
Comparison of Resorbable and Non-Resorbable Osteosynthesis Material in Hallux Surgery: A Systematic Review

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
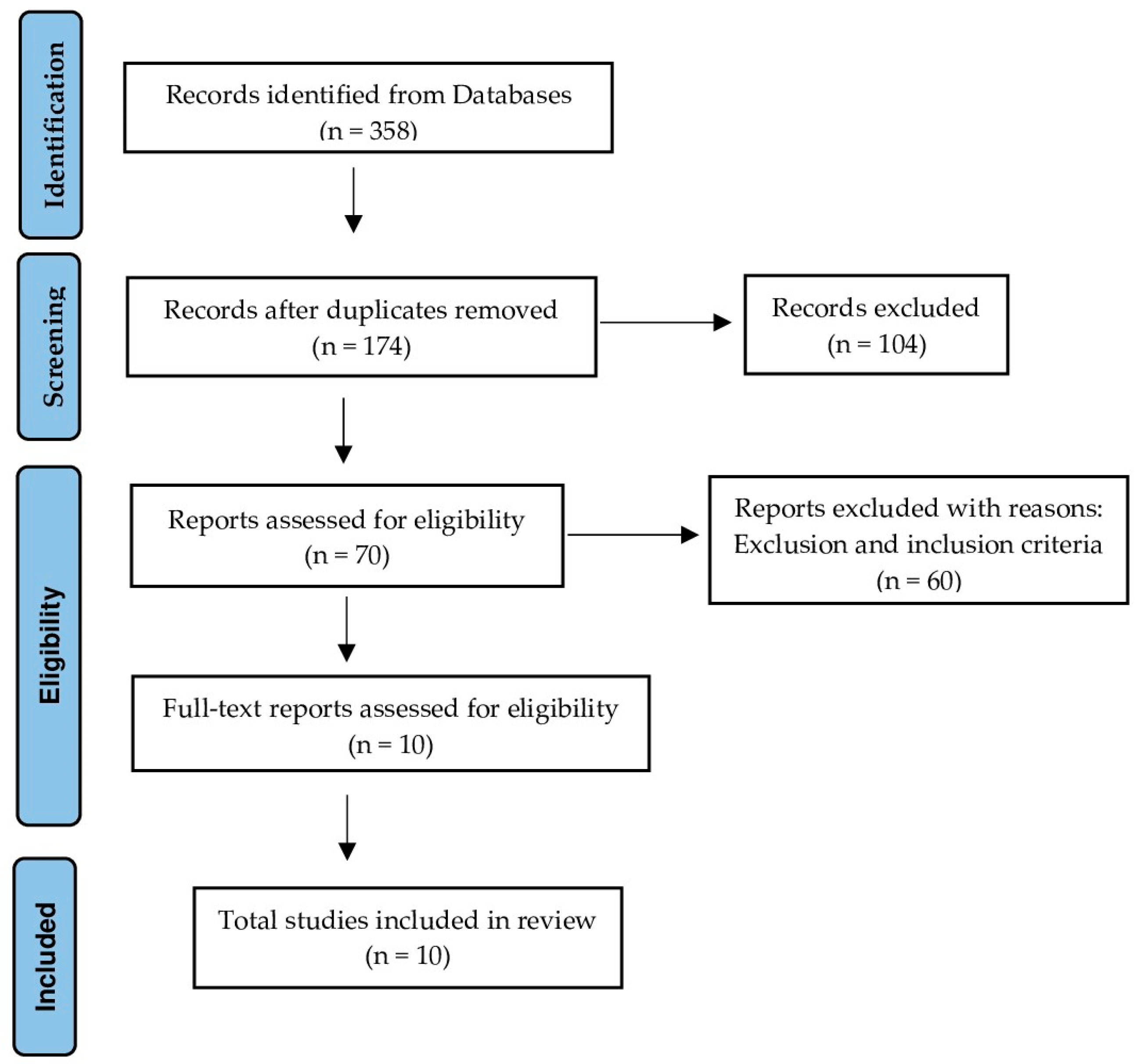
2.2. Databases and Search Strategy
2.3. Selection of Studies
2.4. Data Extraction
2.5. Quality Assessment
3. Results
3.1. Quality of Studies
3.2. Materials
3.3. Functionality
3.4. Angular Corrections
3.5. Pain
3.6. Complications
3.7. Quality of Life and Satisfaction
4. Discussion
4.1. Functionality
4.2. Angular Corrections
4.3. Pain
4.4. Complications
4.5. Quality of Life
4.6. Satisfaction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hecht, P.J.; Lin, T.J. Hallux valgus. Med. Clin. North Am. 2014, 98, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Attum, B.; Douleh, D.; Whiting, P.S.; White-Dzuro, G.A.; Dodd, A.C.; Shen, M.S.; Mir, H.R.; Obremskey, W.T.; Sethi, M.K. Outcomes of distal femur nonunions treated with a combined nail/plate construct and autogenous bone grafting. J. Orthop. Trauma 2017, 31, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Pariat, J. History of internal fixations (Part 1): Early developments with wires and plates before World War II. Int. Orthop. 2017, 41, 1273–1283. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.A.; Coughlin, M.J. Hallux valgus—Etiology, anatomy, treatment and surgical considerations. Clin. Orthop. Relat. Res. 1981, 157, 31–41. [Google Scholar] [CrossRef]
- Farraro, K.F.; Kim, K.E.; Woo, S.L.; Flowers, J.R.; McCullough, M.B. Revolutionizing orthopedic biomaterials: The potential of biodegradable and bioresorbable magnesium-based materials for functional tissue engineering. J. Biomech. 2014, 47, 1979–1986. [Google Scholar] [CrossRef] [PubMed]
- Wülker, N.; Mittag, F. The treatment of hallux valgus. Dtsch. Arztebl. Int. 2012, 109, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Izturov, B.Z.; Abilmazhinov, M.T.; Tsoi, O.G. Acquired hallux varus. etiology, pathology, classification, and treatment algorithm. Literature review. Arch. Razi Inst. 2022, 77, 2037–2048. [Google Scholar] [CrossRef]
- Donley, B.G. Acquired hallux varus. Foot Ankle Int. 1997, 18, 586–592. [Google Scholar] [CrossRef]
- Geetha, M.; Singh, A.K.; Asokamani, R.; Gogia, A.K. Ti based biomaterials, the ultimate choice for orthopaedic implants—A review. Prog. Mater. Sci. 2009, 54, 397–425. [Google Scholar] [CrossRef]
- Rangdal, S.; Singh, D.; Joshi, N.; Soni, A.; Sament, R. Functional outcome of ankle fracture patients treated with biodegradable implants. Foot Ankle Surg. 2012, 18, 153–156. [Google Scholar] [CrossRef]
- An, J.; Jia, P.; Zhang, Y.; Gong, X.; Han, X.; He, Y. Application of biodegradable plates for treating pediatric mandibular fractures. J. Craniomaxillofac. Surg. 2015, 43, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Sonnow, L.; Konneker, S.; Vogt, P.M.; Wacker, F.; VonFalck, C. Biodegradable magnesium Herbert screw—Image quality and artifacts with radiography, CT and MRI. BMC Med. Imaging 2017, 17, 16. [Google Scholar] [CrossRef] [PubMed]
- Chou, D.T.; Hong, D.; Saha, P.; Ferrero, J.; Lee, B.; Tan, Z.; Dong, Z.; Kumta, P.N. In vitro and in vivo corrosion, cytocompatibility and mechanical properties of biodegradable Mg-Y-Ca-Zr alloys as implant materials. Acta Biomater. 2013, 9, 8518–8533. [Google Scholar] [CrossRef] [PubMed]
- Pelto-Vasenius, K.; Hirvensalo, E.; Vasenius, J.; Rokkanen, P. Osteolytic changes after polyglycolide pin fixation in chevronosteotomy. Foot Ankle Int. 1997, 18, 21–25. [Google Scholar] [CrossRef]
- Hussein, M.A.; Mohammed, A.S.; Al-Aqeeli, N. Wear characteristics of metallic biomaterials: A review. Materials 2015, 8, 2749–2768. [Google Scholar] [CrossRef]
- Böstman, O.M.; Pihlajamäki, H.K. Adverse tissue reactions to bioabsorbable fixation devices. Clin. Orthop. Relat. Res. 2000, 371, 216–227. [Google Scholar] [CrossRef]
- Zhou, H.; Liang, B.; Jiang, H.; Deng, Z.; Yu, K. Magnesium-based biomaterials as emerging agents for bone repair and regeneration: From mechanism to application. J. Magnesium Alloys 2021, 9, 779–804. [Google Scholar] [CrossRef]
- Seitz, J.M.; Lucas, A.; Kirschner, M. Magnesium-based compression screws: A novelty in the clinical use of implants. JOM 2016, 68, 1177–1182. [Google Scholar] [CrossRef]
- Witte, F. The history of biodegradable magnesium implants: A review. Acta Biomater. 2010, 6, 1680–1692. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, Z.; Smith, C.; Sankar, J. Recent advances on the development of magnesium alloys for biodegradable implants. Acta Biomater. 2014, 10, 4561–4573. [Google Scholar] [CrossRef]
- Krüger, D.; Galli, S.; Zeller-Plumhoff, B.; Wieland, D.C.F.; Peruzzi, N.; Wiese, B.; Heuser, P.; Moosmann, J.; Wennerberg, A.; Willumeit-Romer, R. High-resolution ex vivo analysis of the degradation and osseointegration of Mg-xGd implant screws in 3D. Bioact. Materials 2022, 13, 37–52. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials. 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses—Ottawa Hospital Research Institute. 2009. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 June 2023).
- Giner, M.; Santana, L.; Costa, A.F.; Vázquez-Gámez, M.A.; Colmenero, M.; Olmo, F.J.; Chicardi, E.; Torres, Y.; Montoya-Garcia, M.J. Study of biocompatibility and osseointegration of new prosthetic materials. Rev. Osteoporos. Metab. Miner. 2020, 12, 92–97. [Google Scholar] [CrossRef]
- May, H.; Alper-Kati, Y.; Gumussuyu, G.; Yunus-Emre, T.; Unal, M.; Kose, O. Bioabsorbable magnesium screw versus conventional titanium screw fixation for medial malleolar fractures. J. Orthop. Traumatol. 2020, 21, 9. [Google Scholar] [CrossRef]
- Plaass, C.; VonFalck, C.; Ettinger, S.; Sonnow, L.; Calderone, F.; Weizbauer, A.; Reifenrath, J.; Claassen, L.; Waizy, H.; Daniilidis, K.; et al. Bioabsorbable magnesium versus standard titanium compression screws for fixation of distal metatarsalosteotomies—3 year results of a randomized clinical trial. J. Orthop. Sci. 2018, 23, 321–327. [Google Scholar] [CrossRef]
- Windhagen, H.; Radtke, K.; Weizbauer, A.; Diekmann, J.; Noll, Y.; Kreimeyer, U.; Schavanm, R.; Stukenborg-Colsman, C.; Waizy, H. Biodegradable magnesium-based screwclinically equivalent to titanium screw in hallux valgus surgery: Short term results of the first prospective, randomized, controlled clinical pilot study. BioMed. Eng. Online 2013, 12, 62. [Google Scholar] [CrossRef]
- Song, J.H.; Kang, C.; Park, W.H.; Lee, G.S.; Lee, J.K.; Kim, D.H.; Lee, S.W. Extended distal Chevron osteotomy and Akin osteotomy using bioabsorbable materials for treatment of moderate to severe hallux valgus. J. Foot Ankle Surg. 2021, 60, 1110–1116. [Google Scholar] [CrossRef]
- Wendelstein, J.; Holzbauer, M.; Neubauer, M.; Steiner, G.; Gruber, F.; Schneider, W. Matched retrospective analysis of three different fixation devices for chevron osteotomy. Foot 2021, 47, 101779. [Google Scholar] [CrossRef]
- Choo, J.T.; Lai, S.H.S.; Tang, C.Q.Y.; Thevendran, G. Magnesium-based bioabsorbable screw fixation for hallux valgus surgery: A suitable alternative to metallic implants. Foot Ankle Surg. 2019, 25, 727–732. [Google Scholar] [CrossRef]
- Atkinson, H.D.; Khan, S.; Lashgari, Y.; Ziegler, A. Hallux valgus correction using a modified short Scarf osteotomy with a biodegradable magnesium ortitanium compression screw—A comparative study of clinical outcomes. BMC Musculoskel Disord. 2019, 20, 334. [Google Scholar] [CrossRef] [PubMed]
- Klauser, H. Internal fixation of three-dimensional distal metatarsal I osteotomies in the treatment of hallux valgus deformities using biodegradable magnesium screws in comparison to titanium screws. Foot Ankle Surg. 2019, 25, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Komur, B.; Yilmaz, B.; Kaan, E.; Yucel, B.; Duymus, T.M.; Ozdemir, G.; Guler, O. Mid-term results of two different fixation methods for chevron osteotomy for correction of hallux valgus. Foot Ankle Surg. 2018, 57, 904–909. [Google Scholar] [CrossRef]
- Acar, B.; Kose, O.; Turan, A.; Unal, M.; Kati, Y.A.; Guler, F. Comparison of bioabsorbable magnesium versus titanium screw fixation for modified distal Chevron osteotomy in hallux valgus. BioMed. Res. Int. 2018, 1, 5242806. [Google Scholar] [CrossRef] [PubMed]
- Morandi, A.; Ungaro, E.; Fraccia, A.; Sansone, V. Chevron osteotomy of the first metatarsal stabilized with an absorbable pin: Our 5-year experience. Foot Ankle Int. 2013, 34, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Kamrani, S.; Fleck, C. Biodegradable magnesium alloys as temporary orthopedic implants: A review. Biometals 2019, 32, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Jastifer, J.R.; Gustafson, P.A.; Silva, L.F.; Noffsinger, S.; Coughlin, M.J. Nitinol, stainless steel, and titanium Kirschner wire durability. Foot Ankle Spec. 2021, 14, 317–323. [Google Scholar] [CrossRef]
- Amukarimi, S.; Mozafari, M. Biodegradable magnesium-based biomaterials: An overview of challenges and opportunities. Med. Comm. 2021, 2, 123–144. [Google Scholar] [CrossRef]

{kind=link}
| Author and Year | Type of Study | Sample Size | Middle Ages | Intervention/ Follow-up | Main Features/Results | Conclusions |
|---|---|---|---|---|---|---|
| Plaass et al. (2018) [27] | Randomized clinical trial | EG: 8 patients CG: 6 patients | EG: 56 ± 8.9 years CG: 52 ± 9.0 years | EG: Chevron + MAGNEZIX® Magnesium Screw CG: Chevron + Titanium Screw /36 months | ROM 1º AMTF: No significant difference between groups in pre vs. post-surgical results. Significant reduction in ROM in both groups at 3 years. AOFAS-MTP-IP; Pain (NRS): No significant difference between groups in pre- vs. post-surgical results. Significant improvement in both groups at 3 years. FAAM ADL; FAAM Sport; SF-36: No significant differences between groups. All patients were very satisfied with the surgery. Associated complications: Screw extraction in 1 patient of the CG. | No significant differences between groups. Magnesium screws show comparable results to titanium screws. |
| Winha-gen et al. (2013) [28] | Randomized clinical trial | EG: 13 patients CG: 13 patients | EG: 57.2 years CG: 49.9 years | GE: Chevron + MAGNEZIX® Magnesium Screw GC: Chevron + Titanium Screw /6 months | ROM 1st AMTF, AOFAS-MTP-IP; Pain (VAS): No significant difference between groups at the follow-up visit. Improvement at the end of follow-up without observing stiffness of the 1st TMA, Pain (VAS). IMA, HVA and DMAA: Decrease in angles in both groups at the end of the follow-up. 23/24 patients were very satisfied Complications: Screw extraction: 1 CG patient. Post-surgical discomfort: EG: 2 patients and CG 1 patient. Delayed consolidation: EG: 2 patients, CG: 1 patient. | No significant differences between groups. Magnesium screws show comparable results to titanium screws. Complications were considered as a result of the surgical procedure itself. |
| Song et al. (2021) [29] | Cases and controls study | EG: 33 patients CG: 28 patients | EG: 58 years (21–77) CG: 56 years (22–75) | GE: Chevron + PLA needle trim-it ® GC: Chevron + Kirschner needle /36 months | No significant difference between groups at 3 years of follow-up. MOXFQ: Significant improvement at 3-year follow-up compared to pre-surgical values in the EG. Patient satisfaction: EG: Coughlin scale: 47.6% excellent; 40.5% good; 7.1% medium; 4.8% little. Likert scale: Mean satisfaction: 3.2 (range: 1–4). IMA, HVA, HIA: In the EG, it improved significantly after 3 years of follow-up compared to pre-surgical values. Complications: EG: 7/42 (16.6%)/12/38 (31.5%) feet had complications. | Fixation with PLA needles obtained favorable clinical and radiological results with fewer complications and providing stable fixation until bone consolidation. |
| Wen-delstein et al. (2021) [30] | Cases and controls study | GE: 16 feet GC1: 16 feet GC2: 16 feet | GE: 60.6 ± 12.1 years GC1: 60.2 ± 11.5 years GC2: 59.1 ± 11.3 years | GE: Chevron + MAGNEZIX® magnesium screw GC1: Chevron + Autofix ® titanium screw GC2: Chevron + Kirschner needle /12 months | AOFAS-MTP-IP; FFI: No significant difference between the 3 groups in the post-surgical follow-up results. IMA and HVA: Significantly improved at 12-month follow-up compared to pre-surgical values in the 3 study groups. IMA: Significantly smaller post-surgical angles in the GE compared to the K-wire group. However, between the GE and the titanium screw group, there were no statistically significant results. HVA, Pain, Satisfaction: No significant difference between the 3 groups in the postoperative results at follow-up. Satisfaction: All GE patients would undergo surgery again if necessary, resulting in significantly higher satisfaction in this group. Complications: GE: Tenderness in the osteotomy area (2.13%); Implant rupture (2.13%); Dislocation of the metatarsal head (2.13%); Early radiolucency around the implant (3.19%); GC1: Deep infection (1.6%); Superficial infection (1.6%); Delayed bone healing (1.6%); Tenderness in the osteotomy area (2;13%); Early radiolucency around the implant (1.6%). GC2: Deep infection (1.6%); Bunion recurrence (1.6%); Tenderness in the osteotomy area (1.6%); 15 of 16 patients underwent elective K-wire removal. | Screws: Show results comparable to titanium screws. Patients showed a higher satisfaction rate and were significantly more likely to repeat the same procedure. The IMA was lower compared to the K-wire group, as the additional compression properties of the magnesium screw cause more stable osteosynthesis and lower intermetatarsal angles. |
| Choo et al. (2019) [31] | Cases and controls study | GE: 24 patients CG: 69 patients | GE: 54.5 ± 12.0 years GC: Non indicated | GE: Scarf + magnesium screwsMAGNEZIX ® GC: Scarf + titanium screws. /12 months. | AOFAS-MTP-IP: No significant difference between groups in post-surgical results. Significant improvement in both groups one year after surgery. Pain (VAS): Significant improvement in both groups one year after surgery. SF-36: GE: Significant improvement in all domains of the questionnaire except role limitation due to emotional problems. SF-36: GC: Significant improvement in all domains of the questionnaire. The “general health” domain was significantly better in the GE than in the GC. HVA; IMA: Significant decrease in both groups in post-surgical results compared to pre-surgical results. There is a significant difference between groups in the means of post-surgical results, being significantly better in the GC than in the GE. Complications: GE: Superficial cellulitis (12.5%) and localized post-surgical neuropathic pain (4.2%). GC: Superficial cellulite (4.3%); complex regional pain syndrome (1.4%) and implant removal due to discomfort (1.4%). | Magnesium screws show comparable results to titanium screws. There were no significant differences between groups in functional outcomes, although radiological improvements were significantly better in the GC. |
| Atkinson et al. (2019) [32] | Cases and controls study | GE: 11 patients GC: 25 patients | GE: 38 (25–51) years. GC: 41 (26–72) years. | GE: short Scarf + MAGNEZIX® magnesium screw GC: Yeshort scarf + titanium screw /12 months | MOXFQ: All scoring parameters improved significantly after surgery (GE and GC). The highest levels of improvement were with the parameters “foot pain” and “social interaction”. However, the GE had a significantly greater improvement in the parameters “walk/stand” and “index”. FAOS; EQ-5D-3L: All scoring parameters improved significantly after surgery in both groups. There were no significant differences when comparing post-surgical scores between the two groups for any of the individual scoring parameters. Complications: No intra or post-operative complications were observed in both groups. No patient in either group required surgery to remove the implant. | Screws are clinically effective and safe, showing results comparable to titanium screws. The material characteristics of magnesium screws are different from those of conventional metal screws, requiring a learning process to be able to use them correctly. |
| Klauser (2019) [33] | Cases and controls study | GE: 100 patients CG: 100 patients | GE: 50.9 years GC: 52.3 years | GE: Chevron or Youngswick -Austin + MAGNEZIX® magnesium screw GC: Chevron or Youngswick -Austin + Fixos ® titanium screw /3 months | Complications: No significant difference between groups. Delay in healing: 3 patients in GE and 4 patients in GC; Soft tissue irritation due to the implant: No patients in the GE and 1 patient in the GC; Site infection: 2 patients in GE and 1 patient in GC; Screw breakage: 1 patient in the GE and none in GC. Radiological findings: GE: Correct placement of the implants and bone healing without anomalies (60% of cases). Phenomena such as osteolysis, lytic areas, radiolucency or demineralization were found around the magnesium screw (40% of cases). GC: Correct placement of the implants and early signs of bone consolidation and healing without anomalies (100% of cases). | Magnesium screws show comparable results to titanium screws. The radiological phenomena found in patients with magnesium screws are associated with their degradation process, subsequently disappearing. |
| Komur et al. (2018) [34] | Cases and controls study | GE: 40 patients CG: 40 patients | GE: 43.1 years GC: 43.5 years | GE: Chevron + resorbable L- lactide and trimethylcarbonate OTPS® copolymer needle. GC: Chevron + titanium screw /3.5 months | AOFAS-MTP-IP: No significant difference between groups in postoperative results. The score improved significantly after surgery in both groups. Pain (VAS): No significant difference between groups in postoperative results. Significant improvement in both groups. IMA; HVA; DMAA: No significant difference between groups in postoperative results. Significant angle decrease in both groups. | Both fixation methods are safe and reliable for the surgical correction of the hallux valgus under appropriate conditions and when performed by an experienced surgeon; however, the cost of the resorbable material is higher. |
| Acar et al. (2018) [35] | Cases and controls study | GE: 16 patients GC: 15 patients | GE: 49.9 ± 15.1 years GC: 48.5 ± 14.6 years | GE: Chevron + MAGNEZIX® magnesium screw GC: Chevron + Titanium Screw /GE: 19 ± 6.8 months. GC: 16 ± 6.19 months | ROM 1º AMTF, AOFAS-MTP-IP; Pain (VAS): No significant difference between groups in the final pre- and post-surgical results. Significant decrease in ROM in both groups at the end of follow-up compared to pre-surgical values. AOFAS-MTP-IP; Pain (VAS): Significant improvement in both groups. IMA; HVA: No significant difference between groups in pre-surgical, early and final post-surgical results. Significant decrease in the angle in both groups in the final results. Complications: Implant removal rate: GE: none; GC: 1 case. Statistically similar in both groups; Mild edema and hyperemia around the surgical incision: GE: 1 case; GC: none. Statistically similar in both groups. Gas accumulation in soft tissues: GE: 13 cases; CG: none. | Similar clinical and radiological results in both groups. Magnesium screws provide the advantage of a lower implant removal rate. The radiological findings of magnesium screws are the result of their degradation process; therefore, it is necessary for surgeons and radiologists to be familiar with these images for their correct interpretation. |
| Morandi et al. (2013) [36] | Cases and controls study | GE: 251 patients GC: 132 patients | GE: 58.6 (19–74) years GC: 63.2 (26–80) years | GE: Chevron + resorbable needle composed of a copolymer of PLLA and PDLLA Osteo-Tec® GC: Chevron + Integra® Bold Titanium Screw /12 months | AOFAS-MTP-IP and HVA: No significant difference between groups in the final results. Significant improvement in both groups at the final follow-up. IMA: Significant difference between groups in the final results. Significant decrease in both groups at the final follow-up. Complications: Giant cell granuloma: 0.7% (GE); Slight loss of correction: 3.2% (EG); Dorsal edema, erythema and pain in the hallux when wearing shoes: 0.6% (GC). The screw was removed after one year without loss of correction. Satisfaction: 100% of patients declared themselves very satisfied with the procedure. | Both methods are effective, allowing important angular corrections and with a low complication rate. The only difference found between the two fixation methods was the cost, since the titanium screw is 25% cheaper than the resorbable one. The selection of the patient, the implant and the surgical technique helps to minimize complications. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coheña-Jiménez, M.; Prieto-Domínguez, R.; Pérez-Belloso, A.J.; Muriel-Sánchez, J.M.; Gómez-Carrión, Á.; Montaño-Jiménez, P. Comparison of Resorbable and Non-Resorbable Osteosynthesis Material in Hallux Surgery: A Systematic Review. Life 2023, 13, 2018. https://doi.org/10.3390/life13102018
Coheña-Jiménez M, Prieto-Domínguez R, Pérez-Belloso AJ, Muriel-Sánchez JM, Gómez-Carrión Á, Montaño-Jiménez P. Comparison of Resorbable and Non-Resorbable Osteosynthesis Material in Hallux Surgery: A Systematic Review. Life. 2023; 13(10):2018. https://doi.org/10.3390/life13102018
Chicago/Turabian StyleCoheña-Jiménez, Manuel, Raquel Prieto-Domínguez, Ana Juana Pérez-Belloso, Juan Manuel Muriel-Sánchez, Álvaro Gómez-Carrión, and Pedro Montaño-Jiménez. 2023. "Comparison of Resorbable and Non-Resorbable Osteosynthesis Material in Hallux Surgery: A Systematic Review" Life 13, no. 10: 2018. https://doi.org/10.3390/life13102018
APA StyleCoheña-Jiménez, M., Prieto-Domínguez, R., Pérez-Belloso, A. J., Muriel-Sánchez, J. M., Gómez-Carrión, Á., & Montaño-Jiménez, P. (2023). Comparison of Resorbable and Non-Resorbable Osteosynthesis Material in Hallux Surgery: A Systematic Review. Life, 13(10), 2018. https://doi.org/10.3390/life13102018