


Morphological Evaluation of the Splenic Artery, Its Anatomical Variations and Irrigation Territory


Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Covantev, S.; Uzdenov, R.; Turovets, D.; Belic, O. Spleen: An organ of multiple shapes. Iberoam. J. Med. 2021, 3, 326–331. [Google Scholar] [CrossRef]
- Coccolini, F.; Montori, G.; Catena, F.; Kluger, Y.; Biffl, W.; Moore, E.E.; Reva, V.; Bing, C.; Bala, M.; Fugazzola, P.; et al. Splenic trauma: WSES classification and guidelines for adult and pediatric patients. World J. Emerg. Surg. 2017, 12, 40. [Google Scholar] [CrossRef]
- Morgenstern, L. A history of Splenectomy. In Surgical Diseases of the Spleen; Hiatt, J.R., Phillips, E.H., Morgenstern, L., Eds.; Springer: Berlin/Heidelberg, Germany, 1997; pp. 3–14. [Google Scholar]
- El-Matbouly, M.; Jabbour, G.; El-Menyar, A.; Peralta, R.; Abdelrahman, H.; Zarour, A.; Al-Hassani, A.; Al-Thani, H. Blunt splenic trauma: Assessment, management and outcomes. Surgeon 2016, 14, 52–58. [Google Scholar] [CrossRef]
- Carlin, A.M.; Tyburski, J.G.; Wilson, R.F.; Steffes, C. Factors affecting the outcome of patients with splenic trauma. Am. Surgeon. 2002, 68, 232–239. [Google Scholar] [CrossRef]
- Kumari, M.; Parwez, M.; Jain, A.; Pandya, B. Management of a delayed, post-traumatic rupture of splenic artery pseudoaneurysm in a patient with life threatening co-morbidities: A treatment challenge. Int. J. Surg. Case Rep. 2020, 75, 479–482. [Google Scholar] [CrossRef]
- Madoff, D.C.; Denys, A.; Wallace, M.J.; Murthy, R.; Gupta, S.; Pillsbury, E.P.; Ahrar, K.; Bessoud, B.; Hicks, M.E. Splenic arterial interventions: Anatomy, indications, technical considerations, and potential complications. Radiographics 2005, 25 (Suppl. 1), S191–S211. [Google Scholar] [CrossRef]
- Guillon, R.; Garcier, J.M.; Abergel, A.; Mofid, R.; Garcia, V.; Chahid, T.; Ravel, A.; Pezet, D.; Boyer, L. Management of splenic artery aneurysms and false aneurysms with endovascular treatment in 12 patients. Cardiovasc. Interv. Radiol. 2003, 26, 256–260. [Google Scholar] [CrossRef]
- Poulin, E.C.; Thibault, C. The anatomical basis for laparoscopic splenectomy. Can. J. Surg. J. Can. Chir. 1993, 36, 484–488. [Google Scholar]
- Ekingen, A.; Hatipoğlu, E.S.; Hamidi, C.; Tuncer, M.C.; Ertuğrul, Ö. Splenic artery angiography: Clinical classification of origin and branching variations of splenic artery by multi-detector computed tomography angiography method. Folia Morphol. 2020, 79, 236–246. [Google Scholar] [CrossRef]
- Cleypool, C.G.J.; Lotgerink Bruinenberg, D.; Roeling, T.; Irwin, E.; Bleys, R. Splenic artery loops: Potential splenic plexus stimulation sites for neuroimmunomodulatory-based anti-inflammatory therapy? Clin. Anat. 2021, 34, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, D.J.; Troquay, S.; de Jonge, W.J.; Irwin, E.D.; Vervoordeldonk, M.J.; Luyer, M.D.; Nederend, J. Morphometric analysis of the splenic artery using contrast-enhanced computed tomography (CT). Surg. Radiol. Anat. 2021, 43, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, P.A.; Stewart, R.; Ellis, H. Tortuosity of the human splenic artery. Clin. Anat. 1995, 8, 214–218. [Google Scholar] [CrossRef]
- Golder, W.A. Tortuosity and calcification of the splenic artery. More than an additional finding. Der Radiol. 2008, 48, 1066–1067. [Google Scholar] [CrossRef]
- Fataftah, J.; Manasrah, Z.; Tayyem, R.; Qandeel, H.; Al-Omari, M.; Shatarat, A.; Badran, D.; Fataftah, J.; Manasrah, Z.; Tayyem, R.; et al. Splenic Artery Tortuosity Index on Abdominal CT Scan: Correlation with Age, Sex, BMI and Abdominal Cavity Diameters. Int. J. Morphol. 2020, 38, 17–22. [Google Scholar] [CrossRef]
- Michels, N.A. Blood Supply and Anatomy of the Upper Abdominal Organs; Pitman Medical Publishing Co., Ltd.: London, UK, 1995. [Google Scholar]
- Michels, N.A. The variational anatomy of the spleen and splenic artery. Am. J. Anat. 1942, 70, 21–72. [Google Scholar] [CrossRef]
- Covantev, S.; Mazuruc, N.; Belic, O. The Arterial Supply of the Distal Part of the Pancreas. Surg. Res. Pract. 2019, 2019, 5804047. [Google Scholar] [CrossRef] [PubMed]
- Covantsev, S.; Chicu, C.; Mazuruc, N.; Belic, O. Pancreatic ductal anatomy: More than meets the eye. Surg. Radiol. Anat. 2022, 44, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.H.; Xu, M.; Huang, C.M.; Li, P.; Xie, J.W.; Wang, J.B.; Lin, J.X.; Lu, J.; Chen, Q.Y.; Cao, L.L.; et al. Anatomy and influence of the splenic artery in laparoscopic spleen-preserving splenic lymphadenectomy. World J. Gastroenterol. 2015, 21, 8389–8397. [Google Scholar] [CrossRef]
- Ashok, K.R.; Kiran, T.V. Study of branching pattern of splenic artery. Int. J. Anat. Res. 2016, 4, 2073–2075. [Google Scholar]
- Krishna, M.; Oraon, S.; Thakur, N. Study of Anatomical Variation of The Segmental Branches of Splenic Artery in The Population of Jharkhand. J. Dent. Med. Sci. 2017, 16, 34–41. [Google Scholar]
- Gangadhara, R.P.; Hemasankar, C. Study on origin, course, branching pattern and morphometry of splenic artery and its branches supplying. Int. J. Curr. Res. Rev. 2014, 6, 16. [Google Scholar]
- Pandey, S.K.; Bhattacharya, S.; Mishra, R.N.; Shukla, V.K. Anatomical variations of the splenic artery and its clinical implications. Clin. Anat. 2004, 17, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Kong, S.H.; Kim, T.H.; Park, S.H.; Ang, R.R.G.; Diana, M.; Soler, L.; Suh, Y.S.; Lee, H.J.; Marescaux, J.; et al. The anatomical configuration of the splenic artery influences suprapancreatic lymph node dissection in laparoscopic gastrectomy: Analysis using a 3D volume rendering program. Surg. Endosc. 2018, 32, 3697–3705. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Aoki, T.; Murakami, M.; Fujimori, A.; Koizumi, T.; Kusano, T.; Matsuda, K.; Nogaki, K.; Hakozaki, T.; Shibata, H.; et al. Individualized procedures for splenic artery dissection during laparoscopic distal pancreatectomy. BMC Surg. 2020, 20, 32. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.L.; Li, S.L.; Wang, Y.; Shi, B.J.; Li, M.; Li, Y.C.; Zhong, Z.Y.; Li, Z.D. Laparoscopic splenectomy: Color Doppler flow imaging for preoperative evaluation. Chin. Med. J. 2009, 122, 1203–1208. [Google Scholar] [PubMed]
- Sundar, G.; Sangeetha, V. Variation in branching pattern of splenic artery and its surgical importance. Indian J. Clin. Anat. Physiol. 2020, 7, 301–303. [Google Scholar]
- Silva, L.F.; Silveira, L.M.; Timbó, P.S.; Pinheiro, S.R.; Barros, L.V.; da Silva Filho, A.R. Morfometric study of arterial branching of the spleen compared to radiological study. Rev. Col. Bras. Cir. 2011, 38, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Daisy Sahni, A.; Indar Jit, B.; Gupta, C.N.M.; Gupta, D.M.; Harjeet, E. Branches of the splenic artery and splenic arterial segments. Clin. Anat. 2003, 16, 371–377. [Google Scholar] [CrossRef]
- Shashikala Londhe, R. Study of vascular pattern in human spleen by corrosion cast method. Al Ameen J. Med. Sci. 2013, 6, 167–169. [Google Scholar]
- Liu, D.L.; Xia, S.; Xu, W.; Ye, Q.; Gao, Y.; Qian, J. Anatomy of vasculature of 850 spleen specimens and its application in partial splenectomy. Surgery 1996, 119, 27–33. [Google Scholar] [CrossRef]
- García-Porrero, J.A.; Lemes, A. Arterial segmentation and subsegmentation in the human spleen. Acta Anat. 1988, 131, 276–283. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SP | IP | RP | AP | Total | |
|---|---|---|---|---|---|
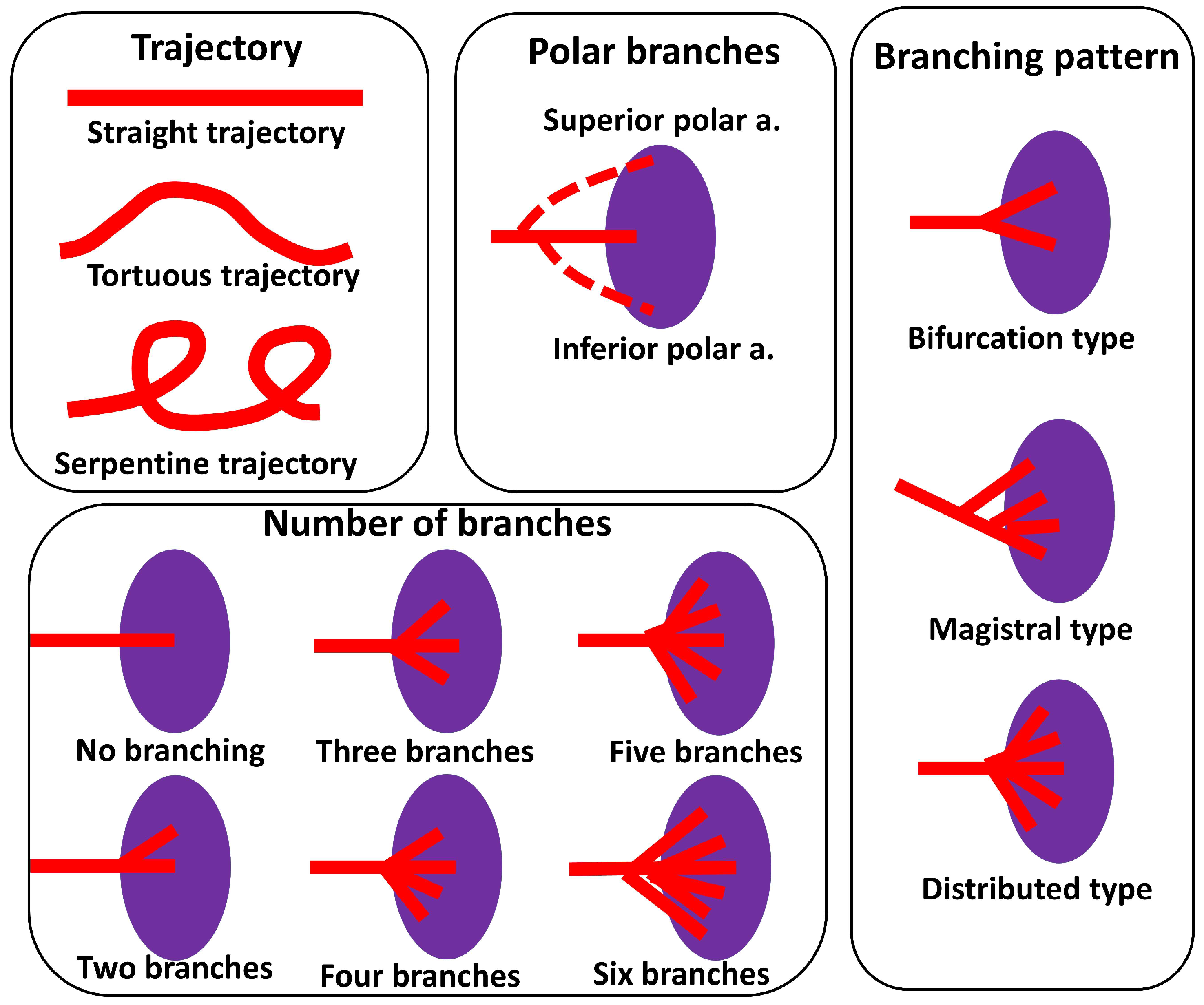
| Straight, n (%) | 109 (33.03) | 15 (4.55) | 16 (4.85) | 2 (0.61) | 142 (43.03) |
| Sinuous, n (%) | 56 (16.97) | 15 (4.55) | 9 (2.73) | 11 (3.33) | 91 (27.58) |
| Serpentine, n (%) | 45 (13.64) | 17 (5.15) | 7 (2.12) | 0 (0.00) | 69 (20.91) |
| Alternating, n (%) | 22 (6.67) | 2 (0.61) | 1 (0.30) | 3 (0.91) | 28 (8.48) |
| Total, n (%) | 232 (70.30) | 49 (14.85) | 33 (10.00) | 16 (4.85) | 330 (100) |
| Number of Branches | n (%) |
|---|---|
| No branching | 11 (3.33) |
| Two branches | 273 (82.73) |
| Three branches | 32 (9.70) |
| Four branches | 10 (3.03) |
| Five branches | 2 (0.61) |
| Six branches | 2 (0.61) |
| Total | 330 (100%) |
| Author, Year | Number of Specimens | SP | IP | RP | AP | References |
|---|---|---|---|---|---|---|
| Pandey et al., 2004 | 320 | 74.1% | 4.6% | 8.2% | 18.5 | [24] |
| Gangadhara et al., 2014 | 30 | 63.3% | - | 36.3% | - | [23] |
| Ashok et al., 2016 | 76 | 68% | - | 32% | - | [21] |
| Meet Krishna, 2017 | 317 | 99.3% | 6.66% | - | - | [22] |
| Zhu et al., 2018 | 169 | 36.7% | 14.2% | 49.1 | [25] | |
| Current study | 330 | 70.3% | 14.85% | 10% | 4.55% | |
| Author, Year | Number of Specimens | No Branching | Magistral Type | Distributed Type | References |
|---|---|---|---|---|---|
| Pandey et al., 2004 | 320 | 2.8% | 97.2 | [24] | |
| Xu et al., 2009 | 48 | - | 60.9 | 39.1 | [27] |
| Zheng et al., 2015 | 317 | - | 64.7 | 35.3 | [20] |
| Ashok et al., 2016 | 76 | 10.5 | 55.3 | 34.2 | [21] |
| Sangeetha, & Sundar, 2020 | 60 | 16.7 | 60 | 23.3 | [28] |
| Current study | 330 | 3.33 | 20 | 36.06 | |
| Author, Year | Number of Specimens, n | Number of Splenic Artery Branches, % | Polar Arteries, % | References | |||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | More than 3 | Superior | Inferior | Both | |||
| Liu et al., 1996 | 850 | 0.8 | 86 | 12.2 | 1 | ** 31.3 | ** 38.8 | ** 13.3 | [32] |
| Daisy Sahni et al., 2003 | 200 | - | 80 (M) 79.5 (F) | 20 (M) 19,5(F) | - | 53 | 33 | - | [30] |
| Pandey, 2004 | 320 | 2.8% | 63.1 | - | 4–18.8 6–9.7 >6–5.6 | - | [24] | ||
| Silva et al., 2011 | 60 + 30 * | - | 93.34 90 * | 6.66 10 * | - | 16% and 20% respectively | [29] | ||
| Shashikala Londhe, 2013 | 50 | 90 | 10 | - | 33 | 54 | 24.4 | [31] | |
| Gangadhara et al., 2014 | 30 | - | 80 | 16.6 | - | 26.6 | 36.6 | 16.6 | [23] |
| Zheng et al., 2015 | 317 | 6.9 | 78.9 | 13.6 | 0.6 | 16.4 | 5.05 | - | [20] |
| Meet Krishna, 2017 | 317 | - | 100 | - | - | 6.66 | - | 6.66 | [22] |
| Current study | 330 | 3.33 | 82.73 | 9.70 | 4.25 | 60.27 | 19.69 | 4.85 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Covantsev, S.; Alieva, F.; Mulaeva, K.; Mazuruc, N.; Belic, O. Morphological Evaluation of the Splenic Artery, Its Anatomical Variations and Irrigation Territory. Life 2023, 13, 195. https://doi.org/10.3390/life13010195
Covantsev S, Alieva F, Mulaeva K, Mazuruc N, Belic O. Morphological Evaluation of the Splenic Artery, Its Anatomical Variations and Irrigation Territory. Life. 2023; 13(1):195. https://doi.org/10.3390/life13010195
Chicago/Turabian StyleCovantsev, Serghei, Fariza Alieva, Karina Mulaeva, Natalia Mazuruc, and Olga Belic. 2023. "Morphological Evaluation of the Splenic Artery, Its Anatomical Variations and Irrigation Territory" Life 13, no. 1: 195. https://doi.org/10.3390/life13010195
APA StyleCovantsev, S., Alieva, F., Mulaeva, K., Mazuruc, N., & Belic, O. (2023). Morphological Evaluation of the Splenic Artery, Its Anatomical Variations and Irrigation Territory. Life, 13(1), 195. https://doi.org/10.3390/life13010195