
The Influence of an Acute Bout of Aerobic Exercise on Vascular Endothelial Function in Moderate Stages of Chronic Kidney Disease

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
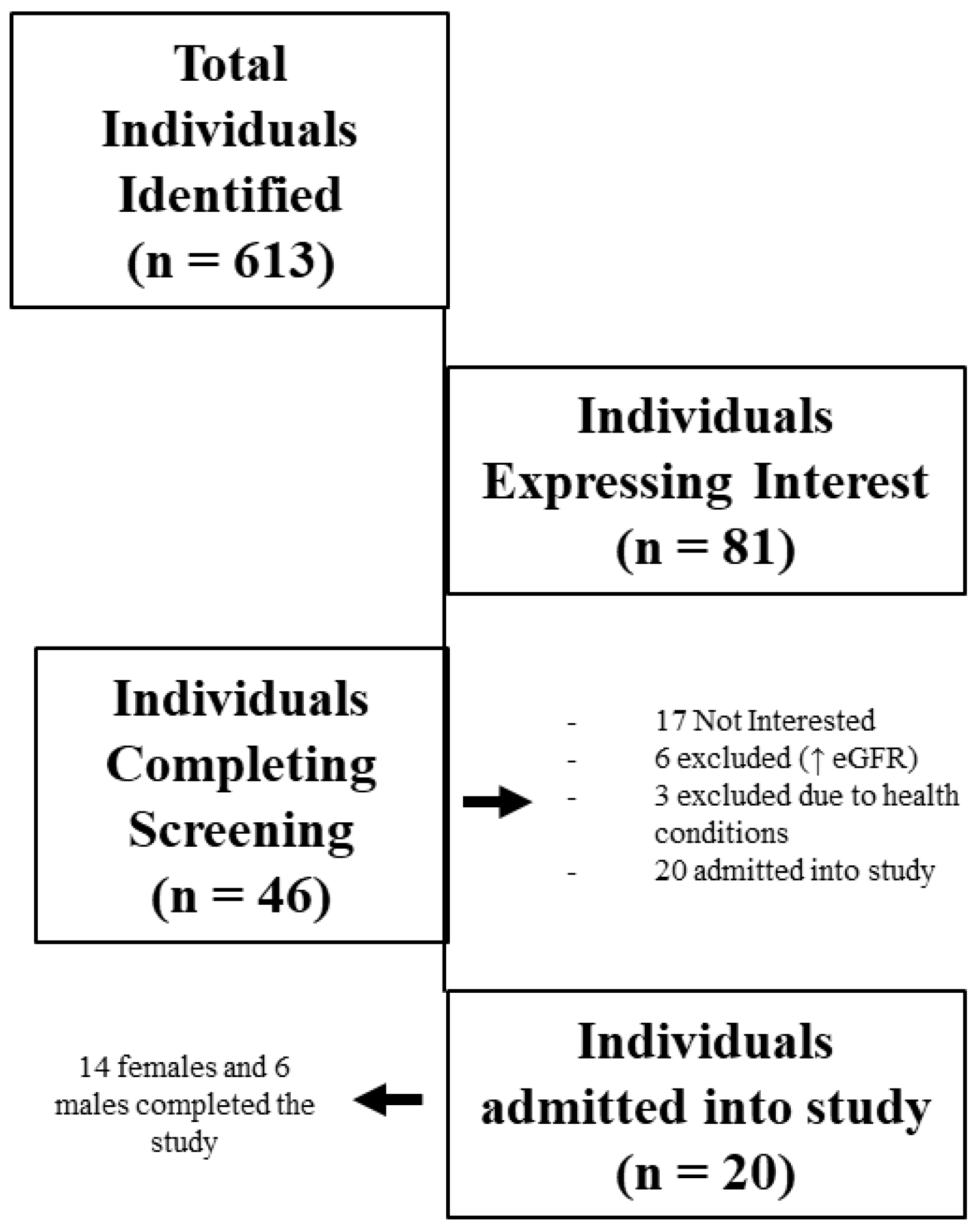
2.1. Participant Recruitment
2.2. Screening
2.3. Exercise Intervention
2.4. Brachial Artery Reactivity Measurement
2.5. Analysis of FMD Data
2.6. Blood Sampling
2.7. Biochemical Analysis
2.8. Statistics
3. Results
3.1. Baseline Physiological Characteristics
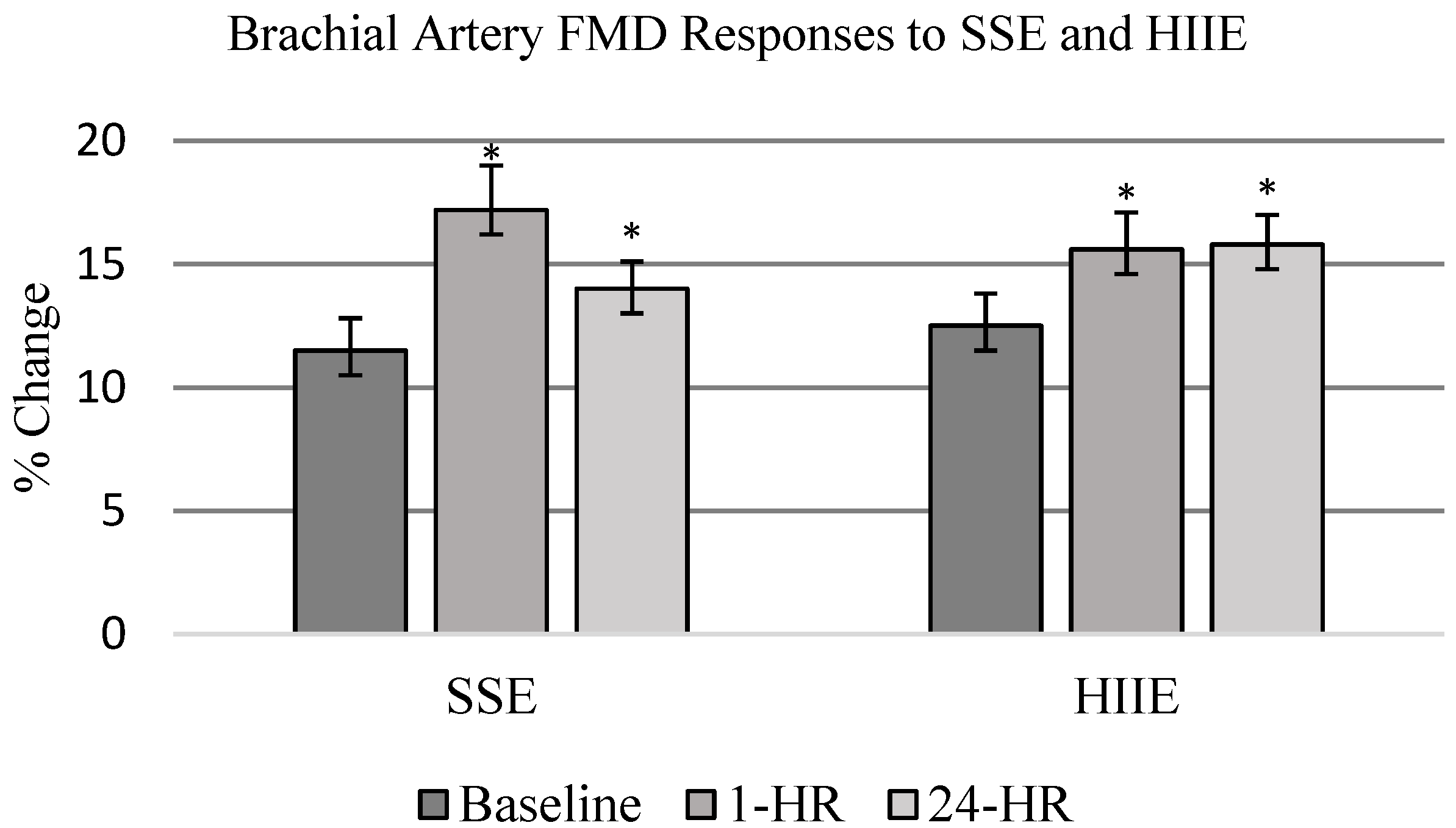
3.2. Flow-Mediated Dilation Outcomes
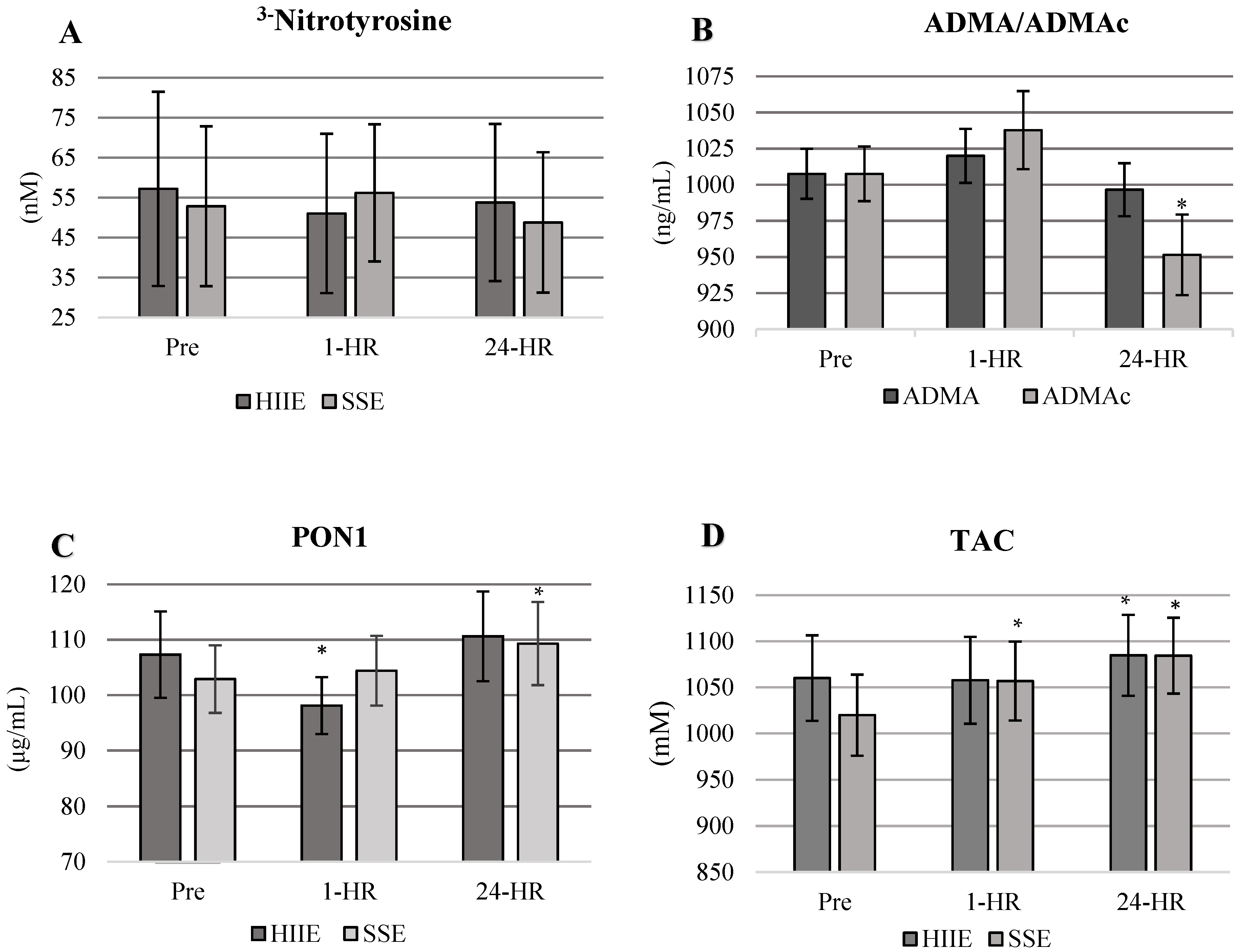
3.3. Biochemical Analysis Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gielen, S.; Sandri, M.; Erbs, S.; Adams, V. Exercise-induced modulation of endothelial nitric oxide production. Curr. Pharm. Biotechnol. 2011, 12, 1375–1384. [Google Scholar] [CrossRef]
- Green, D.J.; Maiorana, A.; O’Driscoll, G.; Taylor, R. Effect of exercise training on endothelium-derived nitric oxide function in humans. J. Physiol. 2004, 561, 1–25. [Google Scholar] [CrossRef]
- Duru, O.K.; Vargas, R.B.; Kermah, D.; Nissenson, A.R.; Norris, K.C. High Prevalence of Stage 3 Chronic Kidney Disease in Older Adults Despite Normal Serum Creatinine. J. Gen. Intern. Med. 2008, 24, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.J. Nitric Oxide, Atherosclerosis and the Clinical Relevance of Endothelial Dysfunction. Hear. Fail. Rev. 2003, 8, 71–86. [Google Scholar] [CrossRef] [PubMed]
- Saran, A.M.; DuBose, T.D. Cardiovascular disease in chronic kidney disease. Ther. Adv. Cardiovasc Dis. 2008, 2, 425–434. [Google Scholar] [CrossRef]
- Howden, E.J.; Leano, R.; Petchey, W.; Coombes, J.S.; Isbel, N.M.; Marwick, T.H. Effects of Exercise and Lifestyle Intervention on Car-diovascular Function in CKD. CJASN 2013, 8, 1494–1501. [Google Scholar] [CrossRef]
- Baylis, C. Nitric oxide deficiency in chronic kidney disease. Am. J. Physiol. Physiol. 2008, 294, F1–F9. [Google Scholar] [CrossRef]
- Tousoulis, D.; Kampoli, A.-M.; Tentolouris Nikolaos Papageorgiou, C.; Stefanadis, C. The Role of Nitric Oxide on Endothelial Function. Curr. Vasc. Pharmacol. 2012, 10, 4–18. [Google Scholar] [CrossRef]
- Baylis, C. Nitric oxide synthase derangements and hypertension in kidney disease. Curr. Opin. Nephrol. Hypertens. 2012, 21, 1–6. [Google Scholar] [CrossRef]
- Schiffrin, E.L. Oxidative Stress, Nitric Oxide Synthase, and Superoxide Dismutase: A Matter of Imbalance Underlies Endothe-lial Dysfunction in the Human Coronary Circulation. Hypertension 2008, 51, 31–32. [Google Scholar] [CrossRef] [PubMed]
- Landmesser, U.; Dikalov, S.; Price, S.R.; McCann, L.; Fukai, T.; Holland, S.M.; Mitch, W.E.; Harrison, D.G. Oxidation of tetrahydrobiopterin leads to uncoupling of endothelial cell nitric oxide synthase in hypertension. J. Clin. Investig. 2003, 111, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Galley, H.F.; Webster, N.R. Physiology of the endothelium. Br. J. Anaesth. 2004, 93, 105–113. [Google Scholar] [CrossRef]
- Bjork, L.; Jenkins, N.T.; Witkowski, S.; Hagberg, J.M. Nitro-Oxidative Stress Biomarkers in Active and Inactive Men. Int. J. Sports Med. 2012, 33, 279–284. [Google Scholar] [CrossRef]
- Szostak, J.; Laurant, P. The forgotten face of regular physical exercise: A “natural” anti-atherogenic activity. Clin. Sci. 2011, 121, 91–106. [Google Scholar] [CrossRef]
- Bloodsworth, A.; O’Donnell, V.B.; Freeman, B.A. Nitric Oxide Regulation of Free Radical- and Enzyme-Mediated Lipid and Lip-oprotein Oxidation. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1707–1715. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.I.; Saglam, M.; Caglar, K.; Cakir, E.; Sonmez, A.; Ozgurtas, T.; Aydin, A.; Eyileten, T.; Ozcan, O.; Acikel, C.; et al. The De-terminants of Endothelial Dysfunction in CKD: Oxidative Stress and Asymmetric Dimethylarginine. Am. J. Kidney Dis. 2006, 47, 42–50. [Google Scholar] [CrossRef]
- Chen, J.; Hamm, L.L.; Mohler, E.R.; Hudaihed, A.; Arora, R.; Chen, C.-S.; Liu, Y.; Browne, G.; Mills, K.T.; Kleinpeter, M.A.; et al. Interrelationship of Multiple Endothelial Dysfunction Biomarkers with Chronic Kidney Disease. PLoS ONE 2015, 10, e0132047. [Google Scholar] [CrossRef]
- Reddy, Y.S.; Kiranmayi, V.S.; Bitla, A.R.; Krishna, G.S.; Rao, P.; Sivakumar, V. Nitric oxide status in patients with chronic kidney disease. Indian J. Nephrol. 2015, 25, 287–291. [Google Scholar]
- Currie, K.D.; Mckelvie, R.S.; Macdonald, M.J. Flow-Mediated Dilation Is Acutely Improved after High-Intensity Interval Exercise. Med. Sci. Sports Exerc. 2012, 44, 2057–2064. [Google Scholar] [CrossRef]
- Harris, R.A.; Padilla, J.; Hanlon, K.P.; Rink, L.D.; Wallace, J.P. The Flow-mediated Dilation Response to Acute Exercise in Overweight Active and Inactive Men. Obesity 2008, 16, 578–584. [Google Scholar] [CrossRef]
- Harvey, P.J.; Morris, B.L.; Kubo, T.; Picton, P.E.; Su, W.S.; Notarius, C.F.; Floras, J.S. Hemodynamic after-effects of acute dynamic exercise in sedentary normotensive postmenopausal women. J. Hypertens. 2005, 23, 285–292. [Google Scholar] [CrossRef]
- Padilla, J.; Harris, R.A.; Fly, A.D.; Rink, L.D.; Wallace, J.P. The effect of acute exercise on endothelial function following a high-fat meal. Graefe’s Arch. Clin. Exp. Ophthalmol. 2006, 98, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Fisher-Wellman, K.; Bell, H.K.; Bloomer, R.J. Oxidative Stress and Antioxidant Defense Mechanisms Linked to Exercise During Cardiopulmonary and Metabolic Disorders. Oxidative Med. Cell. Longev. 2009, 2, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Radak, Z.; Chung, H.Y.; Koltai, E.; Taylor, A.W.; Goto, S. Exercise, oxidative stress and hormesis. Ageing Res. Rev. 2008, 7, 34–42. [Google Scholar] [CrossRef]
- Papadakis, Z.; Forsse, J.S.; Peterson, M.N. Acute partial sleep deprivation and high-intensity interval exercise effects on postprandial endothelial function. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 120, 2431–2444. [Google Scholar] [CrossRef]
- Bode-Böger, S.; Böger, R.H.; Schröder, E.P.; Frölich, J.C. Exercise Increases Systemic Nitric Oxide Production in Men. Eur. J. Cardiovasc. Prev. Rehabil. 1994, 1, 173–178. [Google Scholar] [CrossRef]
- Suhr, F.; Porten, S.; Hertrich, T.; Brixius, K.; Schmidt, A.; Platen, P.; Bloch, W. Intensive exercise induces changes of endothelial nitric oxide synthase pattern in human erythrocytes. Nitric Oxide. 2009, 20, 95–103. [Google Scholar] [CrossRef]
- Son, Y.; Kim, K.; Jeon, S.; Kang, M.; Lee, S.; Park, Y. Effect of Exercise Intervention on Flow-Mediated Dilation in Overweight and Obese Adults: Meta-Analysis. Int. J. Vasc. Med. 2017, 2017, 7532702. [Google Scholar] [CrossRef]
- Early, K.S.; Stewart, A.; Johannsen, N.; Lavie, C.J.; Thomas, J.R.; Welsch, M. The Effects of Exercise Training on Brachial Artery Flow-Mediated Dilation: A Meta-analysis. J. Cardiopulm Rehabil Prev. 2017, 37, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Fox, B.M.; Brantley, L.; White, C.; Seigler, N.; Harris, R.A. Association beween resting heart rate, shear and flow-mediated dilation in healthy adults. Exp. Physiol. 2014, 99, 1439–1448. [Google Scholar] [CrossRef]
- Thijssen, D.H.J.; Bruno, R.M.; Van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.; Luscher, T.; et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Hear. J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef]
- Koyoshi, R.; Miura, S.-I.; Kumagai, N.; Shiga, Y.; Mitsutake, R.; Saku, K. Clinical significance of flow-mediated dilation, brachial intima-media thickness and pulse wave velocity in patients with and without coronary artery disease. Circ. J. 2012, 76, 1469–1475. [Google Scholar] [CrossRef]
- Birk, G.; Dawson, E.; Batterham, A.; Atkinson, G.; Cable, T.; Thijssen, D.H.J.; Green, D.J. Effects of Exercise Intensity on Flow Mediated Dilation in Healthy Humans. Int. J. Sports Med. 2012, 34, 409–414. [Google Scholar]
- Padilla, J.; Johnson, B.D.; Newcomer, S.C.; Wilhite, D.P.; Mickleborough, T.D.; Fly, A.D.; Mather, K.J.; Wallace, J.P. Normalization of flow-mediated dilation to shear stress area under the curve eliminates the impact of variable hyperemic stimulus. Cardiovasc. Ultrasound 2008, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Horvath, T.; Pinter, A.; Kollai, M. Carotid artery stiffness is not related to endothelial function in young healthy subjects. Auton. Neurosci. 2012, 166, 85–88. [Google Scholar] [CrossRef]
- Tarro Genta, F.; Eleuteri, E.; Temporelli, P.L.; Comazzi, F.; Tidu, M.; Bouslenko, Z.; Bertolin, F.; Vigorito, C.; Giannuzzi, P.; Giallauria, F.; et al. Flow-Mediated Dilation Normalization Predicts Outcome in Chronic Heart Failure Patients. J. Card. Fail. 2013, 19, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Takase, B.; Uehata, A.; Akima, T.; Nagai, T.; Nishioka, T.; Hamabe, A.; Satomura, K.; Ohsuzu, F.; Kurita, A. Endothelium-dependent flow-mediated vasodilation in coronary and brachial arteries in suspected coronary artery disease. Am. J. Cardiol. 1998, 82, 1535–1539. [Google Scholar] [CrossRef]
- Green, D.J.; Eijsvogels, T.; Bouts, Y.M.; Maiorana, A.J.; Naylor, L.H.; Scholten, R.R.; Spaanderman, M.E.A.; Pugh, C.J.A.; Sprung, V.S.; Schreuder, T.; et al. Exercise training and artery function in humans: Nonresponse and its relationship to cardiovas-cular risk factors. J. Appl. Physiol. 2014, 117, 345–352. [Google Scholar] [CrossRef]
- Wen, Y.; Wang, X.; Guo, Y.; Jin, M.; Xi, J.; Chen, T.; Shi, K.; Lu, Y. Predictive value of brachial artery flow-mediated dilation on coronary artery abnormality in acute stage of Kawasaki disease. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Eiselt, J.; Rajdl, D.; Racek, J.; Vostrý, M.; Rulcová, K.; Wirth, J. Asymmetric Dimethylarginine and Progression of Chronic Kid-ney Disease—A One-Year Follow-Up Study. Kidney Blood Press Res. 2014, 39, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Van Craenenbroeck, A.H.; Van Craenenbroeck, E.M.; Van Ackeren, K.; Vrints, C.J.; Conraads, V.M.; Verpooten, G.A.; Kouidi, E.; Cout-tenye, M.M. Effect of Moderate Aerobic Exercise Training on Endothelial Function and Arterial Stiffness in CKD Stages 3-4: A Randomized Controlled Trial. Am. J. Kidney Dis. 2015, 66, 285–296. [Google Scholar] [CrossRef]
- Widlansky, M.E.; Gokce, N.; Keaney, J.; John, F.; Vita, J.A. The clinical implications of endothelial dysfunction. J. Am. Coll Cardiol. 2003, 42, 1149–1160. [Google Scholar] [CrossRef]
- Woodman, R.J.; Playford, D.A.; Watts, G.F.; Cheetham, C.; Reed, C.; Taylor, R.R.; Puddey, I.B.; Beilin, L.J.; Burke, V.; Mori, T.A.; et al. Im-proved analysis of brachial artery ultrasound using a novel edge-detection software system. J. Appl. Physiol. 2001, 91, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Pyke, K.E.; Tschakovsky, M.E. The relationship between shear stress and flow-mediated dilatation: Implications for the as-sessment of endothelial function. J. Physiol. 2005, 568 Pt 2, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Forsse, J.S.; Peterson, M.; Papadakis, Z.; Gutierrez, F.; Schwedock, N.; Hess, B.W.; Griggs, J.O.; Allison, D.C.; Wilson, R.L.; Grandjean, P.W.; et al. Brachial Artery FMD Responses To Steady-State Moderate-Intensity And High-Intensity Interval Exercise In Mid-Spectrum Chronic Kidney Disease: 1202 Board #10 May 31 8. Med. Sci. Sports Exerc. 2018, 50, 276–277. [Google Scholar]
- Van Beaumont, W. Red cell volume with changes in plasma osmolarity during maximal exercise. J. Appl. Physiol. 1973, 35, 47–50. [Google Scholar] [CrossRef]
- Welsch, M.A.; Allen, J.; Geaghan, J.P. Stability and reproducibility of brachial artery flow-mediated dilation. Med. Sci. Sports Exerc. 2002, 34, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Sales, A.R.K.; Fernandes, I.A.; Rocha, N.G.; Costa, L.S.; Rocha, H.N.M.; Mattos, J.D.M.; Vianna, L.C.; Silva, B.M.; Nobrega, A.C.L. Aerobic exercise acutely prevents the endothelial dysfunction induced by mental stress among subjects with metabolic syn-drome: The role of shear rate. Am. J. Physiol.—Heart Circ. Physiol. 2014, 306, H963–H971. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhang, M.; Wang, H.; Sun, C.; Feng, Y.; Zhu, W.; Cao, D.; Shao, Q.; Li, N.; Xia, Y.; et al. Vitamin D supplementation im-proves endothelial dysfunction in patients with non-dialysis chronic kidney disease. Int Urol Nephrol. 2018, 50, 923–927. [Google Scholar] [CrossRef]
- Coutinho, M.N.; Carvalho, A.B.; Dalboni, M.A.; Mouro, M.G.; Higa, E.M.S.; Costa-Hong, V.; Bortolotto, L.A.; Figueiredo, R.; Canziani, M.E.F. There Is No Impact of Diabetes on the Endothelial Function of Chronic Kidney Disease Patients. J. Diabetes Res. 2018, 2018, 7926473. [Google Scholar] [CrossRef]
- Llewellyn, T.L.; Chaffin, M.E.; Berg, K.E.; Meendering, J.R. The relationship between shear rate and flow-mediated dilation is al-tered by acute exercise. Acta Physiol. 2012, 205, 394–402. [Google Scholar] [CrossRef]
- Hwang, I.-C.; Kim, K.-H.; Choi, W.-S.; Kim, H.-J.; Im, M.-S.; Kim, Y.-J.; Kim, S.-H.; Kim, M.-A.; Sohn, D.-W.; Zo, J.-H. Impact of acute exercise on brachial artery flow-mediated dilatation in young healthy people. Cardiovasc. Ultrasound 2012, 10, 39. [Google Scholar] [CrossRef]
- Riccioni, G.; Scotti, L.; Guagnano, M.T.; Bosco, G.; Bucciarelli, V.; Ilio, E.D.; Speranza, L.; Martini, F.; Bucciarelli, T. Physical exercise reduces synthesis of ADMA, SDMA, and L-Arg. Front. Biosci 2015, 7, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Tanahashi, K.; Akazawa, N.; Miyaki, A.; Choi, Y.; Ra, S.-G.; Matsubara, T.; Kumagai, H.; Oikawa, S.; Miyauchi, T.; Maeda, S.; et al. Plas-ma ADMA concentrations associate with aerobic fitness in postmenopausal women. Life Sci. 2014, 108, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Böger, R.H. Asymmetric Dimethylarginine, an Endogenous Inhibitor of Nitric Oxide Synthase, Explains the “l-Arginine Par-adox” and Acts as a Novel Cardiovascular Risk Factor. J. Nutr. 2004, 134, 2842S–2847S. [Google Scholar] [CrossRef] [PubMed]
- Tomás, M.; Elosua, R.; Sentí, M.; Molina, L.; Vila, J.; Anglada, R.; Fito, M.; Covas, M.I.; Marrugat, J. Paraoxonase1-192 polymor-phism modulates the effects of regular and acute exercise on paraoxonase1 activity. J. Lipid Res. 2002, 43, 713–720. [Google Scholar] [CrossRef]
- Taylor, J.K.; Esco, M.R.; Qian, L.; Dugan, K.; Jones, K. A single session of aerobic exercise influences paraoxonase 1 activity and concentration (Una sola sesión de ejercicio aeróbico influye en la actividad y concentración de la paraoxonasa). Retos 2015, 222–225. [Google Scholar] [CrossRef]
- Arslan, C.; Gulcu, F.; Gursu, M.F. Effects of oxidative stress caused by acute and regular exercise on levels of some serum metabolites and the activities of paraoxonase and arylesterase. Biol. Sport 2005, 22, 375. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | (n = 20) |
|---|---|
| Age (y) | 62.0 ± 10 |
| Height (cm) | 167.1 ± 8.6 |
| Weight (kg) | 80.9 ± 15.8 |
| BMI (kg/m2) | 28.8 ± 4.3 |
| Waist (cm) | 98.9 ± 12.7 |
| BF (%) | 28.8 ± 12.7 |
| Rest SBP (mmHg) | 125.4 ± 10.7 |
| Rest DBP (mmHg) | 81.4 ± 5.1 |
| Rest HR (bpm) | 71.3 ± 11.5 |
| Creatinine (mg/dL) | 1.11 ± 0.2 |
| eGFR | 51.5 ± 6.5 |
| Glucose (mg/dL) | 117 ± 70.2 |
| Total Cholesterol (mg/dL) | 173.7 ± 36.3 |
| LDL (mg/dL) | 91.9 ± 28.8 |
| HDL (mg/dL) | 50.7 ± 15.2 |
| Triglycerides (mg/dL) | 155.9 ± 53.2 |
| VO2 max (mL/kg/min) | 19.4 ± 4.6 |
| Medications | Users (total n = 20) |
| ARB | 3 (20) |
| ACE Inhibitor | 6 (20) |
| α-Blocker | 2 (20) |
| β-Blocker | 4 (20) |
| Metformin | 7 (20) |
| Statin | 10 (20) |
| Steroids | 2 (20) |
| T3/T4 | 3 (20) |
| Pre | 1-HR | 24-HR | ||||
|---|---|---|---|---|---|---|
| Condition | Pre-OCC | Post-OCC | Pre-OCC | Post-OCC | Pre-OCC | Post-OCC |
| HIIE (mm) | 3.42 ± 0.13 | 3.83 ± 0.12 | 3.44 ± 0.13 | 3.96 ± 0.13 * | 3.35 ± 0.12 | 3.86 ± 0.13 * |
| SSE (mm) | 3.37 ± 0.13 | 3.75 ± 0.12 | 3.33 ± 0.13 | 3.87 ± 0.11 * | 3.43 ± 0.13 | 3.89 ± 0.13 * |
| Condition | Pre | 1-HR | 24-HR |
|---|---|---|---|
| HIIE | |||
| Max Flow (cm−1) | 171.9 ± 11.7 | 173.5 ± 16.8 | 195.9 ± 14.2 |
| Shear Rate (s−1) | 374.7 ± 35.2 | 370.9 ± 52.2 | 429.1 ± 41.6 |
| SSE | |||
| Max Flow (cm−1) | 172.9 ± 10.5 | 154.3 ± 9.3 | 165.9 ± 9.3 |
| Shear Rate (s−1) | 373.8 ± 22.4 | 325.5 ± 23.5 | 351.4 ± 26.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsse, J.S.; Papadakis, Z.; Peterson, M.N.; Taylor, J.K.; Hess, B.W.; Schwedock, N.; Allison, D.C.; Griggs, J.O.; Wilson, R.L.; Grandjean, P.W. The Influence of an Acute Bout of Aerobic Exercise on Vascular Endothelial Function in Moderate Stages of Chronic Kidney Disease. Life 2022, 12, 91. https://doi.org/10.3390/life12010091
Forsse JS, Papadakis Z, Peterson MN, Taylor JK, Hess BW, Schwedock N, Allison DC, Griggs JO, Wilson RL, Grandjean PW. The Influence of an Acute Bout of Aerobic Exercise on Vascular Endothelial Function in Moderate Stages of Chronic Kidney Disease. Life. 2022; 12(1):91. https://doi.org/10.3390/life12010091
Chicago/Turabian StyleForsse, Jeffrey S., Zacharias Papadakis, Matthew N. Peterson, James Kyle Taylor, Burritt W. Hess, Nicholas Schwedock, Dale C. Allison, Jackson O. Griggs, Ronald L. Wilson, and Peter W. Grandjean. 2022. "The Influence of an Acute Bout of Aerobic Exercise on Vascular Endothelial Function in Moderate Stages of Chronic Kidney Disease" Life 12, no. 1: 91. https://doi.org/10.3390/life12010091
APA StyleForsse, J. S., Papadakis, Z., Peterson, M. N., Taylor, J. K., Hess, B. W., Schwedock, N., Allison, D. C., Griggs, J. O., Wilson, R. L., & Grandjean, P. W. (2022). The Influence of an Acute Bout of Aerobic Exercise on Vascular Endothelial Function in Moderate Stages of Chronic Kidney Disease. Life, 12(1), 91. https://doi.org/10.3390/life12010091