
Evaluation of Surgical Cleavage Plane by Preoperative Magnetic Resonance Imaging Findings in Adult Intracranial Meningiomas


 ,
,  ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Operational Definition
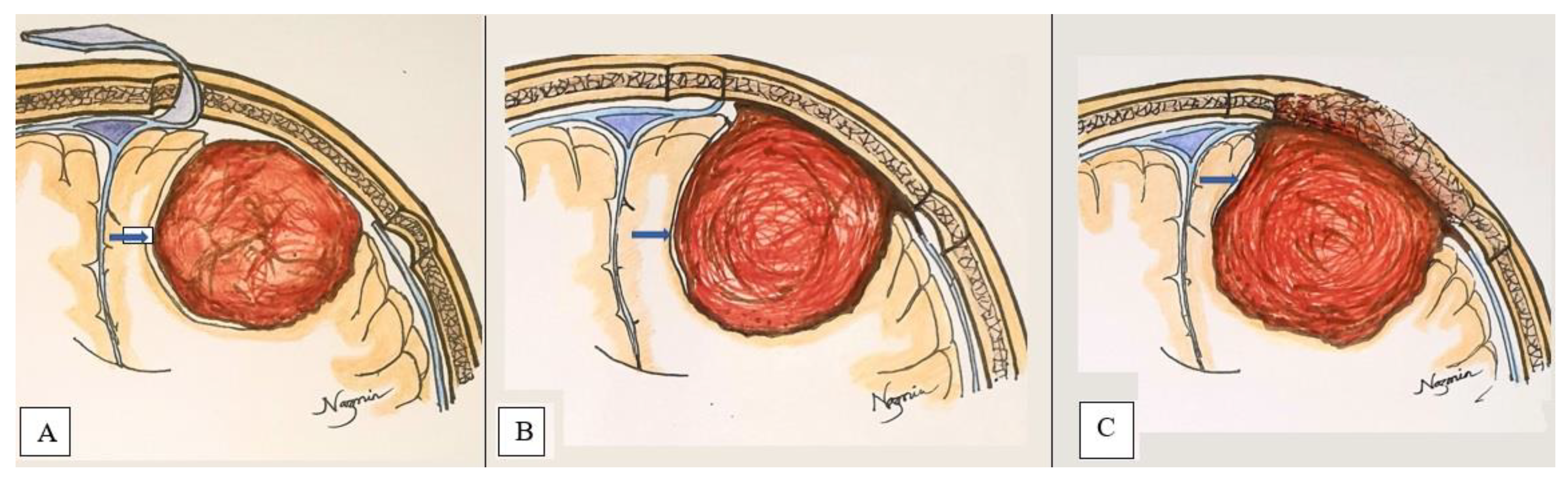
2.2. Characterization of Surgical Cleavage Plane
- Extrapial: Surgical cleavage plane lies outside the pia mater in more than two-thirds of the overall interface between tumor and cortex, regardless of whether an arachnoid membrane could be clearly identified (Figure 4A);
- Mixed: Cleavage plane lies outside the pia mater in more than one-third but less than two-thirds of overall interface (Figure 4B);
- Subpial: Tumor capsule exceeds the pia mater in more than two-thirds of the tumor cortex interface, and the surgeon was required to pass underneath the pia mater because of its incorporation into the tumor capsule (Figure 4C).
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Cioffi, G.; Gittleman, H.; Patil, N.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2012–2016. Neuro Oncol. 2019, 21, V1–V100. [Google Scholar] [CrossRef] [PubMed]
- Alexiou, G.A.; Gogou, P.; Markoula, S.; Kyritsis, A.P. Management of meningiomas. Clin. Neurol. Neurosurg. 2010, 112, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Watts, J.; Box, G.; Galvin, A.; Brotchie, P.; Trost, N.; Sutherland, T. Magnetic resonance imaging of meningiomas: A pictorial review. Insights Imaging 2014, 5, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Rezaei, S.; Faeghi, F.; Samadian, M.; Shekarchi, B. Preoperative evaluation of tumor adhesion to adjacent brain tissue in patients with meningioma with BSMI method and its comparison with the width of edema around tumor. Asian Pac. J Cancer Prev. 2018, 19, 2007–2012. [Google Scholar] [CrossRef] [PubMed]
- Hale, A.T.; Wang, L.; Strother, M.K.; Chambless, L.B. Differentiating meningioma grade by imaging features on magnetic resonance imaging. J. Clin. Neurosci. 2018, 48, 71–75. [Google Scholar] [CrossRef]
- Yang, S.Y.; Park, C.K.; Park, S.H.; Kim, D.G.; Chung, Y.S.; Jung, H.W. Atypical and anaplastic meningiomas: Prognostic implications of clinicopathological features. J. Neurol. Neurosurg Psychiatry 2008, 79, 574–580. [Google Scholar] [CrossRef]
- Güdük, M.; Ekşi, M.Ş.; Bozkurt, B.; Usseli, M.İ.; Danyeli, A.E.; Pamir, M.N. Treatment and follow-up results of WHO grade II meningiomas. J. Clin. Neurosci. 2021, 91, 354–364. [Google Scholar] [CrossRef]
- Güdük, M.; Ekşi, M.Ş.; Bozkurt, B.; Usseli, M.İ.; Danyeli, A.E.; Pamir, M.N. Neurosurgical follow-up and treatment of a series of 26 WHO grade III meningiomas. J. Clin. Neurosci. 2021, 91, 219–225. [Google Scholar] [CrossRef]
- Taoka, T.; Yamada, S.; Yamatani, Y.; Akashi, T.; Miyasaka, T.; Emura, T.; Nakase, H.; Kichikawa, K. Brain surface motion imaging to predict adhesions between meningiomas and the brain surface. Neuroradiology 2010, 52, 1003–1010. [Google Scholar] [CrossRef]
- Kayaselçuk, F.; Zorludemir, S.; Bal, N.; Erdogan, B.; Erdogan, S.; Erman, T. The expression of survivin and Ki-67 in meningiomas: Correlation with grade and clinical outcome. J. Neurooncol. 2004, 67, 209–214. [Google Scholar] [CrossRef]
- Yin, Z.; Hughes, J.D.; Glaser, K.J.; Manduca, A.; Van Gompel, J.; Link, M.J.; Romano, A.; Ehman, R.L.; Huston, J. Slip interface imaging based on MR-elastography preoperatively predicts meningioma–brain adhesion. J. Magn. Reason. Imaging 2017, 46, 1007–1016. [Google Scholar] [CrossRef] [Green Version]
- Tsermoulas, G.; Turel, M.K.; Wilcox, J.T.; Shultz, D.; Farb, R.; Zadeh, G.; Bernstein, M. Management of multiple meningiomas. J. Neurosurg. 2017, 128, 1403–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatoe, H.S.; Singh, P.; Dutta, V. Intraventricular meningiomas: A clinicopathological study and review of the literature. Neurosurg. Focus 2006, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Klinger, D.R.; Flores, B.C.; Lewis, J.J.; Barnett, S.L. The treatment of cavernous sinus meningiomas: Evolution of a modern approach. Neurosurg. Focus 2013, 35, E8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otani, N.; Mori, K.; Wada, K.; Tomiyama, A.; Toyooka, T.; Takeuchi, S. Multistaged, multidirectional strategy for safe removal of large meningiomas in the pineal region. Neurosurg. Focus 2018, 44, E13. [Google Scholar] [CrossRef]
- Mahmood, A.; Caccamo, D.V.; Tomecek, F.J.; Malik, G.M. Atypical and malignant meningiomas: A clinicopathological review. Neurosurgery 1993, 33, 955–963. [Google Scholar] [CrossRef]
- Paulino, A.C.; Ahmed, I.M.; Mai, W.Y.; Teh, B.S. The influence of pretreatment characteristics and radiotherapy parameters on time interval to development of radiation-associated meningioma. Int. J. Radiat. Oncol. Biol. Physics. 2009, 75, 1408–1414. [Google Scholar] [CrossRef]
- Thenier-Villa, J.L.; Alejandro Galárraga Campoverde, R.; Ramón De La Lama Zaragoza, A.; Conde Alonso, C. Predictors of morbidity and cleavage plane in surgical resection of pure convexity meningiomas using cerebrospinal fluid sensitive image subtraction magnetic resonance imaging. Neurol. Med. Chir. 2017, 57, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Moradi, A.; Semnani, V.; Djam, H.; Tajodini, A.; Zali, A.; Ghaemi, K.; Nikzad, N.; Madani-Civi, M. Pathodiagnostic parameters for meningioma grading. J. Clin. Neurosci. 2008, 15, 1370–1375. [Google Scholar] [CrossRef]
- Buerki, R.A.; Horbinski, C.M.; Kruser, T.; Horowitz, P.M.; James, C.D.; Lukas, R.V. An overview of meningiomas. Future Oncol. 2018, 14, 2161–2177. [Google Scholar] [CrossRef]
- Alvernia, J.E.; Sindou, M.P. Preoperative neuroimaging findings as a predictor of the surgical plane of cleavage: Prospective study of 100 consecutive cases of intracranial meningioma. J. Neurosurg. 2004, 100, 422–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.W.; Kim, M.S.; Kim, S.W.; Chang, C.H.; Kim, O.L. Peritumoral brain edema in meningiomas: Correlation of radiologic and pathologic features. J. Korean Neurosurg. Soc. 2011, 49, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Salimi-Sotoodeh, M.; Saffarian, A.; Taghipour, M.; Dehghanian, A.-R.; Chenari, N.; Ghaderi, A.; Razmkhah, M. Correlation of Peritumoral Edema and Microvessel Density with Tissue Expression of VEGF, Semaphorins 3A and 3C in Patients with Meningioma. Asian Pac. J. Cancer Biol. 2019, 3, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Takeguchi, T.; Miki, H.; Shimizu, T.; Kikuchi, K.; Mochizuki, T.; Ohue, S.; Ohnishi, T. Evaluation of the tumor-brain interface of intracranial meningiomas on MR imaging including FLAIR images. Magn. Reason. Med. Sci. 2003, 2, 165–169. [Google Scholar] [CrossRef] [Green Version]
- Celikoglu, E.; Suslu, H.T.; Hazneci, J.; Bozbuga, M. The relation between surgical cleavage and preoperative neuroradiological findings in intracranial meningiomas. Eur. J. Radiol. 2011, 80, e109–e115. [Google Scholar] [CrossRef]
- Salpietro, F.M.; Alafaci, C.; Tomasello, F.; Ildan, F.; Tuna, M.; Gocer, A.I. Meningioma cleavage. J. Neurosurg. 2000, 93, 159–160. [Google Scholar] [CrossRef]
- Jessurun, C.A.C.; Hulsbergen, A.F.C.; Cho, L.D.; Aglio, L.S.; Nandoe Tewarie, R.D.S.; Broekman, M.L.D. Evidence-based dexamethasone dosing in malignant brain tumors: What do we really know? J. Neurooncol. 2019, 144, 249–264. [Google Scholar] [CrossRef] [Green Version]
- Bebawy, J.F. Perioperative steroids for peritumoral intracranial edema: A review of mechanisms, efficacy, and side effects. J. Neurosurg. Anesthesiol. 2012, 24, 173–177. [Google Scholar] [CrossRef]
- Sun, S.Q.; Cai, C.; Ravindra, V.M.; Gamble, P.; Yarbrough, C.K.; Dacey, R.G.; Dowling, J.L.; Zipfel, G.J.; Wright, N.M.; Santiago, P.; et al. Simpson grade I-III resection of spinal atypical (world health organization grade II) meningiomas is associated with symptom resolution and low recurrence. Neurosurgery 2015, 76, 739–746. [Google Scholar] [CrossRef]
- Pavelin, S.; Becic, K.; Forempoher, G.; Mrklic, I.; Pogorelić, Z.; Titlic, M.; Andelinović, Š. Expression of Ki-67 and p53 in meningiomas. Neoplasma 2013, 60, 480–485. [Google Scholar] [CrossRef] [Green Version]
- Umana, G.E.; Scalia, G.; Vats, A.; Pompili, G.; Barone, F.; Passanisi, M.; Graziano, F.; Maugeri, R.; Tranchina, M.G.; Cosentino, S.; et al. Primary Extracranial Meningiomas of the Head and Neck. Life 2021, 11, 942. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.; Chaurasia, B.K.; Shalike, N.; Uddin, A.N.; Chowdhury, D.; Khan, A.H.; Ansari, A.; Barua, K.K.; Majumder, M.R. Surgical management of clinoidal meningiomas: 10 cases analysis. Neuroimmunol. Neuroinflammation 2018, 24, 5. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Category | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Age | ≤30 | 10 | 20.8 |
| 31–40 | 13 | 27.1 | |
| 41–50 | 10 | 20.8 | |
| 51–60 | 12 | 25.0 | |
| >60 | 3 | 6.3 | |
| Gender | Male | 31 | 64.6 |
| Female | 17 | 35.4 | |
| Location of meningioma | Convexity | 14 | 29.16 |
| Sphenoid wing | 11 | 22.91 | |
| Parasagittal | 10 | 20.83 | |
| Falcine | 7 | 14.58 | |
| Others | 6 | 12.5 | |
| Tumor size | Small | 5 | 10.4 |
| Medium | 33 | 68.8 | |
| Large | 10 | 20.8 | |
| Tumor intensity | Hyperintense | 36 | 75.0 |
| Iso- to hypointense | 9 | 18.8 | |
| Mixed | 3 | 6.3 | |
| Peritumoral edema | Focal edema | 16 | 33.3 |
| Lobar or hemispheric edema | 16 | 33.3 | |
| No edema | 16 | 33.3 | |
| Simpson’s grading | Grade 0 | 3 | 6.2% |
| Grade I | 15 | 31.5 | |
| Grade II | 30 | 62.5 | |
| Histopathological findings | Meningioma, WHO—I | 47 | 97.9 |
| Meningioma, WHO—II | 1 | 2.1 |
| Variables | Category | Surgical Plane of Cleavage | p Value | ||
|---|---|---|---|---|---|
| Extrapial (%) | Mixed (%) | Subpial (%) | |||
| Tumor size | Small | 4 (80.0) | 1 (20.0) | 0 (0.0) | 0.055 |
| Medium | 17 (81.8) | 3 (9.1) | 3 (9.1) | ||
| Large | 5 (50.0) | 5 (50.0) | 0 (0.0) | ||
| Intensity of tumor parenchyma | Hyperintense | 28 (77.8) | 6 (16.7) | 2 (5.6) | 0.881 |
| Iso- to hypointense | 6 (66.7) | 2 (22.2) | 1 (11.1) | ||
| Mixed | 2 (66.7) | 1 (33.3) | 0 (0.0) | ||
| Peritumoral edema | No edema | 12 (75.0) | 3 (18.8) | 1 (6.3) | 0.934 |
| Focal | 13 (81.3) | 2 (12.5) | 1 (6.3) | ||
| Lobar or hemispheric | 11 (68.8) | 4 (25.0) | 1 (6.3) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, N.; Ferini, G.; Hossain, M.A.T.M.; Barua, K.K.; Hossain, M.N.; Umana, G.E.; Shlobin, N.A.; Scalia, G.; Palmisciano, P.; Tomasi, O.S.; et al. Evaluation of Surgical Cleavage Plane by Preoperative Magnetic Resonance Imaging Findings in Adult Intracranial Meningiomas. Life 2022, 12, 473. https://doi.org/10.3390/life12040473
Ahmed N, Ferini G, Hossain MATM, Barua KK, Hossain MN, Umana GE, Shlobin NA, Scalia G, Palmisciano P, Tomasi OS, et al. Evaluation of Surgical Cleavage Plane by Preoperative Magnetic Resonance Imaging Findings in Adult Intracranial Meningiomas. Life. 2022; 12(4):473. https://doi.org/10.3390/life12040473
Chicago/Turabian StyleAhmed, Nazmin, Gianluca Ferini, Mosharef A. T. M. Hossain, Kanak Kanti Barua, Mohammad Nazrul Hossain, Giuseppe Emmanuele Umana, Nathan A. Shlobin, Gianluca Scalia, Paolo Palmisciano, Ottavio S. Tomasi, and et al. 2022. "Evaluation of Surgical Cleavage Plane by Preoperative Magnetic Resonance Imaging Findings in Adult Intracranial Meningiomas" Life 12, no. 4: 473. https://doi.org/10.3390/life12040473
APA StyleAhmed, N., Ferini, G., Hossain, M. A. T. M., Barua, K. K., Hossain, M. N., Umana, G. E., Shlobin, N. A., Scalia, G., Palmisciano, P., Tomasi, O. S., & Chaurasia, B. (2022). Evaluation of Surgical Cleavage Plane by Preoperative Magnetic Resonance Imaging Findings in Adult Intracranial Meningiomas. Life, 12(4), 473. https://doi.org/10.3390/life12040473