
Mediating Effect of Self-Cognitive Oral Health Status on the Effect of Obstructive Sleep Apnea Risk Factors on Quality of Life (HINT-8) in Middle-Aged Korean Women: The Korea National Health and Nutrition Examination Survey


Abstract
1. Introduction
2. Materials and Methods
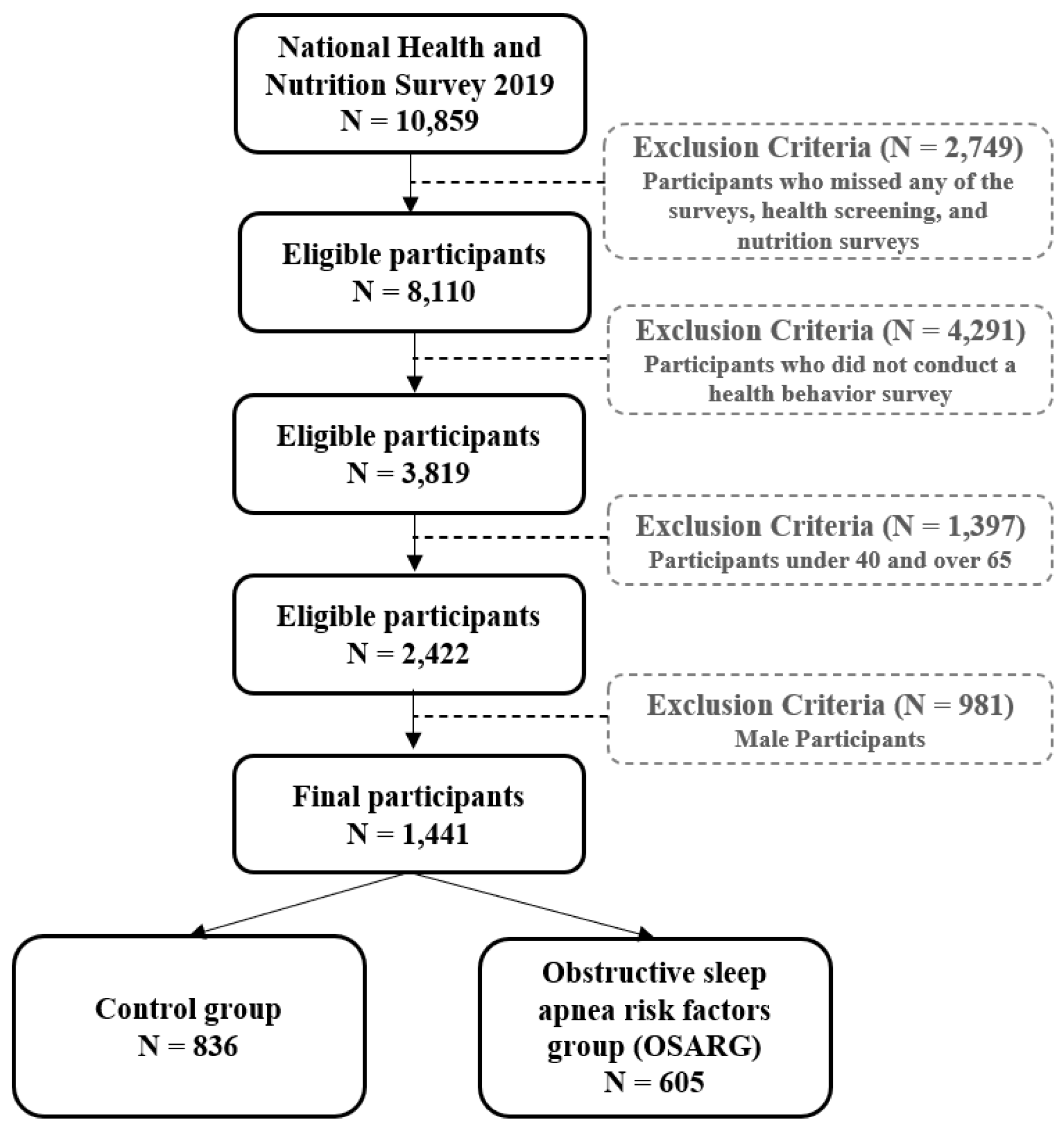
2.1. Participants and Data Collection
2.2. Tools
2.2.1. Covariance
Sociodemographic Characteristics
Systemic Health Status
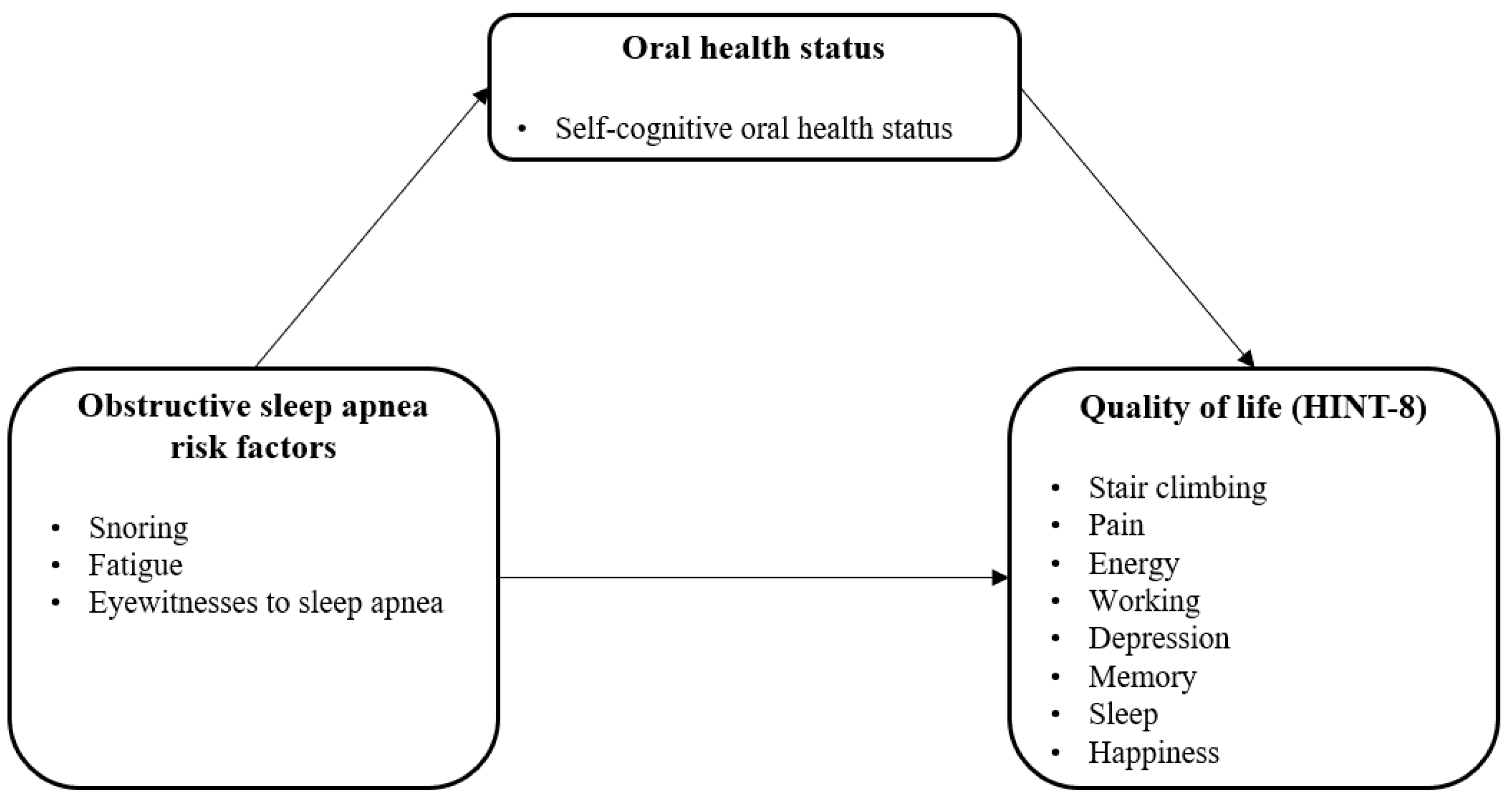
2.2.2. Self-Cognitive Oral Health Status
2.2.3. HINT-8
2.2.4. OSA Risk Factors
2.3. Methodology
3. Results
3.1. Sociodemographic Characteristics
3.2. Systemic Health Status and Self-Cognitive Oral Health Status According to the Two Groups
3.3. HINT-8 According to the Two Groups
3.4. Mediating Effect of Self-Cognitive Oral Health Status on the Effect of OSA Risk Factors on HINT-8
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Pilcher, J.J.; Ginter, D.R.; Sadowsky, B. Sleep quality versus sleep quantity: Relationship between sleep and measures of health, well-being and sleepiness in college students. J. Psychosom. Res. 1997, 42, 583–596. [Google Scholar] [CrossRef]
- Eichling, P.S.; Sahni, J. Menopause-related sleep disorders. J. Clin. Sleep Med. 2005, 1, 291–300. [Google Scholar] [CrossRef]
- Owens, J.F.; Matthews, K.A. Sleep disturbance in healthy middle-aged women. Maturitas 1998, 30, 41–50. [Google Scholar] [CrossRef]
- Takahashi, T.A.; Johnson, K.M. Menopause. Med. Clin. N. Am. 2016, 99, 521–534. [Google Scholar] [CrossRef]
- Kim, Y.H.; Ha, E.H.; Shin, S.J. A study on the menopausal symptoms and quality of life in middle aged women. J. Korean Acad. Nurs. 2003, 33, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Heinzer, R.; Marti-Soler, H.; Marques-Vidal, P.; Tobback, N.; Andries, D.; Waeber, G.; Preisig, M.; Vollenweider, P.; Haba-Rubio, J. Impact of sex and menopausal status on the prevalence, clinical presentation, and comorbidities of sleep-disordered breathing. Sleep Med. 2018, 51, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Franklin, K.A.; Lindberg, E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J. Thorac. Dis. 2015, 7, 1311–1322. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.H.; Park, S.Y.; Chang, K.S. Correlation between Clinical Characteristics and Apnea-Hypopnea Index with Obstructive Sleep Apnea Syndrome. Korean J Clin Lab Sci. 2006, 38, 212–217. [Google Scholar]
- Vorona, R.D.; Winn, M.P.; Babineau, T.W.; Eng, B.P.; Feldman, H.R.; Ware, J.C. Overweight and obese patients in a primary care population report less sleep than patients with a normal body mass index. Arch. Intern. Med. 2005, 165, 25–30. [Google Scholar] [CrossRef]
- Shaver, J.L.; Zenk, S.N. Sleep disturbance in menopause. J. Womens Health Gend. Based Med. 2000, 9, 109–118. [Google Scholar] [CrossRef]
- Rotenberg, B.W.; Vicini, C.; Pang, E.B.; Pang, K.P. Reconsidering first-line treatment for obstructive sleep apnea: A systematic review of the literature. J. Otolaryngol. Head Neck Surg. 2016, 45, 23. [Google Scholar] [CrossRef] [PubMed]
- Sher, A.E.; Schechtman, K.B.; Piccirillo, J.F. The efficacy of surgical modifications of the upper airway in adults with obstructive sleep apnea syndrome. Sleep 1996, 19, 156–177. [Google Scholar] [CrossRef] [PubMed]
- Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances. American Sleep Disorders Association. Sleep 1995, 18, 511–513. [CrossRef] [PubMed]
- Eckert, D.J.; White, D.P.; Jordan, A.S.; Malhotra, A.; Wellman, A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am. J. Respir. Crit. Care Med. 2013, 188, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, K.; Lee, R.W.W.; Chan, T.O.; Ng, S.; Hui, D.S.; Cistulli, P.A. Craniofacial phenotyping in Chinese and Caucasian patients with sleep apnea: Influence of ethnicity and sex. J. Clin. Sleep Med. 2018, 14, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Banno, K.; Kryger, M.H. Sleep apnea: Clinical investigations in humans. Sleep Med. 2007, 8, 400–426. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. Validity and Reliability Evaluation for EQ-5D in KOREA. Available online: http://scienceon.kisti.re.kr/commons/util/originalView.do?cn=TRKO201300000474&dbt=TRKO&rn= (accessed on 1 July 2022).
- Lee, J.E.; Ahn, J.H. A study on deriving a conversion formulae using mapping between HINT-8 and EQ-5D instruments. Korean J. Health Econ. Policy 2019, 25, 77–103. [Google Scholar]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. Women’s Lives through Statistics in 2020. Available online: http://kostat.go.kr/portal/eng/pressReleases/13/1/index.board?bmode=read&bSeq=&aSeq=385880&pageNo=1&rowNum=10&navCount=10&currPg=&searchInfo=&sTarget=title&sTxt= (accessed on 1 October 2022).
- Chang, H.K. Influencing factors on health-related quality of life in middle age. Korean J. Adult Nurs. 2012, 24, 339–347. [Google Scholar] [CrossRef][Green Version]
- Nelson, H.D. Menopause. Lancet 2008, 371, 760–770. [Google Scholar] [CrossRef]
- Tkacova, R.; Dorkova, Z. Clinical presentations of OSA in adults. Eur. Respir. Monogr. 2010, 50, 86–103. [Google Scholar]
- Liu, L.; Kang, R.; Zhao, S.; Zhang, T.; Zhu, W.; Li, E.; Li, F.; Wan, S.; Zhao, Z. Sexual dysfunction in patients with obstructive sleep apnea: A systematic review and meta-analysis. J. Sex. Med. 2015, 12, 1992–2003. [Google Scholar] [CrossRef]
- Ustun, B.; Westover, M.B.; Rudin, C.; Bianchi, M.T. Clinical prediction models for sleep apnea: The importance of medical history over symptoms. J. Clin. Sleep Med. 2016, 12, 161–168. [Google Scholar] [CrossRef]
- Cunningham, J.; Hunter, M.; Budgeon, C.; Murray, K.; Knuiman, M.; Hui, J.; Hillman, D.; Singh, B.; James, A. The prevalence and comorbidities of obstructive sleep apnea in middle-aged men and women: The Busselton Healthy Ageing Study. J. Clin. Sleep Med. 2021, 17, 2029–2039. [Google Scholar] [CrossRef]
- Kim, K.S.; Kim, J.H.; Park, S.Y.; Won, H.R.; Lee, H.J.; Yang, H.S.; Kim, H.J. Smoking induces oropharyngeal narrowing and increases the severity of obstructive sleep apnea syndrome. J. Clin. Sleep Med. 2012, 8, 367–374. [Google Scholar] [CrossRef]
- Gopalakrishnan, P.; Tak, T. Obstructive sleep apnea and cardiovascular disease. Cardiol. Rev. 2011, 19, 279–290. [Google Scholar] [CrossRef]
- Tasci, I. Oxidative stress, obstructive sleep apnea and cardiovascular disease. Sleep Breath 2012, 16, 585. [Google Scholar] [CrossRef][Green Version]
- Davies, R.J.; Stradling, J.R. The relationship between neck circumference, radiographic pharyngeal anatomy, and the obstructive sleep apnea syndrome. Eur. Respir. J. 1990, 3, 509–514. [Google Scholar]
- Morgenthaler, T.I.; Kapen, S.; Lee-Chiong, T.; Alessi, C.; Boehlecke, B.; Brown, T.; Coleman, J.; Friedman, L.; Kapur, V.; Owens, J.; et al. Practice parameters for the medical therapy of obstructive sleep apnea. Sleep 2006, 29, 1031–1035. [Google Scholar]
- Wysocki, J.; Charuta, A.; Kowalcze, K.; Ptaszyńska-Sarosiek, I. Anthropometric and physiologic assessment in sleep apnea patients regarding body fat distribution. Folia Morphol. 2015, 75, 393–399. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kawaguchi, Y.; Fukumoto, S.; Inaba, M.; Koyama, H.; Shoji, T.; Shoji, S.; Nishizawa, Y. Different impacts of neck circumference and visceral obesity on the severity of obstructive sleep apnea syndrome. Obesity 2011, 19, 276–282. [Google Scholar] [CrossRef]
- Cha, J.D.; Jang, K.A. The factors of oral health impact profile of workers-industrial workers in Gyeong-Nam province. J. Korea Acad.-Ind. Coop. Soc. 2012, 13, 4604–4611. [Google Scholar] [CrossRef]
- Park, H.M. Effects of oral health behavior and status of elderly people in Korea on mental health and quality of life. Korean J. Health Serv. Manag. 2014, 8, 175–185. [Google Scholar] [CrossRef]
- Wilson, I.B.; Cleary, P.D. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA 1995, 273, 59–65. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Division | CG (N = 836) | OSARG (N = 605) | p * |
|---|---|---|---|---|
| Age | 40–49 | 331 (41.5) | 223 (39.9) | 0.564 |
| 50–59 | 345 (42.4) | 245 (41.8) | ||
| 60–64 | 160 (16.1) | 137 (18.3) | ||
| Marriage status | Single | 32 (3.1) | 20 (3.3) | 0.861 |
| Married | 804 (96.9) | 585 (96.7) | ||
| Education level | ≤Elementary school | 71 (7.5) | 74 (11.2) | 0.013 |
| Middle school | 75 (8.2) | 72 (10.1) | ||
| High school | 347 (42.5) | 253 (43.4) | ||
| ≥College | 343 (41.9) | 205 (35.3) | ||
| Income level | Low | 139 (15.7) | 130 (19.8) | 0.127 |
| Low-middle | 165 (20.3) | 114 (19.5) | ||
| Middle | 161 (18.7) | 133 (22.3) | ||
| Middle-high | 183 (22.4) | 110 (18.8) | ||
| High | 186 (22.9) | 114 (19.5) | ||
| Economic activity | Employed | 516 (62.4) | 353 (57.4) | 0.078 |
| Unemployed | 320 (37.6) | 252 (42.6) | ||
| Drinking | Not at all | 309 (53.9) | 215 (52.2) | 0.931 |
| Less than once a month | 119 (20.5) | 82 (20.6) | ||
| About once a month | 76 (14.2) | 62 (14.1) | ||
| Once a week | 51 (9.0) | 38 (10.9) | ||
| Almost everyday | 17 (2.5) | 10 (2.3) | ||
| Smoking | Non-smoking | 806 (96.1) | 563 (92.4) | 0.019 |
| Smoking | 27 (3.9) | 41 (7.6) |
| Characteristics | CG (N = 1295) | OSARG (N = 1127) | p * |
|---|---|---|---|
| * OSA (have, %) | 0 (0.0) | 2 (0.3) | 0.113 |
| * High blood pressure (have, %) | 138 (16.2) | 119 (19.9) | 0.092 |
| * Dyslipidemia (have, %) | 156 (18.4) | 136 (23.4) | 0.033 |
| * Diabetes (have, %) | 41 (4.9) | 44 (6.6) | 0.191 |
| * Cervical cancer (have, %) | 4 (0.4) | 4 (0.8) | 0.305 |
| * Depression (have, %) | 41 (4.9) | 59 (9.1) | 0.005 |
| * Allergic rhinitis (have, %) | 137 (15.9) | 117 (20.5) | 0.066 |
| * Sinusitis (have, %) | 42 (4.5) | 41 (6.5) | 0.153 |
| * Otitis media (have, %) | 41 (4.5) | 30 (5.4) | 0.451 |
| †Body mass index | 23.28 ± 0.15 | 23.84 ± 0.18 | 0.009 |
| †Neck circumference | 32.59 ± 0.10 | 32.99 ± 0.10 | <0.001 |
| †Menopause age | 50.11 ± 0.20 | 49.82 ± 0.27 | 0.385 |
| †Self-awareness of oral health status | 2.78 ± 0.03 | 2.64 ± 0.03 | 0.001 |
| Characteristics | CG (N = 1295) | OSARG (N = 1127) | p * |
|---|---|---|---|
| 1. Climbing stairs | 3.63 ± 0.02 | 3.37 ± 0.03 | <0.001 |
| 2. Pain | 3.44 ± 0.02 | 3.19 ± 0.03 | <0.001 |
| 3. Energy | 3.12 ± 0.03 | 2.65 ± 0.40 | <0.001 |
| 4. To work | 3.67 ± 0.20 | 3.37 ± 0.03 | <0.001 |
| 5. Depressed | 3.60 ± 0.02 | 3.31 ± 0.03 | <0.001 |
| 6. Memory | 3.52 ± 0.02 | 3.34 ± 0.02 | <0.001 |
| 7. Sleep | 3.52 ± 0.02 | 3.25 ± 0.03 | <0.001 |
| 8. Happiness | 2.88 ± 0.03 | 2.59 ± 0.04 | <0.001 |
| HINT-8 | 27.37 ± 0.12 | 25.07 ± 0.14 | <0.001 |
| Step | Model | β | t | p * |
|---|---|---|---|---|
| 1 | OSA risk factors → self-awareness of oral health status | −0.072 | −2.401 | 0.018 |
| 2 | OSA risk factors → HINT-8 | −1.329 | −9.268 | <0.001 |
| 3 | OSA risk factors → HINT-8 | −1.280 | −8.690 | <0.001 |
| Self-awareness of oral health status → HINT-8 | 0.713 | 5.944 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-R. Mediating Effect of Self-Cognitive Oral Health Status on the Effect of Obstructive Sleep Apnea Risk Factors on Quality of Life (HINT-8) in Middle-Aged Korean Women: The Korea National Health and Nutrition Examination Survey. Life 2022, 12, 1569. https://doi.org/10.3390/life12101569
Kim Y-R. Mediating Effect of Self-Cognitive Oral Health Status on the Effect of Obstructive Sleep Apnea Risk Factors on Quality of Life (HINT-8) in Middle-Aged Korean Women: The Korea National Health and Nutrition Examination Survey. Life. 2022; 12(10):1569. https://doi.org/10.3390/life12101569
Chicago/Turabian StyleKim, Yu-Rin. 2022. "Mediating Effect of Self-Cognitive Oral Health Status on the Effect of Obstructive Sleep Apnea Risk Factors on Quality of Life (HINT-8) in Middle-Aged Korean Women: The Korea National Health and Nutrition Examination Survey" Life 12, no. 10: 1569. https://doi.org/10.3390/life12101569
APA StyleKim, Y.-R. (2022). Mediating Effect of Self-Cognitive Oral Health Status on the Effect of Obstructive Sleep Apnea Risk Factors on Quality of Life (HINT-8) in Middle-Aged Korean Women: The Korea National Health and Nutrition Examination Survey. Life, 12(10), 1569. https://doi.org/10.3390/life12101569