietowski, J.; Baran, E. Treatment of superficial fungal infections—Recommendations of experts of Mycological Section of Polish Dermatological Society. Dermatol. Rev. 2015, 4, 305–315. [Google Scholar] [CrossRef]
- Crespo-Erchiga, V.; Florencio, V.D. Malassezia yeasts and pityriasis versicolor. Curr. Opin. Infect. Dis. 2006, 19, 139–147. [Google Scholar] [CrossRef]
- Dobler, D.; Schmidts, T.; Wildenhain, S.; Seewald, I.; Merzhäuser, M.; Runkel, F. Impact of Selected Cosmetic Ingredients on Common Microorganisms of Healthy Human Skin. Cosmetics 2019, 6, 45. [Google Scholar] [CrossRef]
- Ashbee, H.R.; Evans, E.G. Immunology of diseases associated with Malassezia species. Clin. Microbiol. Rev. 2002, 15, 21–57. [Google Scholar] [CrossRef] [PubMed]
- Prohic, A.; Jovovic Sadikovic, T.; Krupalija-Fazlic, M.; Kuskunovic-Vlahovljak, S. Malassezia species in healthy skin and in dermatological conditions. Int. J. Dermatol. 2016, 55, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Goh, B.N.; Teh, W.K.; Jiang, Z.; Goh, J.P.Z.; Goh, A.; Wu, G.; Hoon, S.S.; Raida, M.; Camattari, A.; et al. Skin Commensal Malassezia globosa Secreted Protease Attenuates Staphylococcus aureus Biofilm Formation. J. Investig. Dermatol. 2018, 138, 1137–1145. [Google Scholar] [CrossRef]
- Yang, H.O.; Cho, Y.J.; Lee, J.M.; Kim, K.D. Transcriptional Interplay between Malassezia restricta and Staphylococcus Species Co-Existing in the Skin Environment. J. Microbiol. Biotechnol. 2023, 33, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Goh, J.P.Z.; Ruchti, F.; Poh, S.E.; Koh, W.L.C.; Tan, K.Y.; Lim, Y.T.; Thng, S.T.G.; Sobota, R.M.; Hoon, S.S.; Liu, C.; et al. The human pathobiont Malassezia furfur secreted protease Mfsap1 regulates cell dispersal and exacerbates skin inflammation. Proc. Natl. Acad. Sci. USA 2022, 119, e2212533119. [Google Scholar] [CrossRef] [PubMed]
- Satala, D.; Bras, G.; Kozik, A.; Rapala-Kozik, M.; Karkowska-Kuleta, J. More than Just Protein Degradation: The Regulatory Roles and Moonlighting Functions of Extracellular Proteases Produced by Fungi Pathogenic for Humans. J. Fungi. 2023, 9, 121. [Google Scholar] [CrossRef]
- Poh, S.E.; Goh, J.P.Z.; Fan, C.; Chua, W.; Gan, S.Q.; Lim, P.L.K.; Sharma, B.; Leavesley, D.I.; Dawson, T.L., Jr.; Li, H. Identification of Malassezia furfur Secreted Aspartyl Protease 1 (MfSAP1) and Its Role in Extracellular Matrix Degradation. Front. Cell. Infect. Microbiol. 2020, 10, 148. [Google Scholar] [CrossRef]
- DeAngelis, Y.M.; Gemmer, C.M.; Kaczvinsky, J.R.; Kenneally, D.C.; Schwartz, J.R.; Dawson, T.L., Jr. Three etiologic facets of dandruff and seborrheic dermatitis: Malassezia fungi, sebaceous lipids, and individual sensitivity. J. Investig. Dermatol. Symp. Proc. 2005, 10, 295–297. [Google Scholar] [CrossRef]
- Kanitakis, J.; Giannopoulos, Z.; Tourkantonis, A.; Kanitakis, C. HLA antigens in pityriasis versicolor. Tissue Antigens 1984, 23, 47–49. [Google Scholar] [CrossRef]
- Grice, E.A.; Dawson, T.L. Host–microbe interactions: Malassezia and human skin. Curr. Opin. Microbiol. 2017, 40, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Mayser, P.; Schäfer, U.; Krämer, H.J.; Irlinger, B.; Steglich, W. Pityriacitrin—An ultraviolet-absorbing indole alkaloid from the yeast Malassezia furfur. Arch. Dermatol. Res. 2002, 294, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Krämer, H.J.; Boms, S.; Skrygan, M.; Tomi, N.S.; Altmeyer, P.; Mayser, P. Quantification of ultraviolet protective effects of pityriacitrin in humans. Arch. Dermatol. Res. 2007, 299, 517–520. [Google Scholar] [CrossRef] [PubMed]
- Galadari, I.; el Komy, M.; Mousa, A.; Hashimoto, K.; Mehregan, A.H. Tinea versicolor: Histologic and ultrastructural investigation of pigmentary changes. Int. J. Dermatol. 1992, 31, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Chebil, W.; Rhimi, W.; Haouas, N.; Romano, V.; Belgacem, S.; Belhadj Ali, H.; Babba, H.; Cafarchia, C. Virulence factors of Malassezia strains isolated from pityriasis versicolor patients and healthy individuals. Med. Mycol. 2022, 60, myac060. [Google Scholar] [CrossRef]
- Dawson, T.; Gemmer, C. Dandruff and seborrheic dermatitis likely result from scalp barrier breach and irritation induced by Malassezia metabolites, particularly free fatty acids. J. Am. Acad. Dermatol. 2005, 52, P49. [Google Scholar] [CrossRef]
- Takahagi, S.; Tanaka, A.; Hide, M. Sweat allergy. Allergol. Int. 2018, 67, 435–441. [Google Scholar] [CrossRef]
- Ishii, K.; Hiragun, M.; Hiragun, T.; Kan, T.; Kawaguchi, T.; Yanase, Y.; Tanaka, A.; Takahagi, S.; Hide, M. A human monoclonal IgE antibody that binds to MGL_1304, a major allergen in human sweat, without activation of mast cells and basophils. Biochem. Biophys. Res. Commun. 2015, 468, 99–104. [Google Scholar] [CrossRef]
- Hiragun, M.; Hiragun, T.; Ishii, K.; Suzuki, H.; Tanaka, A.; Yanase, Y.; Mihara, S.; Haruta, Y.; Kohno, N.; Hide, M. Elevated serum IgE against MGL_1304 in patients with atopic dermatitis and cholinergic urticaria. Allergol. Int. 2014, 63, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Gallo, L.; Fabbrocini, G.; Picone, V. “PiMa sign”: A possible correlation between dermographism and pityriasis versicolor? J. Cosmet. Dermatol. 2023, 22, 689–691. [Google Scholar] [CrossRef]
- Gaitanis, G.; Chasapi, V.; Velegraki, A. Novel application of the masson-fontana stain for demonstrating Malassezia species melanin-like pigment production in vitro and in clinical specimens. J. Clin. Microbiol. 2005, 43, 4147–4151. [Google Scholar] [CrossRef] [PubMed]
- Youngchim, S.; Nosanchuk, J.D.; Pornsuwan, S.; Kajiwara, S.; Vanittanakom, N. The role of L-DOPA on melanization and mycelial production in Malassezia furfur. PLoS ONE 2013, 8, e63764. [Google Scholar] [CrossRef]
- Hoffmann, R.; Wenzel, E.; Huth, A.; van der Steen, P.; Schäufele, M.; Henninger, H.P.; Happle, R. Cytokine mRNA levels in Alopecia areata before and after treatment with the contact allergen diphenylcyclopropenone. J. Invest. Dermatol. 1994, 103, 530–533. [Google Scholar] [CrossRef] [PubMed]
- Tazi-Ahnini, R.; McDonagh, A.J.G.; Cox, A.; Messenger, A.G.; Britton, J.E.R.; Ward, S.J.; Båvik, C.O.; Duff, G.W.; Cork, M.J. Association analysis of IL1A and IL1B variants in alopecia areata. Heredity 2001, 87, 215–219. [Google Scholar] [CrossRef]
- Hoffmann, R.; Eicheler, W.; Wenzel, E.; Happle, R. Interleukin-1beta-induced inhibition of hair growth in vitro is mediated by cyclic AMP. J. Investig. Dermatol. 1997, 108, 40–42. [Google Scholar] [CrossRef]
- Mostafa, W.Z.; Assaf, M.I.; Ameen, I.A.; El Safoury, O.S.; Al Sulh, S.A. Hair loss in pityriasis versicolor lesions: A descriptive clinicopathological study. J. Am. Acad. Dermatol. 2013, 69, e19–e23. [Google Scholar] [CrossRef]
- Gaitanis, G.; Magiatis, P.; Hantschke, M.; Bassukas, I.D.; Velegraki, A. The Malassezia genus in skin and systemic diseases. Clin. Microbiol. Rev. 2012, 25, 106–141. [Google Scholar] [CrossRef]
- Al-Refu, K. Dermoscopy is a new diagnostic tool in diagnosis of common hypopigmented macular disease: A descriptive study. Dermatol. Rep. 2019, 11, 7916. [Google Scholar] [CrossRef]
- Kaur, I.; Jakhar, D.; Singal, A. Dermoscopy in the Evaluation of Pityriasis Versicolor: A Cross Sectional Study. Indian Dermatol. Online J. 2019, 10, 682–685. [Google Scholar] [CrossRef] [PubMed]
- Han, A.; Calcara, D.; Stoecker, W.; Daly, J.; Siegel, D.; Shell, A. Evoked Scale Sign of Tinea Versicolor. Arch. Dermatol. 2009, 145, 1078. [Google Scholar] [CrossRef] [PubMed]
- Rivard, S.C. Pityriasis versicolor: Avoiding pitfalls in disease diagnosis and therapy. Mil. Med. 2013, 178, 904–906. [Google Scholar] [CrossRef]
- Thomas, I.N.; James, J.J.; Bala, A.; Mohan, S.; Dogiparthi, S.; Shanmugam, N.P., Sr. Usage of Dermoscopy as an Effective Diagnostic Tool in Pityriasis Alba: A Prospective Observational Study Among Children in a Suburban Hospital in South India. Cureus 2023, 15, e40271. [Google Scholar] [CrossRef]
- Lallas, A.; Errichetti, E.; Ioannides, D. (Eds.) Dermoscopy in General Dermatology, 1st ed.; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar] [CrossRef]
- Mohta, A.; Jain, S.K.; Agrawal, A.; Kushwaha, R.K.; Sharma, P.; Sethia, K.; Jain, M. Dermoscopy in Leprosy: A Clinical and Histopathological Correlation Study. Dermatol. Pract. Concept. 2021, 11, e2021032. [Google Scholar] [CrossRef]
- Bhat, Y.J.; Khare, S.; Nabi, N. Dermoscopy of disorders of hypopigmentation. Pigment. Int. 2022, 9, 4–13. [Google Scholar] [CrossRef]
- Jindal, R.; Sethi, S.; Chauhan, P. Dermoscopy of Facial Angiofibromas in Four Patients of Skin of Color with Tuberous Sclerosis Complex: A Case-Series. Dermatol. Pract. Concept. 2021, 11, e2021036. [Google Scholar] [CrossRef]
- Thakur, V.; Dev, A.; Vinay, K. Dermatoscopy of Nevus Anemicus. Indian Dermatol. Online J. 2022, 13, 822–823. [Google Scholar] [CrossRef]
- Nakamura, M.; Huerta, T.; Williams, K.; Hristov, A.C.; Tejasvi, T. Dermoscopic Features of Mycosis Fungoides and Its Variants in Patients with Skin of Color: A Retrospective Analysis. Dermatol. Pract. Concept 2021, 11, e2021048. [Google Scholar] [CrossRef] [PubMed]
- Errichetti, E.; Maione, V.; Stinco, G. Dermatoscopy of confluent and reticulated papillomatosis (Gougerot-Carteaud syndrome). J. Dtsch. Dermatol. Ges. 2017, 15, 836–838. [Google Scholar] [CrossRef] [PubMed]
- Ingordo, V.; Iannazzone, S.S.; Cusano, F.; Naldi, L. Dermoscopic features of congenital melanocytic nevus and Becker nevus in an adult male population: An analysis with a 10-fold magnification. Dermatology 2006, 212, 354–360. [Google Scholar] [CrossRef]
- Vasani, R.J. Idiopathic Eruptive Macular Pigmentation—Uncommon Presentation of an Uncommon Condition. Indian J. Dermatol. 2018, 63, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Aslam, A.; Bhat, Y.J.; Latif, I.; Saqib, N.U.; Hassan Shah, I. A rare diagnosis of idiopathic eruptive macular pigmentation with dermoscopy. A case report. Our Dermatol. Online 2020, 11, 252–254. [Google Scholar] [CrossRef]
- Hamdino, M.; Saudy, A.A.; El-Shahed, L.H.; Taha, M. Identification of Malassezia species isolated from some Malassezia associated skin diseases. J. Mycol. Med. 2022, 32, 101301. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Koticha, A.; Ubale, M.; Wanjare, S.; Mehta, P.; Khopkar, U. Identification and speciation of malassezia in patients clinically suspected of having pityriasis versicolor. Indian J. Dermatol. 2013, 58, 239. [Google Scholar] [CrossRef]
- Porto, J.A. The use of cellophane tape in the diagnosis of Tinea versicolor. J. Investig. Dermatol. 1953, 21, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Guarner, J.; Brandt, M.E. Histopathologic diagnosis of fungal infections in the 21st century. Clin. Microbiol. Rev. 2011, 24, 247–280. [Google Scholar] [CrossRef] [PubMed]
- Allen, H.B.; Charles, C.R.; Johnson, B.L. Hyperpigmented tinea versicolor. Arch. Dermatol. 1976, 112, 1110–1112. [Google Scholar] [CrossRef]
- Pietkiewicz, P.; Navarrete-Dechent, C.; Goldust, M.; Korecka, K.; Todorovska, V.; Errichetti, E. Differentiating Fordyce Spots from Their Common Simulators Using Ultraviolet-Induced Fluorescence Dermatoscopy—Retrospective Study. Diagnostics 2023, 13, 985. [Google Scholar] [CrossRef]
- Mojeski, J.A.; Almashali, M.; Jowdy, P.; Fitzgerald, M.E.; Brady, K.L.; Zeitouni, N.C.; Colegio, O.R.; Paragh, G. Ultraviolet imaging in dermatology. Photodiagn. Photodyn. Ther. 2020, 30, 101743. [Google Scholar] [CrossRef]
- Pietkiewicz, P.; Navarrete-Dechent, C.; Salwowska, N.; Cantisani, C.; Goldust, M.; Errichetti, E. Ultraviolet-Induced Fluorescence Dermoscopy Reveals Fluorescent Clues in Pitted Keratolysis. Dermatol. Pract. Concept. 2023, 13, e2023242. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, R.; Soares-de-Almeida, L.; Arzberger, E.; Ferreira, J.; Leal-Filipe, P.; Bastos, P.M.; Oliveira, A.L. Reflectance confocal microscopy for the diagnosis of skin infections and infestations. Dermatol. Online J. 2020, 26. [Google Scholar] [CrossRef]
- Errichetti, E.; Zalaudek, I.; Kittler, H.; Apalla, Z.; Argenziano, G.; Bakos, R.; Blum, A.; Braun, R.P.; Ioannides, D.; Lacarrubba, F.; et al. Standardization of dermoscopic terminology and basic dermoscopic parameters to evaluate in general dermatology (non-neoplastic dermatoses): An expert consensus on behalf of the International Dermoscopy Society. Br. J. Dermatol. 2020, 182, 454–467. [Google Scholar] [CrossRef]
- Kapadia, F.; Kharkar, V.; Vishwanath, T. Dermoscopy to the Rescue in an Annular Enigma: A Rare Case of Annular Pityriasis Versicolor Presenting in an Unusual Location. Dermatol. Pract. Concept. 2022, 12, e2022057. [Google Scholar] [CrossRef] [PubMed]
- Al-Nasiri, M.; Navarrete-Dechent, C.; Korecka, K.; Salwowska, N.; Goldust, M.; Pietkiewicz, P. Ultraviolet-Induced Fluorescence Dermatoscopy of Trichobacteriosis Axillaris Reveals Peripilar Yellow-Green Luminescent Concretions. Dermatol. Pract. Concept. 2023, 13, e2023169. [Google Scholar] [CrossRef] [PubMed]
- Asawanonda, P.; Taylor, C.R. Wood’s light in dermatology. Int. J. Dermatol. 1999, 38, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Mayser, P.; Stapelkamp, H.; Krämer, H.J.; Podobinska, M.; Wallbott, W.; Irlinger, B.; Steglich, W. Pityrialactone—A new fluorochrome from the tryptophan metabolism of Malassezia furfur. Antonie Van Leeuwenhoek 2003, 84, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Patwardhan, S.V.; Richter, C.; Vogt, A.; Blume-Peytavi, U.; Canfield, D.; Kottner, J. Measuring acne using Coproporphyrin III, Protoporphyrin IX, and lesion-specific inflammation: An exploratory study. Arch. Dermatol. Res. 2017, 309, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Brennan, B.; Leyden, J.J. Overview of topical therapy for common superficial fungal infections and the role of new topical agents. J. Am. Acad. Dermatol. 1997, 36, S3–S8. [Google Scholar] [CrossRef]
- Choi, F.D.; Juhasz, M.L.W.; Atanaskova Mesinkovska, N. Topical ketoconazole: A systematic review of current dermatological applications and future developments. J. Dermatol. Treat. 2019, 30, 760–771. [Google Scholar] [CrossRef]
- Bakr, E.; Abdo, H.; Abd-Elaziz, H.; Abd-Elrazek, H.; Amer, M. Adapalene gel 0.1% vs ketoconazole cream 2% and their combination in treatment of pityriasis versicolor: A randomized clinical study. Dermatol. Ther. 2020, 33, e13319. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.W.; Zhang, J.A.; Tang, Y.B.; Yu, H.X.; Li, Z.G.; Yu, J.B. A randomized controlled trial of combination treatment with ketoconazole 2% cream and adapalene 0.1% gel in pityriasis versicolor. J. Dermatol. Treat. 2015, 26, 143–146. [Google Scholar] [CrossRef]
- Birnbaum, J.E. Pharmacology of the allylamines. J. Am. Acad. Dermatol. 1990, 23, 782–785. [Google Scholar] [CrossRef] [PubMed]
- Aste, N.; Pau, M.; Pinna, A.L.; Colombo, M.D.; Biggio, P. Clinical efficacy and tolerability of terbinafine in patients with pityriasis versicolor. Mycoses 1991, 34, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Faergemann, J.; Hersle, K.; Nordin, P. Pityriasis versicolor: Clinical experience with Lamisil cream and Lamisil DermGel. Dermatology 1997, 194 (Suppl. S1), 19–21. [Google Scholar] [CrossRef]
- Vermeer, B.J.; Staats, C.C. The efficacy of a topical application of terbinafine 1% solution in subjects with pityriasis versicolor: A placebo-controlled study. Dermatology 1997, 194 (Suppl. S1), 22–24. [Google Scholar] [CrossRef] [PubMed]
- Savin, R.; Eisen, D.; Fradin, M.S.; Lebwohl, M. Tinea versicolor treated with terbinafine 1% solution. Int. J. Dermatol. 1999, 38, 863–865. [Google Scholar] [CrossRef] [PubMed]
- Chopra, V.; Jain, V.K. Comparative study of topical terbinafine and topical ketoconazole in pityriasis versicolor. Indian J. Dermatol. Venereol. Leprol. 2000, 66, 299–300. [Google Scholar]
- Abdul Bari, M.A. Comparison of superficial mycosis treatment using Butenafine and Bifonazole nitrate clinical efficacy. Glob. J. Health Sci. 2012, 5, 150–154. [Google Scholar] [CrossRef]
- Albanese, G.; Giorgetti, P.; Santagostino, L.; Di Cintio, R.; Colombo, M.D. Evaluation of the efficacy of a new antimycotic molecule for topical use: Naftifine. G. Ital. Dermatol. Venereol. 1989, 124, xxxiii–xxxvii. [Google Scholar]
- Gold, M.H.; Bridges, T.; Avakian, E.; Plaum, S.; Pappert, E.J.; Fleischer, A.B., Jr.; Hardas, B. An open-label study of naftifine hydrochloride 1% gel in the treatment of tinea versicolor. Skinmed 2011, 9, 283–286. [Google Scholar]
- Hira, S.K.; Abraham, M.S.; Mwinga, A.; Kamanga, J.; Schmidt, C. Naftifine solution (1%) in the treatment of pityriasis versicolor in Zambia. Mykosen 1986, 29, 378–381. [Google Scholar] [CrossRef]
- Sonthalia, S.; Agrawal, M.; Sehgal, V.N. Topical Ciclopirox Olamine 1%: Revisiting a Unique Antifungal. Indian Dermatol. Online J. 2019, 10, 481–485. [Google Scholar] [CrossRef]
- Gupta, M.; Sharma, V.; Chauhan, N.S. Chapter 11—Promising Novel Nanopharmaceuticals for Improving Topical Antifungal Drug Delivery. In Nano- and Microscale Drug Delivery Systems; Grumezescu, A.M., Ed.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 197–228. [Google Scholar] [CrossRef]
- del Palacio-Hernanz, A.; Guarro-Artigas, J.; Figueras-Salvat, M.J.; Esteban-Moreno, J.; Lopez-Gomez, S. Changes in fungal ultrastructure after short-course ciclopiroxolamine therapy in pityriasis versicolor. Clin. Exp. Dermatol. 1990, 15, 95–100. [Google Scholar] [CrossRef]
- Kudriavskaia, V.M.; Rudenko, A.V.; Pyrig, L.A. Drug sensitivity of Candida in patients with kidney diseases receiving immunosuppressive therapy. Antibiot. Khimioter. 1989, 34, 769–773. [Google Scholar] [PubMed]
- Gupta, A.K.; Daigle, D.; Foley, K.A. Drug safety assessment of oral formulations of ketoconazole. Expert Opin. Drug Saf. 2015, 14, 325–334. [Google Scholar] [CrossRef]
- Sayed, C. Tinea Versicolor Treatment & Management. Available online: https://emedicine.medscape.com/article/1091575-treatment (accessed on 14 September 2023).
- Sepaskhah, M.; Sadat, M.S.; Pakshir, K.; Bagheri, Z. Comparative efficacy of topical application of tacrolimus and clotrimazole in the treatment of pityriasis versicolor: A single blind, randomised clinical trial. Mycoses 2017, 60, 338–342. [Google Scholar] [CrossRef]
- Mayser, P.; Rieche, I. Rapid reversal of hyperpigmentation in pityriasis versicolor upon short-term topical cycloserine application. Mycoses 2009, 52, 541–543. [Google Scholar] [CrossRef]
- Fisher, D.; Kaplan, D.L. Common Dermatoses: How to Treat Safely and Effectively During Pregnancy. Consultant 2001, 41, 1174. [Google Scholar]
- Villars, V.V.; Jones, T.C. Special features of the clinical use of oral terbinafine in the treatment of fungal diseases. Br. J. Dermatol. 1992, 126, 61–69. [Google Scholar] [CrossRef]
- Faergemann, J.; Zehender, H.; Millerioux, L. Levels of terbinafine in plasma, stratum corneum, dermis-epidermis (without stratum corneum), sebum, hair and nails during and after 250 mg terbinafine orally once daily for 7 and 14 days. Clin. Exp. Dermatol. 1994, 19, 121–126. [Google Scholar] [CrossRef]
- Balevi, A.; Üstüner, P.; Kakşi, S.A.; Özdemir, M. Narrow-band UV-B phototherapy: An effective and reliable treatment alternative for extensive and recurrent pityriasis versicolor. J. Dermatolog. Treat. 2018, 29, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Hald, M.; Arendrup, M.C.; Svejgaard, E.L.; Lindskov, R.; Foged, E.K.; Saunte, D.M. Evidence-based Danish guidelines for the treatment of Malassezia-related skin diseases. Acta Derm.-Venereol. 2015, 95, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Faergemann, J.; Gupta, A.K.; Al Mofadi, A.; Abanami, A.; Shareaah, A.A.; Marynissen, G. Efficacy of itraconazole in the prophylactic treatment of pityriasis (tinea) versicolor. Arch. Dermatol. 2002, 138, 69–73. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Clinical Characteristics | Dermatoscopy |
|---|---|---|
| Hypopigmented Disorders | ||
| Pityriasis alba [55,56] | Flat, acquired roundish, asymptomatic hypopigmented macules with a subtle scaling, often located on the facial skin in children and adolescents. | Poorly demarcated hypopigmented areas covered with fine scales (lamellar or branny). |
| Vitiligo [51,56] | Flat, acquired and persistent, uni- or bilateral, well-demarcated hypopigmented roundish or linear macules. | Well-demarcated, non-scaly, diffuse white areas, usually accompanied with perifollicular hyperpigmentation and leukotrichia. |
| Idiopathic guttate hypomelanosis [51,56] | Flat, acquired hypo- or depigmented, variably sized roundish or polygonal macules predominantly located on sun-exposed sites and sparing the face. | Numerous well- to poorly defined hypopigmented areas characterised by various shades of white, bordering randomly distributed hyperpigmented reticular lines (cloudy sky-like pattern). |
| Leprosy (borderline or borderline tuberculoid) [56,57] | Distinct, acquired, circular, erythematous plaques with well-defined edges, forming a saucer-like shape, where the margins slope inside. | Orange-yellow or white structureless areas, with reduced number of hair units/follicular and eccrine ostia (white clods and dots, respectively). Orange clods, and vascular polymorphism (lines serpentine, clods, dots) can be present in some cases. |
| Progressive macular hypomelanosis [58] | Flat, acquired, symmetrically distributed, coalescing, non-scaly hypopigmented macules affecting the trunk and back. | Disseminated folliculocentric depigmented areas displaying subtle pigmentation of reticular lines. If present, delicate white scales are mainly restricted to skin creases. |
| Ash leaf macules in tuberous sclerosis [56,59] | Congenital, flat lanceolate depigmented macules present in tuberous sclerosis or isolated. | Poorly demarcated depigmented areas. Subtle background reticular lines are preserved. |
| Nevus depigmentosus [51,56] | Congenital, asymptomatic flat pale macules with fixed shape, typically present at birth. | Poorly defined hypopigmented area with subtle faded physiological reticular lines of background pigmentation and peripheral islands of normal-coloured skin. |
| Nevus anemicus [56,60] | Congenital, segmental flat area of depigmentation. | Poorly defined whitish area surrounded with red peripheral zone that often feature linear serpentine vessels. |
| Extragenital lichen sclerosus [51,56] | Acquired, usually asymptomatic, flat-topped papules or plaques affecting the trunk or/and extremities. | Well-delineated structureless white-yellowish areas. Active lesions feature typical yellowish follicular plugs. Diffuse white scale, polarising-dependent white structures (lines, areas, 4-dotted clods, and rainbow pattern), haemorrhages, dotted, linear serpentine and/or branching vessels can be present. |
| Hypopigmented mycosis fungoides [56,61] | Acquired, patchy hypopigmented areas. | Poorly defined hypopigmented pink-white areas deprived of physiological background pigmentation of lines reticular. |
| Hyperpigmented disorders | ||
| Confluent and reticulated papillomatosis [56,62] | Acquired, flat, asymptomatic, grey-brown scaly papules coalescing into larger patches arranged in a reticular fashion, commonly affecting the torso. | Subtle/small white scales and brownish clods separated by hypopigmented lines (cobblestone appearance, or gyri and sulci pattern). |
| Becker’s nevus [56,63] | Congenital, irregularly shaped hyperpigmented macule often accompanied by hypertrichosis, commonly affecting shoulder girdle or upper chest. | Poorly demarcated brown reticular or structureless areas and increased hair density. |
| Idiopathic eruptive macular hyperpigmentation [64,65] | Disseminated, nonconfluent, and asymptomatic pigmented macules affecting the trunk, neck, and proximal extremities, developing in childhood or adolescence without any background of inflammatory lesions or drug trigger. | Pigmented dots and clods distributed over the accentuated lines reticular (physiological pigmentation) with preservation of normally pigmented skin markings and follicular ostia. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Łabędź, N.; Navarrete-Dechent, C.; Kubisiak-Rzepczyk, H.; Bowszyc-Dmochowska, M.; Pogorzelska-Antkowiak, A.; Pietkiewicz, P. Pityriasis Versicolor—A Narrative Review on the Diagnosis and Management. Life 2023, 13, 2097. https://doi.org/10.3390/life13102097
Łabędź N, Navarrete-Dechent C, Kubisiak-Rzepczyk H, Bowszyc-Dmochowska M, Pogorzelska-Antkowiak A, Pietkiewicz P. Pityriasis Versicolor—A Narrative Review on the Diagnosis and Management. Life. 2023; 13(10):2097. https://doi.org/10.3390/life13102097
Chicago/Turabian StyleŁabędź, Nina, Cristian Navarrete-Dechent, Honorata Kubisiak-Rzepczyk, Monika Bowszyc-Dmochowska, Anna Pogorzelska-Antkowiak, and Paweł Pietkiewicz. 2023. "Pityriasis Versicolor—A Narrative Review on the Diagnosis and Management" Life 13, no. 10: 2097. https://doi.org/10.3390/life13102097
APA StyleŁabędź, N., Navarrete-Dechent, C., Kubisiak-Rzepczyk, H., Bowszyc-Dmochowska, M., Pogorzelska-Antkowiak, A., & Pietkiewicz, P. (2023). Pityriasis Versicolor—A Narrative Review on the Diagnosis and Management. Life, 13(10), 2097. https://doi.org/10.3390/life13102097