
Maternal Obesity as a Risk Factor for Caesarean Delivery in Sub-Saharan Africa: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis
3. Results
3.1. Literature Search
3.2. Study Characteristics
3.2.1. Study Setting
3.2.2. Study Design
3.3. Population
3.4. Types of Exposure
3.5. Outcome Measure
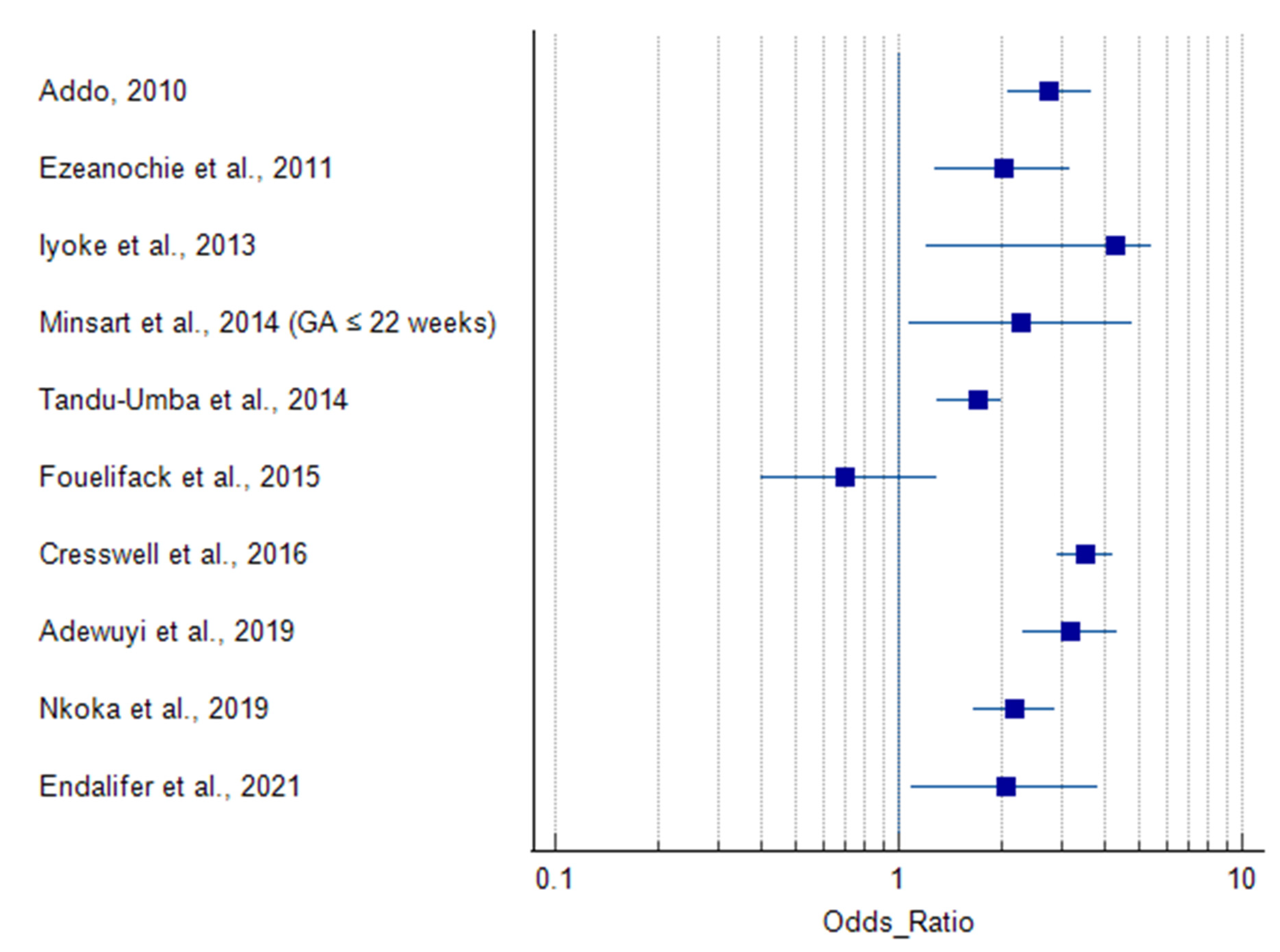
3.6. Association of Maternal Obesity and Caesarean Delivery
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, R.S.M.; Woo, J. Prevention of overweight and obesity: How effective is the current public health approach. Int. J. Environ. Res. Public Health 2010, 7, 765–783. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Amabebe, E.; Robert, F.O.; Agbalalah, T.; Orubu, E.S.F. Microbial dysbiosis-induced obesity: Role of gut microbiota in homoeostasis of energy metabolism. Br. J. Nutr. 2020, 123, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; WHO Technical Report Series; WHO: Geneva, Switzerland, 2000; Volume 894, pp. i–xii, 1–253. [Google Scholar]
- Popkin, B.M. Part II. What is unique about the experience in lower-and middle-income less-industrialised countries compared with the very-highincome industrialised countries?: The shift in stages of the nutrition transition in the developing world differes from past experiences! Public Health Nutr. 2002, 5, 205–214. [Google Scholar] [CrossRef]
- Fezeu, L.; Minkoulou, E.; Balkau, B.; Kengne, A.P.; Awah, P.; Unwin, N.; Alberti, G.K.; Mbanya, J.C. Association between socioeconomic status and adiposity in urban Cameroon. Int. J. Epidemiol. 2006, 35, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Sodjinou, R.; Agueh, V.; Fayomi, B.; Delisle, H. Obesity and cardio-metabolic risk factors in urban adults of Benin: Relationship with socio-economic status, urbanisation, and lifestyle patterns. BMC Public Health 2008, 8, 84. [Google Scholar] [CrossRef]
- Davis, E.M.; Zyzanski, S.J.; Olson, C.M.; Stange, K.C.; Horwitz, R.I. Racial, ethnic, and socioeconomic differences in the incidence of obesity related to childbirth. Am. J. Public Health 2009, 99, 294–299. [Google Scholar] [CrossRef]
- Kleinman, K.P.; Oken, E.; Radesky, J.S.; Rich-Edwards, J.W.; Peterson, K.E.; Gillman, M.W. How should gestational weight gain be assessed? A comparison of existing methods and a novel method, area under the weight gain curve. Int. J. Epidemiol. 2007, 36, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Minsart, A.F.; N’Guyen, T.-S.; Dimtsu, H.; Ratsimanresy, R.; Dada, F.; Ali Hadji, R. Maternal obesity and rate of cesarean delivery in Djibouti. Int. J. Gynaecol. Obstet. 2014, 127, 167–170. [Google Scholar] [CrossRef]
- Onubi, O.J.; Marais, D.; Aucott, L.; Okonofua, F.; Poobalan, A.S. Maternal obesity in Africa: A systematic review and meta-analysis. J. Public Health 2016, 38, e218–e231. [Google Scholar] [CrossRef] [PubMed]
- Madlala, H.P.; Steyn, N.P.; Kalk, E.; Davies, M.-A.; Nyemba, D.; Malaba, T.R.; Mehta, U.; Petro, G.; Boulle, A.; Myer, L. Association between food intake and obesity in pregnant women living with and without HIV in Cape Town, South Africa: A prospective cohort study. BMC Public Health 2021, 21, 1504. [Google Scholar] [CrossRef]
- Rooney, B.L.; Schauberger, C.W. Excess pregnancy weight gain and long-term obesity: One decade later. Obstet. Gynecol. 2002, 100, 245–252. [Google Scholar] [CrossRef]
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalán, C.; Uauy, R.; Herring, S.; Gillman, M.W. Preconceptional and maternal obesity: Epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016, 4, 1025–1036. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D.O. Diabetogenically beneficial gut microbiota alterations in third trimester of pregnancy. Reprod. Fertil. 2021, 2, R1–R12. [Google Scholar] [CrossRef]
- Thangaratinam, S.; Rogozińska, E.; Jolly, K.; Glinkowski, S.; Duda, W.; Borowiack, E.; Roseboom, T.; Tomlinson, J.; Walczak, J.; Kunz, R.; et al. Interventions to reduce or prevent obesity in pregnant women: A systematic review. Health Technol. Assess. 2012, 16, iii–iv, 1–191. [Google Scholar] [CrossRef]
- Ozodiegwu, I.D.; Mamudu, H.M.; Wang, L.; Wallace, R.; Quinn, M.; Liu, Y.; Doctor, H.V. Country-Level Analysis of the Association between Maternal Obesity and Neonatal Mortality in 34 Sub-Saharan African Countries. Ann. Glob. Health 2019, 85, 139. [Google Scholar] [CrossRef]
- Nurul-Farehah, S.; Rohana, A.J. Maternal obesity and its determinants: A neglected issue? Malays. Fam. Physician 2020, 15, 34–42. [Google Scholar]
- Leddy, M.A.; Power, M.L.; Schulkin, J. The impact of maternal obesity on maternal and fetal health. Rev. Obstet. Gynecol. 2008, 1, 170–178. [Google Scholar]
- Neal, K.; Ullah, S.; Glastras, S.J. Obesity Class Impacts Adverse Maternal and Neonatal Outcomes Independent of Diabetes. Front. Endocrinol. 2022, 13, 832678. [Google Scholar] [CrossRef] [PubMed]
- Ma, R.C.W.; Schmidt, M.I.; Tam, W.H.; McIntyre, H.D.; Catalano, P.M. Clinical management of pregnancy in the obese mother: Before conception, during pregnancy, and post partum. Lancet Diabetes Endocrinol. 2016, 4, 1037–1049. [Google Scholar] [CrossRef]
- Poston, L.; Harthoorn, L.F.; van der Beek, E.M.; On Behalf of Contributors to The ILSI Europe Workshop. Obesity in Pregnancy: Implications for the Mother and Lifelong Health of the Child. A Consensus Statement. Pediatr. Res. 2011, 69, 175–180. [Google Scholar] [CrossRef]
- Alfadhli, E.M. Maternal obesity influences birth weight more than gestational diabetes. BMC Pregnancy Childbirth 2021, 21, 111. [Google Scholar] [CrossRef]
- Grieger, J.A.; Hutchesson, M.J.; Cooray, S.D.; Bahri Khomami, M.; Zaman, S.; Segan, L.; Teede, H.; Moran, L.J. A review of maternal overweight and obesity and its impact on cardiometabolic outcomes during pregnancy and postpartum. Ther. Adv. Reprod. Health 2021, 15, 2633494120986544. [Google Scholar] [CrossRef]
- Betran, A.; Torloni, M.; Zhang, J.; Gülmezoglu, A.; WHO Working Group on Caesarean Section. WHO Statement on Caesarean Section Rates. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 667–670. [Google Scholar] [CrossRef]
- Sebire, N.J.; Jolly, M.; Harris, J.P.; Wadsworth, J.; Joffe, M.; Beard, R.W.; Regan, L.; Robinson, S. Maternal obesity and pregnancy outcome: A study of 287,213 pregnancies in London. Int. J. Obes. 2001, 25, 1175–1182. [Google Scholar] [CrossRef]
- Damodaran, S.; Swaminathan, K. 6—Obesity and Contraception. In Obesity; Mahmood, T., Arulkumaran, S., Eds.; Elsevier: Oxford, UK, 2013; pp. 69–89. [Google Scholar]
- Shrestha, A.; Prowak, M.; Berlandi-Short, V.-M.; Garay, J.; Ramalingam, L. Maternal Obesity: A Focus on Maternal Interventions to Improve Health of Offspring. Front. Cardiovasc. Med. 2021, 8, 674. [Google Scholar] [CrossRef]
- Poobalan, A.S.; Aucott, L.S.; Gurung, T.; Smith, W.C.; Bhattacharya, S. Obesity as an independent risk factor for elective and emergency caesarean delivery in nulliparous women--systematic review and meta-analysis of cohort studies. Obes. Rev. 2009, 10, 28–35. [Google Scholar] [CrossRef]
- Chu, S.Y.; Kim, S.Y.; Schmid, C.H.; Dietz, P.M.; Callaghan, W.M.; Lau, J.; Curtis, K.M. Maternal obesity and risk of cesarean delivery: A meta-analysis. Obes. Rev. 2007, 8, 385–394. [Google Scholar] [CrossRef]
- Olayemi, O.O.; Umuerri, C.O.; Aimakhu, C.O. Obstetric Performance of Nigerian Obese Parturients. Trop. J. Obstet. Gynaecol. 2002, 19, 17–20. [Google Scholar] [CrossRef]
- Puotege, S.k.; Seidu, M.; Kangkpi, L.; Yussif, A.R.M.; Yakong, V.N.; Mumuni, A.N. Maternal body mass index, gestational weight gain and birth outcome among puerperal women in the Tamale metropolis of Ghana. Afr. J. Midwifery Women’s Health 2020, 14, 1–13. [Google Scholar] [CrossRef]
- Akinola, O.I.; Fabamwo, A.O.; Tayo, A.O.; Rabiu, K.A.; Oshodi, Y.A.; Alokha, M.E. Caesarean section—An appraisal of some predictive factors in Lagos Nigeria. BMC Pregnancy Childbirth 2014, 14, 217. [Google Scholar] [CrossRef]
- Edomwonyi, N.P.; Osaigbovo, P.E. Incidence of obesity in parturients scheduled for caesarean section, intra-operative complications, management and outcome. East Afr. Med. J. 2006, 83, 112–119. [Google Scholar] [CrossRef]
- Efiong, E.I. Pregnancy in the overweight Nigerian. Br. J. Obstet. Gynaecol. 1975, 82, 903–906. [Google Scholar] [CrossRef]
- Moraes, A.N.; Likwa, R.N.; Nzala, S.H. A retrospective analysis of adverse obstetric and perinatal outcomes in adolescent pregnancy: The case of Luapula Province, Zambia. Matern. Health Neonatol. Perinatol. 2018, 4, 20. [Google Scholar] [CrossRef]
- Mpotora, J.C.; Yahaya, J.J.; Ngw’eshemi, S.K.; Mwampagatwa, I.H. Rationale of indications for caesarean delivery and associated factors among primigravidae in Tanzania. J. Taibah Univ. Med. Sci. 2021, 16, 350–358. [Google Scholar] [CrossRef]
- Cresswell, J.A.; Campbell, O.M.; De Silva, M.J.; Slaymaker, E.; Filippi, V. Maternal obesity and Caesarean delivery in sub-Saharan Africa. Trop. Med. Int. Health 2016, 21, 879–885. [Google Scholar] [CrossRef]
- Adesina, K.; Aderibigbe, S.; Fawole, A.; Ijaiya, M.; Olarinoye, A. Pregnancy outcome of the obese in Ilorin. Obstet. Med. 2011, 4, 160–163. [Google Scholar] [CrossRef]
- Ezeanochie, M.C.; Ande, A.B.; Olagbuji, B.N. Maternal obesity in early pregnancy and subsequent pregnancy outcome in a Nigerian population. Afr. J. Reprod. Health 2011, 15, 55–59. [Google Scholar]
- Israel, J.; Solomon, N.; Chris, A.; Nwadiuto, A. Pregnancy outcome among obese paturients at the University of Port Harcourt Teaching Hospital, Nigeria. J. Med. Med. Sci. 2011, 2, 1152–1156. [Google Scholar]
- Ugwuja, E.I.; Akubugwo, E.I.; Obidoa, O.; Ibiam, A.U. Maternal BMI during Pregnancy: Effect on trace elements Status and Pregnancy Outcomes. Int. J. Health Res. 2011, 3, 71–78. [Google Scholar] [CrossRef]
- Iyoke, C.A.; Ugwu, G.O.; Ezugwu, F.O.; Lawani, O.L.; Onyebuchi, A.K. Retrospective cohort study of the effects of obesity in early pregnancy on maternal weight gain and obstetric outcomes in an obstetric population in Africa. Int. J. Womens Health 2013, 5, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Adewuyi, E.O.; Auta, A.; Khanal, V.; Tapshak, S.J.; Zhao, Y. Cesarean delivery in Nigeria: Prevalence and associated factors―A population-based cross-sectional study. BMJ Open 2019, 9, e027273. [Google Scholar] [CrossRef]
- Ngoga, E.; Hall, D.; Mattheyse, F.; Grové, D. Outcome of pregnancy in the morbidly obese woman. SA Fam. Pract. 2009, 51, 39–41. [Google Scholar] [CrossRef]
- Basu, J.K.; Jeketera, C.M.; Basu, D. Obesity and its outcomes among pregnant South African women. Int. J. Gynaecol. Obstet. 2010, 110, 101–104. [Google Scholar] [CrossRef]
- Davies, H.; Visser, J.; Tomlinson, M.; Rotheram-Borus, M.; Gissane, C.; Harwood, J.; LeRoux, I. An investigation into utilising gestational body mass index as a screening tool for adverse birth outcomes and maternal morbidities in a group of pregnant women in Khayelitsha. S. Afr. J. Clin. Nutr. 2013, 26, 116–122. [Google Scholar] [CrossRef][Green Version]
- Mwanamsangu, A.H.; Mahande, M.J.; Mazuguni, F.S.; Bishanga, D.R.; Mazuguni, N.; Msuya, S.E.; Mosha, D. Maternal obesity and intrapartum obstetric complications among pregnant women: Retrospective cohort analysis from medical birth registry in Northern Tanzania. Obes. Sci. Pract. 2020, 6, 171–180. [Google Scholar] [CrossRef]
- Fouelifack, F.Y.; Fouedjio, J.H.; Fouogue, J.T.; Sando, Z.; Fouelifa, L.D.; Mbu, R.E. Associations of body mass index and gestational weight gain with term pregnancy outcomes in urban Cameroon: A retrospective cohort study in a tertiary hospital. BMC Res. Notes 2015, 8, 806. [Google Scholar] [CrossRef]
- Tandu-Umba, B.; Mbangama, M.A.; Kamongola, K.M.B.; Kamgang Tchawou, A.G.; Kivuidi, M.P.; Kasonga Munene, S.; Kambashi Meke, I.; Kapuku Kabasele, O.; Kondoli, B.J.; Kikuni, K.R.; et al. Pre-pregnancy high-risk factors at first antenatal visit: How predictive are these of pregnancy outcomes? Int. J. Womens Health 2014, 6, 1011–1018. [Google Scholar] [CrossRef]
- Addo, V.N. Body Mass Index, Weight Gain during Pregnancy and Obstetric Outcomes. Ghana Med. J. 2010, 44, 64–69. [Google Scholar] [CrossRef]
- Endalifer, M.L.; Diress, G.; Almaw, H.; Endalifer, B.L. Effect of overweight/obesity on caesarean section occurrence among reproductive-aged women in Ethiopia: A secondary data analysis. BMJ Nutr. Prev. Health 2021, 4, 111–114. [Google Scholar] [CrossRef]
- Nkoka, O.; Ntenda, P.A.M.; Senghore, T.; Bass, P. Maternal overweight and obesity and the risk of caesarean birth in Malawi. Reprod. Health 2019, 16, 40. [Google Scholar] [CrossRef] [PubMed]
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Modder, J.; Fitzsimons, K. CMACE/RCOG Joint Guideline: Management of Women with Obesity in Pregnancy; Centre for Maternal and Child Enquiries; Royal College of Obstetricians and Gynaecologists: London, UK, 2010. [Google Scholar]
- Davies, G.A.; Maxwell, C.; McLeod, L.; Gagnon, R.; Basso, M.; Bos, H.; Delisle, M.F.; Farine, D.; Hudon, L.; Menticoglou, S.; et al. SOGC Clinical Practice Guidelines: Obesity in pregnancy. No. 239, February 2010. Int. J. Gynaecol. Obstet. 2010, 110, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Slack, E.; Brandon, H.; Heslehurst, N. Chapter 13—Obesity and Pregnancy. In Practical Guide to Obesity Medicine; Weaver, J.U., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 143–151. [Google Scholar]



{kind=link}
{kind=link}
| MEDLINE via Web of Science searched on 20 May 2020; updated on 25 April 2022 |
|---|
|
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Pregnant women (mean/median age ≥ 18 years) living in sub-Saharan African countries | Adult women with specific disease conditions such as HIV infection, COVID-19, uterine haemorrhage, mastitis, uterine abnormality and infectious pregnancy complications, infant new-born diseases and multiple gestation |
| Exposure | BMI ≥ 30 kg/m2 | Interventions to increase maternal weight, episiotomy, symphysiotomy, spinal anaesthesia, and hysterectomy |
| Comparator | BMI < 30 kg/m2 (normal weight or a combination of overweight and normal weight participants) | Studies that did not measure BMI |
| Outcomes | Delivery of a live neonate by caesarean section. | Studies that did not report caesarean delivery as an outcome |
| Study type | Observational studies such as case-control studies, cross-sectional studies, and cohort studies | Randomised controlled trials, studies on evaluation of health care, non-English language studies |
| Study | Country | Study Design | Population | BMI, kg/m2 Categories | Gestational Age |
|---|---|---|---|---|---|
| Ngoga et al., 2009 [45] | South Africa | Case-control | 309 | Morbidly obese (≥40) | Antenatal booking |
| Addo, 2010 [51] | Ghana | Retrospective cohort | 1755 | Overweight + Obese (≥25.1) * | First trimester |
| Basu et al., 2010 [46] | South Africa | Retrospective cross-sectional | 767 | Obese (30–39.9); Morbidly obese (≥40) | Antenatal booking |
| Adesina et al., 2011 [39] | Nigeria | Case-control | 236 | Obese (≥30) | ≤32 weeks |
| Ezeanochie et al., 2011 [40] | Nigeria | Case-control | 402 | Obese (≥30) | First trimester |
| Israel et al., 2011 [41] | Nigeria | Prospective cohort | 300 | Obese (≥30) | Antenatal booking |
| Ugwuja et al., 2011 [42] | Nigeria | Prospective cohort | 349 | Obese (30–34.9); Morbidly obese (>35.0) | ≤25 weeks |
| Davies et al., 2013 [47] | South Africa | RCT sub-study | 1058 | Obese (≥29) | Antenatal booking |
| Iyoke et al., 2013 [43] | Nigeria | Retrospective cohort | 648 | Obese (≥30) | First trimester |
| Minsart et al., 2014 [10] | Djibouti | Prospective cohort | 497 | Obese Class I: (30.0–34.9) Obese Class II: (≥35) | ≤14 weeks ≤22 weeks At delivery |
| Tandu-Umba et al., 2014 [50] | Democratic Republic of Congo | Cross-sectional | 2086 | Overweight + Obese (≥28) * | Booking |
| Fouelifack et al., 2015 [49] | Cameroon | Retrospective cohort | 462 | Obese (≥30) | Pre-pregnancy |
| Cresswell et al., 2016 [38] | 31 sub- Saharan African countries † | Pooled cross-sectional | 153,102 | Obese Class I: (30.0–34.9) Obese Class II: (35–39.9)Obese Class III: (≥40) | Up to 5 years post delivery |
| Adewuyi et al., 2019 [44] | Nigeria | Cross-sectional | 31,171 | Obese (≥30) | Up to 5 years post delivery |
| Nkoka et al., 2019 [53] | Malawi | Cross-sectional | 15,732 | Obese (≥30) | Up to 5 years post delivery |
| Mwanamsangu et al., 2020 [48] | Tanzania | Retrospective cohort | 11,873 | Obese (≥30) | First antenatal care visit |
| Endalifer et al., 2021 [52] | Ethiopia | Cross-sectional | 6928 | Overweight + Obese (≥25) * | Up to 5 years post delivery |
| Study | Sample Size (n) | Obesity Prevalence (%) | Maternal Obesity Exposure (BMI, kg/m2) | Caesarean Delivery Outcomes OR/RR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Ngoga et al., 2009 [45] | 309 | NA | Morbidly obese (≥40) | - | <0.001 |
| Addo, 2010 [51] | 1755 | 17.9 (314/1755) | Overweight + Obese (≥25.1) | OR: 2.74 (2.07, 3.64) | <0.01 |
| Basu et al., 2010 [46] | 767 | 44 (337/767) | Obese (30–39.9) Morbidly obese (≥40) | - | 0.15 |
| Adesina et al., 2011 [39] | 236 | NA | Obese (≥30) | - | 0.00 |
| Ezeanochie et al., 2011 [40] | 402 | 9.6 a (201/2086) | Obese (≥30) | OR: 2.01 (1.27, 3.18) | 0.003 |
| Israel et al., 2011 [41] | 300 | 7.4 b (357/4832) | Obese (≥30) | - | <0.001 |
| Ugwuja et al., 2011 [42] | 349 | 17.2 (60/349) 5.4 (19/349) | Obese (30–34.9) Morbidly obese (>35.0) | - | Not significant <0.05 |
| Davies et al., 2013 [47] | 1058 | 33.1 (350/1058) | Obese (≥29) | - | <0.001 |
| Iyoke et al., 2013 [43] | 648 | 17.9 c (340/1806) | Obese (≥30) | OR: 4.3 (1.2, 5.44) | <0.001 |
| Minsart et al., 2014 [10] | 497 | 25.2 d (112/445) | Obese (≥30) | GA ≤ 22 weeks: aOR: 2.27 (1.07, 4.82) | 0.0321 |
| Tandu-Umba et al., 2014 [50] | 2086 | 21.9 (456/2086) | Overweight + Obese (≥28) | OR: 1.7 (1.3, 2.0) | <0.05 |
| Fouelifack et al., 2015 [49] | 462 | 14 (65/462) | Obese (≥30) | aOR: 0.7 (0.4, 1.3) | NS |
| Cresswell et al., 2016 [38] | 153,102 | 3.9 (5970/153,102) 1.0 (1531/153,102) 0.4 (612/153,102) | Obese Class I: (30.0–34.9) Obese Class II: (35–39.9) Obese Class III: (≥40) | aOR: 3.50 (2.89, 4.24) aOR: 3.76 (2.71, 5.22) aOR: 5.90 (3.82, 9.11) | 0.001 |
| Adewuyi et al., 2019 [44] | 31,171 | 8 (2469/31,171) | Obese (≥30) | aOR: 3.16 (2.30, 4.32) | <0.001 |
| Nkoka et al., 2019 [53] | 15,732 | 4.1 (643/15,732) | Obese (≥30) | aOR: 2.16 (1.65, 2.84) | <0.0001 |
| Mwanamsangu et al., 2020 [48] | 11,873 | 12.3 (1464/11,873) | Obese (≥30) | Elective CS: RR = 2.4 (1.88, 3.6) Emergency CS: RR = 1.53 (1.34, 1.75) | <0.001 |
| Endalifer et al., 2021 [52] | 6928 | 10 (692/6928) | Overweight + Obese (≥25) | aOR: 2.05 (1.09, 3.83) | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brizan, J.B.; Amabebe, E. Maternal Obesity as a Risk Factor for Caesarean Delivery in Sub-Saharan Africa: A Systematic Review. Life 2022, 12, 906. https://doi.org/10.3390/life12060906
Brizan JB, Amabebe E. Maternal Obesity as a Risk Factor for Caesarean Delivery in Sub-Saharan Africa: A Systematic Review. Life. 2022; 12(6):906. https://doi.org/10.3390/life12060906
Chicago/Turabian StyleBrizan, Jessica B., and Emmanuel Amabebe. 2022. "Maternal Obesity as a Risk Factor for Caesarean Delivery in Sub-Saharan Africa: A Systematic Review" Life 12, no. 6: 906. https://doi.org/10.3390/life12060906
APA StyleBrizan, J. B., & Amabebe, E. (2022). Maternal Obesity as a Risk Factor for Caesarean Delivery in Sub-Saharan Africa: A Systematic Review. Life, 12(6), 906. https://doi.org/10.3390/life12060906